
Abstract
Study Design
Retrospective cohort.
Objectives
To compare outcomes of posterior osteotomized debridement (OD) with combined anterior and posterior approach (AP) in treating thoracolumbar tuberculosis (TB).
Methods
This study reviewed 178 patients who were diagnosed as active thoracolumbar TB and surgically treated in our center. One hundred and two patients underwent posterior OD, interbody fusion with titanium mesh cage (TMC), and instrumentation (group A). Seventy-six patients underwent one-stage posterior instrumentation, anterior debridement, and interbody fusion with TMC (group B). Patients’ clinical outcomes were compared between the 2 groups.
Results
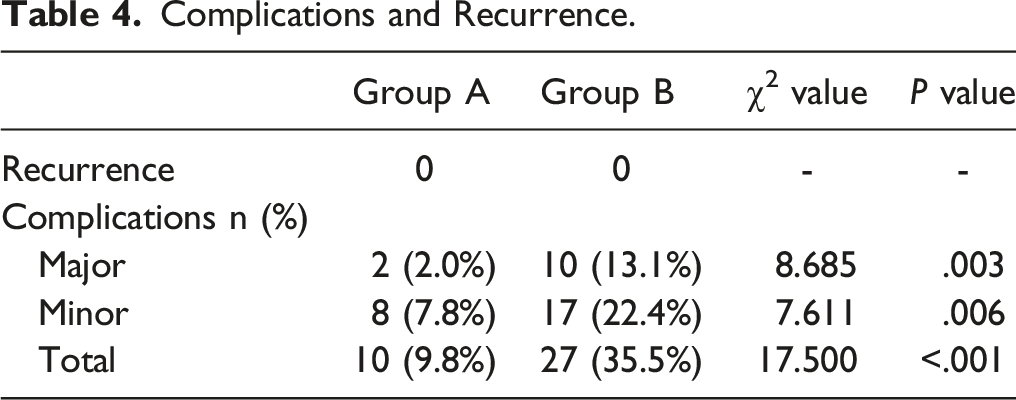
Erythrocyte sedimentation rate and C-reactive protein in all patients returned to normal levels within 3 months after surgery, and no recurrence occurred during the follow-up. Compared with AP approach, OD surgery was less invasive and with a lower cost (¥ 70 581 ± 17 645 vs ¥ 87 600 ± 27 328; P < .05). Patients treated by OD showed more significant improvements in Visual Analog Scale (VAS) and Oswestry Disability Index (ODI) than those treated by AP approach 3 months postoperatively (VAS: 3.0 ± .7 vs 3.7 ± .9; ODI: 14.7 ± 4.4 vs 20.6 ± 4.6). Two groups showed similar postoperative kyphosis correction and final follow-up correction loss (P = .361 and P = .162, respectively). The OD method had a lower complication rate than AP approach (9.8% [10/102] vs 35.5% [27/76]; P < .05).
Conclusions
Posterior OD is effective in treating active thoracolumbar TB. Compared with traditional AP approach, OD surgery has less surgical invasiveness, lower complication rate, and shorter fusion time.
Introduction
Spinal tuberculosis (TB), which mainly occurs in thoracic and lumbar spine and often leads to kyphotic deformity and neurological deficits, has shown a steady increase in developing countries. It is acknowledged that anti-TB drugs are the mainstay for the treatment of spinal TB. However, for patients with spinal instability, progressive kyphosis, and spinal cord compression, surgical interventions are usually required. 1
There are a variety of surgical strategies for the treatment of thoracolumbar TB; however, no standardized surgical procedure has been established until now. The anterior approach provides direct access to the TB lesion and can achieve satisfactory debridement without destroying the posterior column. However, the anterior fixation is not biomechanically strong enough, which often leads to graft failure and insufficient kyphosis correction.2,3 As a result, currently, anterior surgery is not used as frequently as before in clinical practice. Some scholars put forward that the spinal stability and kyphosis correction can be better accomplished with posterior instrumentation.4,5 Anterior debridement combined with posterior instrumentation (AP), therefore, was applied to the surgical treatment of thoracolumbar TB and achieved good outcomes.6,7 Posterior-only approach is another common method as it is less aggressive and provides a strong three-column fixation with the use of pedicle screws. Nevertheless, some surgeons pointed out that because spinal TB lesions are generally located in the anterior and middle column, traditional posterior curetted debridement (CD) cannot achieve complete lesion clearance and it may cause spreading of Mycobacterium tuberculosis and recurrence of spinal TB.8,9 To compensate for the deficiency of CD, osteotomized debridement (OD) technique was proposed, and its superiorities over CD, including shorter fusion time, lower recurrence rate, and lower complication rate, were elaborated in a recent study. 10
AP approach and posterior-only approach with OD are both common methods in treating thoracolumbar TB at present. However, studies comparing the 2 methods remain rare. In this study, we evaluated patients with thoracolumbar TB who were treated with one-stage posterior OD, interbody fusion with titanium mesh cages (TMCs), and instrumentation, and compared the clinical outcomes with those of patients who were treated with one-stage posterior instrumentation, anterior debridement, and interbody fusion with TMCs to determine the clinical efficacy of the 2 surgical methods.
Materials and Methods
Patient Population
Between November 2013 and November 2019, 178 patients who were diagnosed with active thoracolumbar TB and received operative treatment at our hospital were included in this study. The Ethics Committee of the First Affiliated Hospital of Nanchang University approved the study (No. 2021042). All patients provided written informed consent for use of the data.
Operations were performed by consultant orthopedists from several surgical teams. One hundred and two patients were treated by one-stage posterior OD, interbody fusion with TMCs, and instrumentation (group A); and seventy-six patients were treated with one-stage posterior instrumentation, anterior debridement, and interbody fusion with TMCs (group B). Patients were diagnosed as active spinal TB by clinical symptoms, laboratory tests such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and radiological examinations including x-ray, computed tomography (CT), and magnetic resonance imaging. Confirmation of TB was ultimately made using pathological examinations.
