
Abstract
Study Design
Retrospective Case-control Study.
Objectives
To determine the requisite exercise compliance (EC) of physiotherapeutic scoliosis-specific exercise (PSSE) for achieving curve regression; to analyze whether the apical translation (AT), apical wedging (AW), and apical rotation (AR) of the major curve improve with regression effect.
Methods
Between 2019 and 2021, a total of 763 patients undertook a 6-month PSSE treatment. This resulted 426 compliable and 302 uncompliable patients remained available for analysis. For compliable patients, 213 with curve regression and 213 age-/sex-matched with curve stabilization/deterioration at the 6-month, were eligible for regression analysis to detect the relationship between EC and regression effect at the 6-month; receiver operating characteristic (ROC) curve analysis and Youden’s index were applied to identify the threshold of EC leading to curve regression at the 6-month. The AT, AW, and AR of the major curve were compared before and after 6-month PSSE to investigate the radiographic parameters that improved with regression effect.
Results
EC was correlated with regression effect (odds ratio: 19.9, 95% confidence interval: 11.3-35.0, P < .001) and the cutoff threshold of EC was 4.4 h/week for 6 months to realize such an effect. AT was improved by 47.6% with curve regression, in which 152 cases remained curve regression and no case progressed into the operative threshold at the 1.5- to 2-year.
Conclusions
A 6-month PSSE protocol of 4.4 hours per week was potentially leading to curve regression in treating mild to moderate scoliosis. An improvement in AT of the major curve was observed with the regression effect.
Keywords
Background
Adolescent idiopathic scoliosis (AIS) is the most common form of structural scoliosis with unknown etiology and is characterized by vertebral deformity in three dimensions. 1 Surgery is reserved for severe curves exceeding 50°, whereas bracing and physiotherapeutic scoliosis-specific exercise (PSSE) are used for preventing curve progression. 2
Studies have reported curve regressions after PSSE in treating mild to moderate scoliosis, with compliance noted as a crucial factor associated with significant improvement.3-8 However, exercise protocols have varied widely in those studies and have been reported using a percentage value of the prescribed dosage, yet without correlation analysis. Thus, the relationship between exercise compliance (EC) and curve regression remains unclear. In addition, the COVID-19 pandemic has greatly affected hospital-visited treatments. Thus, having a PSSE program with appropriate EC to prevent curve progression while avoiding overtreatment is crucial.
PSSE reduces Cobb angles,4-6,8-12 alleviates asymmetrical truncal rotation (ATR)12-16and improves quality of life.3,17 AIS is presented by vertebral side-deviation, rotation and wedging, and is characterized by an apical vertebra with the most deformed in rotation. 18 Previous studies have not discussed the mechanism through which PSSE affects the morphology of deformed vertebrae. 3 Hence, the effects of PSSE on the change in apical translation (AT), apical wedging (AW), and apical rotation (AR) remain unknow. Understanding the mechanism through which PSSE remodels a scoliotic spine aids research and clinical practice. Thus, we hypothesized that EC of a 6-month PSSE program is correlated with curve regression in treating mild to moderate scoliosis, and we aimed to define a threshold leading to such an effect. Furthermore, we aimed to investigate the effects of PSSE on change in radiographic parameters after PSSE.
Materials and Methods
Patient Sampling
This was a retrospective, age-/sex-matched study with a balanced study design (sampling between regression and stabilization/deterioration was at a 1:1 ratio) to analyze the correlation between the EC and curve regression of patients undergoing 6-month PSSE without bracing between 2019 and 2021. This study was approved by the ethic committee of our hospital. The inclusion criteria were as follows: (1) idiopathic scoliosis; (2) adolescents aged ≥ 10 and < 17 years; (3) initial Cobb angle < 50°; (4) available spinal radiographs before and after the 6-month PSSE; (5) initial spinal radiographs for at most 1 month before commencing PSSE; (6) Risser stage ≤ 4; (7) no bracing before and during the 6-month PSSE; and (8) once-monthly supervised PSSE to review performed exercise. The exclusion criteria were as follows: (1) diagnoses other than AIS; (2) reported hypermobility on initial assessment (Beighton score ≥ 4) 19 ; (3) reported adherence to any other conservative treatments rather than the Schroth method; (4) atypical curve pattern. 20 In particular, the second exclusion criterion was set to control systematic bias from hypermobility influencing effects of physiotherapy. 21
PSSE Protocol and Compliance
The supervised PSSE comprised 1-h private sessions on workdays and 1-h group sessions on Saturdays. Each treatment comprised 50 breaths per exercise including: (1) active self-elongation with caudal-cranial spine lengthening in standing; (2) corrective exercise with shoulder counter traction and pelvic pulling strategy on the lumbar concavity in sitting/standing/side-lying; and (3) stabilization exercises, per the protocol of a previous study. 8 The positioning of home exercise (HE) was the same as supervised sessions. The HE comprised self-elongation and corrective exercises for 45-60 min daily. This HE protocol was associated with a significant reduction in Cobb angle after 6 months of Schroth therapy.8,11 Patients in this study completed at least once-monthly supervised PSSE session to review the performed exercise and maintain exercise quality. The supervised PSSE attendance of patients was collected from the hospital’s database. HE compliance, hours per day, was self-reported by patients on a treatment adherence checklist (Supplemental file). This checklist was auto sent to patients/parents every 2-week. For calculation, daily compliance was set to 0 if noncompliance indicated. The patient would be called to refill the from if no reply in a week after checklist sent.
