
Abstract
Study Design:
Retrospective study of a prospectively collected database.
Objective:
To investigate the rate and risk factors for 30-day readmissions and reoperations after 3-column osteotomy (3CO).
Methods:
The American College of Surgeons National Surgical Quality Improvement Program database (2012-2014) was reviewed. Inclusion criteria were adult patients who underwent 3CO. The rate of 30-day readmission/reoperation was examined, and the association between patient/operative characteristics and outcome was investigated via multivariate analysis.
Results:
There were 299 patients who underwent a 3CO for spinal deformity. The rate of 30-day readmission and reoperation was 11.0% and 8.4%, respectively; 7.7% of readmissions were related to the primary procedure and 3.3% were unrelated. The most common unique cause for readmission was wound infection in 27.2% of cases. Among reoperations, the most common unique indications were wound infection (20.0%) and implant-related complications (20.0%). On multivariate analysis, obesity (odds ratio [OR] = 2.96; 95% CI = 1.06-8.25; P = .038), chronic obstructive pulmonary disease (OR = 20.8; 95% CI = 3.49-123.5; P = .001), and fusion of 13 or more spinal levels were independent predictors of readmission (OR = 4.86; 95% CI = 1.21-19.5; P = .025). On the other hand, independent predictors of reoperation included chronic obstructive pulmonary disease (OR = 6.33; 95% CI = 1.16-34.5; P = .033) and chronic steroid use (OR = 6.69; 95% CI = 1.61-27.7; P = .009).
Conclusion:
Wound complications and short-term implant-related complications are important causes of readmission and/or reoperation after 3CO. Preoperative factors such as obesity, chronic lung disease, chronic steroid use, and long-segment fusion procedures may significantly increase the risk of 30-day morbidity following high-grade osteotomies.
Introduction
Three-column osteotomy (3CO) for complex spinal deformity is a technique that involves bony resection of the anterior, middle, and posterior columns of the spine with associated reconstruction in an effort to restore spinal alignment. These techniques mainly include pedicle subtraction osteotomy (PSO) and vertebral column resection (VCR) and are also known as Grade 4-6 osteotomies on the Schwab classification. 1 Common indications include severe adult spinal deformity, postinfectious kyphoscoliosis such as Pott’s disease, iatrogenic fixed sagittal imbalance, flat back syndrome, and others. 2 –4 In recent years, the rate of utilization of 3CO has significantly increased, with Gum et al reporting a 3.2-fold increase in the use of PSO between 2008 and 2011 alone. 5
Given the complexity of these procedures, complication rates have been reported to be as high as 59%. 6 In a report by the Scoliosis Research Society, authors found a considerably increased risk of complications for patients who underwent osteotomy compared with patients who did not, with a particularly higher rate of neurological complications (2.5% vs 1.6%, P = .060). 7 Auerbach et al reported an overall complication rate of 35%—38% for PCO and 22% for VCR—though differences were not found to be significantly different (P = .280). 8 Although multiple studies have focused on perioperative complication rates after 3CO, there is a paucity of literature on overall 30-day readmissions and reoperations, whether this was related or unrelated to the spine surgery itself. Thus, the purpose of this study was to report the 30-day readmission and reoperation rate after 3CO for complex spinal deformity using a large multicenter prospective database and identify risk factors for these occurrences.
Methods
Study Design and Data Source
This is a multicenter study using prospectively collected data for patients who underwent 3CO for spinal deformity between 2012 and 2014; it was deemed exempt from review by the local institutional review board (2016-6862). Data was gathered from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database, which is a risk-adjusted database that captures data from more than 500 hospitals in the United States. Patients are randomly selected to participate in the database, and a trained “Surgical Clinical Reviewer” at each participating hospital prospectively collects patient and operative data throughout 30 days. Follow-up is conducted via clinical visits, telephone calls, and/or mail. Currently, this database collects more than 150 preoperative, intraoperative, and postoperative unique variables; primary and secondary procedures are captured in the form of Current Procedural Terminology (CPT) codes and diagnoses are captured in the form of International Classification of Diseases, 9th Revision (ICD-9) codes (www.facs.org/quality-programs/acs-nsqip).
Adult patients (>18 years of age) who underwent 3CO (PSO or VCR) were identified via use of CPT codes 22 206 or 22 207 for thoracic and lumbar osteotomy, respectively. Multilevel 3CO was identified via use of code 22 208. Primary diagnoses were identified via use of ICD-9 codes.
Collected Variables and Outcome Measures
Reviewed preoperative data included patient age at surgery, sex, body mass index (BMI), baseline comorbidities (diabetes, hypertension, chronic obstructive pulmonary disease [COPD], smoking, chronic steroid use), and functional status (defined as “dependent” if a person requires some or full assistance from another person for activities of daily living). Operative data included revision status, thoracic versus lumbar 3CO, single versus multilevel 3CO, number of levels fused, and operative time.
The main outcome measures examined were readmissions and reoperations occurring within 30 postoperative days. Readmission were further subcategorized into readmissions related to the principal procedure and readmissions unrelated to the primary procedure.
Secondary outcomes included development of at least one major perioperative complication. These included 30-day mortality, reintubation, stroke, pulmonary embolism, cardiac arrest, myocardial infarction, renal failure, sepsis, septic shock, prolonged ventilation, deep wound infection, and organ space infection.
