
Abstract
Study Design
Systematic review and meta-analysis.
Objectives
Determine if tobacco use is associated with increased risk of postoperative adverse events within 90 days in patients undergoing spinal fusion surgery.
Methods
Databases were queried to identify cohort studies that directly compared smokers with non-smokers and provided the absolute number of adverse events and the population at risk. Data quality was evaluated using the Quality in Prognosis Studies tool. Risk ratios (RR) and 95% confidence intervals were calculated and compared between studies. The grading of recommendation, assessment, development and evaluation (GRADE) criteria were used to assess the strength of the evidence.
Results
Seventeen studies assessing 37 897 participants met the inclusion criteria. Of these, 10 031 (26.5%) were smokers and 27 866 (73.5%) were nonsmokers. The mean age for the study population was 58 years, and 45% were males. Smoking was not associated with increased risk of one or more major adverse events within 90 days following spine surgery (seven studies, pooled RR 1.13, 95% CI [.75-1.71], I2 = 41%). However, smoking was significantly associated with one or more major adverse events in ≤2 level fusion (three studies, pooled RR 2.46, 95% CI [1.18-5.12], I2 = 0%), but not in fusions of ≥3 levels (four studies, pooled RR .87, 95% CI [.70-1.08], I2 = 0%). Additionally, there was no statistically significant association between smoking and any adverse event, nor increased reoperation risk due to adverse events.
Conclusions
In this meta-analysis, tobacco use was not associated with a statistically significant increased risk of adverse events within 90 days in patients undergoing spinal fusion surgery. Our results are limited by the variable reporting methodology for both complication rates as well as smoking incidence between the included individual studies.
Introduction
The use of tobacco products is widespread globally and is considered one of the most significant public health threats by the World Health Organization, killing more than eight million annually. 1 The harmful health effects from nicotine and other toxins are far-reaching and multi-organ dependent, causing both local as well as systemic microtrauma secondary to a myriad of inflammatory mechanisms. 2
Smoking increases the risk of various adverse surgical outcomes, including mortality, infection, and poor wound healing.3-6 Tobacco smoking status has been previously associated with poor outcomes after spine surgery in particular, including increased rates of nonunion, 7 adjacent segment disease,8,9 reoperation, 9 and postoperative disability. 10 The process by which smoking may result in such adverse events has been proposed to be secondary to osteoporotic degeneration and decreased disc tissue perfusion; however, the full mechanism has yet to be elucidated.11,12 This has led most spine surgeons to strongly adhere to smoking cessation protocols, which most commonly consist of smoking cessation for at least 4 weeks prior to surgery. 8 In a similar fashion, most hospitals and surgery centers will consent patients for nicotine testing the morning of surgery in order to determine if it is safe to proceed with the procedure.
While there is well-documented evidence that smoking confers deleterious effects on spine surgery outcomes,7,10,13,14 the scope and magnitude of adverse events remain controversial.15-17 Most compiled evidence is derived from retrospective cohort studies. The purpose of this meta-analysis is to determine if tobacco use is associated with an increased risk of adverse events within a 90 days period after cervical or thoracolumbar fusion surgery.
Methods
Protocol and Registration
This work was registered with PROSPERO (CRD42021255534). 18 The study was conducted following the framework outlined by the Cochrane Prognosis Methods Group19,20 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 21
Identification of Studies
Multiple databases were searched including MEDLINE (PubMed), EMBASE (Ovid), Cochrane Central Register of Controlled Trials, and Cochrane Database of Systematic Reviews from inception to April 30, 2021. Supplementary Table S1 in the supplemental material describes the search strategy. In addition to the electronic searches, reference lists of systematic reviews and included studies were reviewed for additional articles. The search was restricted to articles published in English.
Assessment of Eligibility
The titles and abstracts were screened independently by two of the authors to identify articles for full-text review. Citations were retrieved if deemed appropriate for inclusion by at least one of those authors. Each full-text article was independently reviewed for eligibility by the same two authors. Any disagreements were resolved by consensus.
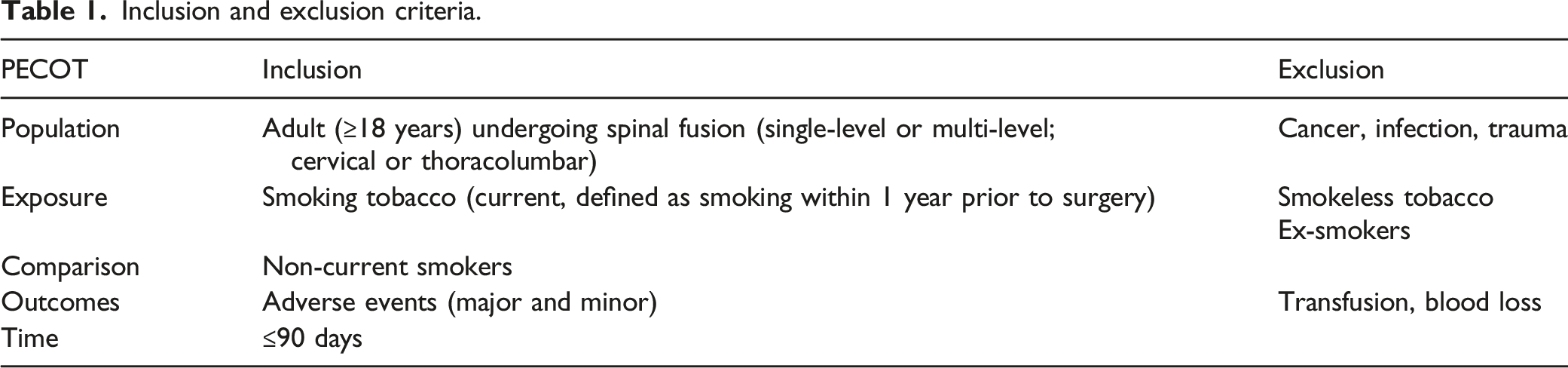
Inclusion and exclusion criteria.