Radiographic Outcome and Group Allocation
Patients had whole spine standing radiographs with arms at the sides of body to assess their curve magnitudes. Cobb angle, AT, AW, and AR of the major curves were independently measured by two spine surgeons who were blinded to this study. The inter- and intra-rater reliabilities of radiographic measurements were studied before group allocation to diminish mislabeling. Prior to correlation analysis, change in Cobb angles at the 6-month was compared between compliable and uncompliable patients. Compliable cohort was the patients completed once-monthly supervised PSSE for consecutively 6 months, this was for reviewing the performed exercise in every month to control exercise quality. Uncompliable cohort included patients undergoing only observation during the 6-month of treatment or did not complete once-monthly supervised PSSE for 6 months consecutively. Correlation analysis, the relationship between the EC and curve regression, would be conducted in the compliable cohort if a greater reduction of Cobb angle was detected with compliable patients. Compliable patients with a decrease of major coronal Cobb angle ≥ 6° were allocated into the regression group, while patients with a change < 6° or an increase ≥ 6° were allocated into the stabilization/deterioration group.
22
This definition of curve progression accounted for measurement error. The AR was graded as I to V using the Nash and Moe system (Figure 1).
23
AW was interpreted using the apical ratio (convex vertebral height/concave vertebral height; Figure 1).
24
AT was defined as the distance between the center of the apical vertebrae of the major curve and central sacral vertical line (Figure 1).
18
The curve classification was defined as either major thoracic curve (single right thoracic or a major right thoracic with a minor left lumbar) or major lumbar curve (single left lumbar, a major left lumbar with a minor right thoracic, or a thoracolumbar). Skeletal maturity was assessed by Risser signs with 0- referring to Risser sign 0 with open triradiate cartilage and 4+ referring capped iliac apophysis but not completely