
Abstract
Study Design
Retrospective cohort study.
Objective
To investigate the effect of HRVA on the intrapedicular accuracy of C2PS placement through the freehand method in patients with BI and analyse the possible risk factors for C2PS malpositioning.
Method
A total of 91 consecutive patients with BI who received 174 unilateral C2PS placements through the freehand method were retrospectively included. The unilateral pedicles were assigned to the HRVA and non-HRVA groups. The primary outcome was the intrapedicular accuracy of C2PS placement in accordance with the Gertzbein–Robbins scale. Moreover, the risk factors that possibly affected intrapedicular accuracy were assessed.
Results
The rate of intrapedicular accuracy in C2PS placement in patients with BI was 23.6%. Results showed that the non-HRVA group had remarkably higher rates of optimal and clinically acceptable C2PS placement than the HRVA group. Nevertheless, the HRVA group exhibited similar results for grade B classification as the non-HRVA group. Moreover, in the HRVA and non-HRVA groups, the most common direction of screw deviations was the lateral direction. Furthermore, the multivariate analyses showed that the obliquity of the lateral atlantoaxial joint in the sagittal plane ≥15°, and that in the coronal plane ≥ 20°, isthmus height < 4.3 mm, and distance from the skin to the spinous process ≥ 2.8 cm independently contributed to a high rate of screw malpositioning in BI patients.
Conclusion
The presence of HRVA in BI patients contributed to the high rate of malpositioning in C2PS placement via the freehand method. However, the rates of intrapedicular accuracy in patients with BI with and without HRVA were considerably low.
Keywords
Introduction
A variety of posterior screw fixation techniques for C2 vertebrae have been utilised for biomechanical stability. These techniques include spinous process/laminar wiring techniques; sublaminar hook fixation; transarticular/pedicle screw fixations and salvage screw techniques involving pars/laminar screw fixations, cortical screw fixation and the ‘in-out-in’ method on the medial or lateral side of the narrow pedicle.1-8 Amongst these methods, the C2 pedicle screw (C2PS) placement, which was first described by Goel et al 4 in the 1980s, has been frequently used due to its high fixation and fusion rates, great pull-out strength and rigid vertebral immobility.9-11 However, the malpositioning of the C2PS might lead to catastrophic results, such as vertebral artery (VA) injury from the lateral or inferior violation of the pedicle cortex and spinal cord injury from medial violation. 7 Thus, safe and accurate placement is essential for avoiding injuries to vital structures.
Many studies have evaluated the safety of C2PS placement through the freehand method in cohorts with normal anatomy and reported high accuracy rates ranging from 82.5% to 100.0%.12-18 Meanwhile, relatively high accuracy rates varying from 74.7% to 98.1% have been reported for patients with atlantoaxial instability.19-22 However, no studies have been performed on the accuracy of C2PS placement in patients who were diagnosed with basilar invagination (BI) because atlantoaxial instability; atlas occipitalisation; pedicle anomalies, including narrow pedicle widths and low isthmus heights; C2-3 assimilation and high-riding VA (HRVA) are commonly seen in these patients; these anomalies increase the difficulties and danger of C2PS placement.7,23-26 Although the low rate of C2 insertion accuracy in patients with BI is a commonly held belief, no works have been conducted to verify this assumption and assess the rate of intrapedicular accuracy. Meanwhile, the related risk factors of anatomical characteristics that might cause malpositioning remain unknown.
HRVA is commonly associated with unusual tortuosity at the isthmus of C2 vertebra that courses more medially, posteriorly or superiorly than normal and alters the morphology and volume of the C2 pedicle, ultimately contributing to the narrowness of the trajectory for C2PS placement. 27 Therefore, pars or laminar screw fixation is usually chosen as the alternative method for placement on the side of the VA variant.7,17 Given that medial tortuosity, rather than posterior and superior tortuosities, mainly increases the risk of VA injury and malpositioning, HRVA is not the absolute contraindication for pedicle screw placement. 28 Nevertheless, Yeom et al reported remarkably high rates of VA injury and malpositioning in C2PS insertion in the presence of HRVA. 29 As a result, the diagnoses of BI and HRVA were considered as the risk factors for malpositioning. However, to the authors’ knowledge, no studies have explored the effects of HRVA on the accuracy of C2PS placement in patients with BI.
Thus, the current study was performed to assess the rate of accurate C2PS placement in patients with BI, compare the rates of accurate insertion between patients with BI with HRVA and those without HRVA and explore the risk factors that possibly affect insertion accuracy in patients with BI through univariate and multivariate logistic regression analyses.