Patients having at least one of the following criteria were included: (1) persistent pain due to spinal instability; (2) progressive local kyphosis; (3) compression of spinal cord or cauda equina by TB lesions; (4) presence of extensive sequestrum or paravertebral abscesses. The exclusion criteria were as follows: (1) severe osteoporosis; (2) history of spine surgery at infected levels; (3) presence of spinal diseases such as scoliosis or ankylosing spondylitis; (4) intolerance of operation due to poor general condition.
Preoperative Preparation
All patients were generally treated with HREZ chemotherapy for 2 weeks prior to the surgery, including isoniazid (300 mg/day), rifampicin (450 mg/day), and pyrazinamide (750 mg/day), and ethambutol (750 mg/day). Surgeries were performed when ESR and CRP significantly decreased, anemia and hypoproteinemia were improved, and the temperature returned to normal.
Operative Technique
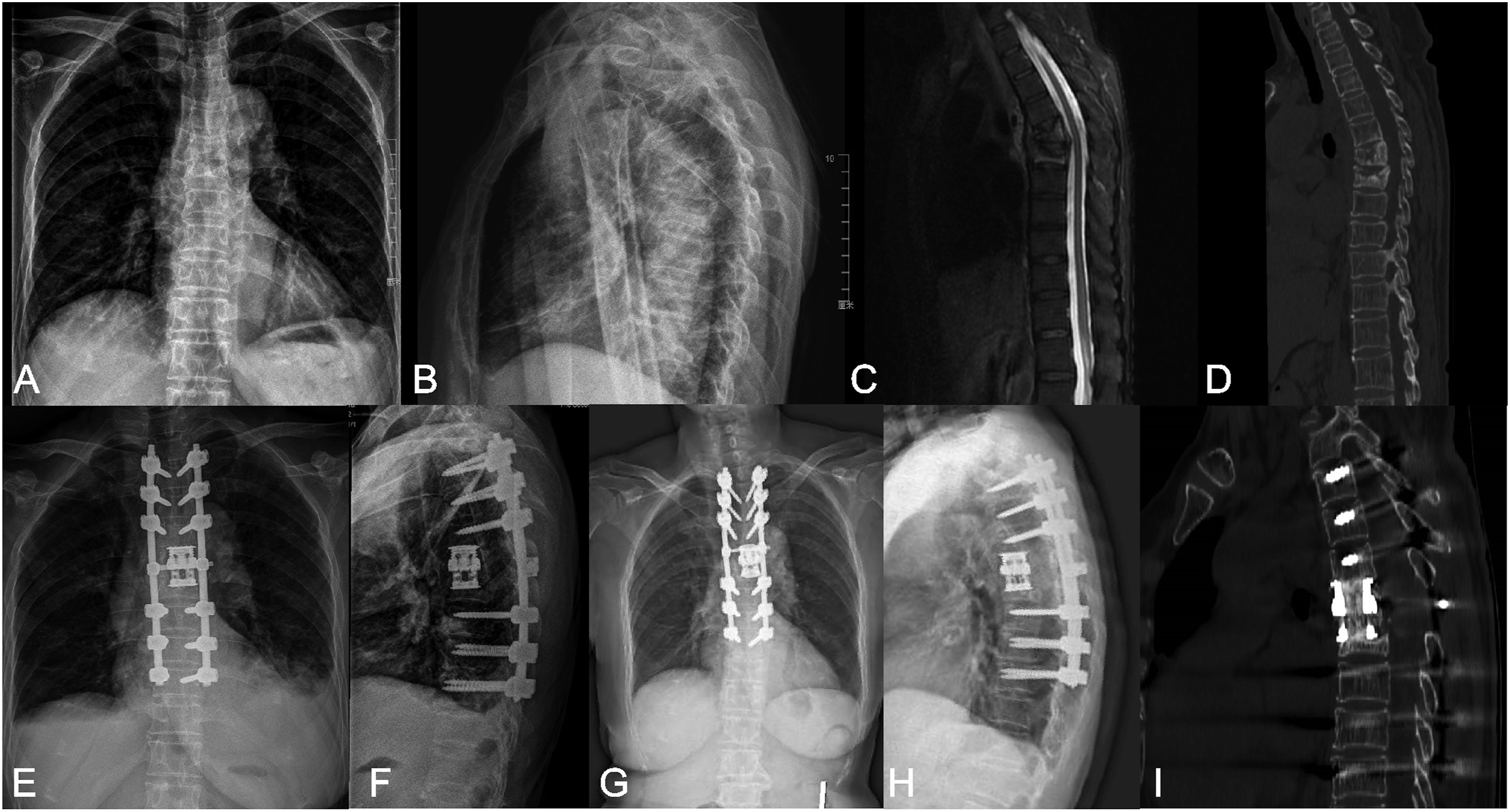
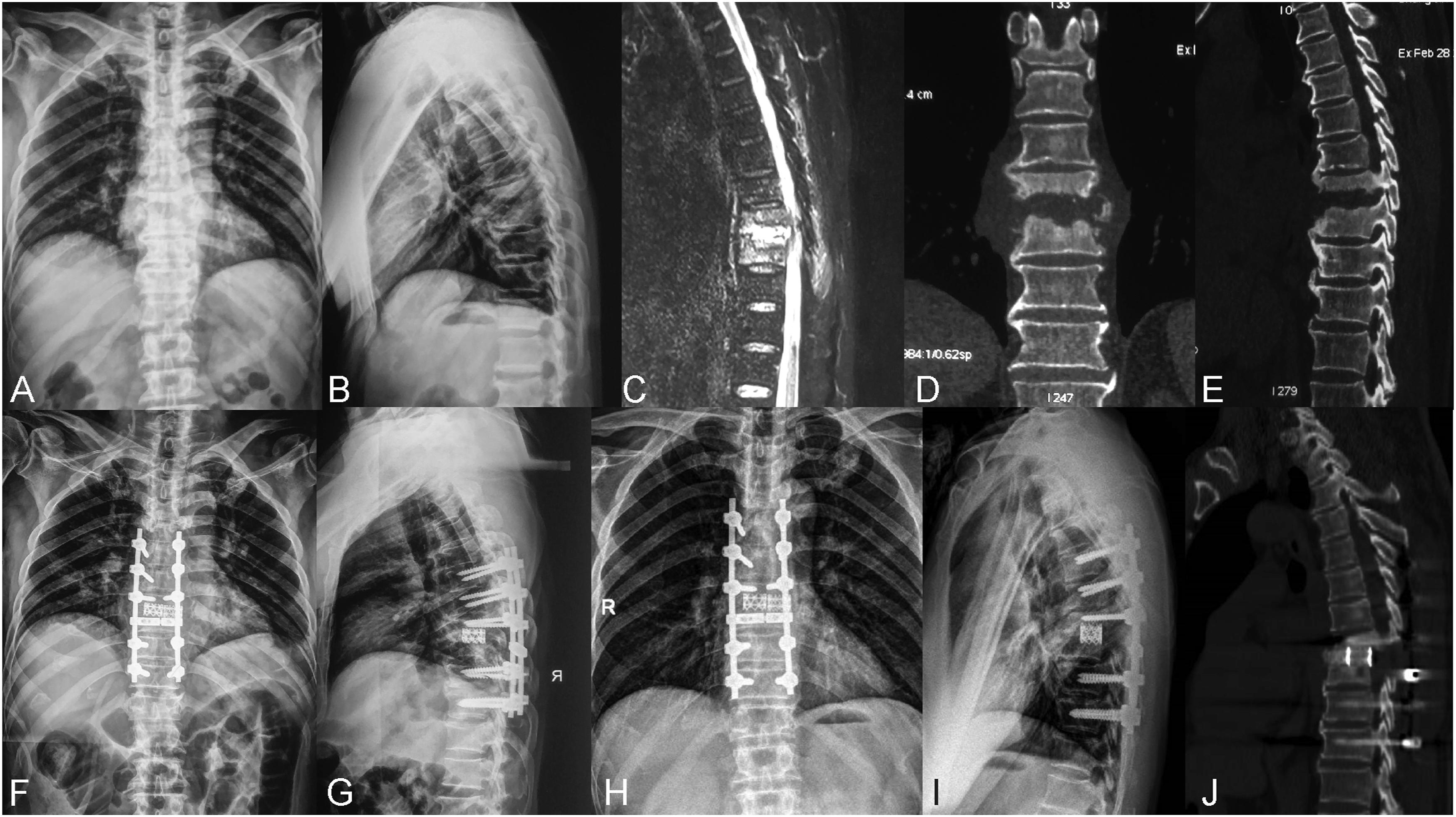
Patients in group A were operated on while under general anesthesia in the prone position. A posterior midline incision was used and subperiosteal dissection was done for the exposure of spinous processes, laminae, facet joints, and transverse processes. Subsequently, pedicle screws were placed into normal vertebrae at least 2 levels above and below the diseased segments, followed by the placement of a temporary rod on the mild side of the focus to stabilize the spine during the osteotomy. Screws were also inserted into the diseased vertebra if the lesion did not affect