Statistical Analysis
Descriptive statistics were used to describe the study sample. Univariate analyses were performed to examine the relationship between patient/operative parameters and the 2 outcomes of interest by using t tests or χ2 tests for data comparison. A multivariate logistical regression analysis was performed, adjusting for patient age, comorbidities, 3CO location (thoracic vs lumbar), multilevel 3CO, number of levels fused, revision procedures, and operative time. Statistical significance was defined as a P value less than .05. All analyses were performed in Stata SE 12 (StataCorp, College Station, Texas).
Results
Demographics of the Study Sample
Two-hundred and ninety-nine patients who underwent 3CO between 2012 and 2014 were identified from the NSQIP database, and general demographics are summarized in Table 1. The mean age at surgery was 61 ± 14 years; 63.9% of patients were female and 36.1% were male. Average BMI was 29.0 kg/m2, and 40.1% of the study population was defined as obese. The 3 most common comorbidities were hypertension (58.9%), smoking (17.7%), and diabetes (11.4%). Revision procedures were performed in 26.4% of cases, thoracic 3CO in 27.1%, lumbar 3CO in 72.9%, and multilevel 3CO in 14.7%. Almost half of the patients (47.7%) underwent fusion of 7 to 12 vertebral segments, and the mean operative time was 6.6 hours.
Characteristics of 299 Patients Who Underwent 3-Column Osteotomy for Spinal Deformity.
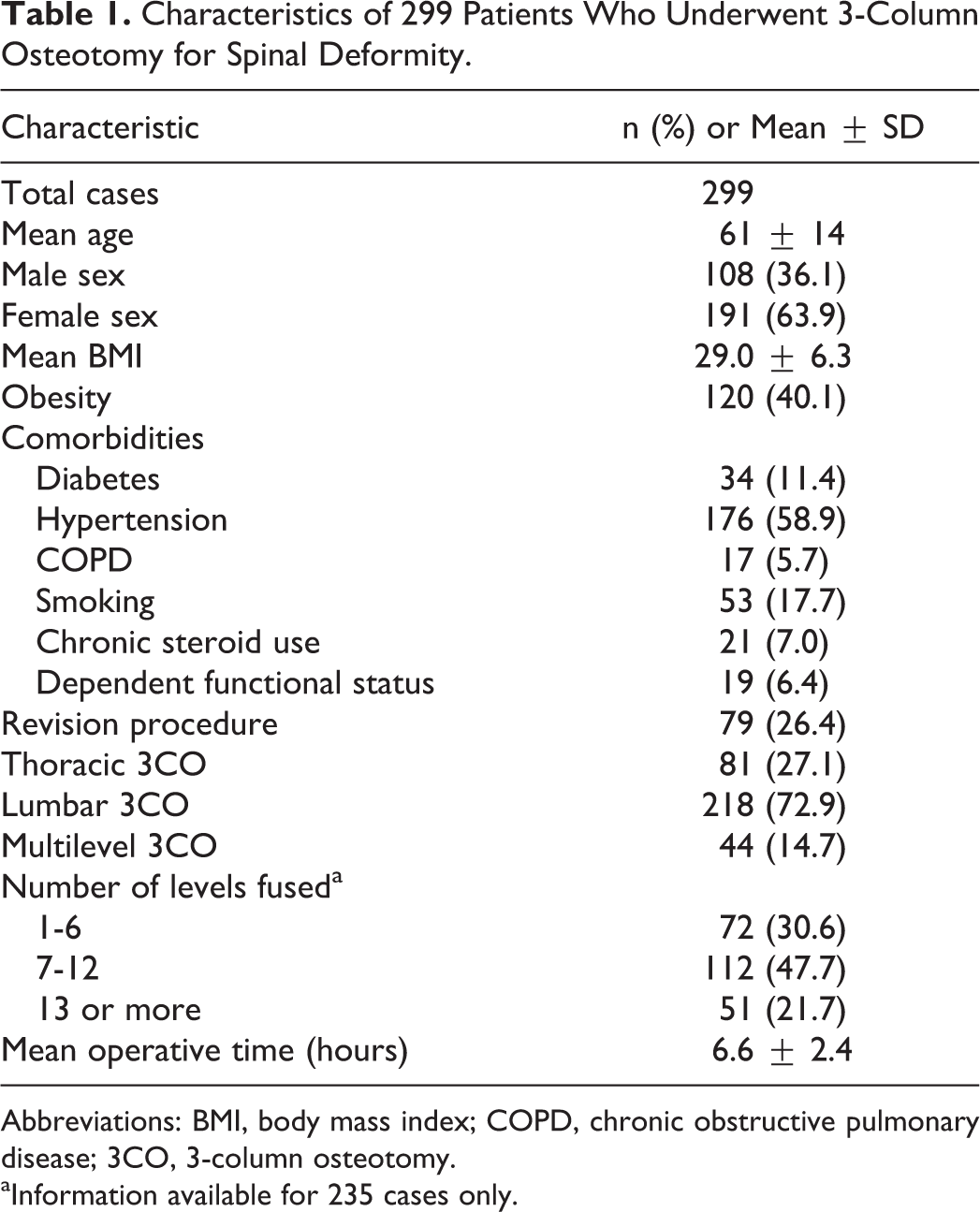
Abbreviations: BMI, body mass index; COPD, chronic obstructive pulmonary disease; 3CO, 3-column osteotomy.
aInformation available for 235 cases only.