Method
Participant Demographics and Study Design
A total of 91 consecutive patients who were diagnosed with BI in reference to the Chamberlain line
30
and who received 174 unilateral C2PS placements in the occipitocervical region via the freehand method during the period of May 2017 to November 2021 were retrospectively included in this comparative study. This study was approved by the Ethics Committees of the 2 medical centers, who waived the requirement for informed consent due to the retrospective nature of the research. According to diagnostic criterion of HRVA with Chung classification
31
(Figure 1), the included 174 unilateral pedicle screws were assigned into HRVA (107 screws) and non-HRVA (67 screws) groups. The high-riding vertebral artery (HRVA) was identified with the sagittal (A) and coronal (B) sections transecting the mid-portion of the C1-2 facet joint. The HRVA was defined as an internal height (a) ≤ 2 mm, isthmus height (b) of the axis ≤5 mm, or both.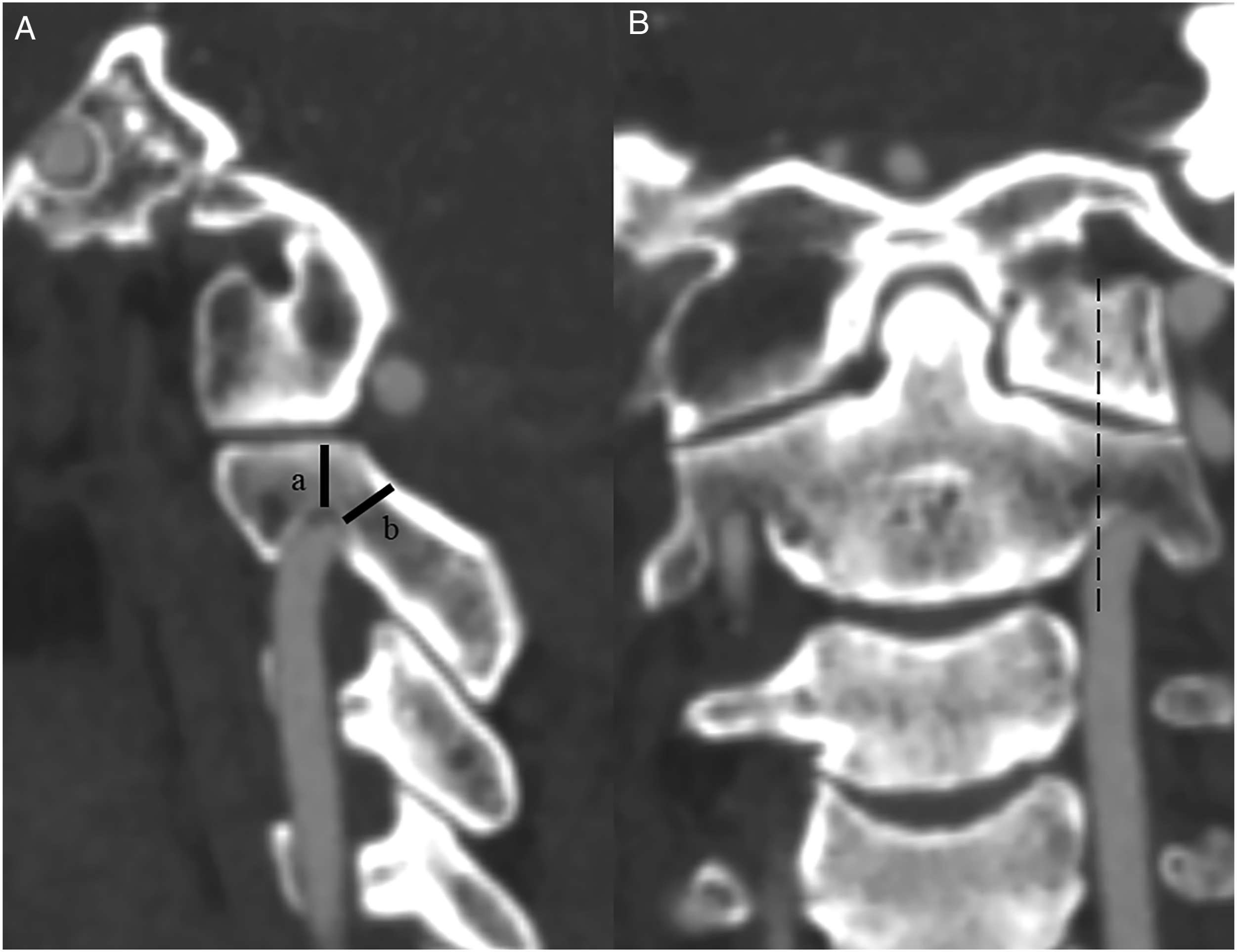
The selected patients fulfilled the following criteria: 1) aged between 20 and 75 years old; 2) diagnosed with BI; 3) had indication for C2PS; 4) received preoperative and postoperative three-dimensional (3D) CT examinations and 5) underwent screw placement through the freehand method instead of with a 3D-printed navigation template, computer-assisted navigation or the robot-guided technique. Exclusion criteria were as follows: 1) the patient previously underwent surgery on the occipitocervical region or required revision surgery; 2) the patient had occipitocervical infections or tumours and 3) the review case had incomplete data.
Surgeries were conducted by 4 surgery teams at 2 medical centres. Radiographic data were independently assessed by an experienced surgeon and a radiologist who were experts on the measurement methods. If divergences existed, a senior surgeon who acted as the third independent evaluator made the final decision on categorical variables. The average values of the continuous variables measured by the observers were utilised in this study.
Surgical Procedures of C2PS Placement
Preoperative 3D-CT scans were performed on all included patients to assess variations in C2 pedicle anatomy and the VA. Computed tomographic angiography (CTA) examinations were further conducted on patients with possible arterial anomalies in the occipitocervical region. C2PS instrumentation was determined on the basis of the anatomy of C2 vertebrae and in accordance the indication for the choice of C2 screw types, 32 and the ideal entry point and trajectory of C2PS were preplanned with 3D reconstruction. 33 Then, pedicle screw placement was carried out on C2.
Outcome Measures
The primary end point was the intrapedicular accuracy of C2PS placement assessed on the basis of postoperative 3D-CT examinations in accordance with the Gertzbein–Robbins scale,
34
which consists of grades A–E (Figure 2). Positions with grade A were regarded as the perfect position, those with grades A + B were considered as clinically acceptable positions and those with grades C + D + E were considered as malpositions. Intra-pedicular accuracy according to the Gertzbin–Robbins scale. (A). Grade A, the screw completely contained in the pedicle (a); (B). Grade B, the cortical penetration of less than 2 mm (b, cortical breach of 1.46 mm); (C). Grade C, the cortical penetration of 2 mm or more but less than 4 mm (c, cortical breach of 2.25 mm); (D). Grade D, the cortical penetration of 4 mm or more but less than 6 mm (d, cortical breach of 5.22 mm); (E). Grade E, the cortical penetration of 6 mm or more (d, cortical breach of 6.49 mm).
The secondary parameters were the statistics of cases with screw deviations in the superior, inferior, medial, lateral, superior–medial, inferior–medial, superior–lateral or inferior–lateral direction in the cortical breach of pedicle, and complications including intraoperative revision due to screw malposition, postoperative revision due to screw malposition, incision infections, cerebrospinal fluid infections, and worsening neurological symptoms after surgery.