the pedicles. According to the degree and distribution of the lesions, the spinous processes, unilateral or bilateral laminae, facet joints and pedicles were removed. Transverse processes, part of ribs, and nerve roots were cut off if necessary for easy manipulation in thoracic spinal TB. Thereafter, the lesions such as sequestrum, caseous necrosis and infected intervertebral discs were preliminarily cleared by curettes in preparation of osteotomy. Then, the most cephalad and caudad vertebrae that were incompletely destroyed were confirmed. Osteotomy was performed through the healthy bone near the focus and the osteotomy planes were parallel to adjacent endplates. When both sides needed to be disposed of, the rod was switched to the opposite side and procedures mentioned above were performed again on the other side. Then, autogenous morselized bone harvested from healthy spinous processes and laminae as well as the iliac crest was filled into appropriately sized TMCs and implanted into the intervertebral space with great care. Finally, the other rod was fixed and both sides were compressed to correct kyphosis deformity (Figure 1). Drains were placed and the incision was closed in layers. Typical cases are shown in Figures 2 and 3. The osteotomized debridement (OD) procedures are shown. (A) The osteotomy range is indicated by the two lines. (B) An appropriately sized titanium mesh cage (TMC) filled with autogenous bone is implanted into the intervertebral space and rods is fixed. A 70-year-old female with a T6-7 TB lesion was treated with posterior osteotomized