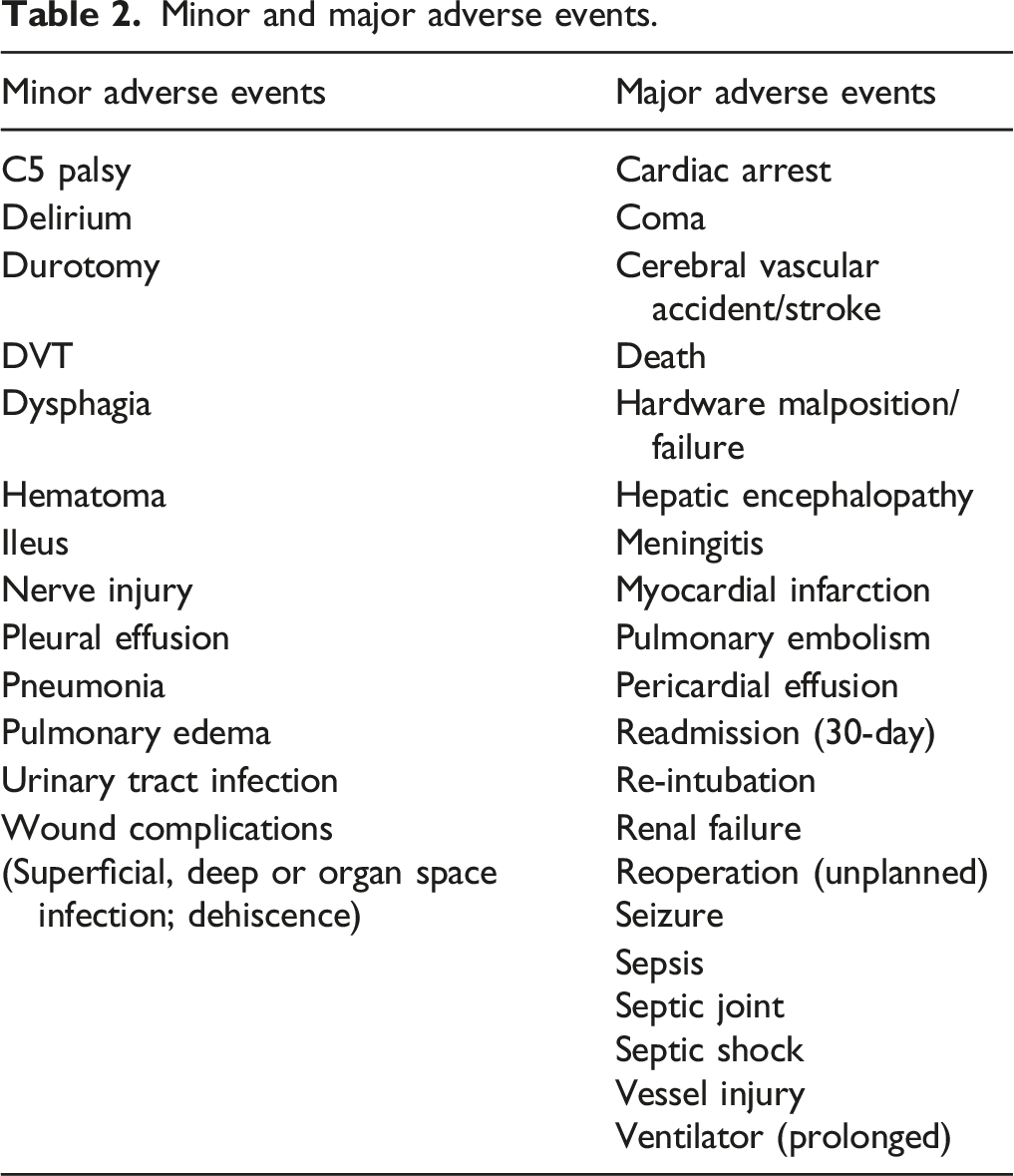
Minor and major adverse events.
Only cohort studies that directly compared smokers with non-smokers and provided the absolute number of adverse events and the population at risk were included. Prognostic studies that looked at several risk factors for adverse events that included smoking in a multivariate analysis but did not list the number of adverse events or the population at risk were excluded.
Data Abstraction and Data Management
Date from each study was extracted into an Excel spreadsheet (Microsoft, Redmond, WA). Data included: author last name, publication year, study design, country, sample size, population characteristics, data source, location and levels of fusion, surgical approach, follow-up time, and adverse events. Adverse events were not extracted as “zero” unless explicitly listed as such in the study report.
Assessment of Methodological Quality of Individual Studies
The risk of bias from these observational studies was determined using the “Quality in Prognosis Studies” (QUIPS) tool. 22 QUIPS evaluates six domains: study participation, study attrition, prognostic factor measurement, outcome measurement, study confounding, statistical analysis, and reporting, Supplementary Material Supplementary Table S2. Studies were judged as “good quality” when the majority of criteria were met (little or no risk of bias); “fair quality” if most criteria were met (some flaws in the study with an associated risk of bias); “poor quality” if either most criteria were not met, or if significant flaws relating to critical aspects of study design were present. 23 The same authors who extracted the data independently assessed the risk of bias and quality, and disagreements were resolved through consensus.
Data Synthesis
A meta-analysis was conducted when at least two studies reported similar adverse events. Results were pooled for specific major adverse events and those with one or more major and one or more minor adverse events via the Mantel-Haenszel method using a random-effects model. Risk ratios (RR) and 95% confidence intervals were calculated. All data analysis and presentation were performed using Review Manager 5. Heterogeneity was inspected by examining forest plots and subsequently quantified using the I2 statistic from the Chi-squared test for heterogeneity (I2 < 40, low heterogeneity; I2 ≥ 75% considerable heterogeneity). Stratified analyses were conducted to investigate whether effects varied by surgical location (cervical or thoracolumbar) or the number of segments fused (≤2 or >3 levels) when data was available. Procedures involving >3 segments of fusion were considered to be of higher complexity than those involving ≤2 levels, therefore this stratified analysis was performed in-line with the majority of screened studies reporting length of segmental instrumentation. The risk of bias due to missing results was examined qualitatively, given the relatively few studies in the meta-analyses. Sensitivity analyses were performed to investigate whether study quality influenced effect estimates by repeating the analyses excluding studies deemed poor quality.
The strength of evidence was evaluated using the GRADE working group criteria to assess evidence regarding prognostic factors. 24 According to GRADE, a body of observational evidence for questions of prognosis begins as high certainty in the evidence. The evidence can be downgraded due to the risk of bias, imprecision, inconsistency, indirectness, and publication bias. Upgrading also applies when estimates of associations between prognostic factors and outcome are robust. The strength of evidence was assigned an overall grade of high, moderate, low, or very low by evaluating and weighing the combined results of the above domains, Supplementary Material Supplementary Table S3.