The following variables that might affect intrapedicular accuracy were also collected for univariate and multivariate analyses: age, gender, body mass index (BMI), the side of screw insertion, atlas occipitalisation, atlantoaxial dislocation, C2-3 assimilation, the classification of Goel A and B types in BI,
35
the configuration of the lateral atlantoaxial articulation (LAA)
36
(Figure 3), the obliquities of the lateral atlantoaxial joint in the sagittal and coronal planes37,38 (Figure 4), pedicle width, lateral mass length, internal and isthmus heights,
39
the distance from the skin to the insertion point, the distance from the skin to the spinous process, the distance from the top of the odontoid to the Chamberlain line, pedicle mediolateral angle
33
and pedicle cephalad angle.
33
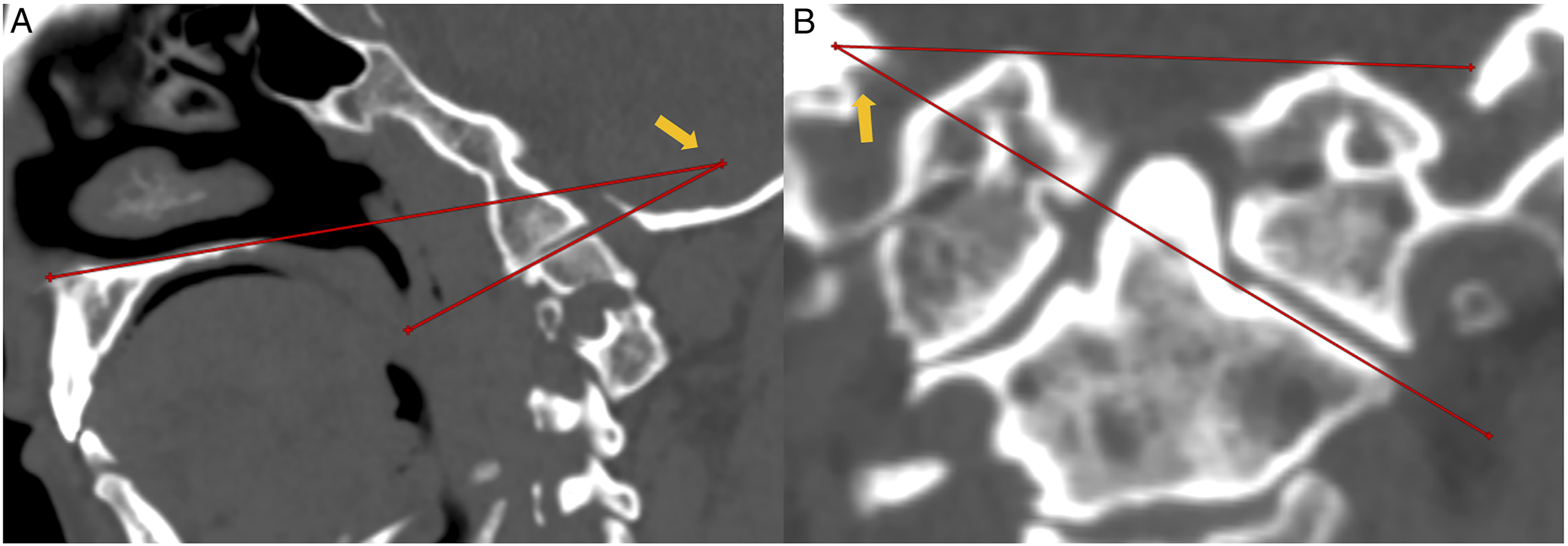
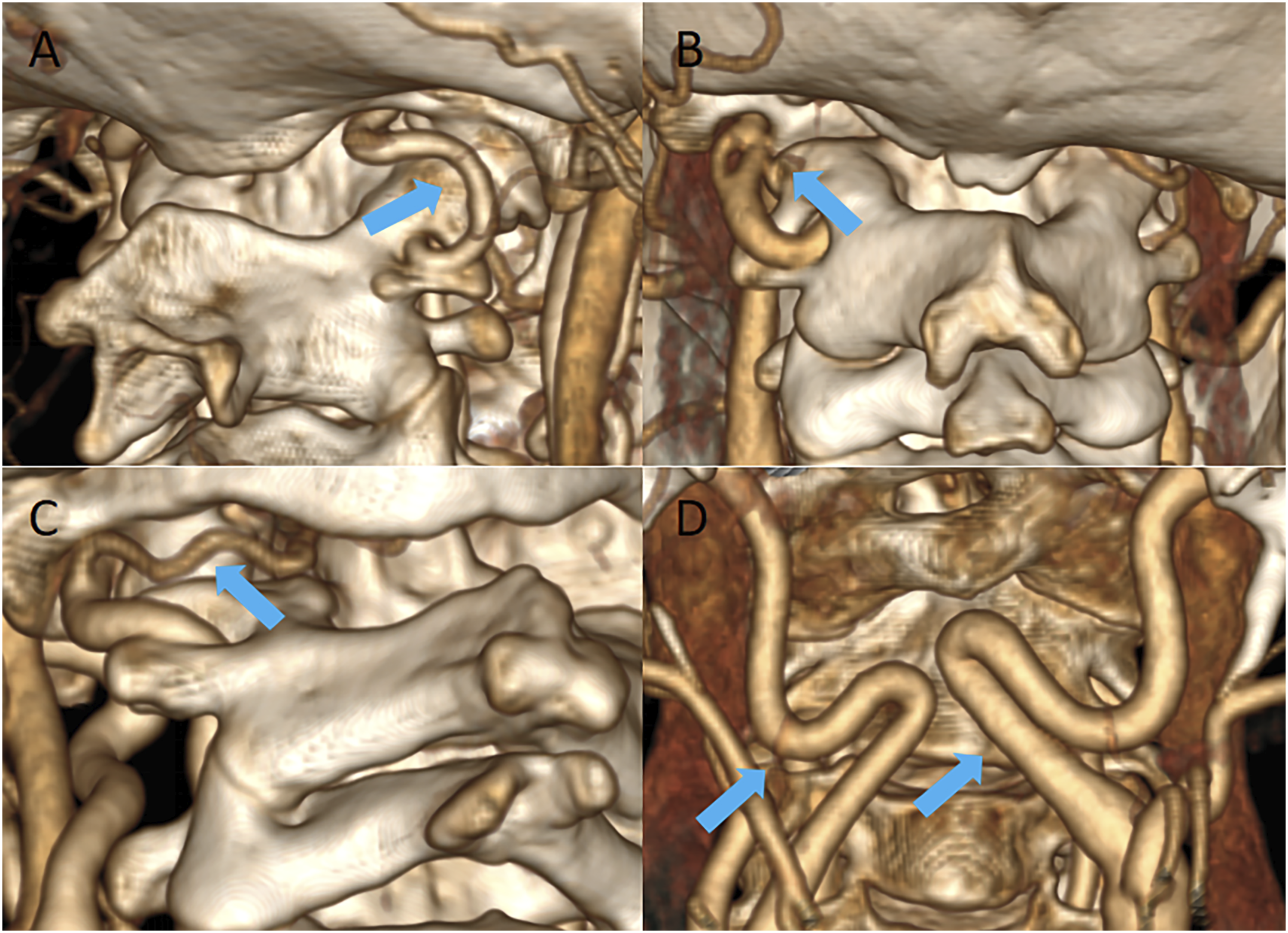
Furthermore, for the patients receiving preoperative CTA, persistent first intersegmental artery (PFIA), fenestrated VA (FEN), the extracranial C1/2 origin of the posterior inferior cerebellar artery (PICA), irregular midline carotid artery loop and the diameter of the VA on both sides were recorded.24,40 (Figure 5) Classification of configuration of lateral atlantoaxial articulations (LAA) in congenital anomaly. (A). normal anatomy; (B). Type I, slight anteversion of LAA without olisthy of the inferior and superior facets; (C). Type II, partial olisthy of 2 facets and the anteversion of LAA; (D). Type III, separation/complete olisthy of 2 facets; (E). Type IV, facts sloped dorsally. (A). The obliquity of the lateral atlantoaxial joint in the sagittal plane was defined as the angle