osteotomy (OD), bone grafting with a titanium mesh cage (TMC), and instrumentation. (A–D) Preoperative anteroposterior and lateral x-rays, MRI and CT showed vertebral destruction with kyphosis. (E–F) Postoperative anteroposterior and lateral x-rays displayed a good position of internal fixation and deformity correction. (G–I) X-rays and CT presented a good spinal alignment and satisfactory bone fusion at 24-month follow-up. A 59-year-old male with a T8-9 TB lesion was treated by posterior osteotomized osteotomy (OD) and reconstruction with two titanium mesh cages (TMCs). (A–E) Severe vertebral destruction was confirmed by preoperative x-rays, MRI and CT. (F–G) Postoperative x-rays showed a good position of the internal fixation. (H–J) X-rays and CT presented a favorable alignment and satisfactory bone fusion at 24-month follow-up.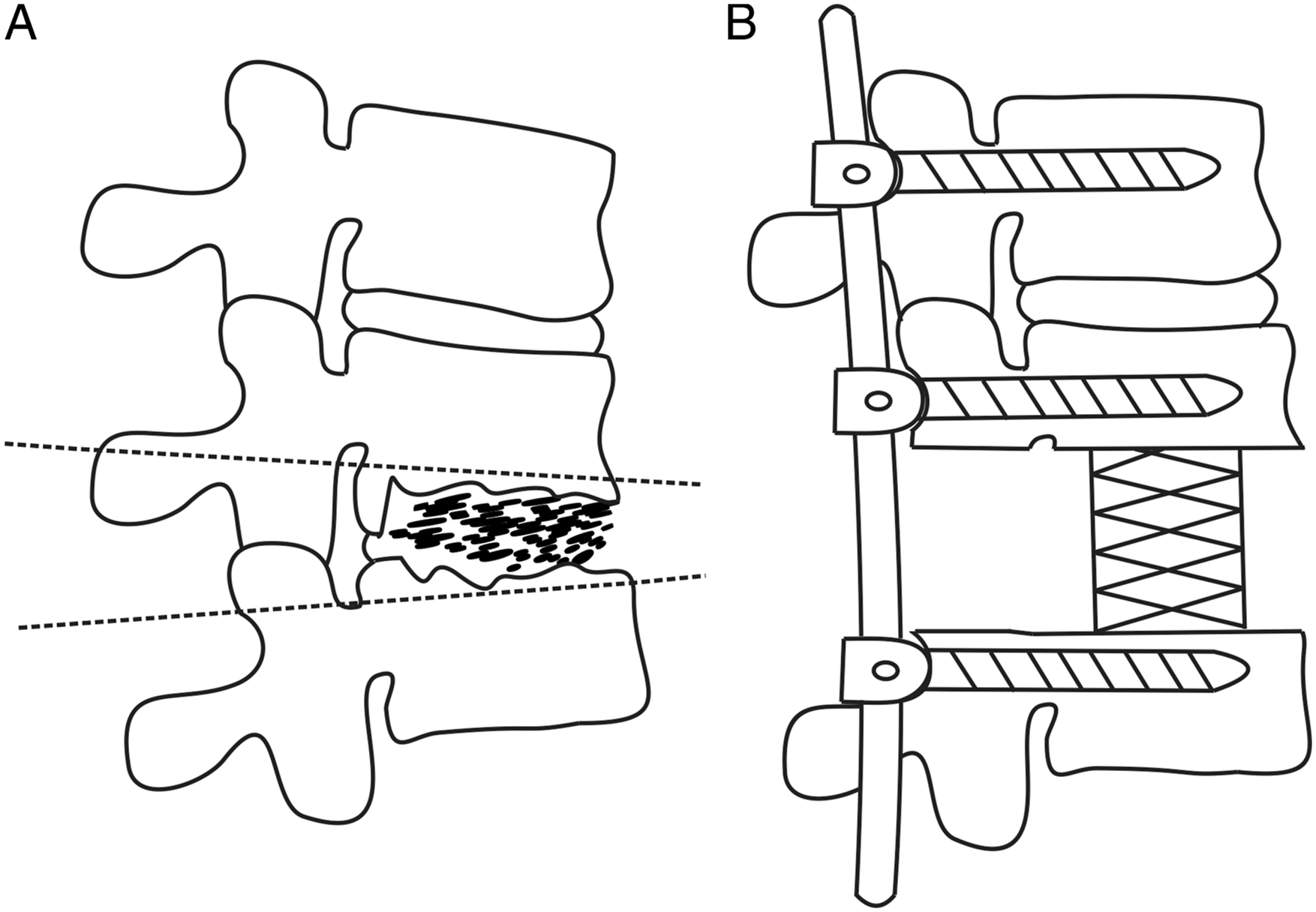
In Group B, posterior exposure and pedicle screw insertion were performed in patients in prone position as described in group A. Of the 76 patients, laminectomy was performed to relieve the compression from posterior column in 8 patients, and canal occupancy was cleared as much as possible. Ponte osteotomy was performed to increase flexibility in 9 patients, as rigidity was found during the surgery. Contoured rods were fixed after kyphosis correction by compression. Then the levels that needed to be fused anteriorly were grafted posteriorly using autogenous or allogeneic bone after the decortication of the laminae and transverse processes. Finally, drains were placed and the incision was closed.