Results
Study Selection
The search identified 6060 citations. A total of 5727 titles/abstracts were screened and, after removing 333 duplicates, 33 full texts were evaluated for study inclusion. Seventeen studies15,16,25-39 assessing 37 897 participants met inclusion criteria, Figure 1. Articles excluded at full-text review and reason for exclusion are listed in Supplementary Material, Supplementary Table S4. Preferred reporting items for systematic reviews and meta-analyses flowchart outlining the search and review process used to identify and select articles for inclusion in this systematic review.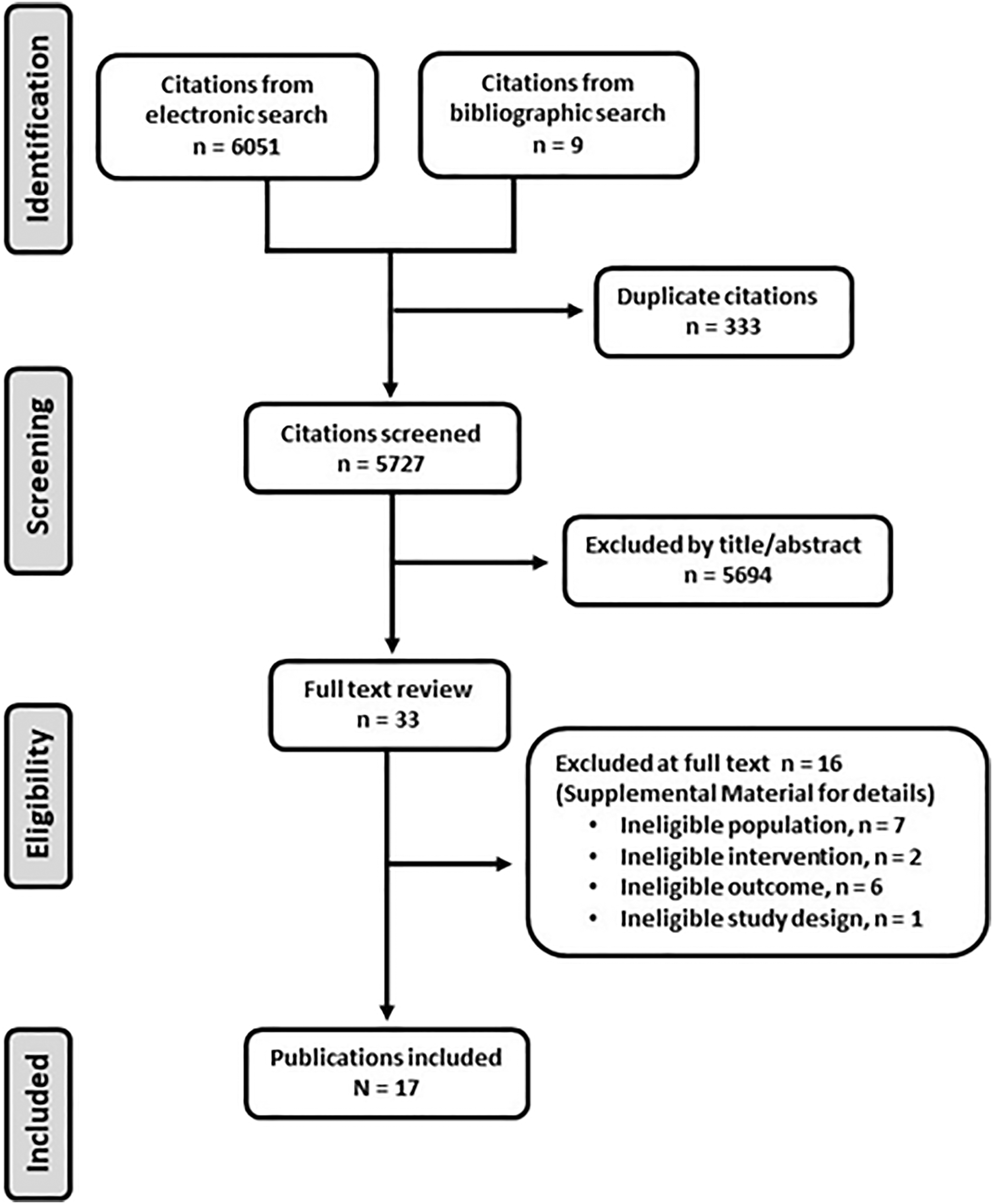
Study Characteristics
Characteristics of included studies.

NR, not reported; NS, nonsmoking; S, smoking.
Study Quality
Four studies were judged as good-quality,16,27,34,39 five as fair-quality15,25,29,32,35 and eight as poor-quality studies.26,28,30,31,33,36-38 The concerns about bias in the studies were primarily related to three domains: outcome measurement, lack of control for confounding, and high or uncertain study attrition.