fused. One radiograph illustrating the measurements of apical translation (AT), apical wedging (AW) and apical rotation (AR). AT was defined as the distance in millimeter (dashed, horizontal yellow line) between the center of the apical vertebrae (T8: white round marker) and the central sacral vertical line (CSVL, solid vertical white line). AW was interpreted as the apical ratio equals convex vertebral height (solid, red vertical line on the T8 convexity) divided by concave vertebral height (solid, red vertical line on the T8 concavity) of the apical vertebrae. AR was graded as rotational I, II, III and V regarding the radiographic location of the pedicle on convexity of the apical vertebrae (three dashed, vertical white lines).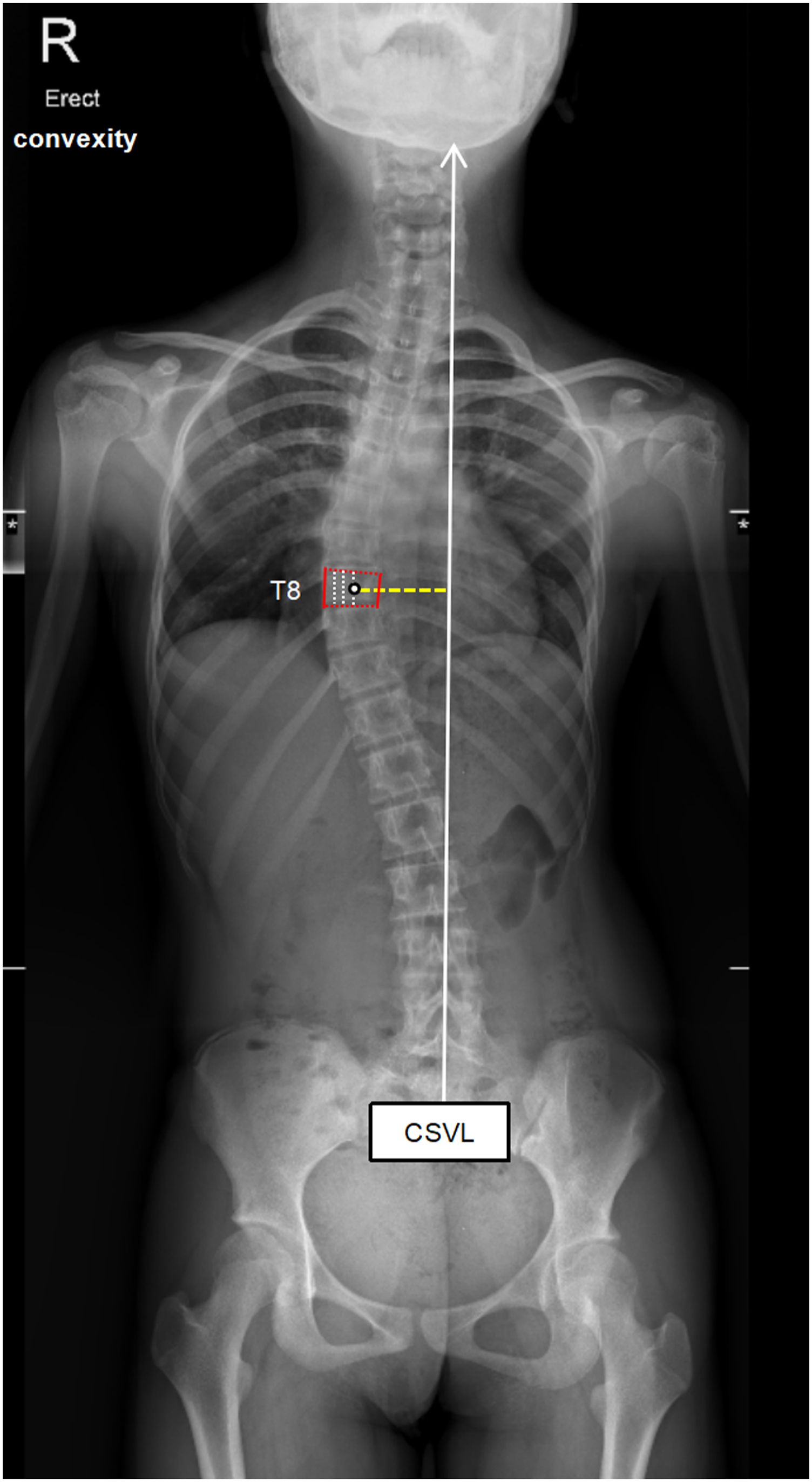
Statistical Analysis
Sample size estimation
This study adopted a balanced design. Thus, the curve regression prevalence (p) was .5; the events per variable (EPV) was set at 40; the failure rate (f) in data collection, such as EC of HE, was estimated to be 20%; and 4 features (k), namely the Risser sign, Cobb angle, curve pattern, and EC, were adopted for the logistic regression analysis (n = [EPV × k/p]/[1 − f]). Overall, 200 in each group were required for intergroup associations to be detected. 25
Data Analysis
Descriptive statistics were calculated for baseline demographic and radiographic data. Continuous variables were presented as mean ± standard deviation (SD) with and without median values depending on normality tests. The intraclass correlation coefficient (ICC) and Cohen weighted kappa (kw) were conducted to investigate the inter- and intra-rater reliability of radiographic outcomes. EC was documented in hours per week of 6 months. Continuous variables, including age, body mass index, initial Cobb angle, Lostein and Carlson risk of progression
The data were analyzed using SPSS version 20.0 (IBM, Chicago, IL). Significance was set at a two-tailed level of .05. The 95% confidence intervals (CIs) and respective odds ratios (ORs) were reported where appropriate.
Results
Patient Sampling
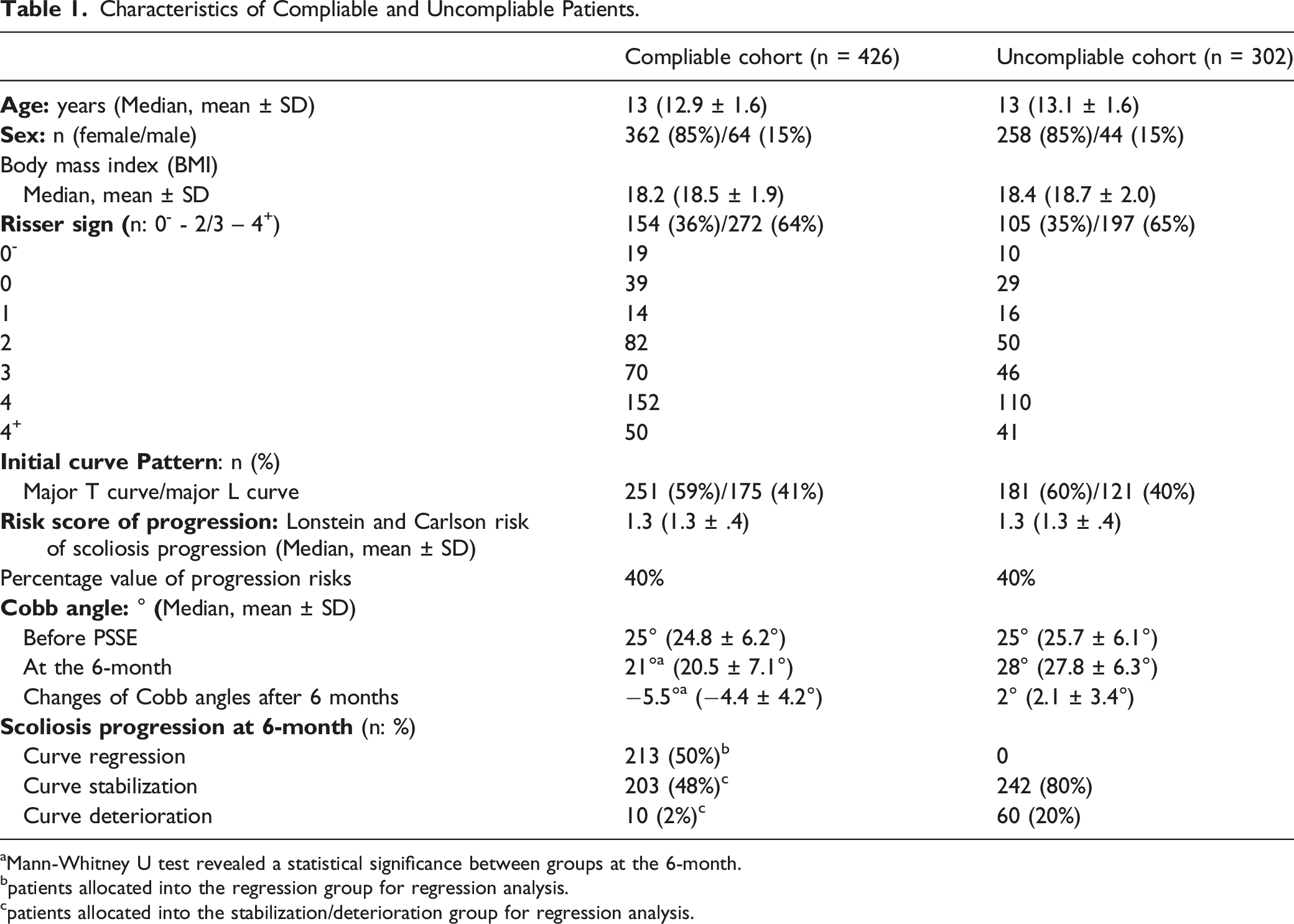
