
Abstract
Study Design
Retrospective cohort study.
Objectives
Due to the close anatomic relationship between the pedicle and neurovascular structures, avoiding pedicle perforations is crucial in pedicle screw placement. Still, the use of larger screws has biomechanical advantages. Intraoperative 2D and 3D imaging, and navigation guidance can be used to combine both goals. The aim of this study was to compare the screw diameter/pedicle width ratio (SPR) and the screw placement accuracy for 3D controlled fluoroscopy-guided pedicle screw placement vs computer navigated transpedicular screw placement in the thoracic and lumbar spine.
Methods
200 cases of thoracic and lumbar pedicle screw placement, of which 100 cases were performed using intraoperative computer navigation and 100 cases were performed using fluoroscopy-guidance were retrospectively registered. In the fluoroscopy group, intraoperative 3D scans were performed to confirm implant position and allow for potential intraoperative revision. In addition to accuracy and SPR, demographics, dose reports, and procedure times were analyzed.
Results
Overall, 716 fluoroscopy-guided screws were compared with 740 screws placed using navigation. Screw accuracy (83.2% vs 90.5%; P = .001) and SPR (0.85 ± 0.17 vs 0.88 ± 0.21; P < .001) were significantly higher using navigation compared to fluoroscopic guidance. Furthermore, dose area product (28,545 ± 17,693 vs 20,638 ± 15,856 mGycm2; P < .001), fluoroscopy time (223.6 ± 93.6 vs 92.3 ± 39.7 seconds; P < .001), and procedure time (154.0 ± 81.0 vs 119.7 ± 48.7 min; P = .004) were significantly lower using navigation.
Conclusions
Intraoperative navigation does not only increase the accuracy of pedicle screw placement, but also allows for the placement of larger screws relative to the pedicle width, which may have biomechanical advantages. Notably, contrary to other studies, the use of navigation did not increase patient radiation exposure or procedure time compared to fluoroscopic guidance.
Keywords
Introduction
Dorsal instrumentation using transpedicular screw placement is a common procedure, particularly for a variety of traumatic and non-traumatic injuries of the thoracic and lumbar spine. 1 It may be performed by using an open approach, which entails extensive tissue trauma. Alternatively, fluoroscopy can be applied to either assist open or percutaneous pedicle screw placement. 2 In recent years, spinal navigation based on intraoperative 3D imaging has become increasingly popular. Numerous studies have demonstrated higher accuracy for navigated screw placement compared to fluoroscopy-based screw placement.3-5
Beyond the need for accurate screw placement to avoid misplacement-related complications, studies have shown that the biomechanical stability is highly dependent of the screw sizing relative to the pedicle dimensions.6,7 The highest possible stability of the fixation is considered a fundamental factor in avoiding long-term complications such as screw loosening and delayed union. 8 In this context, the selection of the appropriate screw size depending on the width of the pedicle has been identified as a critical aspect.9,10 While the use of larger screws increases the risk of pedicle perforation and complications, a larger screw diameter-to-pedicle width ratio (SPR) seems to provide biomechanical advantages.
While the effect of using spinal navigation on the accuracy of screw placement has been the subject of numerous studies, the effect of using spinal navigation on screw dimensioning requires further investigation.3,11,12
Therefore, the aim of this study was to analyze the SPR and the accuracy of pedicle screw placement between navigated and fluoroscopy-assisted techniques. The study hypothesis was that accuracy and SPR would be higher in the navigation group.
Methods
Inclusion and Exclusion Criteria.

Subsequently to the perusal of patient files, each patient was assigned to one of the two groups based on the intraoperative technique applied. Screws were either placed using fluoroscopy and additional 3D scans for verification of implant position (fluoroscopy group) or using intraoperative navigation (navigation group).
In both groups, patients were placed on a radiolucent carbon fiber operating table in prone position. Prior to preparation and draping, instrumentation levels were identified using fluoroscopy in both groups.
In the fluoroscopy group, the appropriate screw size was determined by the surgeon prior to the procedure based on measurements from the preoperative CT scan and communicated to the OR team prior to starting the procedure to ensure the correct screws were present in the operating room. After skin incision and soft tissue preparation, guide wire placement was performed bilaterally using Jamshidi needles under anteroposterior and lateral fluoroscopic imaging using a C-arm CBCT. The C-arms used were Cios Spin (n = 97) or Arcadis Orbic (n = 3; both Siemens Healthineers, Erlangen, Germany). Pedicle screws were then inserted over the guide wires while lateral view fluoroscopy was performed to monitor screw insertion depth. Intraoperative 3D imaging was performed in all cases in the fluoroscopy group after pedicle screw placement. In addition, 3D imaging was performed at the surgeon’s discretion after guide wire placement in cases where 2D fluoroscopy could not rule out incorrect guide wire placement. All patients underwent postoperative CT to document correct screw position.