between the line joining the anterosuperior and posterior points of the hard palate and the line joining the anterosuperior and posterosuperior points of the C-2 facet in that sagittal section (arrow); (B). The obliquity of the lateral atlantoaxial joint in the coronal plane was defined as the angle between the line joining the lateral and medial points along the superior surface of the C-2 facet and the line joining the points on the upper border of foramen magnum in that coronal section (arrow). (A). the persistent first intersegmental artery (PFIA, arrow); (B), the fenestrated vertebral artery (FEN, arrow); (C). the extracranial C1/2 origin of posterior inferior cerebellar artery (PICA, arrow); (D). the irregular bilateral midline carotid artery loop of both sides (arrows).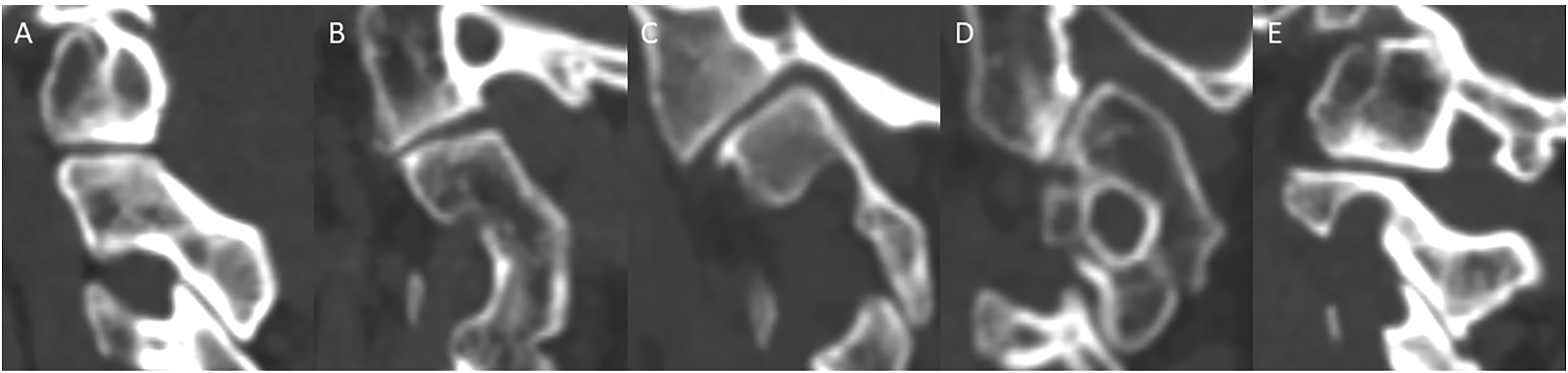
Statistical Analysis
Statistical analyses were conducted by using SPSS 23.0 software (IBM Corp., Armonk, New York, USA). Continuous variables were expressed as the mean and standard deviation. If the samples were in accordance with Gaussian distribution, independent t-test was performed to compare the 2 sets of data. Otherwise, Wilcoxon test was carried out for analysis. The categorical variables were presented as the absolute (no.) and relative (%) frequencies, and the χ2 test was used for the comparison of proportions. The factors that possibly affected intrapedicular accuracy were assessed through univariate and multivariate logistic regression analyses. The significance level was set as α = .05.
Results
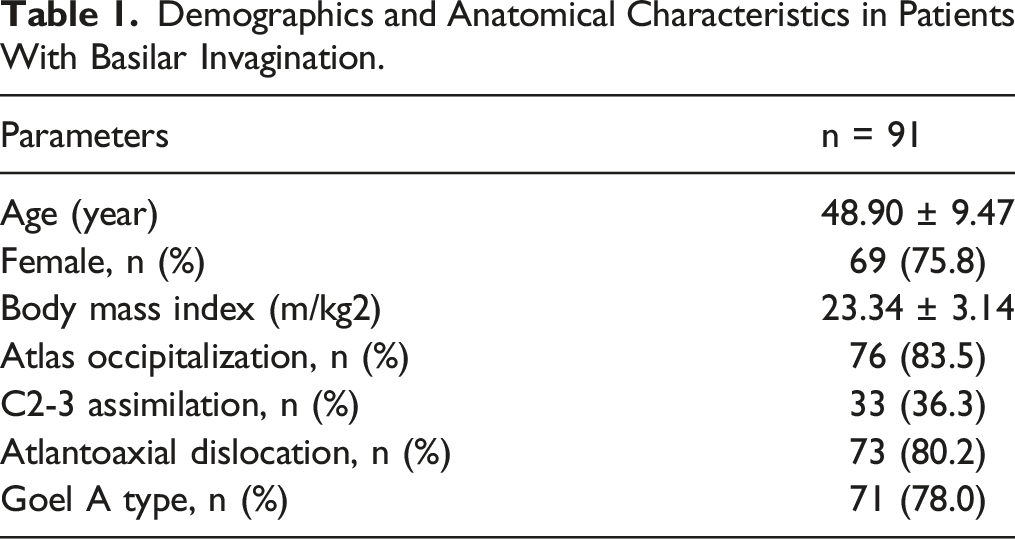
Demographics and Anatomical Characteristics in Patients With Basilar Invagination.