Patients were then readjusted to a lateral decubitus position, leaving the severely involved side upward. The extrapleural or extraperitoneal anterior-lateral approach was taken. Ribs at involved levels were usually resected in thoracic spine for better exposure. Then pus was drained, and sequestrum, caseous necrosis, and infected intervertebral discs were thoroughly debrided by curettes until healthy bleeding bone was obtained. After sufficient nerve decompression and a thorough saline wash, appropriately sized TMCs filled with autogenous bone were implanted into the defect to restore the intervertebral height. Finally, drains were placed and the incision was closed. A typical case is shown in Figure 4. A 21-year-old female patient who showed a T11–12 lesion with bone destruction and dural compression was treated by posterior instrumentation, anterior debridement, and bone grafting with a titanium mesh cage (TMC). (A–E) Preoperative x-rays, CT, and MRIs were shown. (F–G) X-rays showed a good position of instrumentation after surgery. (H–J) X-rays and CT presented satisfactory bone union, and no obvious correction loss was observed at 36-month follow-up.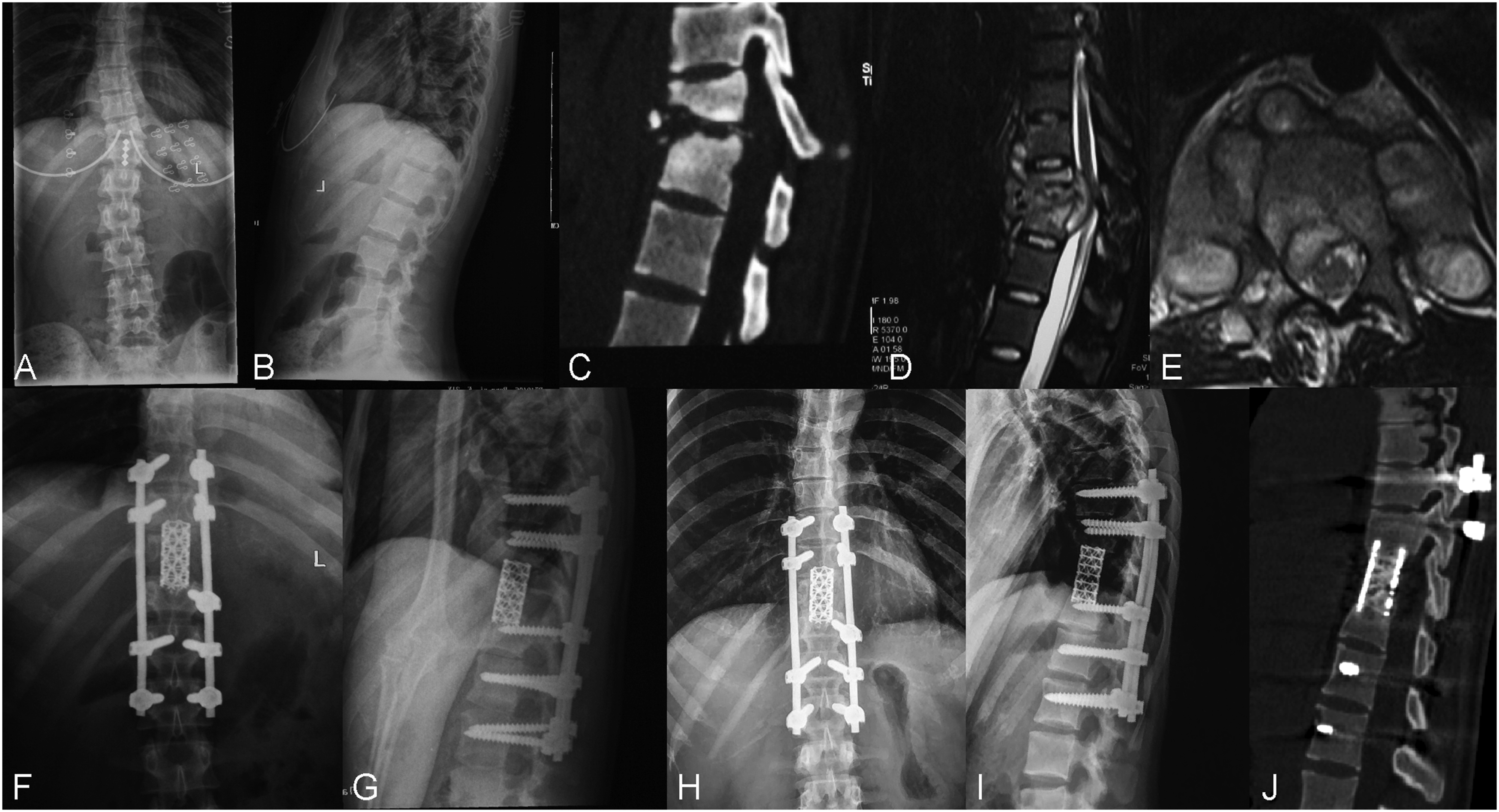
The specimens from 2 groups were sent for bacterial culture and pathological examination.
Postoperative Management
The drainage tubes were usually removed when the volume was less than 50 mL in 24 hours. Intravenous antibiotics were administered for 2 days postoperatively, and patients continued with the oral anti-TB drugs for 6-9 months. Generally, passive exercise of limb muscles, flexion and extension of joints were carried out when anesthesia had subsided. From the second postoperative day, patients were instructed to do active exercise and allowed to get out of bed and sit on the side of the bed with a brace after drainage tubes removal. Gait training was used to improve walking ability during the hospital stay. Ambulation with a brace was allowed 6-8 weeks after discharge. All patients were examined clinically and radiologically at 4 weeks, 3 months, 6 months, 9 months, and 12 months after surgery and then once a year. Laboratory indices such as CRP and ESR were evaluated monthly after surgery.
Clinical Outcomes and Follow-Up Evaluation
Invasiveness of the procedures
To assess the invasiveness of each approach, values of estimated blood loss (EBL), operation time, and length of hospitalization stay (LOS) were analyzed.
Laboratory findings and clinical efficacy
Infection was monitored using CRP and ESR. The severity of pain and the degree of dysfunction were assessed by Visual Analog Scale (VAS) and Oswestry Disability Index (ODI), respectively.
Spinal deformity and fusion
The degree of kyphosis was evaluated by the kyphotic angle, which was measured by Cobb’s method as the angle between the upper and lower endplates of the infected level on a lateral x-ray image of the spine. Bone fusion was confirmed by x-ray and CT images according to the modified criteria described by Lee et al, 11 including bony trabecular bridging across the graft-host interface, no motion (less than 3°) on a flexion-extension radiograph, and no gap at the interface.
Complications and recurrence
Intraoperative complications were recorded and postoperative complications were assessed based on radiographs and clinical findings of each patient. Complications were further compartmentalized into major and minor complications. The complications were considered major if they caused prolonged hospitalization, resulted in a change of functional status, or required an invasive procedure to treat. Recurrence was evaluated by patient’s clinical symptoms, laboratory tests and radiological examinations.