A total of 2072 patients with AIS were assessed for eligibility, of those, 1309 patients were excluded due to the following reasons (Figure 2): (1) they did not perform spinal radiographic assessment at the 6-month (n = 308); (2) their initial spinal radiography was not within 1 month before commencing PSSE (n = 304); (3) they undertook (n = 88) or initiated (n = 128) spinal orthotic treatment at their first consultation; (4) they reported hypermobility at initial assessment (n = 82); (5) they did not complete once-monthly supervised PSSE to review performed exercise (n = 302); (6) they underwent any other conservative treatment rather than the Schroth method during the 6 months of PSSE (n = 58). Consequently, 763 patients met the inclusion criteria, of those, 228 radiographs were randomly captured to test the reliability of radiographic measurements. The interrater reliability of Cobb angle (ICC = .98), AT (ICC = .90), AW (ICC = .95), AR (kw = .93) and Risser sign (ICC = 1.00) revealed a strong agreement between measurements; the intrarater reliability was also satisfactory (Cobb angle [ICC =1.0], AT [ICC = .92], AW [ICC = .87], AR [kw = .99] and Risser sign [ICC= 1.00]). After radiographic measurements, a total of 309 patients exhibited curve regression (reduction in Cobb angle by 6°–15°); 439 patients exhibited curve stabilization, and 15 patients exhibited curve deterioration by 6°–9° after 6-month PSSE. In total, 213 pairs/stratum of age- and sex-matched cases, with 4.4° of reductions compared to the uncompilable cohort (n = 302, 2.1° increase in Cobb angles at 6-month), remained available for correlation analysis (Table 1). Study flow chart. Characteristics of Compliable and Uncompliable Patients. aMann-Whitney U test revealed a statistical significance between groups at the 6-month. bpatients allocated into the regression group for regression analysis. cpatients allocated into the stabilization/deterioration group for regression analysis.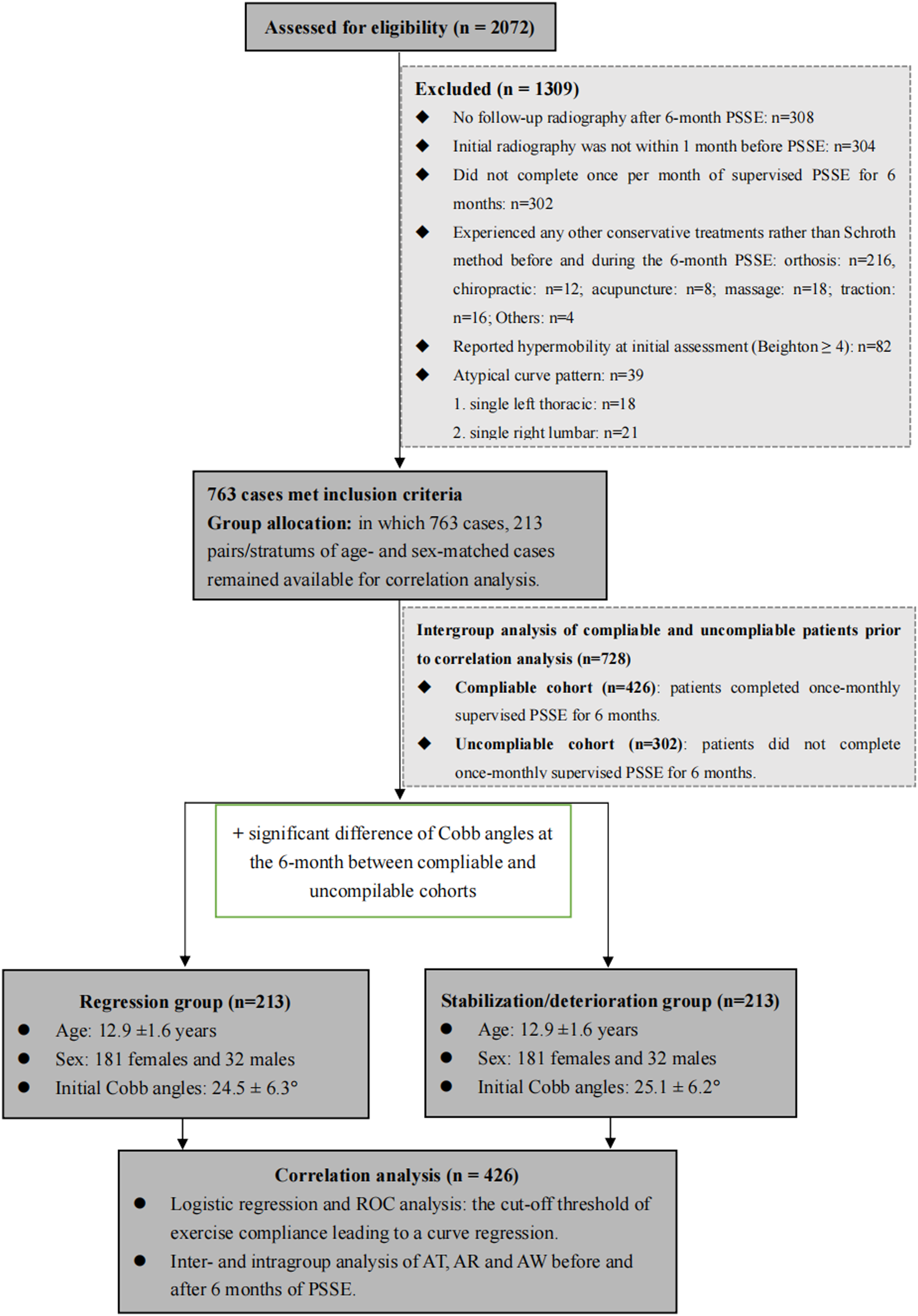
Threshold of EC With Curve Regression
Characteristics of Compliable Patients with Curve Regression and Stabilization/Deterioration.
