
Abstract
Study design
Systematic review.
Objective
En bloc resection is a major, invasive surgical procedure designed to completely resect a vertebral tumor with a sufficient margin. It is technically demanding and potentially poses risks of perioperative complications. In this systematic review, we investigated the incidence of complications after en bloc resection for spinal tumors.
Methods
We screened PubMed and Embase databases for relevant English publications, from 1980 to 2020, using the following terms: spine OR spinal AND en bloc AND tumor. Using a standard PRISMA template, after the initial screening, full-text articles of interest were evaluated.
Results
Thirty-six studies with 961 patients were included. The overall mean age of patients was 49.6 years, and the mean follow-up time was 33.5 months. There were 560 complications, and an overall complication rate of 58.3% (560/961). The 5 most frequent complications were neurological damage (12.7%), hardware failure (12.1%), dural tear and cerebrospinal fluid leakage (10.6%), wound-related complications (7.6%) and vascular injury and bleeding (7.3%). The complication-related revision rate was 10.7% (103/961). The average incidence of complication-related death was 1.2% (12/961).
Conclusions
En bloc resection is a surgical procedure that is very invasive and technically challenging, and the possible risks of perioperative complications should not be neglected. The overall complication rate is high. However, complication-related death was rare. The advantages of surgery should be weighed against the serious perioperative morbidity associated with this technique.
Background
In spine tumor surgery, obtaining adequate resection margins is crucial. En bloc resection is a surgical procedure aimed at achieving complete resection with a sufficient margin around it. The treatment is indicated for primary malignant, aggressive benign, and solitary metastatic tumors. It has proven its efficacy in local disease control and overall survival improvement over the years.1–4
Studies have shown that it reduces the local recurrence and improves prognosis in patients with primary malignant and benign aggressive bone tumors.1,2 For spinal metastases, it is controversial, but may be indicated for selected patients with isolated disease, in whom cure is the goal.3,4
En bloc resection is a large invasive surgical procedure that is considered to be technically demanding owing to the proximity of neurovascular structures, visceral organs, need for a combined anterior and posterior approach, and increased blood loss, surgical time,5–7 even for experienced surgeons. It is important to be aware of the possible risks of perioperative complications, including adjacent structures injury, neurological injury, wound-related complication, medical morbidity associated with surgical trauma, and long-term hardware failure.6,7 Elaborate patient selection, meticulous surgical planning, interdisciplinary cooperation, targeted prevention, and effective management of complications are essential for good oncological prognosis and acceptable complication rates.
A majority of the existing literature describing outcomes after the procedure is based on small, retrospective case studies. There is little reliable evidence available to guide patients in their informed consent regarding complication incidence. In addition to improving patient counseling, understanding complication and mortality rates may help identify opportunities for perioperative quality improvement. To date, there has been no systematic review of these complications. Thus, here we systematically reviewed the current efforts to quantify the perioperative complications in patients who underwent en bloc resection for primary and metastatic spinal tumors.
Methods
Search Strategy
A systematic review was conducted following the PRISMA guidelines. The Embase and PubMed databases were used to search for relevant articles on en bloc resection of spinal tumors, using the following terms: spine OR spinal AND en bloc AND tumor.
The search results were limited to articles that were published between 1980 and 2020 in the English language which reported on and included complications rates of en bloc resection for primary and metastatic spinal tumors. In total, 2009 articles were identified.
Eligibility Criteria
The following criteria were used to select eligible studies: (1) those reported on and included complications rates of en bloc resection for primary and metastatic spinal tumors, (2) a retrospective study, prospective study, cohort study, (3) published between 1980 and 2020.
The exclusion criteria were: (1) non-English language, (2) studies without clear, quantitative data on complications, (3) studies with < 5 cases, (5) studies with a sample including sacral tumors, (6) studies with overlapping cohorts, and (7) reviews, letters, surgical techniques, cadaver studies, etc.