The most common etiology of deformity was acquired deformity (degenerative/idiopathic) in 71.6% of patients, followed by iatrogenic deformity (postlaminectomy kyphosis or deformity secondary to instrumentation failure) in 13.4% of cases (Figure 1). Other less common causes included other diagnoses (7.0%), postfracture (5.0%), congenital (2.3%), and postinfection (0.7%).
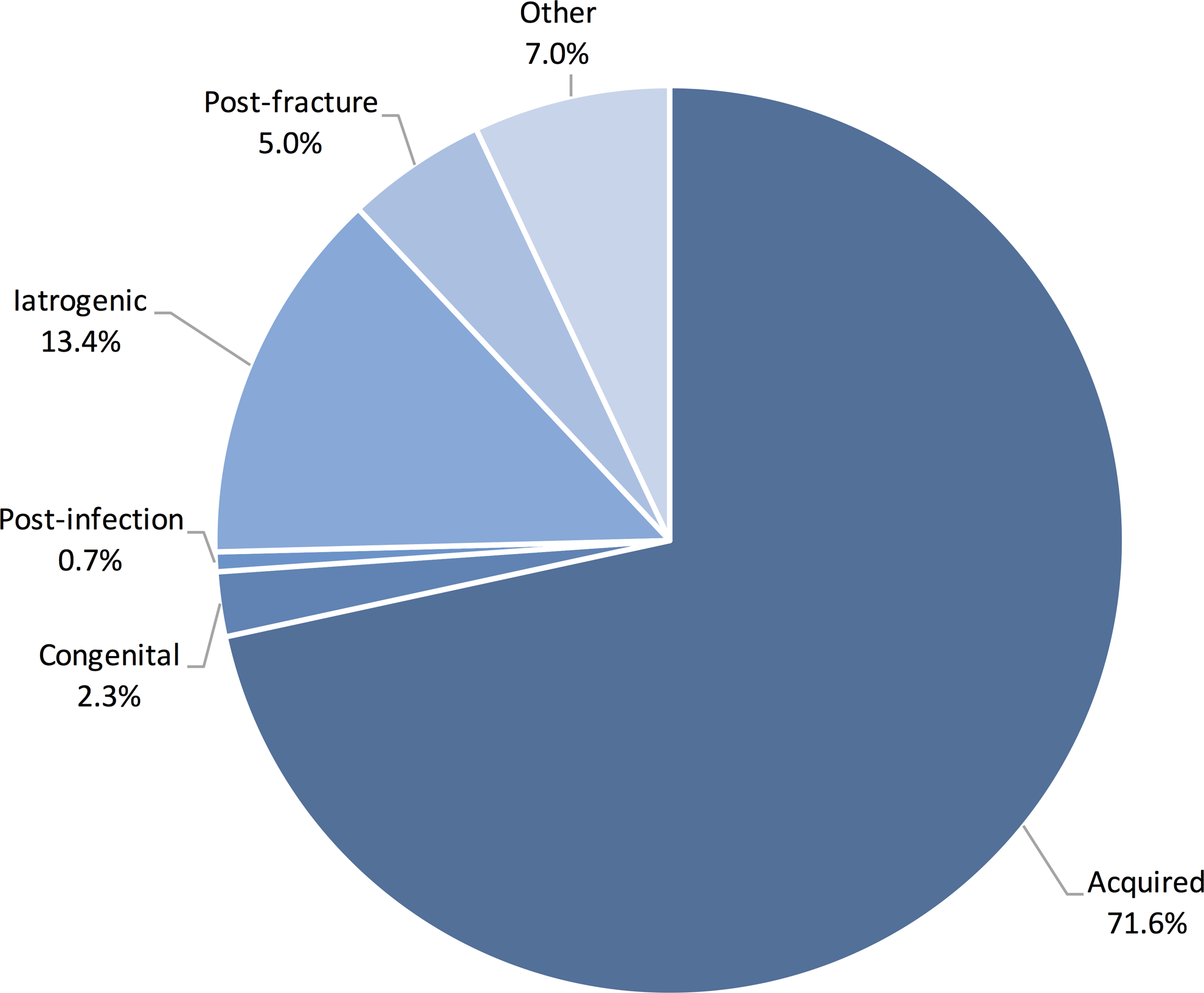
Etiologies of spinal deformity in 299 patients who underwent 3-column osteotomy. Acquired deformities include degenerative or idiopathic kyphoscoliosis. Iatrogenic deformities include postlaminectomy kyphosis and deformity secondary to instrumentation failure. Other causes include ankylosing spondylitis, juvenile osteochondrosis, and other/unknown causes.
The proportion of patients who developed at least one perioperative complication was 12%. In descending order of frequency, these included sepsis (5.4%), deep wound infection (2.7%), prolonged ventilation (2.3%), organ space infection (1.7%), reintubation (1.7%), cardiac arrest (1.7%), mortality within 30 days (1.7%), stroke (1.0%), pulmonary embolism (1.0%), myocardial infarction (0.7%), septic shock (0.7%), and renal failure (0.3%).