Demographic Data of Included Unilateral Pedicles With or Without HRVA.
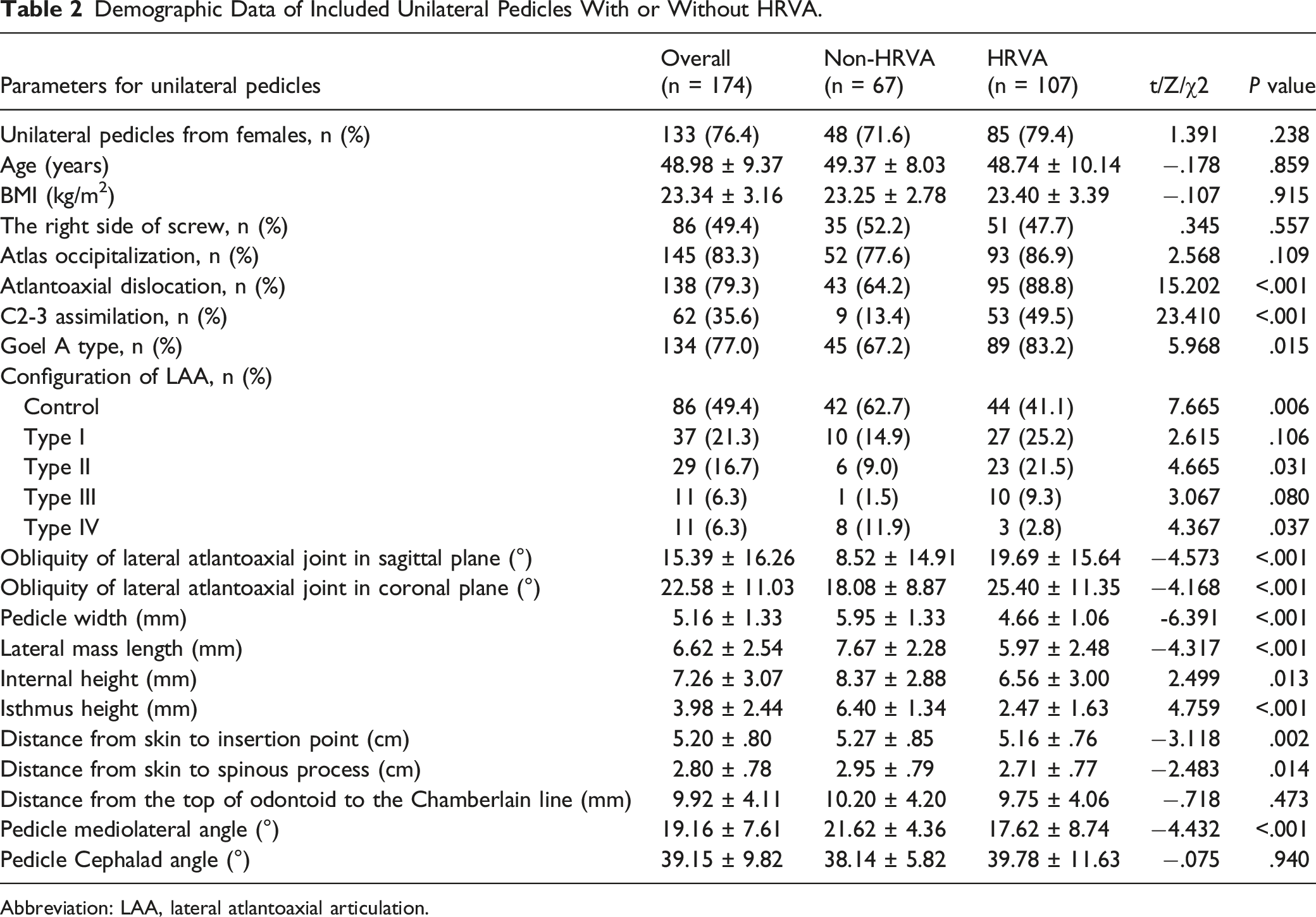
Abbreviation: LAA, lateral atlantoaxial articulation.
Accuracy of Pedicle Screw Placement
The rate of C2PS accuracy (grade A) was 23.6% (41/174 screws), and the rates of grades B, C, D and E were 37.9% (66/174 screws), 25.9% (45/174 screws), 12.6% (22/174 screws) and 0%, respectively.
Pedicle Screw Placement Accuracy in the Unilateral Pedicles With or Without HRVA.