Study Selection
Results were exported into Mendeley software (https://www.mendeley.com). Following the removal of duplicates, 2 independent reviewers screened titles, abstracts, and full texts, obtaining full texts if either judged a study to be potentially eligible. The reviewers discussed discrepancies until a consensus was reached during the fulltext review. Consequently, 36 studies were included in analysis (Figure 1). Flowchart of literature selection.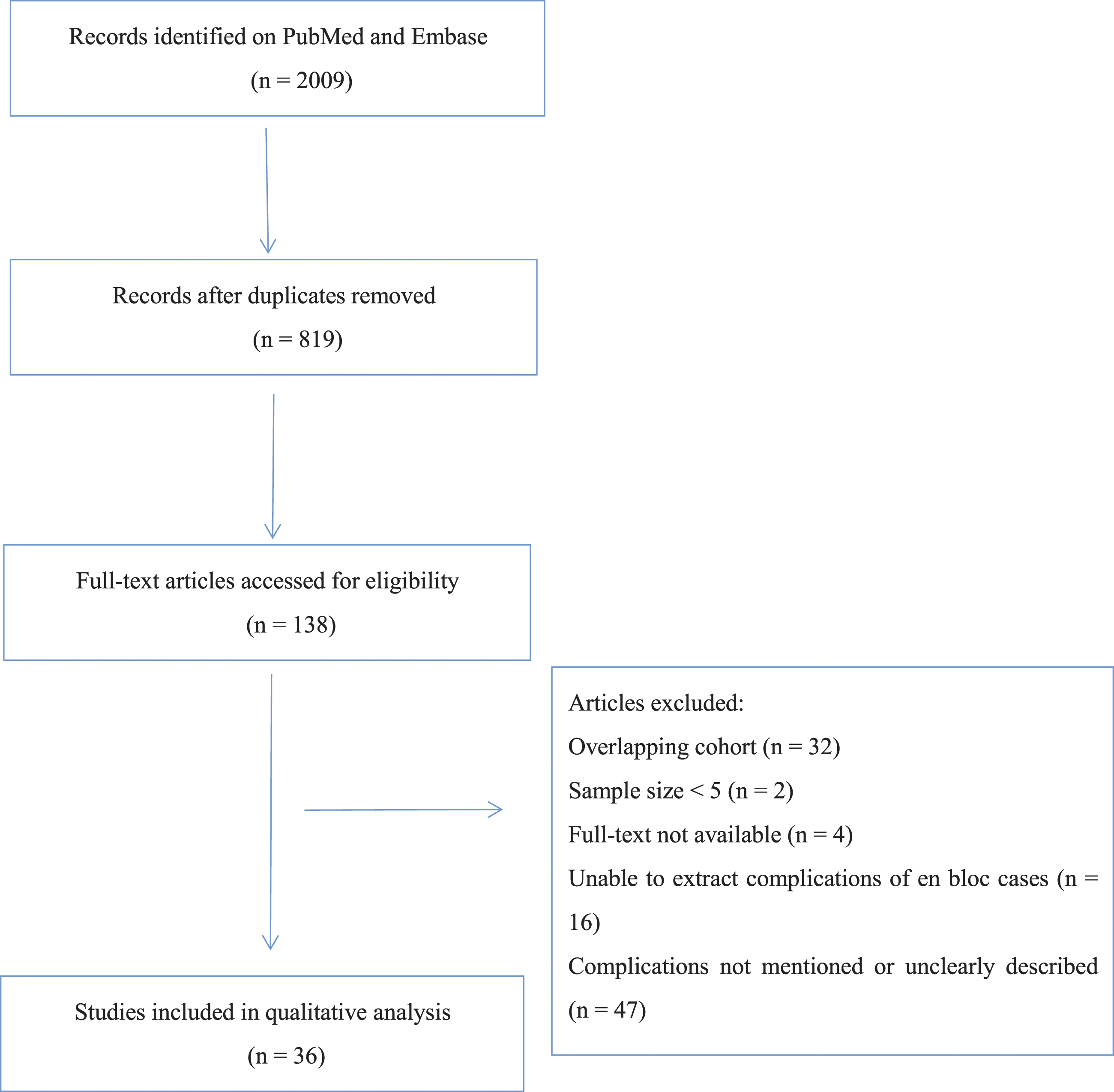
Data Extraction
Two reviewers (ZL, PZ) individually assessed the eligible articles and extracted data, including: first author, year of publication, data collection year, number of patients, study type (prospective or retrospective), tumor type (primary or metastases), complication details, complication-related deaths, and complication-related revisions. Disagreements were resolved by a third reviewer (WY).
Quality Assessment
The risk of bias of the included studies is analyzed using the Joanna Briggs Institute Critical Appraisal tools 8 for prevalence studies. The research quality was assessed using the classification system proposed by the Journal of Bone and Joint Surgery in 2003 9 and adopted by the North American Spine Society, which was widely used among orthopedic societies, 10 level of evidence is ranked from I to V, which Level I indicates the highest quality and Level V shows the lowest quality of evidence. Two independent reviewers (ZL, LG) evaluated the risk of bias and the level of evidence. Disagreements were resolved by a third reviewer (WY).