Based on number of comorbidities, complication rates were 15.0% for patients with 0 comorbidities, 7.2% for patients with 1 comorbidity, 12.7% for patients with 2 comorbidities, and 35.3% for patients with 3 or more comorbidities (P = .006).
Thirty-Day Readmissions
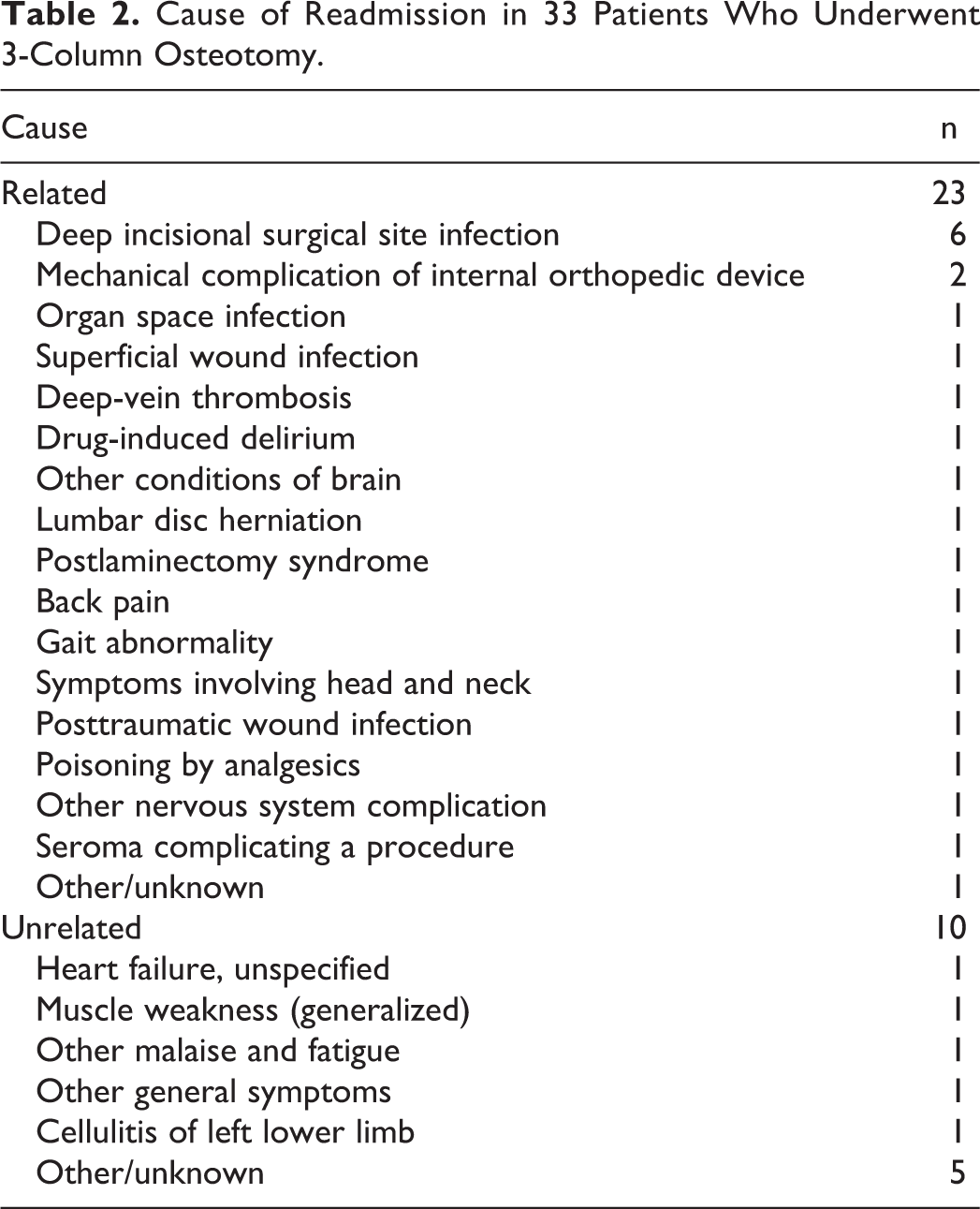
There were 33 patients (11.0%) who experienced a readmission within 30 days after 3CO (Table 2). The average day to readmission was postoperative day 18 ± 8 (range = 5-29). Readmissions were classified as related to the principal procedure in 23/33 cases (69.7% of all readmissions; 7.7% of all patients) and as unrelated in the remaining 10/33 patients (30.3% of all readmissions; 3.3% of all patients). Overall, the most common unique causes were wound infection (27.2% of cases; 6 deep wound infections, 1 superficial, 1 organ space, and 1 unclassified posttraumatic wound infection). Readmission rates were 7.5%, 10.1%, 11.1%, and 35.3% for patients with 0, 1, 2, and ≥3 comorbidities.
Cause of Readmission in 33 Patients Who Underwent 3-Column Osteotomy.