In the navigation group, after skin incision and soft tissue preparation, the dynamic reference base (DRB) was attached to a spinous process centrally within the instrumentation levels, avoiding fractured vertebrae. A registration scan was then performed using a 3D C-arm CBCT (Cios Spin, Siemens Healthineers, Erlangen, Germany). Image acquisition used either standard (200 images in 30s) or high quality (400 images in 30s), depending on surgeon preference. While standard quality is usually sufficient, high quality or the obesity setting (400 images in 60s) was used in cases with spinal implants or obesity for optimal imaging. During the scan acquisition, ventilation was temporarily paused to optimize image quality. After automatic transfer of the image data to the navigation system (Pulse, NuVasive Inc., San Diego, CA, USA), navigated guide wire placement was performed: After verification of navigation accuracy, the navigated drill was used to determine the optimal soft tissue approach, avoiding instrument traction. Following soft tissue preparation to the lamina, the surgeon selected the appropriate screw diameter and length based on live imaging and saved the planned trajectory. High-speed drilling (3.5 mm diameter, 30 mm drilling depth) was then performed, and a guide wire was placed inside of the drill hole. To avoid relative movement of the vertebrae to the DRB which may occur during screw insertion due to the insertional torque and can affect navigation accuracy for the subsequent screws, all guide wires were placed before screw placement was performed. The implant systems used were Reline MAS (n = 73), Precept (n = 24; both NuVasive Inc., San Diego, CA, USA) and Viper (n = 3; DePuy Synthes, West Chester, Pennsylvania, USA) in the fluoroscopy group and Reline MAS (n = 100; NuVasive Inc., San Diego, CA, USA) in the navigation group.
After completion of screw placement, standard a. p. and lateral fluoroscopic images were obtained as part of the institution’s standard. At the surgeon’s discretion, another 3D scan was performed. Again, all patients underwent postoperative CT to document correct screw position.
Both, the pedicle width as well as the screw placement accuracy were assessed by an independent observer. While pedicle width was measured in the preoperative CT scan, the screw placement accuracy was assessed in the postoperative CT scan (slice thickness 2.0 mm, respectively) according to the Gertzbein-Robbins grading system (GRS). Grades A (no pedicle breach) and B (pedicle breach <2 mm) were considered acceptable, while Grades C to E (pedicle breach ≥2 mm) were considered potentially critical. The screw size and the pedicle width were used to calculate the screw diameter-to-pedicle width ratio (SPR). To evaluate the differences in SPR between the two groups, the SPR was calculated individually for each screw by dividing the screw diameter by the corresponding pedicle diameter. The mean SPR (± standard deviation) across all screws was then calculated for both groups. This approach ensures that each screw contributes equally to the group average and provides a representative measure of the typical ratio achieved with each surgical technique. This method was chosen over an alternative method of calculating the ratio of mean screw diameter to mean pedicle diameter because the latter may introduce bias by disproportionately weighting larger values, does not accurately reflect the distribution of individual ratios, and does not allow for valid statistical comparisons between groups.
In addition, patient and procedure-related data such as age, gender, BMI, indication for surgery, surgical approach, operating time, intraoperative fluoroscopy time and the intraoperative dose area product (DAP) were collected from the electronic patient chart and compared between the groups. While no clinical follow-up of the patients was performed, the digital patient record was retrospectively reviewed for follow-up visits and inpatient readmissions with potential complications and revisions.
Statistical analysis was performed using Prism 9 (Graphpad Software, San Diego, California, USA). The Gaussian distribution of the data was tested using Kolmogorov-Smirnov test. Descriptive statistics are given as mean values ± standard deviation for continuous variables and absolute values ± range for nominal and ordinal scaled variables. For normally distributed continuously scaled data, an unpaired t test was used to compare both groups, while Mann-Whitney U test was used as nonparametric alternative. For contingency testing, Fisher’s exact test was used. Pearson’s r was applied to test for correlation. A two-sided P < .05 was considered significant for all tests.
Results
Patient and Surgical Characteristics for Both Groups.