Complications
Complications were categorized as vascular injury and bleeding, hardware failure (including rod fracture, screw broken/loosened/back-out, symptomatic anterior reconstruction subsidence and displacement, etc.), adjacent structure injury, dural tear and cerebrospinal fluid (CSF) leakage, unplanned neurological damage (deterioration, cord injury, nerve root injury, symptomatic epidural hematoma), wound-related problems, hypercoagulable state (deep vein thrombosis, pulmonary embolism, and disseminated intravascular coagulation), medical morbidity (including cardiac, gastrointestinal, renal, and respiratory), and others. 7
Planned structure sacrifice based on the oncological objective of complete tumor en bloc resection was not considered as a complication. 7 Although accidental violation of the margin may lead to a poor prognosis, which is defined as a complication in some articles, we did not regard this as a complication in this article.
The incidence of an individual complications was calculated by dividing the total number of occurrences by the number of affected patients. The “number of affected patients” was calculated by totaling the patient populations of the studies that reported a particular complication. For studies that solely reported a particular complication or particular complications, this part of the sample was only included in the denominator when calculating the specific complication. So every denominator was uniquely altered for a specific complication. Complication data were collected and calculated using Excel Office.
Results
Study Characterstistics
Risk of bias assessed by the Joanna Briggs Institute (JBI) Critical Appraisal Tools for use in JBI Critical Appraisal Checklist for Prevalence Studies
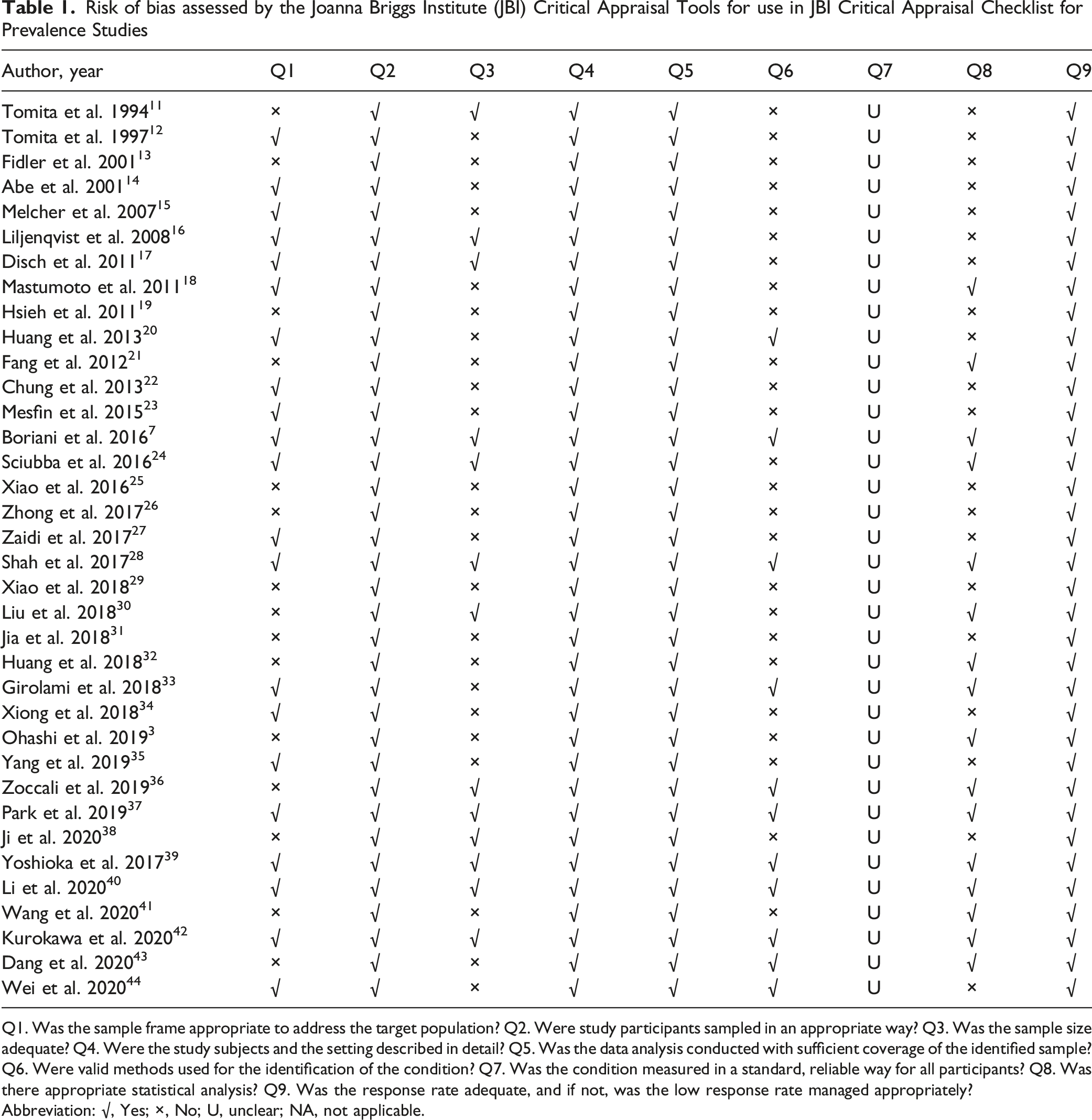
Q1. Was the sample frame appropriate to address the target population? Q2. Were study participants sampled in an appropriate way? Q3. Was the sample size adequate? Q4. Were the study subjects and the setting described in detail? Q5. Was the data analysis conducted with sufficient coverage of the identified sample? Q6. Were valid methods used for the identification of the condition? Q7. Was the condition measured in a standard, reliable way for all participants? Q8. Was there appropriate statistical analysis? Q9. Was the response rate adequate, and if not, was the low response rate managed appropriately?