Statistical analysis
SPSS version 19.0 statistical software (SPSS, Inc., Chicago, IL, USA) was used to analyze the data. Independent sample t-test was applied to assess the differences between the groups with respect to patient data and clinical outcomes. The Chi-square test was used to compare the categorical variables between the 2 groups. The paired t-test was applied to compare the changes of the indices within each group preoperatively, postoperatively, and during follow-up. P values of <.05 were considered statistically significant.
Results
The Clinical Data of Patients in 2 Groups.
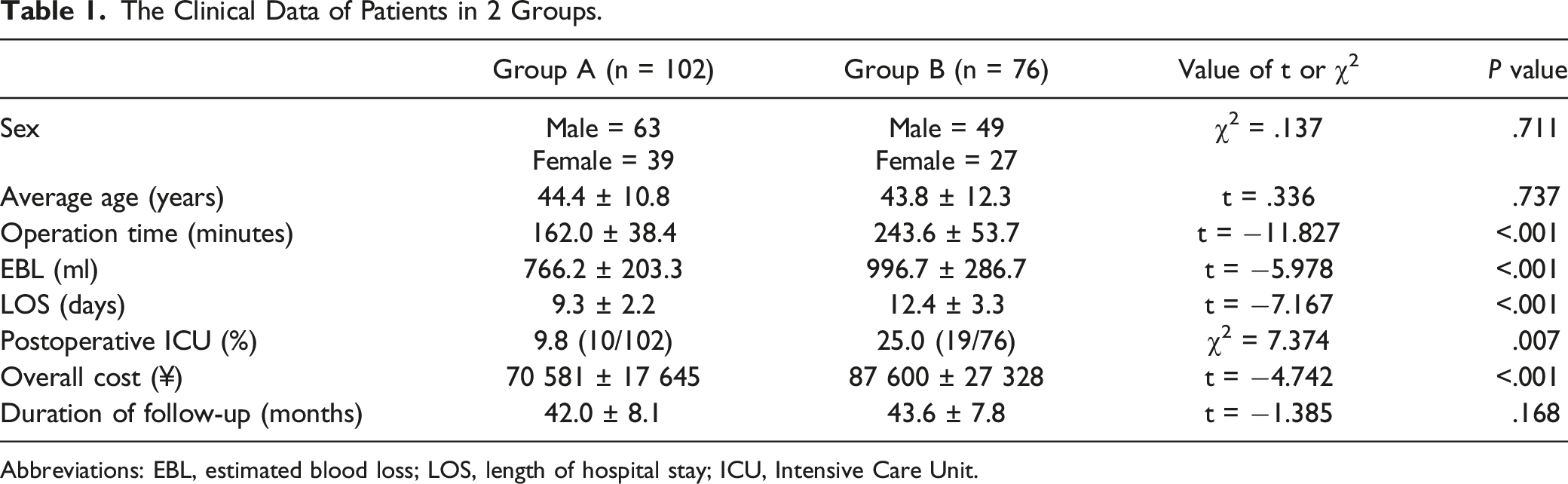
Abbreviations: EBL, estimated blood loss; LOS, length of hospital stay; ICU, Intensive Care Unit.
Clinical Evaluation and Inflammatory Indicators in 2 Groups.
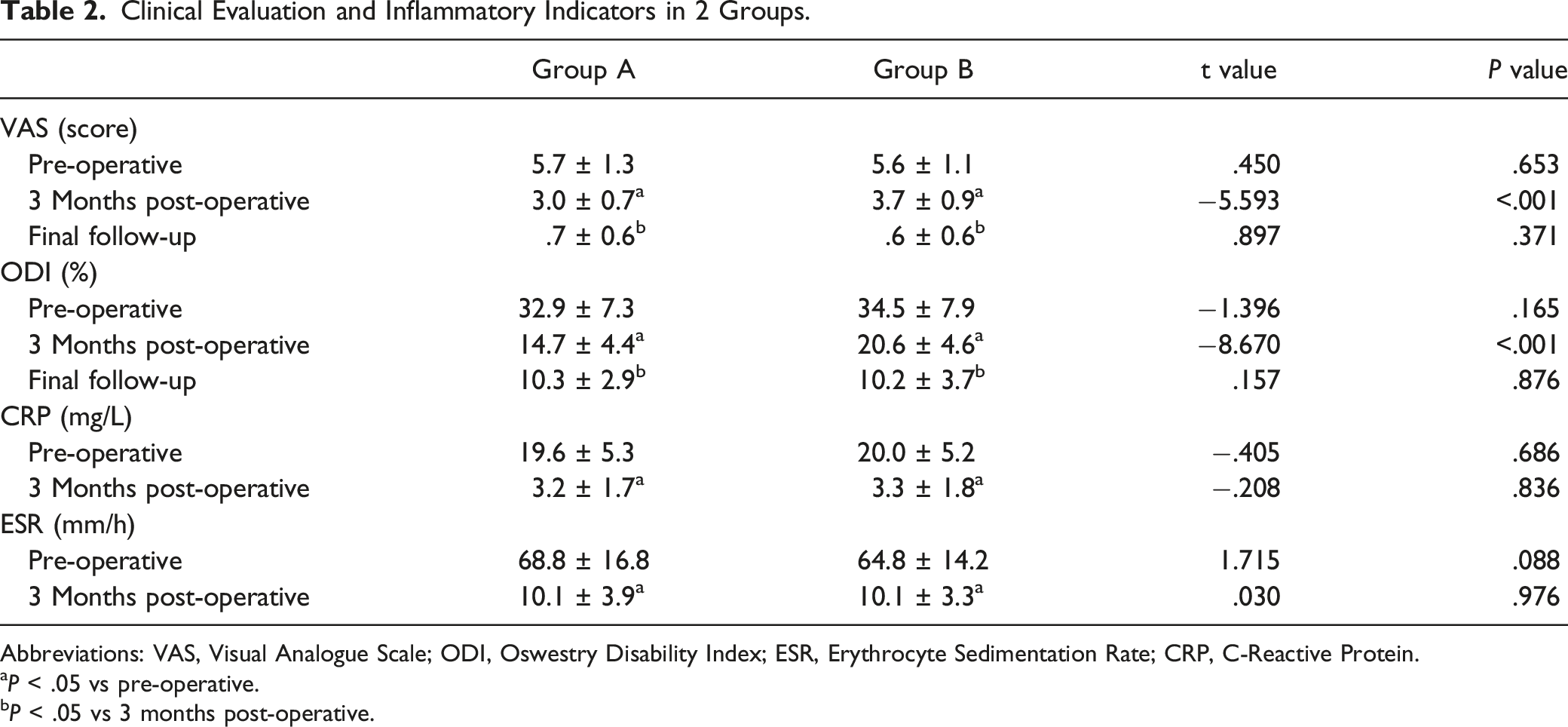
Abbreviations: VAS, Visual Analogue Scale; ODI, Oswestry Disability Index; ESR, Erythrocyte Sedimentation Rate; CRP, C-Reactive Protein.