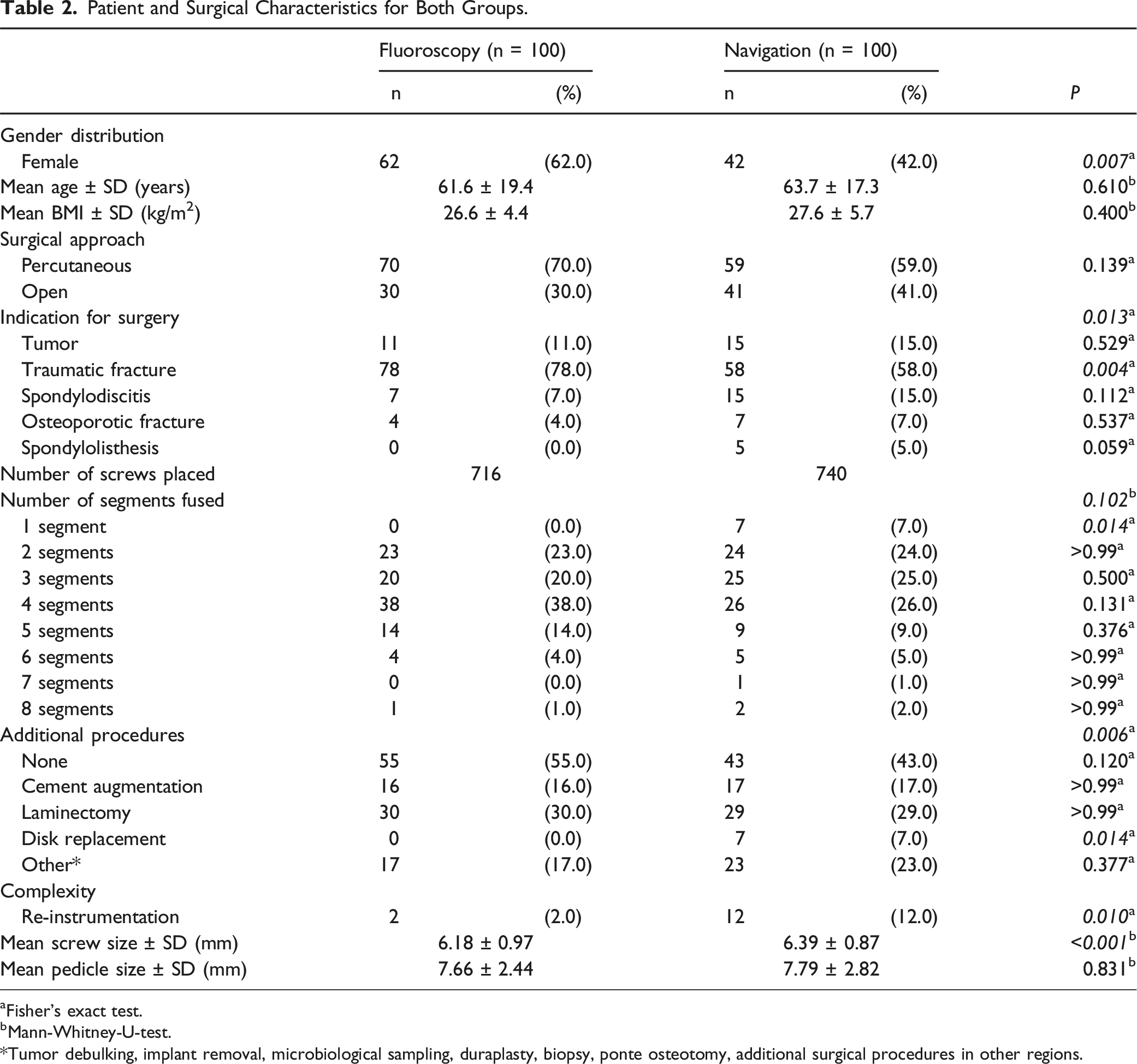
aFisher’s exact test.
bMann-Whitney-U-test. *Tumor debulking, implant removal, microbiological sampling, duraplasty, biopsy, ponte osteotomy, additional surgical procedures in other regions.
Overall screw placement accuracy in the fluoroscopy group was 83.2% (GRS grading: A 39.5%, B 43.7%, C 13.0%, D 3.6%, E 0.001%), whereas 90.5% of the navigated screws (GRS grading: A 48.2%, B 42.3%, C 7.8%, D 1.5%, E 0.001%) were placed accurately (P = .001; Figure 1). Accuracy rates for both groups according to Gertzbein and Robbins grading system (GRS).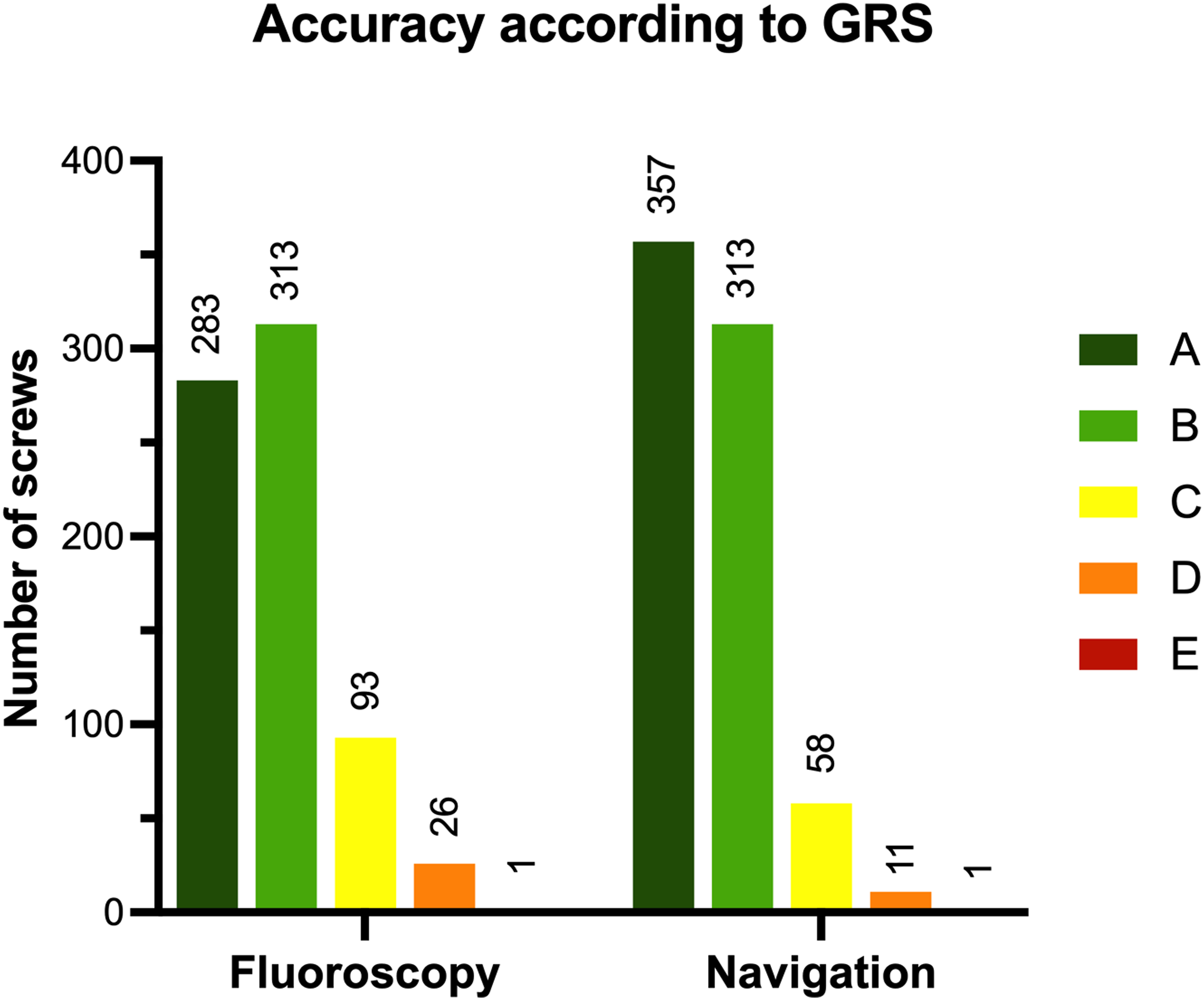