Adverse Events
Any Major Adverse Events
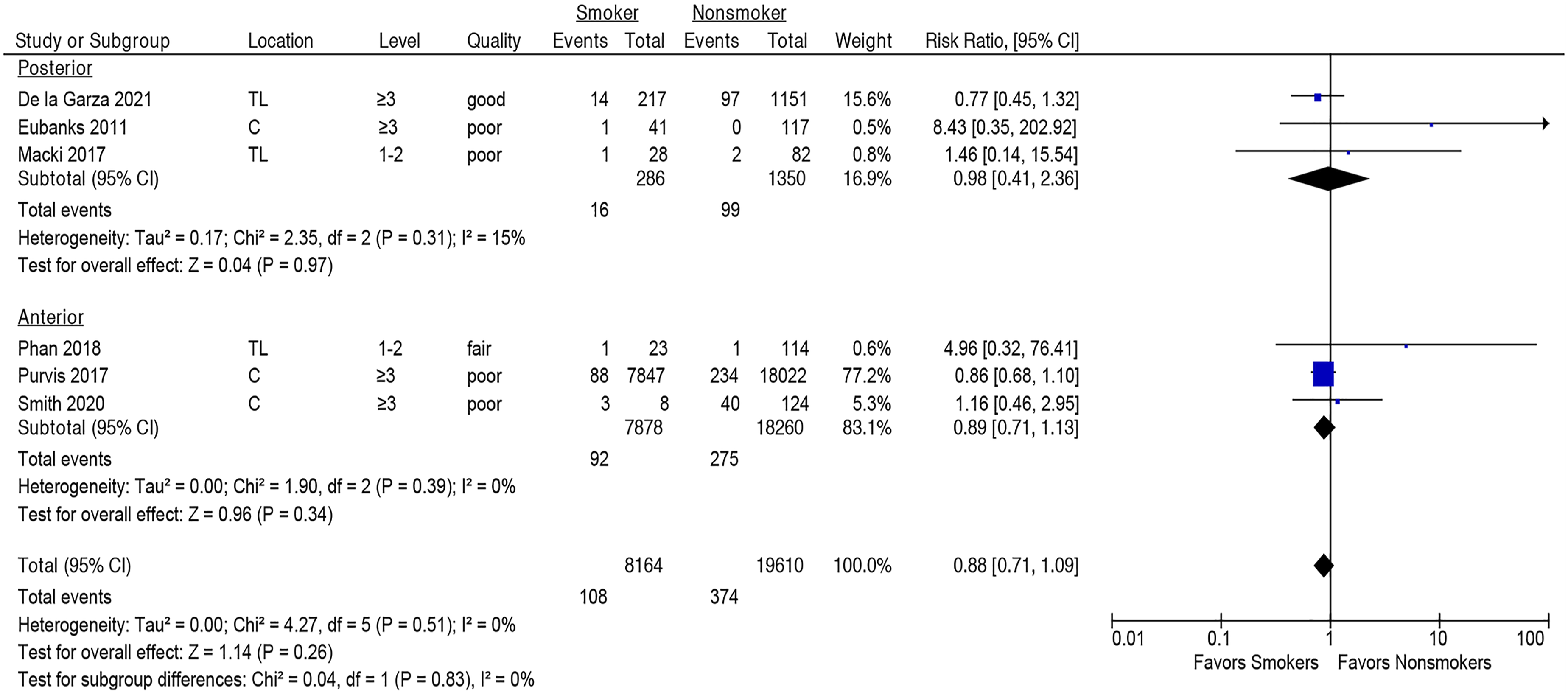
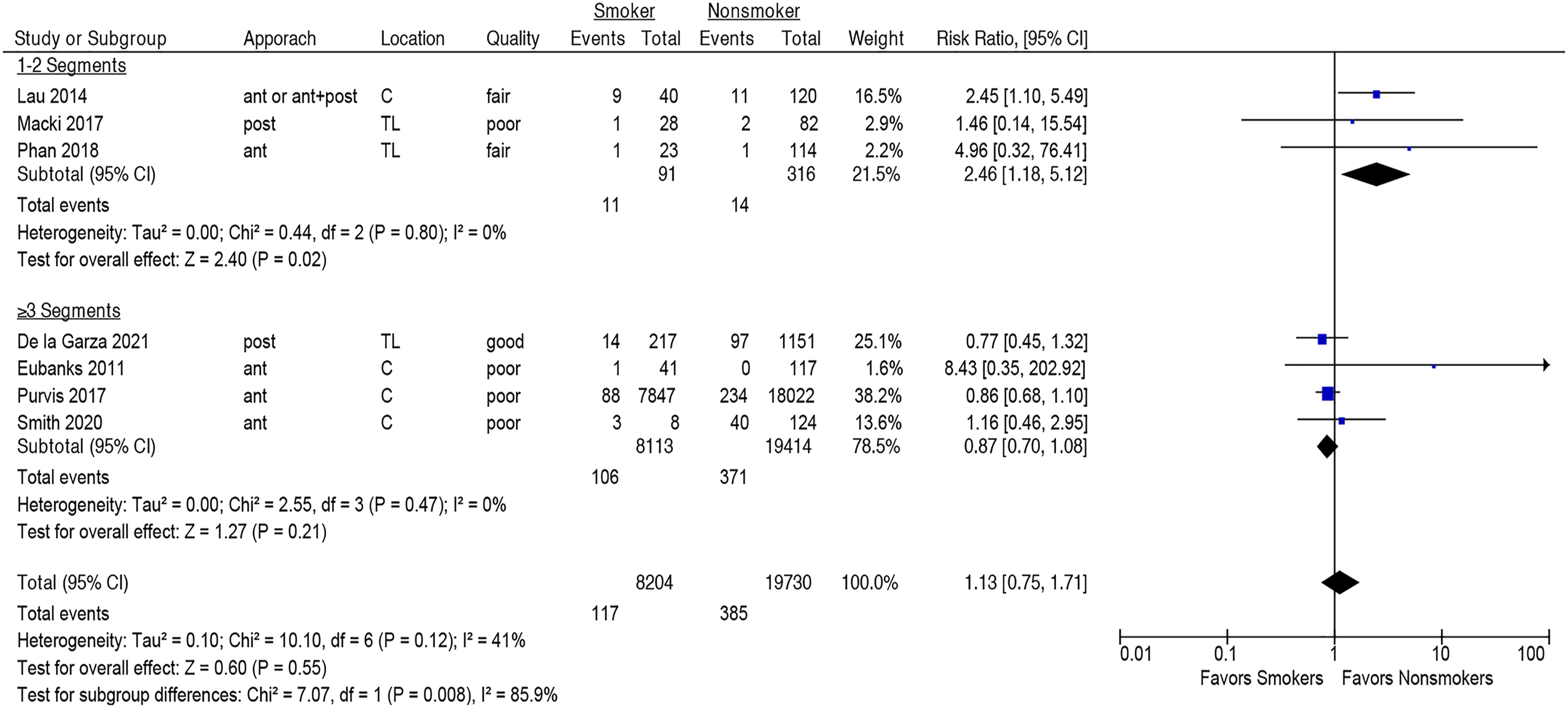
Smoking was not associated with increased risk of one or more major adverse events within 90 days following spine surgery (seven studies, pooled RR 1.13, 95% CI .75-1.71, I2 = 41%) Figure 2 (Strength of Evidence, MODERATE, Supplementary Table S5). This lack of association was seen both in the cervical spine (four studies,28,32,36,38 pooled RR 1.36, 95% CI [.69-2.68], I2 = 62%) and the thoracolumbar spine (three studies,16,33,35 pooled RR .84, 95% CI [.50-1.42], I2 = 0%), Figure 2, and both in the posterior (three studies,16,28,33 pooled RR .88, 95% CI [.41-2.36], I2 = 15%) and anterior approaches (three studies,35,36,38 pooled RR .89, 95% CI [.71-1.13], I2 = 0%), Figure 3. However, smoking was significantly associated with one or more major adverse events in ≤2 level fusion (three studies,32,33,35 pooled RR 2.46, 95% CI [1.18-5.12], I2 = 0%), but not in fusions of ≥3 levels (four studies,16,28,36,38 pooled RR .87, 95% CI [.70-1.08], I2 = 0%); subgroup difference, P = .008, Figure 4. In the sensitivity analysis, smoking was not associated with an increased risk of one or more major adverse events when four poor-quality studies were excluded, Supplementary Figure S1. Association between smoking and risk of one or more adverse events within 90 days following spine surgery. Association between smoking and risk of one or more adverse events within 90 days following spine surgery as compared between posterior and anterior approaches. Subgroup analysis of the association of smoking and risk of one or more adverse events within 90 days following spine surgery between ≤2 level and ≥3 level fusions.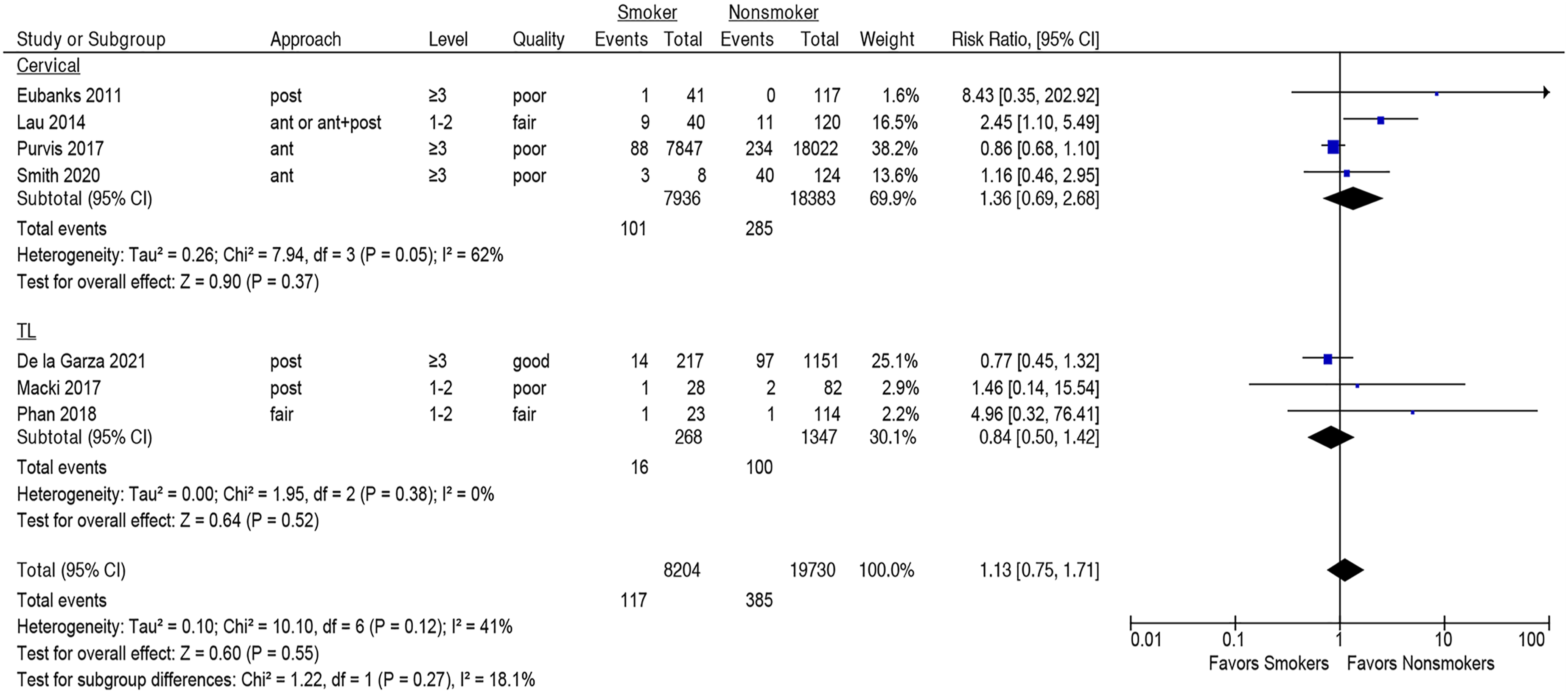