Abbreviation: √, Yes; ×, No; U, unclear; NA, not applicable.
Overall Outcomes
Studies Reporting Complications Following en Bloc Resection for Spinal Tumor.
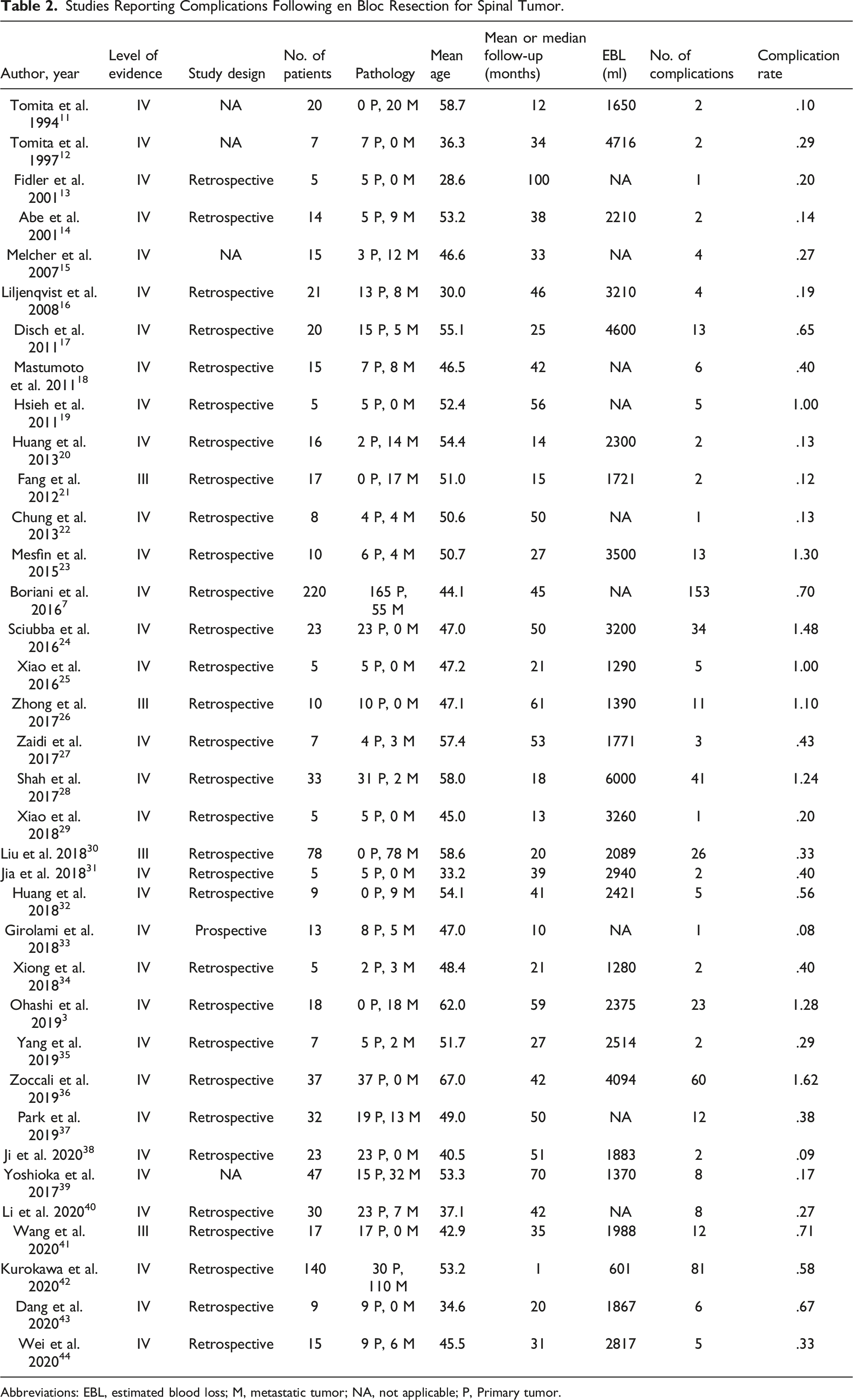
Abbreviations: EBL, estimated blood loss; M, metastatic tumor; NA, not applicable; P, Primary tumor.