In the fluoroscopy group, 85 of the 131 relevant perforations were lateral (64.9%; 66 Grade C, 18 Grade D, 1 Grade E) and 46 were medial (36 Grade C, 10 Grade D). In the navigation group, 60 of the 79 perforations were lateral (75.9%; 48 Grade C, 11 Grade D, 1 Grade E) and 19 were medial (18 Grade C, 1 Grade D).
The mean SPR was 0.85 ± 0.17 in the fluoroscopy group and 0.88 ± 0.21 in the navigation group (P < .001). Both groups showed a significant correlation between the mean SPR and the screw placement accuracy (Fluoroscopy: r = −0,47, R2 = 0.22, P < .001; Navigation: r = −0.54, R2 = 0.29, P < .001). A detailed comparison of accuracy and SPR for both groups per level is shown in Figure 2. Accuracy rate and SPR per level for both groups.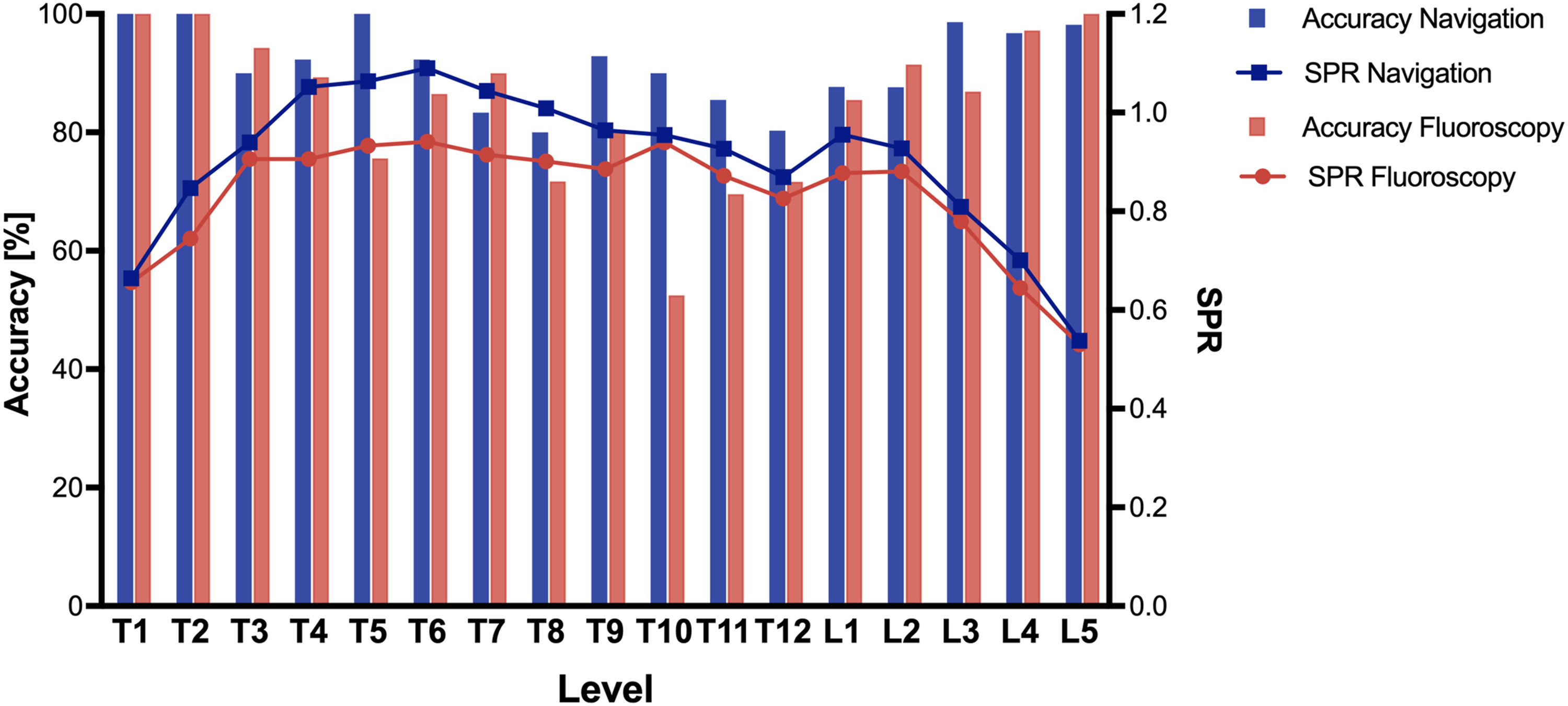
Accuracy Rate in Percent, SPR and Number of Screws Placed per Subregion Divided Into Upper Thoracic Spine (Th1-Th5), Midthoracic Spine (Th6-Th10), Thoracolumbar Spine (Th11-L2) and Lumbar Spine (L3-L5).
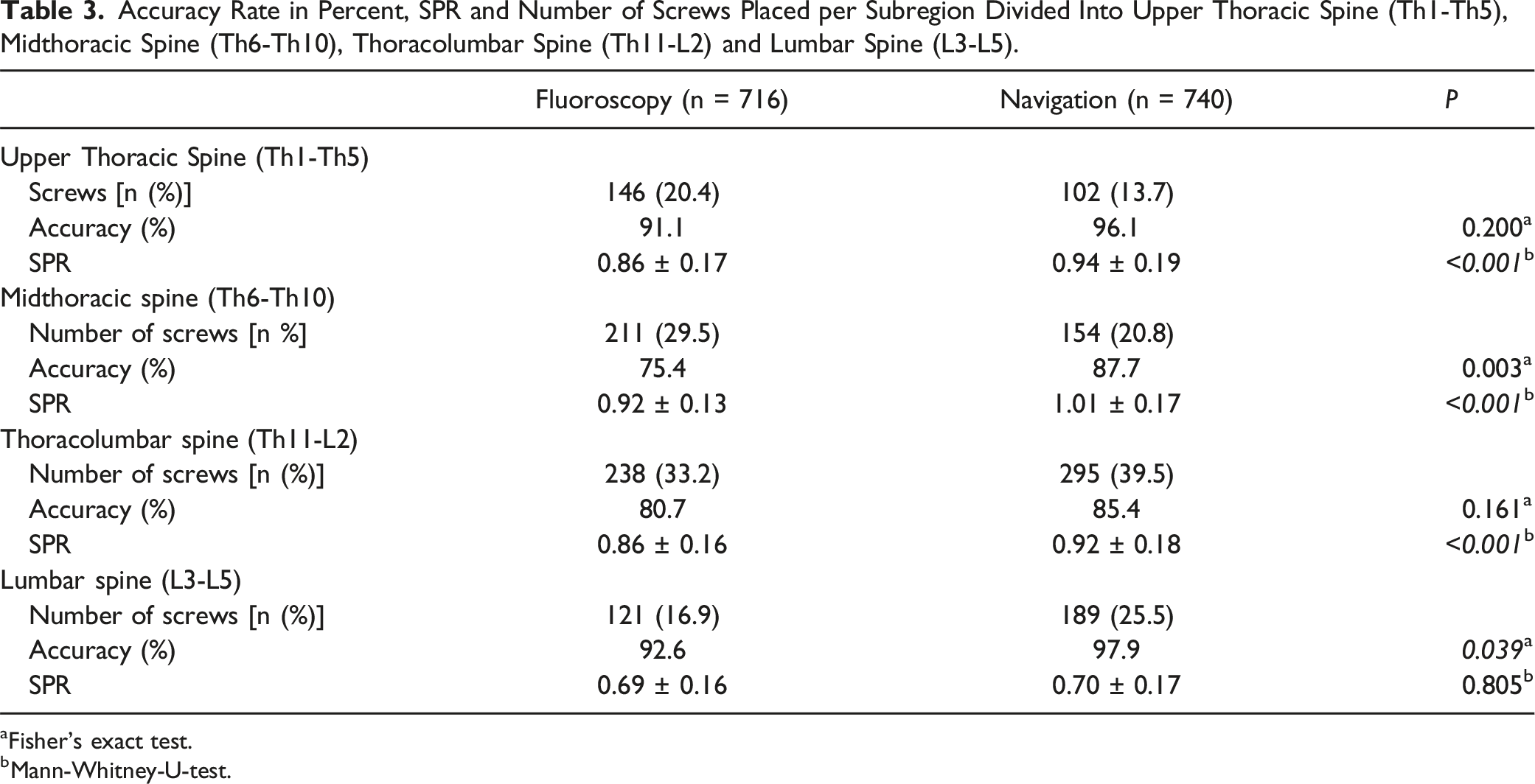
aFisher’s exact test.
bMann-Whitney-U-test.