Any Adverse Events (Major or Minor)
There was no significant association between smoking and any adverse events (one or more major or minor adverse events) within 90 days following spine surgery (six studies,16,25,26,36,38,39 pooled RR .99, 95% CI [.77-1.29], I2 = 65%), Figure 5 (Strength of Evidence, LOW, Supplementary Table S2). There were no differences in the subgroup analyses stratifying by surgical location or approach (Supplemental Material, Supplementary Figures S2 and S3) or when omitting three poor-quality studies in the sensitivity analysis, Supplementary Figure S4. Association between smoking and risk of any adverse event within 90 days following spine surgery.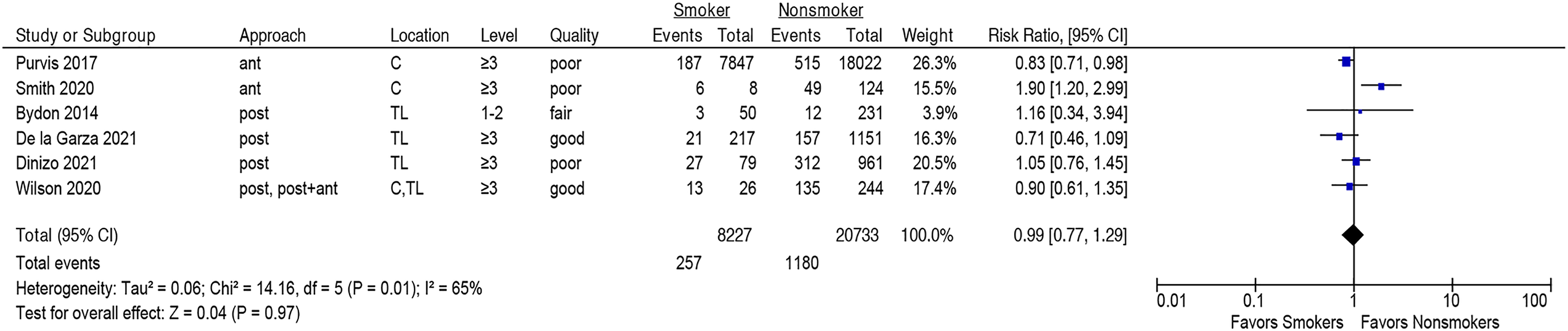
Wound Adverse Events
Smoking tended to be associated with more frequent wound adverse events, though this observed association was not statistically significant (nine studies,15,16,25,27,29,31,33,35,39 pooled RR 1.43, 95% CI [.95-2.16], I2 = 14%), Figure 6 (Strength of Evidence, MODERATE, Supplementary Table S2). There were no differences in subgroup analyses stratifying by surgical location or number of segments fused, Supplementary Figures S5 and S6. The results were unchanged in the sensitivity analysis when two poor-quality studies were omitted, Supplementary Figure S7. Association between smoking and risk of wound adverse events following spine surgery.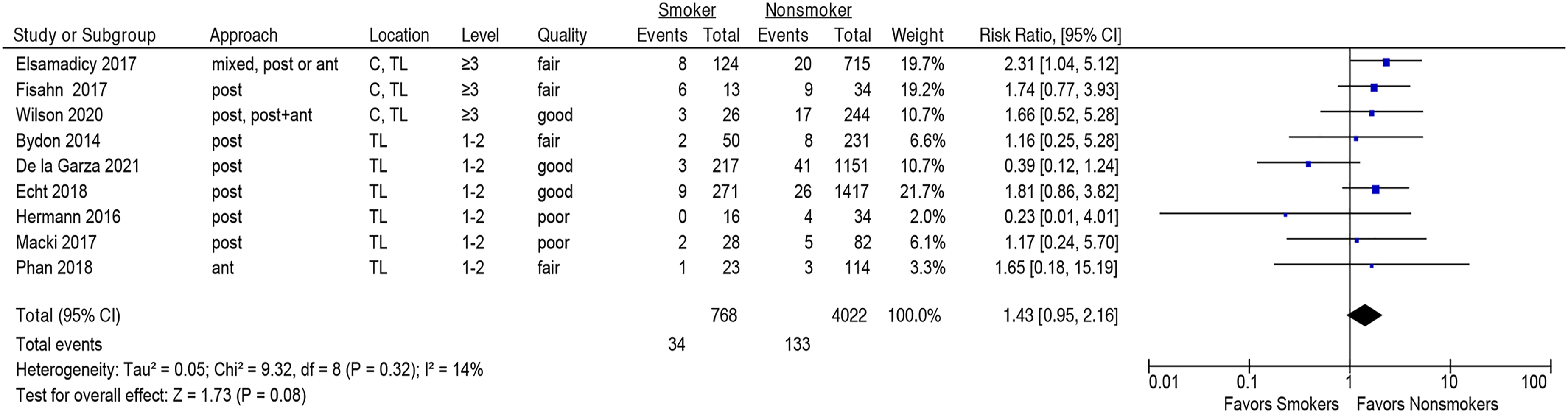
Reoperation due to Adverse Events
Smoking tended to be associated with increased reoperation risk, though the association failed to reach statistical significance (seven studies,16,28,30,32-34,36 pooled RR 1.37, 95% CI [.98-1.91], I2 = 18%), Figure 7 (Strength of Evidence, LOW, Supplementary Table S2). There were no differences in subgroup analyses