Individual Complication Rates.
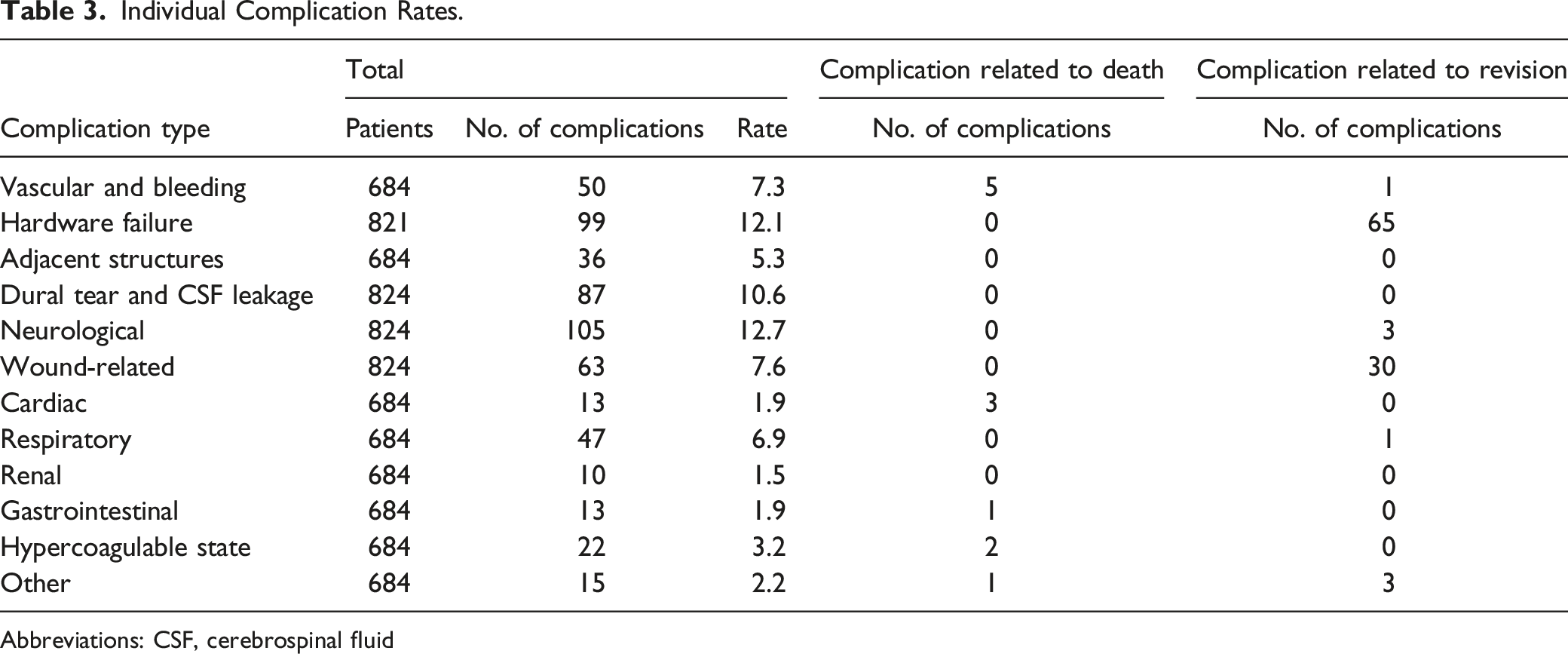
Abbreviations: CSF, cerebrospinal fluid
Perioperative Complications
Neurological Damage
In a retrospective study of prospectively collected data, involving 220 en bloc resections, Boriani et al. 7 reported 8.2% (18/220) with postoperative neurological deficits. Twelve cases were considered to be major complications.
In 2 studies on cervical spine en bloc resection by Xiao et al. 25 and Zhong et al, 26 the neurological complication rates were 60.0% and 50.0%, respectively. However, all complications were minor and did not substantially change the otherwise complete and anticipated road to recovery.