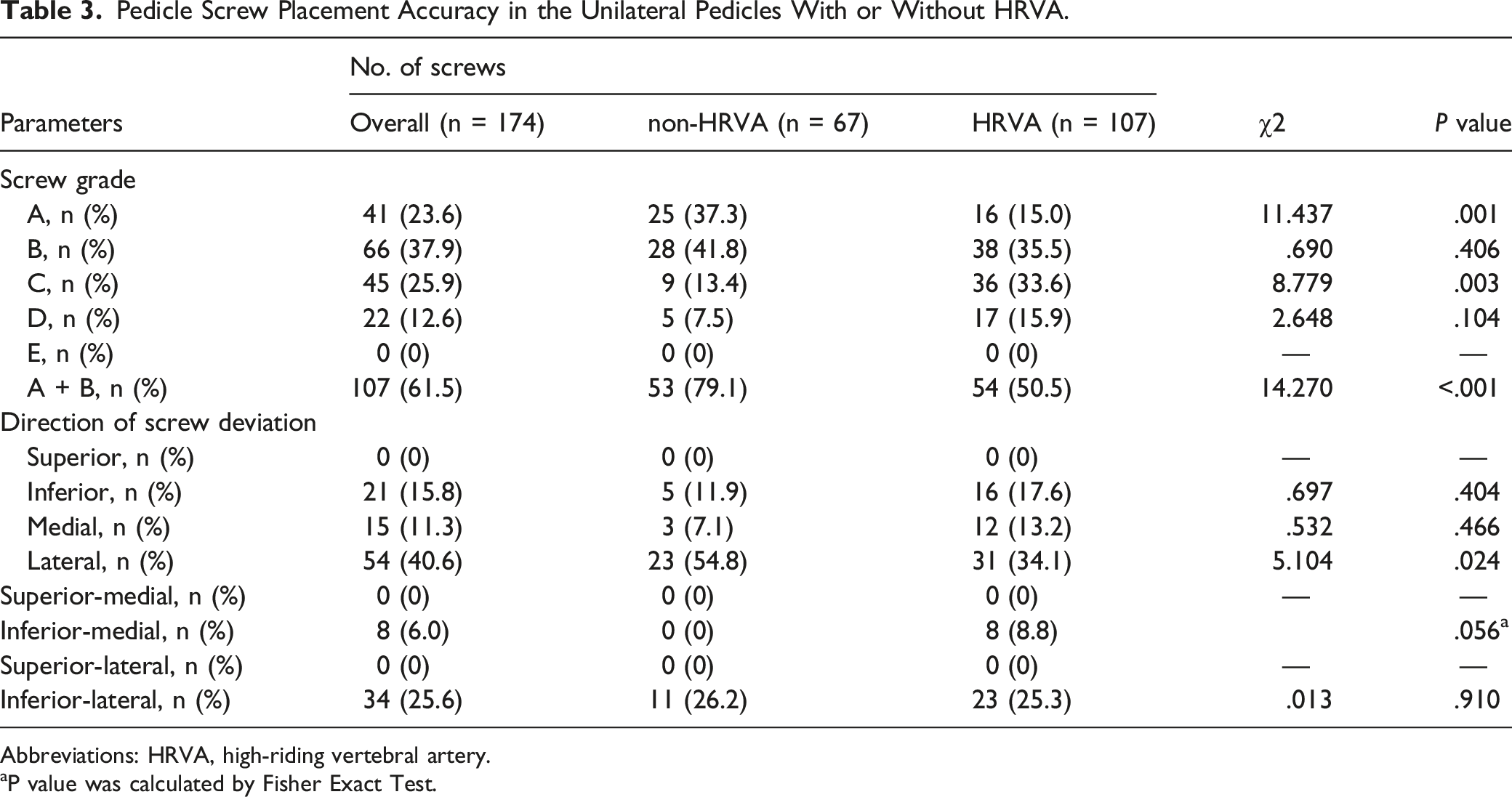
Abbreviations: HRVA, high-riding vertebral artery.
aP value was calculated by Fisher Exact Test.
Secondary Parameters
Amongst the deviations of the 42 screws in the non-HRVA group, the most common was lateral deviation as shown by 23 screws (54.8%), and inferior–lateral, inferior and medial deviations were exhibited by 11 (26.2%), 5 (11.9%) and 3 screws (7.1%), respectively. In addition, 91 screws caused deviations in HRVA group, and the most common screw deviation was also lateral as demonstrated by 31 screws (34.1%). Other deviations were inferior–lateral as shown by 23 screws (25.3%), inferior as exhibited by 16 screws (17.6%), medial as presented by 12 screws (13.2%) and inferior–medial as observed in 8 screws (8.8%). The rate of lateral deviation in the non-HRVA group was significantly higher than that in the HRVA group (P = .024), indicating a high risk of VA injury in the absence of HRVA. No significant differences in the inferior–lateral, inferior, medial and inferior–lateral deviations were found between the 2 groups. Furthermore, no superior, superior–medial and superior–lateral deviations were observed in the 2 groups (Table 3).
No significant differences were observed between the HRVA and non-HRVA groups in terms of surgical complications including intraoperative revision due to screw malposition (P = .764), postoperative revision due to screw malposition (P = .524), incision infections (P = 1.000), cerebrospinal fluid infections (P = 1.000), and worsening neurological symptoms after surgery (P = 1.000). (Supplementary file 2)
Univariate Analyses
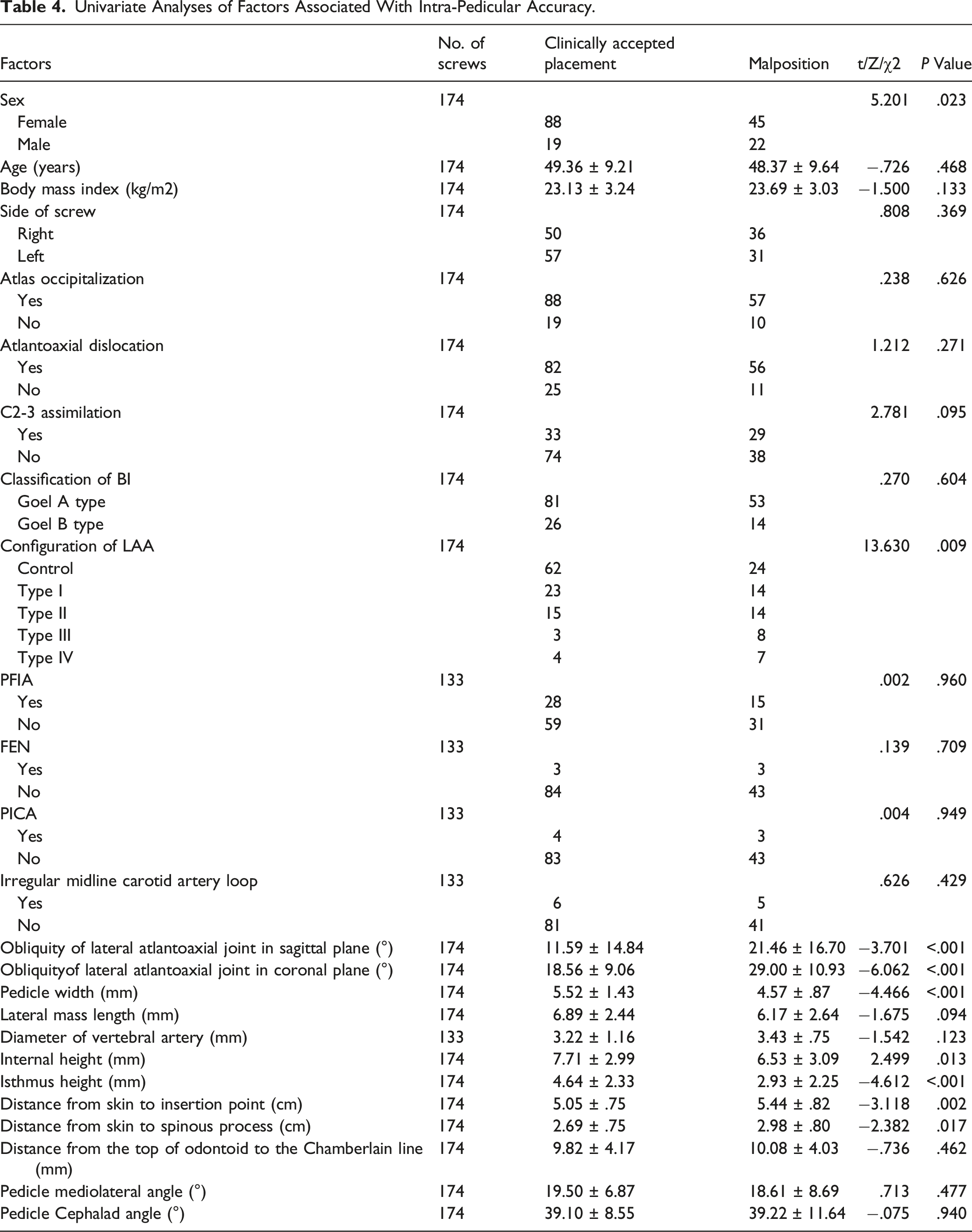
Univariate Analyses of Factors Associated With Intra-Pedicular Accuracy.
Multivariate Analysis
Logistic Regression Model of Variables Associated With Intra-Pedicular.

Discussion
C2PS placement has been regarded as a relatively safe and applicable method for fixation at the craniovertebral junction. 7 Given its benefit of three-column stability, this technique can provide more rigid atlantoaxial immobilisation, superior biomechanical properties and lower risk for nonunion than some alternative strategies, including pars and laminar screw fixations, which are usually applied when C2PS is infeasible due to variations in the VA and pedicle anatomies.9-11 However, high biomechanical stability is required to maintain vertebral immobilisation and facilitate bone fusion, especially in patients with BI and severe craniovertebral anomalies. Thus, for those with BI, the utilisation of C2PS is necessary under its indication, and the safe placement of C2PS is essential. Furthermore, HRVA is commonly associated with narrow pedicle width and high rates of VA injury and intrapedicular inaccuracy.29,41 The incidences of HRVA are 24.1%–33.9% in consecutively included patients and 61.5% in patients with BI.24,42-44 However, whether HRVA has an effect on the rate of accurate insertion in BI or not remains unknown. Furthermore, the related risk factors of anatomical characteristics that might cause malpositioning in BI need to be further explored to provide a reference for insertion procedures.