stratifying by surgical location or number of segments fused, Supplementary Figures S8 and S9. The results were unchanged in the sensitivity analysis when four poor-quality studies were omitted, Supplementary Figure S10. Association between smoking and risk of reoperation.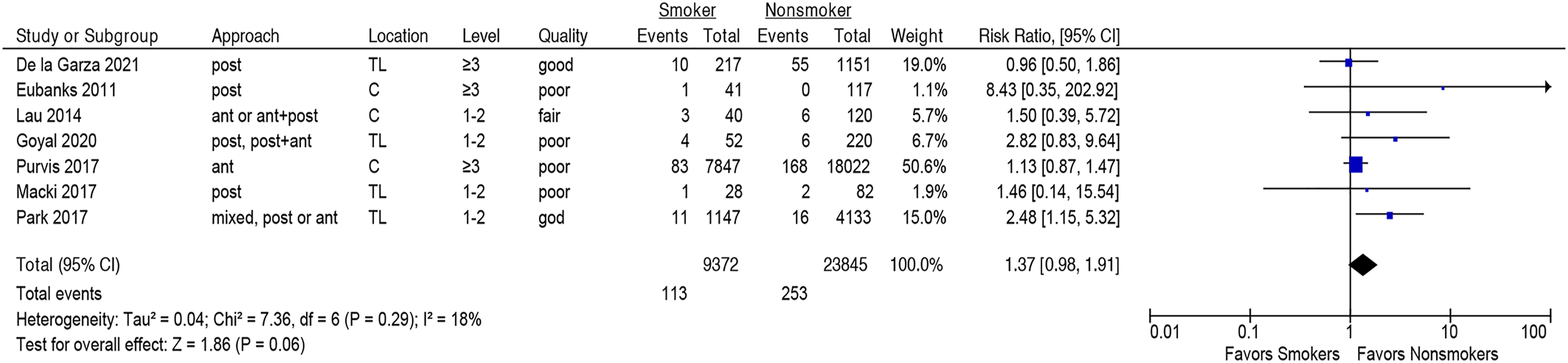
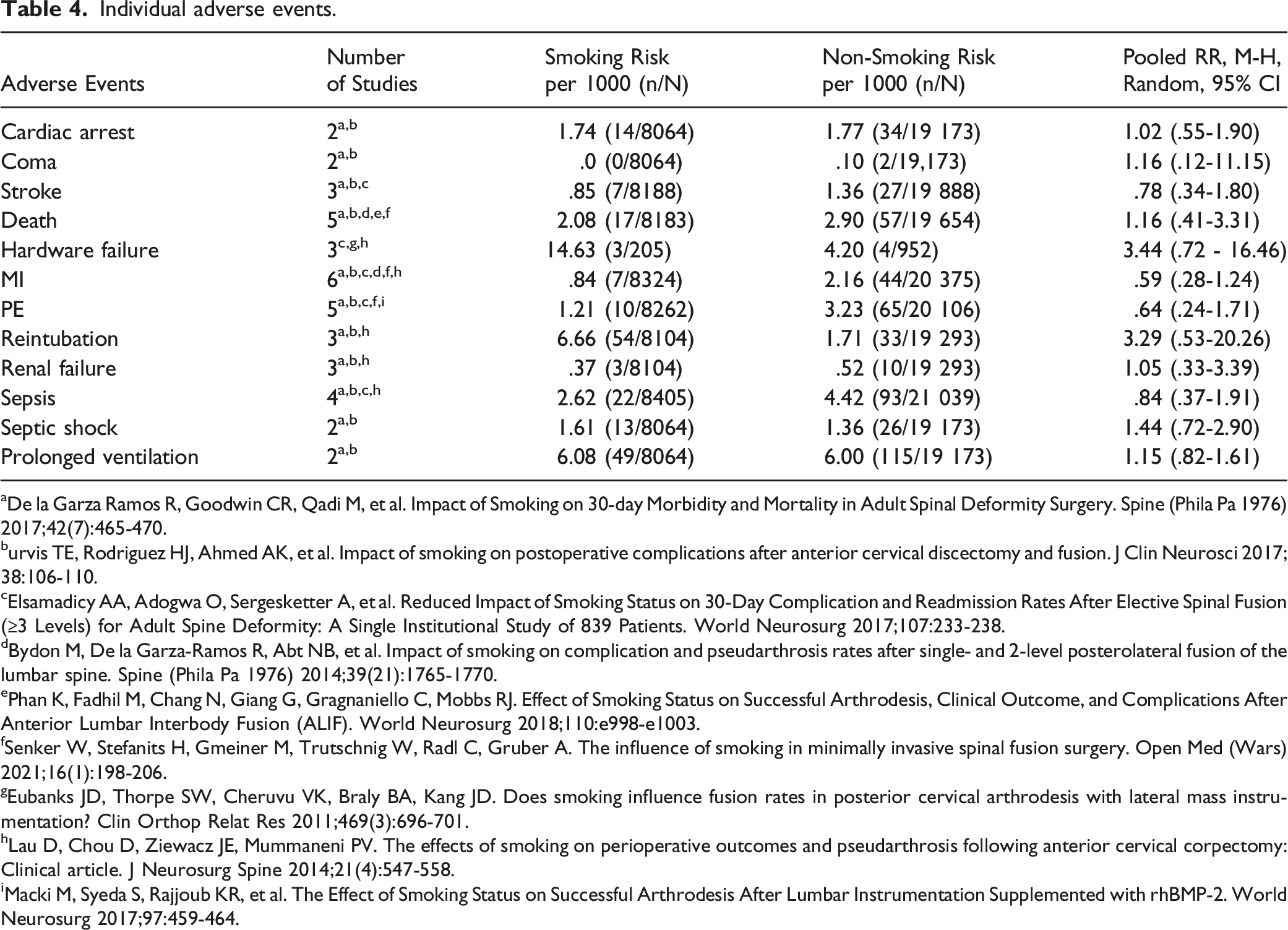
Individual Major Adverse Events
Individual adverse events.
aDe la Garza Ramos R, Goodwin CR, Qadi M, et al. Impact of Smoking on 30-day Morbidity and Mortality in Adult Spinal Deformity Surgery. Spine (Phila Pa 1976) 2017;42(7):465-470.
burvis TE, Rodriguez HJ, Ahmed AK, et al. Impact of smoking on postoperative complications after anterior cervical discectomy and fusion. J Clin Neurosci 2017;38:106-110.
cElsamadicy AA, Adogwa O, Sergesketter A, et al. Reduced Impact of Smoking Status on 30-Day Complication and Readmission Rates After Elective Spinal Fusion (≥3 Levels) for Adult Spine Deformity: A Single Institutional Study of 839 Patients. World Neurosurg 2017;107:233-238.
dBydon M, De la Garza-Ramos R, Abt NB, et al. Impact of smoking on complication and pseudarthrosis rates after single- and 2-level posterolateral fusion of the lumbar spine. Spine (Phila Pa 1976) 2014;39(21):1765-1770.
ePhan K, Fadhil M, Chang N, Giang G, Gragnaniello C, Mobbs RJ. Effect of Smoking Status on Successful Arthrodesis, Clinical Outcome, and Complications After Anterior Lumbar Interbody Fusion (ALIF). World Neurosurg 2018;110:e998-e1003.
fSenker W, Stefanits H, Gmeiner M, Trutschnig W, Radl C, Gruber A. The influence of smoking in minimally invasive spinal fusion surgery. Open Med (Wars) 2021;16(1):198-206.
gEubanks JD, Thorpe SW, Cheruvu VK, Braly BA, Kang JD. Does smoking influence fusion rates in posterior cervical arthrodesis with lateral mass instrumentation? Clin Orthop Relat Res 2011;469(3):696-701.