Kurokawa et al. 42 reported that the rate of neurological deterioration postoperatively (with a decrease of minimal one ASIA score) was 29.3% (41/140). It was significantly correlated to the ability to walk unassisted at 1-month post-surgery.
The overall incidence of neurological damage after en bloc resection was 12.7% (105/824). Nerve root injury accounts for 24.8% (26/105) of all neurological complications, spinal cord injury accounts for 17.1% (17/105), Horner syndrome accounts for 1.9% (2/105), and the remaining 57.1% (60/105) cannot be identified.
Hardware Failure
Matsumoto et al. 45 identified 6 cases (40.0%) of hardware failure: breakage of the rod in 3 patients, and breakage of rod as well as the cage, combined breakage of the cage and screw back-out, and an endplate fracture resulting from cage subsidence occurred in 1 patient each.
Li et al. 40 studied the hardware failure rate after total en bloc spondylectomy (TES) of lumbar and thoracic spine tumors, in which a titanium mesh cage was used for anterior reconstruction. Overall, hardware failure occurred in 8 cases (26.7%). The mean interval duration from TES to hardware failure was 31.8 ± 15.1 months.
Sciubba et al. 24 conducted a retrospective review of 23 patients with aggressive primary or malignant tumors located at the lumbar spine. After TES, hardware failure emerged in 9 patients (39.1 %) at a median time span of 23 months after index spondylectomy. The results of the logistic regression analysis showed that postoperative radiation was significantly correlated to hardware failure (odds ratio [OR] 7.49; 95% confidence interval [CI], 1.02‒54.9).
Using carbon fiber stackable cage system filled with autogenous graft or bone substitutes for anterior reconstruction in most cases, Boriani et al. 7 reported a hardware failure rate of 14.1% (31/220), and 9 cases were clinically significant and requiring revision surgery.
Overall, there was a 12.1% (99/821) incidence of hardware failure. Revision surgery for hardware failure accounted for 63.1% (65/103) of all revision surgeries.
Dural Tear and Cerebrospinal Fluid Leakage
Kurokawa et al. 42 studied 140 patients that underwent TES for spinal tumors. Less than 1 month following surgery, postoperative CSF leakage was detected in 29 of these patients (20.7%). The incidence of surgical site infection (SSI), postoperative CSF leakage, and postoperative neurological deficits were independently related to the motor Functional Independent Measure score.
Shah et al. 28 conducted a retrospective review of two-stage modified en bloc spondylectomy for primary tumor cases and solitary metastases of the thoracic or lumbar spine. The dural tear rate was 33.3% (9/27), 4 cases of CSF leak were observed postoperatively.
Boriani et al. 7 studied 220 en bloc resections. Dural tear occurred in 19 procedures (8.6%). Of them 13 cases were considered major and 6 minor cases were successfully repaired during the same procedure.
In our systematic review, the overall incidence of dural tear and CSF leakage after en bloc resection was 10.6% (87/824).
Wound-Related Complications
In a retrospective study of prospectively collected data study involving 220 en bloc resections, Boriani et al. 7 reported postoperative wound and soft tissue problems in 8.2% (18/220). Six cases required surgical debridement and long-term treatment with multiple types of antibiotics.
Sciubba et al. 24 reported wound infection in 26.1% (6/23). Of these 6 patients with wound infection, 5 needed revision for debridement and one received treatment with antibiotics.
Ohashi et al. 3 reported SSI in four out of 18 consecutive patients who, between 1991 and 2015, underwent en bloc spondylectomy for spinal metastases. Revision surgery was performed in 3 of these.
Thus, the total wound-related complication rate was 7.6% (63/824), with 47.6% (30/63) of these cases requiring revision. Revision surgeries due to wound-related complications accounted for 29.1% (30/103) of all revision surgeries.
Vascular Injury and Bleeding
25 cases of vascular injury and bleeding were reported by Boriani et al. 7 in their series. In them, 19 cases were defined as major, 6 cases were defined as minor. Three patients died of the complication including one intraoperative death due to vena cava injury and 2 fatal aortic dissections.
Zoccali et al. 36 reported 37 cases of patients older than 60 years surgically treated with en bloc spondylectomy. Vascular injury and massive blood loss occurred in 16 cases, 2 of them died after the operation.
In this systematic review, the total complication rate of vascular injury and bleeding was 7.3% (50/684). Five cases lead to death which accounted for 41.7% (5/12) of all complication-related deaths.