Thirty-Day Reoperations
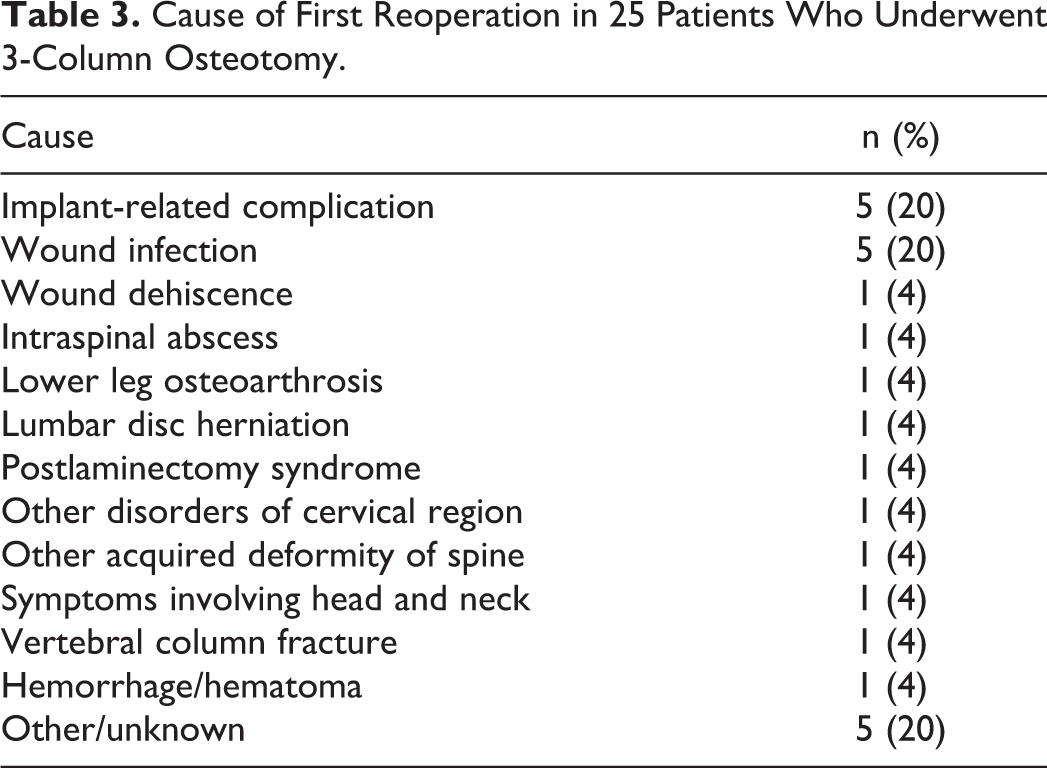
There were 25 patients (8.4%) who experienced at least one reoperation within 30 days (Table 3). The average day to reoperation was postoperative day 14 ± 10 (range = 2-30). The most common indication for reoperation was implant-related complication (20.0%), followed by wound infection (20.0%). Other indications included wound dehiscence, intraspinal abscess, unrelated lower leg osteoarthrosis, lumbar disc herniation, postlaminectomy syndrome, disorders of cervical region, deformity of spine, symptoms involving head/neck, vertebral column fracture, hemorrhage/hematoma, and others. There were an additional 5 patients who underwent a second reoperation, done for unspecified infection, wound infection, lumbar disc herniation, deep vein thrombosis, and other/unknown in one case each. Reoperation rates were 11.3%, 6.5%, 4.8%, and 23.5% for patients with 0, 1, 2, and ≥3 comorbidities, respectively.
Cause of First Reoperation in 25 Patients Who Underwent 3-Column Osteotomy.
Risk Factors for Readmission or Reoperation
On univariate analysis, factors that were significantly associated with readmission and reoperation are summarized in Tables 4 and 5, respectively. The percentage of obese patients was significantly higher in the readmission group (60.6% vs 37.6%, P = .011), as well as the percentage of patients with a history of chronic obstructive pulmonary disease (18.2% vs 4.1%, P = .001). In the reoperation group, a significantly higher proportion of patients also had a history of chronic obstructive pulmonary disease (16.0% vs 4.7%, P = .020) and chronic steroid use (20.0% vs 5.8%, P = .008).
Comparison of Demographic and Surgical Data Based on Readmissiona.