aP < .05 vs pre-operative.
bP < .05 vs 3 months post-operative.
Radiological Data in 2 Groups.
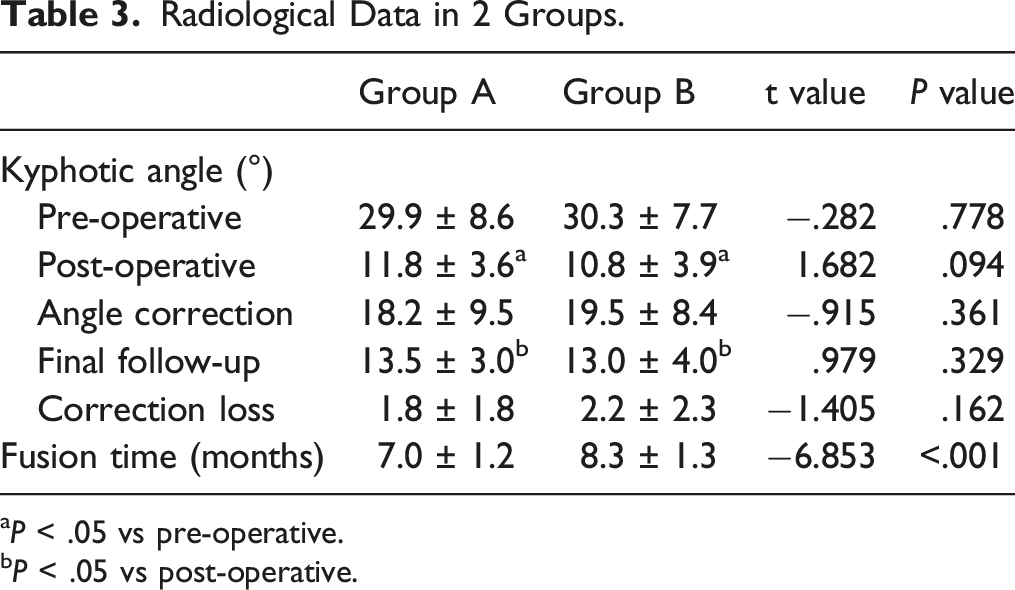
aP < .05 vs pre-operative.
bP < .05 vs post-operative.
Complications and Recurrence.
Discussion
Generally, the surgical methods in treating thoracolumbar TB can be commonly categorized into 3 forms: (1) one-stage anterior debridement with bone grafting and instrumentation; (2) posterior instrumentation, anterior debridement, and bone grafting; and (3) one-stage posterior debridement with bone grafting and instrumentation. No matter what kind of surgical approach we adopt, the main purpose of the surgery remains unified, including radical debridement, stabilization of the spine, nerve decompression, and deformity correction. Numerous studies have been done to evaluate the clinical outcomes of different surgical approaches; however, the literature on posterior approach combined with OD is rare. In this cohort study, we found that posterior OD surgery, compared with AP approach, can achieve a more rapid recovery with high safety and less treatment cost.
With the evidence suggesting that TB lesions almost always affect the anterior and middle column, the anterior-only approach was once widely considered as the “gold standard” as it could provide direct access to the TB foci, allowing for radical debridement and effective decompression. 12 Pu et al 13 used anterior approach combined with debridement, interbody autografting and instrumentation for 22 patients, and all patients exhibited bone fusion and achieved neurological improvement. Lü et al 14 treated 50 patients with thoracic spinal TB by anterior debridement and reconstruction via a thoracoscopy-assisted mini-open approach, and 92% of the patients obtained a good or excellent subjective patient-reported outcome, and no recurrence was observed. Although satisfactory debridement can be achieved by anterior approach, some studies reported that the anterior bone grafting and instrumentation cannot provide spine with sufficient stability and may lead to great loss of correction in a long run.15,16 Kim et al 17 analyzed the data of 140 spinal TB patients who underwent anterior surgery, and reported a 51.0% initial kyphosis correction, but the rate of correction dropped to 7.5% 2 years later. A more recent study of Zeng et al 7 also showed an obviously smaller correction angle and a larger correction loss in anterior approach compared with posterior-only and AP approaches. Taking into account the disadvantages of anterior approach, additional posterior instrumentation that can effectively enhance spinal stability and prevent correction loss and graft failure was suggested by many surgeons.4,5,18,19 Furthermore, it has been demonstrated in several previous studies that the strong three-column fixation by pedicle screws not only helps to relieve back pain but also promotes neurological recovery.20,21 As a result, the AP surgery, described as 360° reconstruction of the vertebra and considered as a mature surgical method, has been widely used in the treatment of spinal TB in recent years. In the present study, pedicle screw fixation and TMCs were applied to all patients, and 2 groups got similar kyphosis correction as well as the correction loss during the follow-up, which is consistent with the results described by Zeng et al. 7 However, the AP approach does not avoid the extra complications related to exposure from an anterior approach such as vascular and visceral injury, hemothorax, pleural effusion and so on.22-24 Additionally, during the operation, surgeons have to reposition the patients, which may increase the duration of surgery and the risks of anesthesia and wound infection. Zhang et al 25 performed posterior-only surgery to 20 patients and AP surgery to 16 patients in treating thoracic spinal TB and reported a significantly higher operative complication rate of AP approach compared with posterior-only approach (75% vs 15%). Wang et al compared 3 approaches for treating spinal TB in adults and showed a 40.0% complication rate of AP approach, which was the highest among the 3. Likewise, in this study, the AP approach showed a significantly higher total complication rate than the posterior approach (35.5% [27/76] vs 9.8% [10/102]). Furthermore, ten major complications occurred in patients treated with AP surgery and seven of them were related to anterior procedures. Although most pleural effusion and pneumothorax can be well addressed by postoperative drainage, increased hospitalization time and cost is still a concern. Given all of the results discussed above, the AP approach may not be the optimal method due to the relatively high surgical risk.