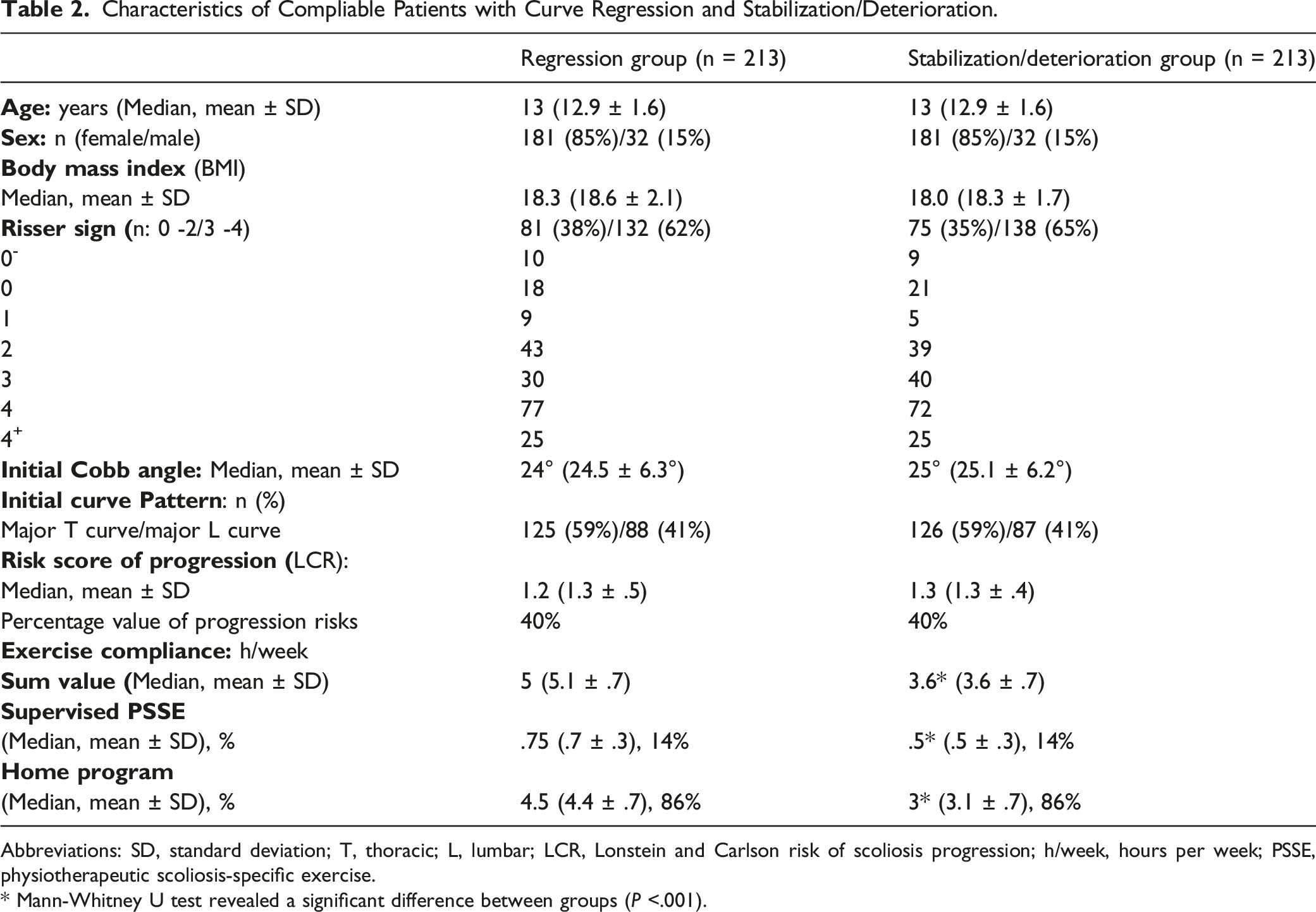
Abbreviations: SD, standard deviation; T, thoracic; L, lumbar; LCR, Lonstein and Carlson risk of scoliosis progression; h/week, hours per week; PSSE, physiotherapeutic scoliosis-specific exercise.
* Mann-Whitney U test revealed a significant difference between groups (P <.001).