In the current study, we found that the rate of accurate C2PS placement in patients with BI was 23.6% and was lower than the previously published rates of 82.5% to 100.0% for accurate C2PS placement via the freehand method in cohorts with normal anatomy and of 74.7% to 98.1% in patients with atlantoaxial instability.12-22 Furthermore, the patients with BI in the non-HRVA group showed substantially higher rates of optimal and clinically acceptable pedicle screw placements than those in the HRVA group, indicating that the anomaly of HRVA remarkably decreased intrapedicular accuracy in patients with BI. However, the non-HRVA group had the low rate of optimal insertion of 37.3%, and the similar grade B classification results of the HRVA and non-HRVA groups hinted that the anomaly of BI also contributed to a large portion of intrapedicular inaccuracy.
The results may be ascribed to the following factors: Firstly, patients with BI and HRVA had more complicated anatomical landmarks and insertion trajectory for C2PS placement than those without. The congenital developmental anomalies of BI, such as irreducible atlantoaxial dislocation; atlas assimilation; C2-3 assimilation and variations in the posterior elements on C2 vertebrae, including the absence, incompleteness and ambiguity of the isthmus and spinous process, make identifying the anatomical landmarks for entry points difficult.26,45 Byun et al 41 and Yeom et al 29 demonstrated that HRVA was remarkably associated with a narrow pedicle and that the location of the HRVA groove in the caudal surface of C2 reduced the safe zone for screw trajectory, increased the mediolateral and upward insertion angles and easily resulted in cortex breaches and VA injuries. Furthermore, the significant correlation of HRVA with osteoarthritis and the severe obliquities of C1-2 facet joints contributed to C1-2 instability, bony pedicle malformation and C2 isthmus thinning.36,46 Moreover, in this study, we found that the presence of HRVA was also highly associated with the other bone anomalies, including atlantoaxial dislocation, C2-3 assimilation, Goel type A, LAA types II and IV and low internal height. Overall, these congenital and degenerative deformities changed the common landmarks for the entry point and the ideal position for the screw trajectory, ultimately increasing the risk of C2PS malpositioning.
The incidences of other VA anomalies, including the PFIA, FEN, PICA, irregular midline carotid artery loop and short VA diameter, have been reported to be higher in patients with BI than in those without.24,40 Thus, we evaluated whether these VA variants were the reasons why the HRVA led to the high rate of malpositioning in patients with BI. Finally, no remarkable differences were seen between the HRVA and non-HRVA groups. Meanwhile, univariate analyses revealed that these variants were not the risk factors that affected intrapedicular accuracy.