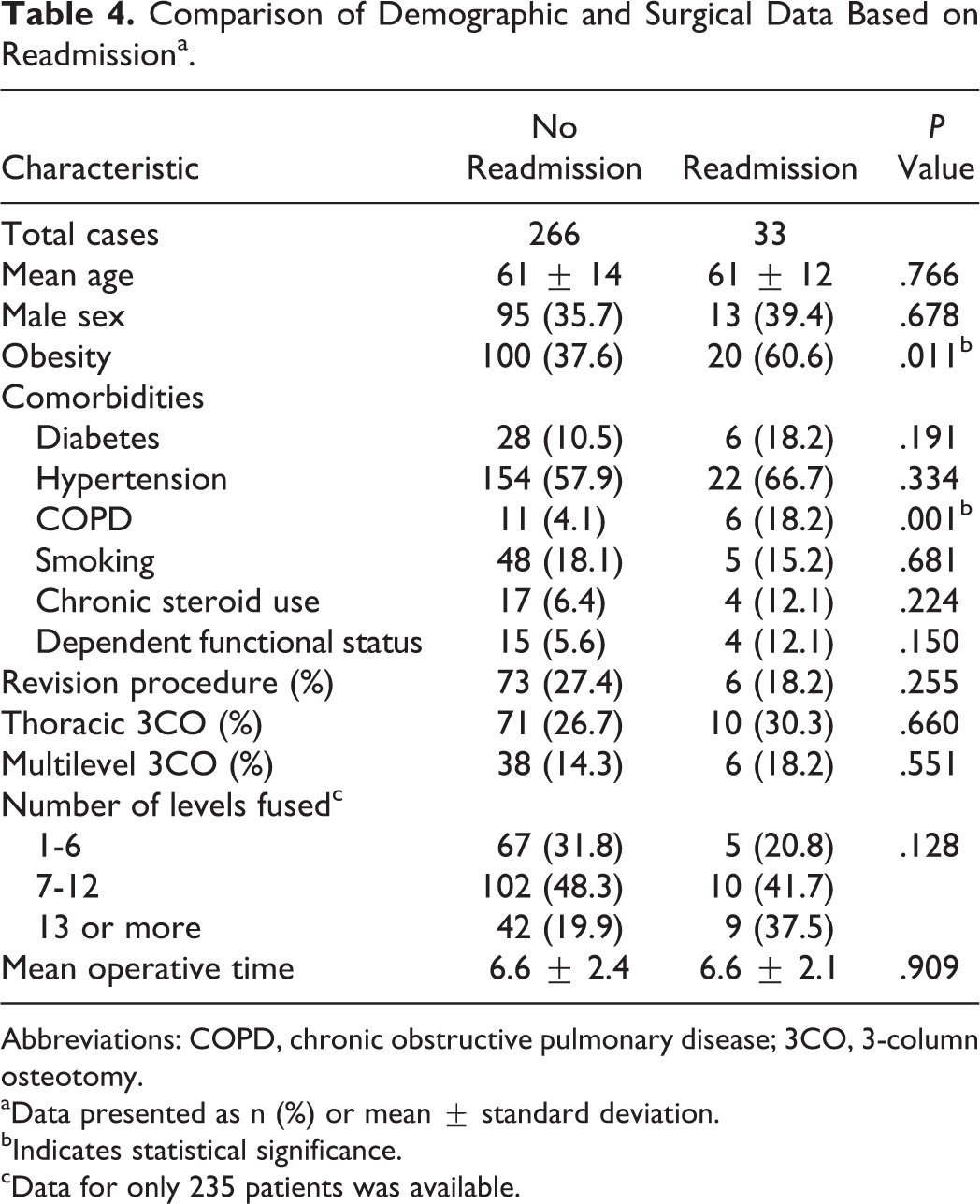
Abbreviations: COPD, chronic obstructive pulmonary disease; 3CO, 3-column osteotomy.
aData presented as n (%) or mean ± standard deviation.
bIndicates statistical significance.
cData for only 235 patients was available.
Comparison of Demographic and Surgical Data Based on Reoperationa.
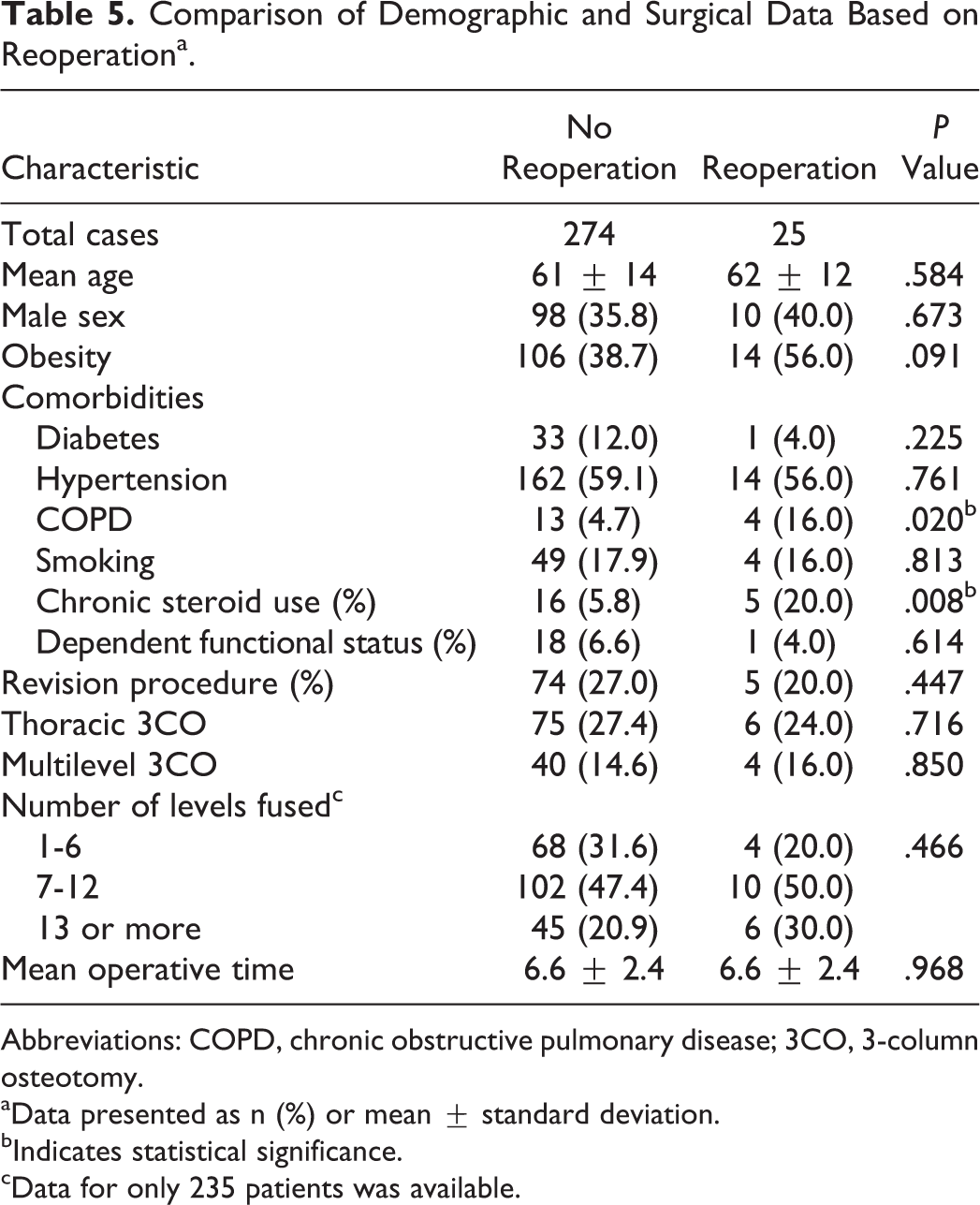
Abbreviations: COPD, chronic obstructive pulmonary disease; 3CO, 3-column osteotomy.
aData presented as n (%) or mean ± standard deviation.
bIndicates statistical significance.
cData for only 235 patients was available.
On multivariate analysis, after controlling for patient age, comorbidities, 3CO location (thoracic vs lumbar), multilevel 3CO, number of levels fused, revision procedures, and operative time, obesity (OR = 2.96; 95% CI = 1.06-8.25; P = .038), COPD (OR = 20.8; 95% CI = 3.49-123.5; P = .001), and fusion of 13 or more spinal levels were independent predictors of readmission (OR = 4.86; 95% CI = 1.21-19.5; P = .025). On the other hand, independent predictors of reoperation included COPD (OR = 6.33; 95% CI = 1.16-34.5; P = .033) and chronic steroid use (OR = 6.69; 95% CI = 1.61-27.7; P = .009).
Discussion
Spinal deformity, especially in adults, is an increasing public health concern due to an aging population, increase in the use of spinal fusion techniques, and overall expectancy of high quality of life. 9,10 In cases of severe sagittal or coronal imbalance due to fixed deformities, spinal osteotomies allow for lengthening/shortening of the spinal column and thus correction. Three-column osteotomies involve the highest degree of bony resection, but also allow for the highest degree of correction (approximately 30° to 40° per level). 11 These techniques, including PSO and VCR, are powerful surgical tools, but not without risks of major perioperative complications. 9,12 In this study, we sought to examine the rates of 30-day readmission and reoperation after 3CO, finding rates of 11.0%, and 8.4%, respectively.
Manoharan et al reported a 7.5% (56/747) rate of 30-day readmission after surgery for adult spinal deformity, with the most common indications being infection (n = 11), bleeding or seroma (n = 5), pain (n = 3), implant-related complications (n = 2), thromboembolic (n = 2), neurologic (n = 2), other medical (n = 2), and other/unknown (n = 30). 13 However, no data on readmissions for 3CO procedures was reported, so results may not be directly comparable to the present study. Despite this, the readmission rate in our study was also relatively similar at 11.0%, with the most common indication also being wound infection (27.2% of all 30-day readmissions). Thus, these findings suggest that surgical site infection remains an important cause of postoperative morbidity, and efforts in prevention of these occurrences should continue.