Subgroup analysis was also performed for the comparison of percutaneous procedures vs an open approach. While in percutaneous procedures significant higher accuracy was reached using navigation (91.4% vs 82.5%; P < .001; Fisher’s exact test), no significant difference was found for procedures using an apen approach (89.4% vs 84.8%; P = .145; Fisher’s exact test). The SPR was significantly higher in the navigation group for percutaneous (0.87 ± 0.20 vs 0.84 ± 0.17; P = .002; Mann-Whitney-U-test) and open procedures (0.92 ± 0.21 vs 0.87 ± 0.17; P = .001; Mann-Whitney-U-test).
Complications and Number of Revision Surgery due to the Complications Listed in Each Group. CSF: Cerebrospinal Fluid.
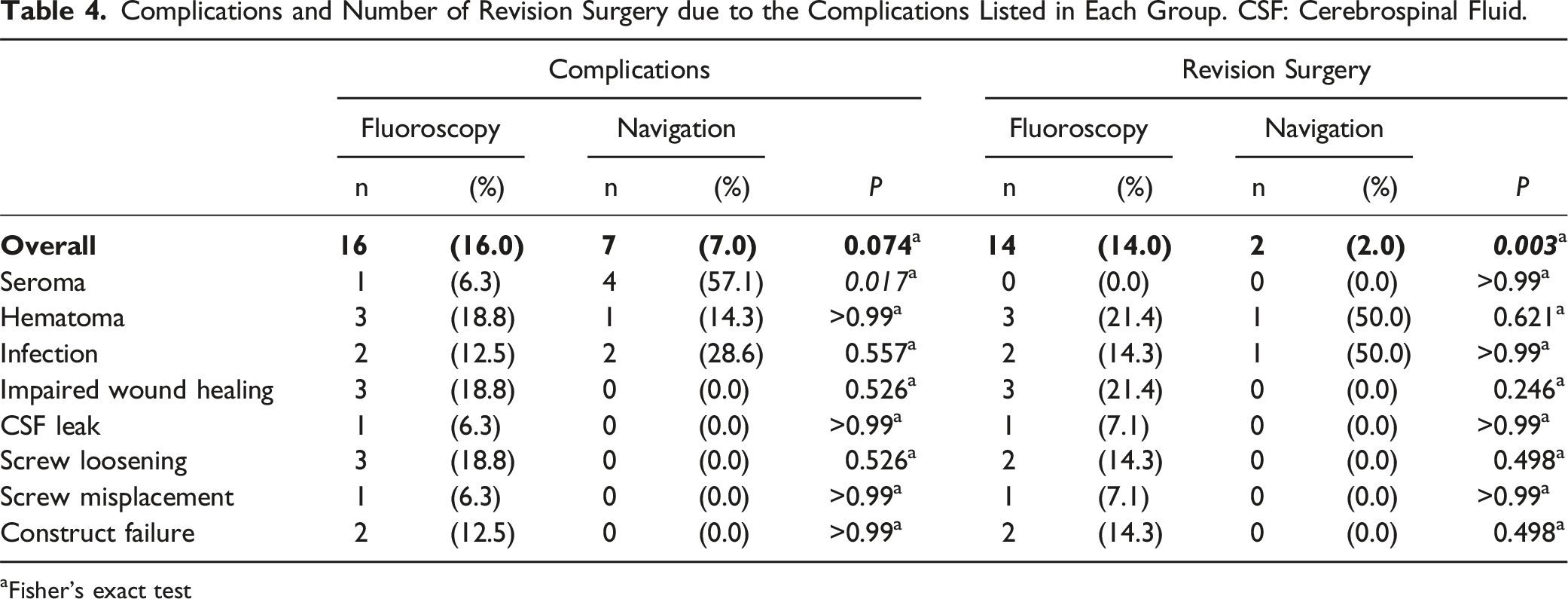
Fisher's exact test
Number and Objective of Scans in Both Groups.