We also found that in the HRVA and non-HRVA groups, lateral deviations were shown by most of the pedicle screws, followed by inferior–lateral, inferior and medial breaches. These results were similar to the findings of Yeom et al, 29 who found that in patients with or without HRVA, pedicle screws were more likely to breach the lateral portion of the pedicle than transarticular screws. Nevertheless, the incidence of lateral deviation in the non-HRVA group was substantially higher than that in the HRVA group, indicating a high risk of VA injury in the absence of HRVA. This result might be attributed to the medially angled insertion of C2PS for the avoidance of VA injury due to the diagnosis of HRVA. Overall, the patients with BI with or without HRVA easily suffered from lateral pedicle breaches that might contribute to severe complications, especially VA injuries. Recent years, with the applications of computer-assisted navigation and robotic guidance techniques in spine surgery, high intrapedicular accuracy was achieved, and the the identification of landmarks for optimal entry point and trajectory in BI might benefit from the image guidance and navigation technique.47,48
The risk factors that possibly resulted in pedicle screw malpositioning in patients with BI were assessed through univariate and multivariate logistic regression analyses.
Univariate analysis revealed that male sex, severe LAA configuration, large obliquities of the lateral atlantoaxial joint in the sagittal and coronal planes, distance from the skin to the insertion point and distance from the skin to the spinous process and low pedicle width and internal and isthmus heights were the risk factors related to screw malpositioning. Multivariate logistic regression analyses showed that obliquity of the lateral atlantoaxial joint in the sagittal plane ≥ 15°, obliquity of the lateral atlantoaxial joint in the coronal plane ≥ 20°, isthmus height < 4.3 mm and distance from the skin to the spinous process ≥ 2.8 cm were independently associated with screw malpositioning. The obliquities of the lateral atlantoaxial joint that were assessed on the basis of the superior sagittal and coronal C-2 facet angles indicated not only the severity of atlantoaxial dislocation in the sagittal and coronal planes but also the difficulty of its reducibility.37,38 Salunke et al 38 found that patients with the obliquities of the lateral atlantoaxial joint in the sagittal plane of less than 30° could undergo reduction with traction or perioperative facet distraction. In the current study, we found that the large obliquities of the lateral atlantoaxial joint were independent risk factors for predicting the intrapedicular accuracy of C2PS placement in patients with BI because the high sagittal and coronal angles of the obliquities may present severe atlantoaxial instability, high LAA configuration grade and serious pedicle and isthmus bony malformations.36,37,46 Furthermore, an isthmus height of less than 4.3 mm and narrow pedicle width are commonly associated with the high and medial tortuosities of VA and the narrow volume of the pedicle for screw placement; these characteristics all increase the violation rate.29,40 Furthermore, a long distance from the skin to the insertion point and from the skin to the spinous process might contribute to increased resistance from paravertebral soft tissues that results in an inner entry point and trajectory with increased divergence, ultimately reducing insertion accuracy. Meanwhile, compared with females, males might also have greater skin elasticity and muscle strength that then lead to a high incidence of violation, especially in the freehand method. Thus, a preoperative 3D-CT scan is highly recommended for patients with BI to identify the abovementioned risk factors to reduce intraoperative VA injury and increase intrapedicular accuracy.
Therefore, for such patients, preoperative 3D-CT and CTA are highly recommended to evaluate the degree of BI and VA anomalies and the related risk factors for individualised treatment to increase the intraoperative safety of screw placement and reduce postoperative complications. In recent years, 3D-printed navigation templates, computer-assistant navigation and robot-guided techniques have been gradually applied in surgeries on the cervical spine and other complex structures that require precise manipulation and may thus become new directions for individualised screw placement strategies in the future. 49
The potential limitations of this study should be noted. Firstly, given that the included patients were all Chinese who were admitted to 2 medical centres, the generalisability of the measured results may be limited. Thus, studies based on different ethnicities should be performed. Secondly, the sample size was relatively small partly because of the low prevalence of BI. Therefore, this study showed less powerful results in the detection of risk factors than other studies. Comparative cohort studies with large samples are required to confirm the incidence of intrapedicular malpositioning. Thirdly, this study only reported the radiological analyses of C2PS accuracy with 3D-CT slices but not the comparative outcomes of clinical indices and postoperative complications in the follow-up period. Fourth, the surgeries were performed by different teams at different centers, which might limit the comparability. Furthermore, only the accuracy of intrapedicular C2PS placement in patients with BI were discussed, and the insertion outcomes of other fixation techniques, such as the transarticular, pars, laminar and occipital screws, were ignored.
Conclusion
The presence of HRVA in patients with BI contributed to the high malpositioning rate of C2PS placement via the freehand method. However, the rates of intrapedicular accuracy in patients with BI with and without HRVA were considerably low. The obliquity of the lateral atlantoaxial joint in the sagittal plane ≥ 15°, the obliquity of the lateral atlantoaxial joint in the coronal plane ≥ 20°, isthmus height < 4.3 mm and the distance from the skin to the spinous process ≥ 2.8 cm were independent risk factors for C2PS malpositioning in patients with BI.
Supplemental Material
Supplemental Material - Effect of High-Riding Vertebral Artery on the Accuracy and Safety of C2 Pedicle Screw Placement in Basilar Invagination and Related Risk Factors
Supplemental Material for Effect of High-Riding Vertebral Artery on the Accuracy and Safety of C2 Pedicle Screw Placement in Basilar Invagination and Related Risk Factors by Lu-Ping Zhou, PhD, Ren-Jie Zhang, PhD, Hua-Qing Zhang, PhD, Zhen-Fei Jiang, MD, Jin Shang, MD, and Cai-Liang Shen, PhD in Global Spine Journal
Footnotes
Authors’ Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
The manuscript submitted does not contain information about medical device(s)/drug(s).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent
Ethical approvals were provided by the ethics committees of the First Affiliated Hospital of Anhui Medical University Ethics Committee (PJ2021-16-33) and the First Affiliated Hospital of the University of Science and Technology of China Ethics Committee (2021-RE-145). Since this is a retrospective study, formal consent is not required.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.