Logistic Regression Analysis of Intergroup Associations Between Risk Factors with Exercise Compliance and Curve Regression after 6-month of Physiotherapeutic Scoliosis-Specific Exercise.
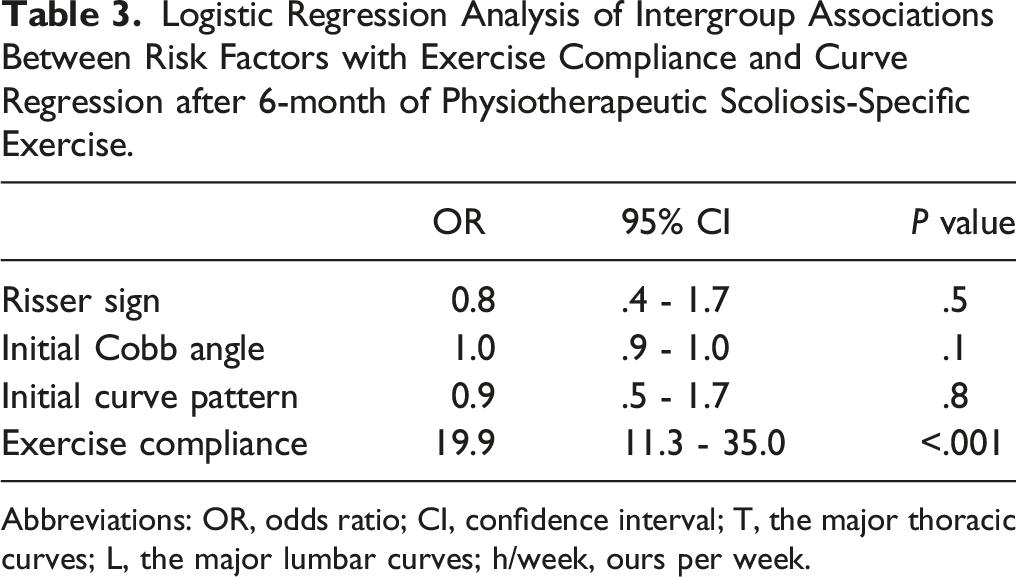
Abbreviations: OR, odds ratio; CI, confidence interval; T, the major thoracic curves; L, the major lumbar curves; h/week, ours per week.
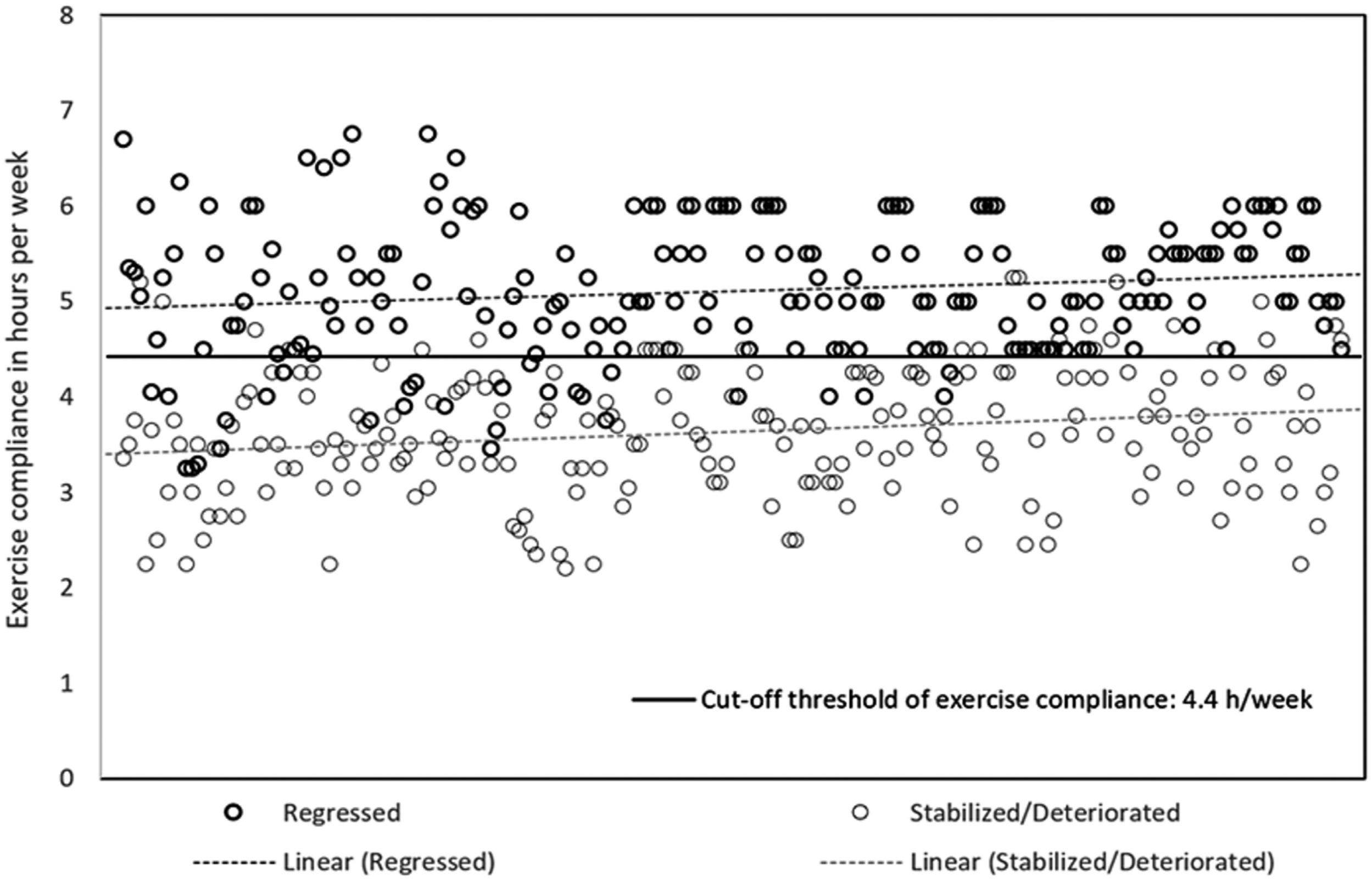
Exercise compliance in hours per week of 6 months. The cut-off threshold was 4.4 hours per week that led to a curve regression.