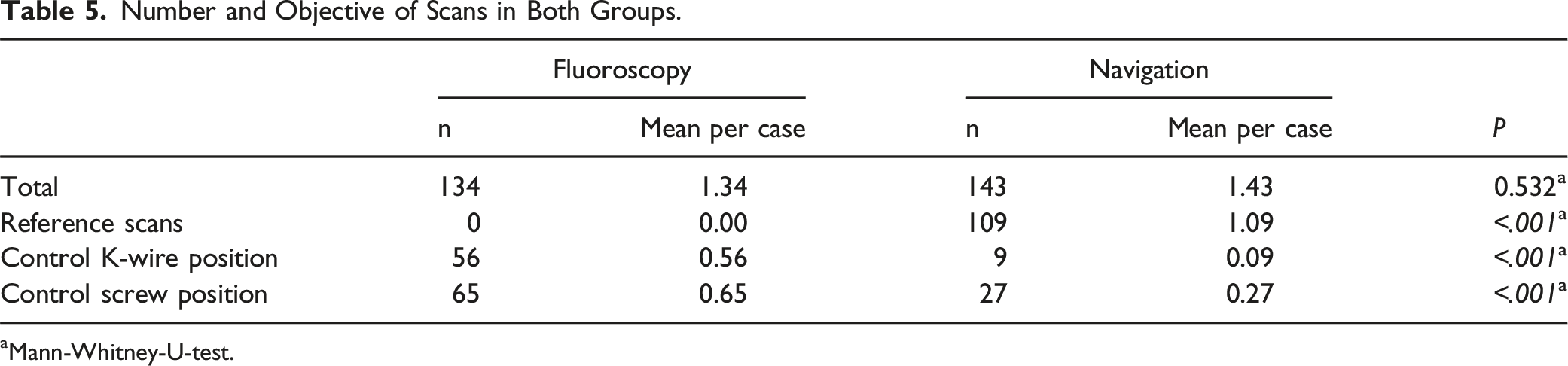
aMann-Whitney-U-test.
Dose area product (20,638 ± 15,586 mGy*cm2 vs 28,545 ± 17,693 mGy*cm2) and fluoroscopy time (92.3 ± 39.7 s vs 223.6 ± 93.6 s) were significantly lower in the navigation group compared to the fluoroscopy group (P < .001, respectively; Mann-Whitney-U-test). Furthermore, the mean duration of the surgical procedure was significantly lower in the navigation group (119.7 ± 48.7 min) compared to the fluoroscopy group (154.0 ± 81.0 min; P = .004).
Discussion
This study aimed to investigate the SPR for fluoroscopy based and navigated pedicle screw placement in the thoracic and lumbar spine. To the authors' knowledge, this is only the second study with a relevant number of cases to show that the use of navigation allows for the placement of significantly larger screws while simultaneously achieving significantly higher screw placement accuracy. As a consequence of this study, navigation is increasingly used at our institution, particularly in cases with potential risk factors for reduced biomechanical stability, such as poor bone quality from known or suspected osteoporosis.
The results presented complement the existing literature insofar as the navigated technique not only leads to more accurate screw placement but also appears to enable the selection of more appropriate screw diameters. 13 This advantage of navigation over fluoroscopy guided screw placement does not appear to be compensated for by additional intraoperative 3D imaging when using fluoroscopy. Upon closer per level analysis, four levels (T1, T2, L4, L5) showed high accuracy rates and relatively small SPRs in both groups. These results suggest that both imaging modalities are suitable for pedicle screw placement in the respective vertebrae due to the large pedicle size. 14 Navigation showed especially high accuracy in the mid to lower thoracic spine, despite consistently higher SPR compared to the fluoroscopy group.
The analysis also showed that the advantages of navigation were especially evident in percutaneous procedures and that the likelihood of perforation increased in both groups with increasing SPR.
A previous study compared pedicle screw placement using 2D fluoroscopy with additional 3D imaging and sole standard 2D fluoroscopy, reporting improved accuracy with the latter. 15 In contrast to the present study, the authors did not consider navigated screw placement. The higher accuracy rates for fluoroscopic guidance with additional 3D imaging may be due to the difference in levels instrumented, as the present study more screws in the critical thoracic region, where accuracy is typically lower. 16 In addition, the authors did not evaluate SPR, which should be taken into account when comparing accuracy rates. Also, the majority of perforations in both groups occurred laterally.
Lateral perforations are associated with a lower risk of clinical symptoms, which is why some authors deliberately place screws in the so-called “in-out-in” technique, thus accepting perforation of the pedicle. 17
Luther et al 13 investigated the accuracy of navigated and non-navigated pedicle screw placement as well as SPR for both groups. In their analysis of 1434 screws across all spinal regions they found that navigation allowed screws to be placed with a significantly higher accuracy, even though relatively larger screws were used. These – results that align with the present study. A different study comparing 45 navigated patients with 45 fluoroscopy guided matched controls also reported significantly larger SPR and higher accuracy in the navigation group. The study also identified a correlation between SPR and severe perforations, which is consistent with the current findings.