Complication-Related Revision Rate
We identified 103 complication-related revisions in a total of 961 patients in these 36 papers, with an overall revision rate of 10.7% (Table 3). The most common complication leading to revision was hardware failure (63.1%) followed by wound-related complications (29.1%). Other complication leading to revision included neurological deterioration caused by hematoma7,17 or misplaced pedicle screws, 3 aortic dissection, 7 pleural effusion requiring surgical thoracoscopic drainage, 7 and others.16,23,29
Complication-Related Deaths
The average incidence of complication-related death was 1.2% (12/961) in our systematic review (Table 3). Among the 12 mortalities, there were 5 of vascular injury and massive blood loss,7,36 3 of cardiac complications,7,36 one of pulmonary embolism, 7 one of disseminated intravascular coagulation, 11 one of bowel necrosis, 28 and one of unmentioned reason. 7
Discussion
En bloc resection is a technically demanding procedure with great risks, which aims to obtain local disease control and improve the patient’s quality of life.1,2 Given the nearness of adjacent visceral organs and neurovascular structures, preoperative treatment, the necessity for a complex approach, and increased loss of blood and surgical duration, oncological resection of spinal tumors is often associated with significant morbidity and mortality, even at experienced centers.7,46 In this systematic review, we analyzed data from 36 articles, including 961 patients, and found an overall mean complication rate of 58.3%. Neurological damage (12.7%) were most common, followed by hardware failure (12.1%), dural tear and CSF leakage (10.6%), wound-related complications (7.6%), and vascular injury and bleeding (7.3%). The complication-related death rate was 1.2% (12/961) and complication-related revision rate was 10.7% (103/961).
Neurological Damage
In the included papers, some neurological damages were permanent and devastating,7,42,43 while some were transient and tolerable. 26 During specimen release, rotation, and removal, particularly in the thoracic spine, manipulation of the spinal cord increases the risk of neurological injury. 2 In the thoracic spine, root resection is often performed to reduce cord traction. However, in the lumbar spine, particularly the lower lumbar spine, when the aim is to preserve the nerve root, the dural tube and nerve root are inclined to sustain injury during the procedure of removing the tumor and installing the prosthesis. 35 We highly recommend the utilization of neuromonitoring.
Although a purposeful breach of oncological standards, such as planned intralesional transgression to retain vital structures or decrease morbidity, should be taken into consideration and discussed with a multidisciplinary team and the patient, a tumor-free margin with acceptable functional loss is preferred if the tumor extent and surgical anatomy make this feasible. 47
Dural Tear and Cerebrospinal Fluid Leakage
The incidence of dural tear in en bloc resection is higher than in other spinal surgeries because of its exceptionally invasive nature, epidural tumor extension, and complicated medical backgrounds, such as a history of radiotherapy. Furthermore, the large dead spaces surrounding the dural sac created by the surgery make CSF leakage more likely, leading to further complications and prolonged hospitalization. 48
Yokogawa et al. 49 found that revision surgery, a history of radiotherapy, and advanced age were independent risk factors for incidental dural tear during en bloc surgery. Scar tissue from prior surgery surrounding the dural sac and radiation-induced fibrosis can result in dural adhesion and obscure the anatomy.49,50 In older patients, the potential mechanism involves the decrease in tissue elastin with age, resulting in a significant decrease in biomechanical strength. 51
Nearly half of dural tears occurred near the nerve roots during the course of dissecting the dura mater from the tumor mass, and more than 60% of dural tears led to postoperative CSF leakage. 49 Covering such tears with polyglycolic acid mesh and fibrin glue spray after suturing has been reported to avert CSF leakage postoperatively.52,53
Hardware Failure
En bloc resection aims at achieving a long life expectancy, however, the wide range of resection results in serious spine instability. The risk of hardware failure in these patients is higher than in patients undergoing palliative intralesional resection surgery. For patients that need en bloc tumor resection, robust spinal reconstruction with strong internal fixation, to achieve solid osseous fusion, is necessary to restore the stability and integrity of the resected area and retain functions of the spine. Hardware failure following en bloc resection indicates pseudoarthrosis within spinal reconstruction structures, and it can aggravate back pain or cause neurological deterioration, resulting in the necessity for revision surgery. 37
The reported risk factors for hardware failure include radiotherapy histology, location of the resected tumor, and the total number of instrumented vertebrae,37,40 Irradiation has a negative impact on the bone quality and recovery process. 54 To lessen the need for postoperative radiotherapy, surgeons should strive for minimization of tumor contamination during surgery. Radiation therapy should solely be applied after thorough treatment planning, and undirected irradiation must be averted.