For less complications and surgical invasiveness, many surgeons performed one-stage posterior surgeries with CD, bone fusion, and instrumentation for thoracolumbar spinal TB and achieved acceptable outcomes.9,18,26,27 Debridement, the most important procedure of the surgery, is mainly about clearing necrotic tissues, sequestrum, abscess, sclerotic walls, and eliminating dead spaces. Radical debridement can not only accelerate the graft fusion, but also promote the patient’s response to chemotherapy after surgery, which may decrease the duration of postoperative chemotherapy. 28 Nevertheless, the procedure of debridement in traditional posterior approach is generally conducted merely by scraping using curettes, which may be unable to achieve complete focus clearance, thus leading to a higher TB recurrence rate than AP approach.7,10,21 Besides, the CD procedure always leaves an irregular cavity, which makes it difficult to insert cages and achieve optimal reconstruction of the anterior column. In this study, no recurrence was observed in either group. On the 1 hand, it revealed a good effectiveness of anterior debridement in AP approach, which is consistent with previous studies. On the other hand, for posterior-only approach, we mainly ascribed the zero recurrence and shorter fusion time to the OD technique, because osteotomy can resect the whole pathological entity and create 100% healthy bone surfaces, which provides a favorable micro-environment for bone fusion. Notably, in this study although patients treated with OD surgery showed statistically lower ODI and VAS at 3 months after surgery, the difference values did not reach minimally clinically important difference, indicating that the posterior OD may not provide a substantial advantage of early postoperative recovery. Additionally, at final follow-up no significant statistical difference in patient-reported outcomes were observed between the 2 groups, and the 2 groups of patients showed similar long-term pain relief and function improvement. Although the AP approach showed as good outcomes as posterior approach with respect to the recurrence rate and kyphosis correction, it had a longer operation time, more blood loss, a longer LOS, and a higher overall cost than posterior OD approach.
OD, a modified surgical procedure for the treatment of spinal TB, has been increasingly widely used in recent years. A recent study conducted by Ma et al 10 compared the efficiency of posterior CD with posterior OD in treating thoracolumbar TB and enumerated the advantages of OD surgery, including less blood loss, shorter fusion time, and lower recurrence rate. From our experience, several key points about OD should be emphasized. Firstly, the range of osteotomy must cover the whole TB lesion and make sure the osteotomy planes are parallel to the adjacent endplates of the vertebrae, which makes it easier to insert TMCs into an ideal position. Secondly, it should be noted that the cage insertion in lumbar spine sometimes is extremely difficult due to the narrow space above or below the obliquely oriented nerve roots. Hence the nerve roots at infected levels should be adequately freed before cage insertion. Furthermore, it is easier to insert a TMC transversely into the intervertebral space and then turn the TMC in suit along the longitudinal axis of the spine to an ideal position in sagittal and coronal planes. Thirdly, since the larger TMC’s contact surface with endplates provides stronger support and better bone fusion, we recommend inserting 2 parallel TMCs, if intervertebral space permits. Beyond that, 2 TMCs with a smaller diameter can be manipulated more easily than using 1 TMC with big diameter in the insertion procedure. Finally, because osteotomy will inevitably sacrifice an extra part of healthy bone and leave a large intervertebral space, sufficient bone grafting around the cages is also required for the healing.
Limitations
There are several limitations in this study. Firstly, this study is a retrospective rather than a prospective study, which may undermine the evidence level. Secondly, all the operations in this study were not performed by the same surgeon, thus leading to inevitable bias regarding the clinical outcomes such as blood loss and operation time due to the different surgeons’ experience and skill. Thirdly, we did not set subgroups according to diseased regions or the number of diseased segments, which may result in a certain degree of bias, and further studies are needed to address this issue.
Conclusion
Posterior OD, fusion with TMCs, and instrumentation for the treatment of active thoracolumbar TB is safe and effective, and can achieve better clinical outcomes than AP approach. The posterior approach with OD is a better surgical strategy for the treatment of active thoracolumbar TB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (No. 81860473), Key project of Natural Science Foundation of Jiangxi Provincial (No. 20202ACB206004), Major Discipline Academic and Technical Leaders Training Program of Jiangxi Province (No. 20204BCJ22026), and the Program of Health Commission of Jiangxi Province (No.20191029).
Ethics Approval
This study was approved by Institutional Review Board of the First Affiliated Hospital of Nanchang University.