Recommended screw diameters in the literature vary from 80%–125% depending on the insertion technique. 18 Biomechanical considerations by various authors suggest that a higher SPR improves stability.9,10,19 The results presented by Hirano et al 20 suggest that meticulous care should be taken for osteoporotic bone regarding the selection of screw size as density and thickness of the pedicle cortex are reduced and risk of pedicle perforation may be increased. In these cases, cement augmentation may enhance pullout force. 21 Solitro et al found a correlation between higher SPR and greater pull-out strength, with optimal fixation at an SPR of 0.83. 22 In this study, SPRs of 0.85 ± 0.17 (fluoroscopy group) and 0.88 ± 0.21 (navigation group) indicate appropriate screw sizing. Still, determination of the minimal pedicle width in CT scans is not trivial and some deviation should be considered. 23 12 navigation and 2 fluoroscopy cases were revision surgeries with implant removal and re-instrumentation, requiring larger screws and highlighting the need for accurate initial placement to avoid repositioning with a subsequent decrease of stability. 7
The analysis of complications showed no statistically significant difference between the groups but more revision surgeries were performed in the fluoroscopy group. In addition, screw loosening was not observed in the navigation group while there were three cases in the fluoroscopy group of which two required revision surgery. This supports the hypothesis that higher SPR offers clinical advantages in terms of stability. Furthermore, one revision surgery had to be performed in the fluoroscopy group due to screw mispositioning, while no revision surgery due to inadequate screw position had to be performed in the navigation group. Overall complication rates align with previous studies, though revision rates in the fluoroscopy group were notably higher, possibly because Shuman et al 24 did not report revisions due to screw loosening, construct failure, or mispositioning.
This study found higher accuracy and SPR in the navigation group, with significantly less radiation exposure, despite more 3D scans. However, the rationale for acquiring the scans was different. In the fluoroscopy group, scans were performed mainly for implant verification, while in the navigation group, they served as reference scans for navigation. When comparing with other studies, variations in data collection, imaging, and surgical techniques must be considered. Still, previous research supports that navigation reduces radiation exposure compared to conventional methods.4,25
More importantly, navigation has been reported to reduce radiation exposure to surgical personnel in spine surgery, who are exposed to significant amounts of radiation over the years. 26 This is consistent with the authors' experience, as personnel are outside the control area during scan acquisition. Mendelsohn et al 27 reported lower surgeon exposure but higher patient exposure with navigation, differing from the present findings – possibly due to different dose protocols and routine intraoperative 3D imaging in the fluoroscopy group, increasing patient exposure.
This study found significantly shorter operating times in the navigation group. Another study observed no statistically significant difference but noted a trend toward shorter times with navigation. 11
Limitations
The results presented should be interpreted in the context of this study’s limitations. The results may not be generalizable because the design of this study was a retrospective, single-center analysis, and no clinical follow-up was performed for the sake of this study. Nevertheless, a retrospective review of the patient records was performed for follow-up clinic visits and inpatient readmissions with potential complications and revisions.
In addition, the study population consisted primarily of patients with traumatic injuries and a small number of oncologic and spondylodiscitis cases. Therefore, the results may not be applicable to patients with high-grade deformities; however, several studies have shown similar results with superiority of spinal navigation in deformity surgery.28-30
Analysis of demographic data showed that the navigation group had a higher proportion of male patients, whereas the fluoroscopy group had a higher proportion of female patients. This difference in gender distribution is most likely due to chance and does not affect the objective of the study. The navigation group had a higher number of re-instrumentation surgeries and disc replacements than the fluoroscopy group, presumably because navigation was favored for re-instrumentation surgery, since previous screw canals are displayed more clearly during instrumentation. This should be taken into account when interpreting the results regarding operating time. However, the overall case numbers are large, and the group data were rather similar. In addition, results reported in the literature support the findings presented.
Conclusion
The results of this study demonstrate that intraoperative navigation allows for more accurate pedicle screw placement and larger pedicle screw diameters compared to fluoroscopy with additional 3D imaging, which may provide biomechanical advantages.
At the same time, operating time and intraoperative radiation dose were not negatively affected by navigation. This relationship was particularly evident in the midthoracic region and in percutaneous procedures.
Supplemental Material
Supplemental Material - Analysis of Screw/Pedicle-Width Ratio and Accuracy in Navigated Versus 3D-Controlled Fluoroscopy-Guided Pedicle Screw Placement
Supplemental Material for Analysis of Screw/Pedicle-Width Ratio and Accuracy in Navigated Versus 3D-Controlled Fluoroscopy-Guided Pedicle Screw Placement by Jula Gierse, Felix Zimmermann, Paul A. Grützner, Jan Stallkamp, Sven Y. Vetter, and Eric Mandelka in Global Spine Journal.
Footnotes
Acknowledgments
We thank Ursula Trinler PhD for providing statistical advisory.
Author Contributions
Jula Gierse: Data acquisition, analysis and interpretation of data, writing of the manuscript. Felix Zimmermann: Data acquisition, manuscript revision. Paul A. Gruetzner: Conception and design, manuscript revision. Jan Stallkamp: Conception and design, manuscript revision. Sven Y. Vetter: Conception and design, manuscript revision. Eric Mandelka: Data acquisition, analysis and interpretation of data, writing of the manuscript. All authors have read and approved the final version of the manuscript.
Declaration of conflicting interests
PAG reports a relationship with Siemens Healthineers that includes: consulting or advisory and travel reimbursement. The research group received grants/has grants pending and technical support from Siemens Healthineers (Erlangen, Germany) and Nuvasive Inc. (San Diego, CA, USA). The funders had no involvement in the study design, collection, analysis, and interpretation of data, writing of the manuscript, or decision to submit the manuscript for publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval Statement
The study was reviewed and approved by the responsible Ethics Committee (application number 2020-15452). All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Data Availability Statement
All data and statistics are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.