hLau D, Chou D, Ziewacz JE, Mummaneni PV. The effects of smoking on perioperative outcomes and pseudarthrosis following anterior cervical corpectomy: Clinical article. J Neurosurg Spine 2014;21(4):547-558.
iMacki M, Syeda S, Rajjoub KR, et al. The Effect of Smoking Status on Successful Arthrodesis After Lumbar Instrumentation Supplemented with rhBMP-2. World Neurosurg 2017;97:459-464.
Discussion
Despite a detailed understanding of its long-term deleterious effects, tobacco use remains the most common cause of preventable morbidity in the United States. 40 Cigarette smoking has been linked with higher rates of complications, delayed recovery time, and poorer functional outcomes in surgical patients. 4 The known impacts of tobacco use on normal physiological functions such as inflammation have resulted in widespread efforts to curb its use.40,41 The increasing population of spine surgical patients both in recent times and in the projected future renders the consideration of tobacco exposure especially relevant. Although the relationship between preoperative smoking and postoperative complications has been studied extensively in the context of bony fusion, 7 abdominal surgery, 42 and surgical patients in general, 43 to our knowledge, our systematic review and meta-analysis is the first to compare smokers to non-smokers in spinal fusion surgery directly and to quantify the relative risk differences for individual and aggregates of complications between these groups. We sought to understand (1) the specific complications associated with smoking in individuals undergoing spinal fusion, as well as (2) the degree to which the risks for these complications differed.