In terms of 30-day reoperation, Bianco et al reported a 19.4% reoperation rate at up to 6 months after 3CO, but unfortunately no data was presented on the exact indications for reoperation. 9 On the other hand, Scheer et al reported a 5% 30-day reoperation rate after adult spinal deformity surgery (with and without 3CO), with the most common indications being neurological compromise (n = 4), instrumentation failure (n = 3), infection (n = 3), and others (n = 7). 14 However, the 1-year reoperation rate after 3CO was 19% (10/53 patients); causes included instrumentation failure (n = 4), neurological compromise (n = 3), radiographic (n = 2), and other surgical (n = 1). The 30-day reoperation rate after 3CO was 5.7%, 14 a relatively similar to the reported rate of 8.4% in the present study. In another study, Hassanzadeh et al found a revision surgery rate of 12% (6/51) after examining 51 patients 60 years or older who underwent 3CO. 4 One patient required decompression due to worsening left lower extremity weakness, 4 patients developed wound infections requiring irrigation and debridement, and 1 patient developed an epidural hematoma requiring emergency decompression. 4
A larger study by Maier et al examined revision surgery after 3CO in 335 patients at 8 different surgical centers: 12.3% at 3 months and 17.6% at 1 year after primary surgery. 15 Patients who underwent revision surgery had similar baseline characteristics to patients who did not require reoperation, but revision was higher in patients who underwent multilevel 3CO versus single-level 3CO (41.7% vs 15.8%, P = .001). Causes for reoperation within the first year included mechanical (4.5% instrumentation failure, 3% pseudoarthrosis, 3.9% proximal junctional kyphosis, and 2.1% sagittal imbalance), nonmechanical (2.1% due to neurological deficit, 2.1% due to wound infection, 0.9% due to painful instrumentation, and 0.9% due to progressive stenosis), and 2.6% for unknown causes. 15 However, one of the most interesting findings of Maier et al’s study was that there was significant variation in the rates of revision surgery by surgical center—6.3% to 31.9%. 15 Nonetheless, some of the most common causes for reoperation were mechanical (including instrumentation failure) and wound infection, similar to the findings of our present investigation.