Robust spinal reconstruction and careful surgical techniques, for example, larger diameter rods, a longer posterior fixation, the satellite rod technique, disc-to-disc cut (no cut that goes through the vertebral body), meticulous endplate preparation, shortening of the spinal column, and appropriate anterior support approach, should be considered.24,44,45,55,56 In recent studies, 3D-printed prosthesis has shown many advantages compared with conventional reconstruction methods,33,57 and it has been used more commonly in our center.
Wound-Related Complications
Wound-related complication is a serious complication of en bloc resection and could undermine the quality of treatment outcomes. En bloc resection is a major, invasive surgical procedure with a long operation time. The major skin incision, devitalization of soft tissue, and incomplete removal of dead space may compromise wound healing. 24 Patients with vertebral tumors may also be in an inadequate nutritional condition and are susceptible of immunosuppression caused by the illness or as a result of treatments. Some patients had prior radiotherapy and/or chemotherapy, both of which impair wound healing.58,59
Hayashi et al. 59 found that independent risk factors for SSI post-TES included combined approaches and the non-use of iodine-supported spinal instruments. A combination of the anterior and posterior approach was another SSI risk factor in en bloc surgery. This approach may be required for tumors located at the lower lumbar level or in cases where a posterior-only approach cannot achieve a safe margin. The combination of anterior and posterior approach is associated with the following disadvantages: the possibility of a staged procedure, the necessity of patient repositioning, a greater degree of surgical trauma, and increase in operation time. Thus, it is imperative to choose surgical methods according to the risk‒benefit assessment. Use of iodine-supported or silver coated spinal instruments may decrease the incidence of infections associated with implants. 59 Betadine irrigation and intrawound vancomycin powder was routinely used in our center prior to wound closure.
Vascular Injury and Bleeding
En bloc resection of spinal lesions poses a significant technical challenge and risk of morbidity due to the proximity of vital neurovascular structures and viseral organs, particularly if these structures were encased. Unexpected bleeding and vascular injury may be encountered during tumor margin free, epidural plexus manipulation, or specimen removal, especially in revision surgery or previously irradiated cases. It may be devastating for not only leading to immediate hemodynamic imbalance, but also increasing the risk of cardiovascular failure at the last steps of such a long procedure. Our research showed that it is the leading cause of complication-related death.
In our opinion, preoperative radiographic anatomy should be extensively reviewed to assess the extent of tumor involvement and to evaluate for aberrant vascular anatomy. Preoperative embolization of the vertebral arteries is often beneficial. Assistance of an approach surgeon may maximizing patient safety particularly for patients with tumor compression or involvement of the major vessels. Patient and careful hemostasis should be maintained throughout the procedure. We are used to administer tranexamic acid intraoperatively in the attempt to minimize operative blood loss.
En bloc resections should be managed by an integrated, multidisciplinary team. The decision-making process prior to en bloc resection should take both the high morbidity, as reviewed in the present study, as well as the positive effect on the oncology prognosis into consideration. Surgeons should not be hindered from conducting the surgery by the high risk of complications when it is indicated, as few patients die from complications 7 . Most cases benefited from the oncosurgical results when proper en bloc resection was accomplished. Conversely, inappropriate surgery leads to local recurrence, which affects prognosis in a negative way and may be related to a greater risk of complications in the course of subsequent revision surgery.
We hope our systematic review will provide some inspiration for preoperative communication, perioperative care, and postoperative surveillance. The potential risk of neurological damage requires adequate preoperative notification. A thorough preplanning is vital to deal with the accidental intraoperative dural tear, vascular injury, and massive bleeding. Wound-related complication should be addressed due to its high incidence rate and impact on postoperative adjuvant therapy. During the postoperative follow-up, particular attention should be paid to the instrumentation as well as oncological status. A local sagittal CT is required to evaluate graft fusion.
This study was limited in that it included patients with primary spine tumors and spine metastases who received surgical treatment, regardless of their prior history of radiation, performance status, or the level of spinal metastases in the spinal column. The diversity in the methodology of classifying and reporting specific procedure-related complications created study heterogeneity. Improved complication classification and grading systems may more accurately reflect the impact of adverse events on spinal tumor patients, thereby optimizing treatment. The level of evidence of these studies was relatively low and future prospective studies with standard outcome assessment are warranted.
Conclusion
Patients who undergo en bloc resection for spine tumors are associated with complicated therapeutic challenges that require assessment within a multidisciplinary team. The overall complication rate is high. However, complication-related death was rare. The advantages of surgery must be weighed against the related severe perioperative morbidity, especially since quality-of-life concerns have become more urgent for tumor patients recently. This systematic review serves as a convenient reference for patients as well as surgeons in the discussion regarding the risk‒benefit assessment of en bloc surgery for spinal tumors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by Scientific Research Startup Fund of Henan Cancer Hospital