Wound Complications
Surprisingly, in the present analysis, smokers undergoing fusion were not associated with a statistically significant higher risk for developing wound-related complications when compared to non-smokers. Further, upon aggregating studies based on location (ie, cervical and thoracolumbar vs thoracolumbar alone), surgery location was not found to be an effect modifier of smoking on risk for wound complications. Smoking induces chronic inflammation and impairs normal wound healing processes, among other negative impacts on overall health. 44 It is hypothesized that surgical site organ trauma in the setting of tobacco-induced damage may impart additional risk for perioperative complications. 4 Studies have shown that smokers have impaired immune function with increased risk of infection, 45 as well as a decreased rate of collagen production, 46 both of which negatively influence the wound healing process. It has been suggested that the deleterious effect of smoking cessation is at least partially reversible, including the associated wound-healing complications. 47 In the present meta-analysis, only the study by Elsamadicy et al demonstrated a significant difference in smokers vs non-smokers regarding wound-related complications, and overall heterogeneity was low (I2 = 14%, Figure 6).
Reoperation
Although most studies reporting reoperation rates tended to show higher rates of reoperation in smokers than non-smokers, the overall effect failed to reach significance (RR 1.37, 95% CI 0.98 to 1.91). Similarly, stratification by region of spinal surgery (ie, cervical vs thoracolumbar) and overall number of levels operated upon lacked statistical significance. Importantly, even though the pooled analysis did not reach significance, the included studies, by and large, showed little heterogeneity in their tendency to report smaller proportions of reoperations in non-smokers (I2 = 18%, Figure 7).
Several studies have evaluated smoking on reoperation in spine surgery and other surgical disciplines. Reoperation, in the short term, may commonly be attributed to occurrences of complications such as wound infections, dehiscence, implant malposition, or other acute findings that necessitate surgical exploration.48,49 At longer follow-up, in addition to the reasons described above, factors such as the development of secondary instability, adjacent segment disease, deformity, or pseudarthrosis may necessitate revision procedures. 48 For example, the impact of smoking on pseudoarthrosis rates following spinal fusion at months to years of follow-up has been well documented. 7 It is plausible that any mechanisms by which smoking predisposes patients to any of the above or alternative causes of reoperation would manifest themselves in a significant association between smoking and reoperation. Intriguingly, such a relationship was not evident in our meta-analysis, although this may be due to sample size limitations.
Any Major or Minor Adverse Events
Preoperative smoking has been implicated as a predictor of adverse outcomes in disciplines such as abdominal surgery, 50 cosmetic procedures, 51 thoracic surgery, 52 and several other surgical fields. 53 Published meta-analyses comparing perioperative outcomes between smokers and non-smokers in the surgical literature suggest that the drivers of increased complication rates in smokers are pulmonary, infectious, or cardiovascular complications. 53 Interestingly, the influence of smoking is not well-defined in every surgical discipline, especially when considering complications other than wound disruption/dehiscence or surgical site infection. Systematic reviews of the head and neck surgery literature, for example, have suggested that tobacco smoking carries a negative impact on perioperative outcomes. However, depending on the specific research methodology and inclusion criteria, statistically significant associations often cannot be established.54,55 In our analysis, we similarly did not find significant associations between major or minor adverse events with smoking status, even when considering individual events, such as pulmonary complications. Notably, surveillance methodology for specific postoperative adverse events is highly variable between studies, with inconsistent reporting of screening strategies, definitions of complications, or unspecified follow-up.
In our analysis of individuals undergoing spinal fusion procedures, there was overall no association between smoking status and the occurrence of any minor or major adverse events within 90 days. While we did identify a significant association between smoking and adverse events in fusions of ≤2 levels, this finding did not persist following a sensitivity analysis that excluded low-quality data. Because the effect of smoking has been studied in numerous individual articles in spine surgery and systematic reviews of studies in other fields, findings in the literature vary widely, from those demonstrating nonsignificant differences to those showing larger effect sizes.39,50,51,53
Strengths and Limitations
The present analysis has several strengths and limitations. While prior meta-analyses have examined the effect of smoking on complications in surgery in general, we performed the first comprehensive systematic review of the spine-specific surgical literature and identified all papers in the English language reporting complications as stratified by smoking status, thereby permitting us to calculate risk differences and quantify effect sizes of smoking on specific complications. The advantage of limiting our scope to spine surgery is reflected in the relatively small degree of heterogeneity in our primary findings. Aggregation of these studies allowed us to perform several subgroup analyses for certain complications as stratified by spinal segment or levels operated upon, and appraisal for quality of evidence permitted sensitivity analyses to exclude low-quality data.
Limitations of this analysis include its reliance upon retrospective studies, which may affect the number and types of reported complications based on the respective authors' definitions and screening criteria. Although we defined “current smoking” as smoking within a year whenever the data was available, in the vast majority of cases, we relied upon the authors of the original articles for their definitions of current vs non-smoker, in the case of individuals who had quit smoking. Similarly, we were unable to explore a dose-response relationship between the extent of cigarette smoking and the effect on complication rates if any such relationship exists. The same goes for alternate delivery modalities for nicotine intake, such as patches, gum and vaping devices Transparent and consistent definitions of current smoking status, abstinence, and reporting for specific complications are necessary for future cohort studies to examine outcomes more clearly in this population.
Conclusion
In this meta-analysis, smokers undergoing spinal fusion procedures in general were not at greater risk for most complications within a 90-day period compared to non-smokers. Our results are limited by the variable reporting methodology for both complication rates as well as smoking incidence between the included individual studies. Further cohort studies directed at this point should clearly define nonsmoking status as well as rates of specific complications experienced in those undergoing spinal fusion procedures.
Supplemental Material
Supplemental Material - The Risk of Adverse Events in Smokers Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis
Supplementary Material for The Risk of Adverse Events in Smokers Undergoing Spinal Fusion: A Systematic Review and Meta-Analysis by Ravi S. Nunna, Darius Ansari, Philip B. Ostrov, Joseph R. Dettori, Periklis Godolias, Elias Elias, Max Gruber, Rod J. Oskouian, and Jens R. Chapman in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.