Obese patients, patients with a history of chronic lung disease, and patients who underwent instrumentation of ≥13 spinal segments were found to be at an increased risk for readmission. Obesity is becoming a worldwide epidemic, and multiple investigations have shown significantly worse outcomes for obese patients undergoing spine surgery. 13,16 –18 Soroceanu et al examined 241 patients who underwent surgery for adult spinal deformity, finding that obese patients had a higher incidence of major complications, wound complications, and less improvement in the Oswestry Disability Index compared with nonobese patients. 17 Nevertheless, although obesity was found to predict readmission, it was not found to be associated with reoperation. Similar to our findings, Maier et al found that obesity was not a risk factor for revision surgery after 3CO, 15 and future research is encouraged to better define the impact of body mass index on short- and long-term outcome after 3CO.
On the other hand, vertebral deformities have been found to be more common in patients with chronic lung disease than in patients without, attributed to a loss in bone mineral density. 19 Similarly, lung disease has found to be an important risk factor for postoperative complications after deformity surgery. 20,21 Last, fusion of 13 or more spinal levels was found to predict 30-day readmission. Long-segment fusion procedures are inherently associated with longer operative times, higher blood loss, and prolonged length of stay, which all contribute to a higher 30-day morbidity. 22 –24 In a study of 1250 patients who underwent spinal fusion for deformity, there was a significant increase in the odds of complication occurrence with increasing number of levels fused. 25 Compared with fusion of <6 levels, fusion of 7 to 12 segments increased the risk by 1.7, whereas fusion of 13 or more levels increased the odds by a factor of 1.9. 25
For reoperation, lung disease and chronic steroid use were found to be significant risk factors. As mentioned above, pulmonary disease is known to decrease bone mineral density, whereas steroids are known to also decrease density and also impair wound healing. 26,27 Thus, this may explain why reoperation rates were significantly higher in our study, given that the most common indications for revision surgery within 30 days were also implant-related complications and wound infection.
In an era of increasing pressure to reduce health care costs, 30-day readmissions and reoperations are important markers for health care quality. As such, the Hospital Readmission Reduction Program, a part of the Affordable Care Act, is known to reduce reimbursements for facilities with considerably high readmission rates. For this reason, efforts in reduction of these occurrences are needed, given the relatively high rate of readmission (11.0%) and reoperation (8.4%) found in this investigation. Nonetheless, future prospective studies of nationally representative data are needed not only to better understand the causes for readmission and reoperation but also to examine potential measures to decrease these events.
Limitations
Although the NSQIP database allows for analysis of large sample of patients, the database design is not nationally representative. Use of CPT or ICD-9 codes for identification of spinal deformity patients carries risk of miscoding or reporting bias, and the fact that NSQIP is not a database tailored for spine surgery patients is also a limitation. For example, no further distinction between VCR and PSO can be made, given that they are broadly categorized as 3CO per CPT coding. Although both are categorized as high-grade osteotomies, PSO is traditionally used for correction in the sagittal plane (although asymmetric PSO may also be performed) whereas VCR can be used for correction in sagittal, axial, or coronal planes. Auerbach et al reported a higher rate of complications for PSO than VCR (even though VCR involves more bony resection), though the difference did not reach statistical significance. 8 Authors attributed differences in complication rates to patient characteristics (patients who underwent PSO were older, more likely to have previous surgery, and with higher BMI), and encouraged further research to identify whether differences in complication were patient or technique-related. 8
Another limitation of our study is that data such as radiographic parameters, preoperative symptoms, and long-term outcomes are not available, so no information on the long-term effects of readmission or reoperation is available. Nevertheless, in spite of these limitations, NSQIP allows for analysis of prospectively collected data from multiple centers and different surgeons.
Conclusion
Three-column osteotomy for spinal deformity correction is a technically demanding procedure with an important risk for perioperative morbidity. In this study, the 30-day readmission and reoperation rates were 11.0% and 8.4%, respectively. Obese patients, patients with a history of chronic lung disease, patients with chronic steroid use, and patients undergoing instrumentation of ≥13 levels may be at a higher risk for these events. Future research into preoperative optimization of these patients is encouraged.
Footnotes
Authors’ Note
The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have been not verified and we are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors. Portions of this work were presented at the 2017 Global Spine Congress in Milan, Italy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.