Radiographic Outcomes
Radiographic Parameters Before and After 6 Months of Physiotherapeutic Scoliosis-Specific Exercise Treatment.
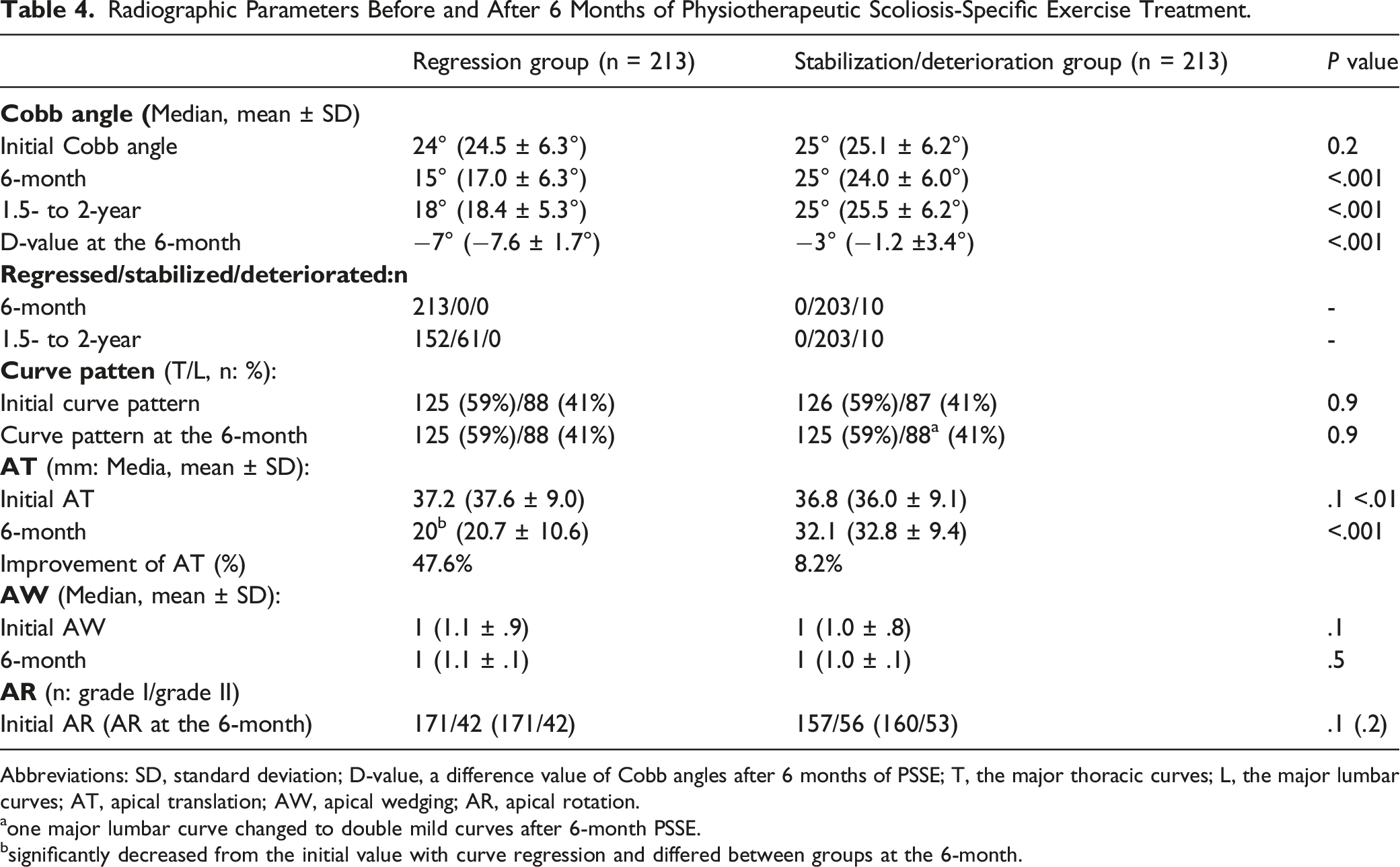
Abbreviations: SD, standard deviation; D-value, a difference value of Cobb angles after 6 months of PSSE; T, the major thoracic curves; L, the major lumbar curves; AT, apical translation; AW, apical wedging; AR, apical rotation.
aone major lumbar curve changed to double mild curves after 6-month PSSE.
bsignificantly decreased from the initial value with curve regression and differed between groups at the 6-month.
Discussion
Studies demonstrated the ability of PSSE to reduce the Cobb angle3,7-9,11,17; it is thus crucial to determine the EC realizes such a reduction. In addition, the effects of PSSE in changing vertebral monography remain unknown, understanding these effects can help researchers discover how PSSE remodels deformed vertebrae. This study defined the cutoff threshold of EC leading to curve regression and revealed that AT improved with the curve regression.
Our findings indicate that 4.4 h of PSSE per week for 6 months is the requisite EC to achieve curve regression with mild to moderate AIS. This finding differs from studies that have only demonstrated that better compliance influences better outcomes without a correlation analysis. 17 Moreover, the reduction of Cobb angle in those studies was noted within the measurement error.3,17 More recent PSSE studies have reported curve regression in mild to moderate scoliosis but with a variation in exercise protocols.4-6,8,11,13 In these trials, spinal orthosis was used with PSSE to treat AIS; thus, the outcome could be influenced by both bracing and exercise. Our study excluded patients with orthotic treatment, which limited the confounding effect of bracing. Two CCTs4,5 have reported a significant reduction by >5° for mild scoliosis, in which EC was related with curve regression, but the threshold of EC was not defined. Investigating this relationship is valuable because PSSE compliance varies between countries. 28 Our study filled this knowledge gap in the literature. Regarding the exercise protocol, daily PSSE for 30-45 min has been consistently prescribed in most studies, 29 and, thus, to achieve 4.4 h/week of PSSE, 45 min/day for 6 days would be a recommended exercise dose for patients undergoing PSSE treatment. Moreover, our study adopted a clinically significant change in Cobb angle by ≥6° to verify improvement, which is of clinical value because any change <5° is not considered a true improvement. 24 Additionally, our findings did not suggest that the effect of supervised PSSE was superior to home PSSE, although previous studies have reported this. 9 This might be because the compliance of supervised PSSE in this study was only 14% in each group. Hence, the effect of HE was underscored in this study. This observation suggests that one supervised session per month, where the aim is to review the exercise performed, with a PSSE program of 45 min/day for 6 days is a feasible PSSE protocol for treating AIS. However, it is possible for mild scoliosis to not progress regardless of interventions. 27 Thus, this exercise protocol may benefit patients in preventing overtreatment of supervised PSSE and lowering the costs; however, a cost-effectiveness study is required to reach a clearer conclusion. In addition, our study suggested that patients’ age did not influence the effects of PSSE in reducing Cobb angles. This differs from previous evidence. One study revealed a greater reduction of Cobb angles in patients ≥ 13 years doing active self-correction exercises. 5 Another study, on the contrary, found a greater reduction in patients < 13 years doing an alternative scoliosis-specific exercise named Xinmiao approach. 4 These differences might be introduced by varied exercise protocols. Thus, the correlation of age and PSSE in alleviating scoliosis requires future study to confirm.
Patients with curve regression exhibited a significant improvement of AT. Prior study explained that exercise can rebuild trunk symmetry with respect to ATR improvement, thereby altering spinal alignment.
30
One study evaluated the effect of PSSE with angular breathing technique on vertebral rotation, reporting a significant improvement in AR by .6° but the study ended at the 3-month.
31
Angular breathing is one practical technique of the Schroth method to open the curve concavity, derotate the asymmetrical ribcage, which may affect vertebral rotation.
30
However, no study has addressed the effect of PSSE on vertebral morphology including AT, AR and AW.
3
Our study filled this knowledge gap, providing clinicians with additional information regarding the benefits of PSSE in correcting vertebral side deviation. One thoracic curve (Figure 4A and B) achieved a 14° reduction, and one lumbar curve (Figure 4C and D) achieved a 10° reduction after PSSE. Those effects were presented with significant improvements in AT. This implies that PSSE balances spinal coronal asymmetry. However, curvature reducibility before PSSE could not be quantified in our analysis owing to the retrospective nature of our study. Nevertheless, our findings form a basis for defining the relationship of PSSE with defined curvature flexibility and curve regression in future studies. No changes in structural rotation and wedging were expected because vertebral morphology cannot be easily altered simply with exercise. However, vertebral rotation and wedging may be altered with prolonged PSSE if the external symmetrical forces can influence internal development during bone growth. However, the current evidence contains no information on such a relationship.
3
Furthermore, one patient exhibited a curve progression of 6° in the lumbar region and developed a mild thoracic curve of 20°. Thus, overcorrection may alter curve pattern. Nine patients with high progression risks gained 6°–9° in Cobb angles after 6 months. Hence, our finding of 4.4 h/week of PSSE may not be applicable for treating scoliosis with a high progression risk. Radiograph of two patients before and after 6-month PSSE. A: radiograph demonstrating a 36° thoracic curve (T4 to T11) with 44.1 mm of apical translation to the right before PSSE. B: radiograph revealing a 22° thoracic curve (T4 to T11) with 19.5 mm apical translation to the right PSSE while the rotation and wedging of the apical vertebrae (T8) remained unchanged. C: radiograph demonstrating a 36° lumbar curve (T12 to L4) with 37.9 mm of apical translation to the left before PSSE. D: radiograph revealing a 26° lumbar curve (T12 to L4) with 20.6 mm apical translation to the left after PSSE, while the rotation and wedging of the apical vertebrae (L2) remained unchanged. Abbreviation: PSSE, physiotherapeutic scoliosis-specific exercise.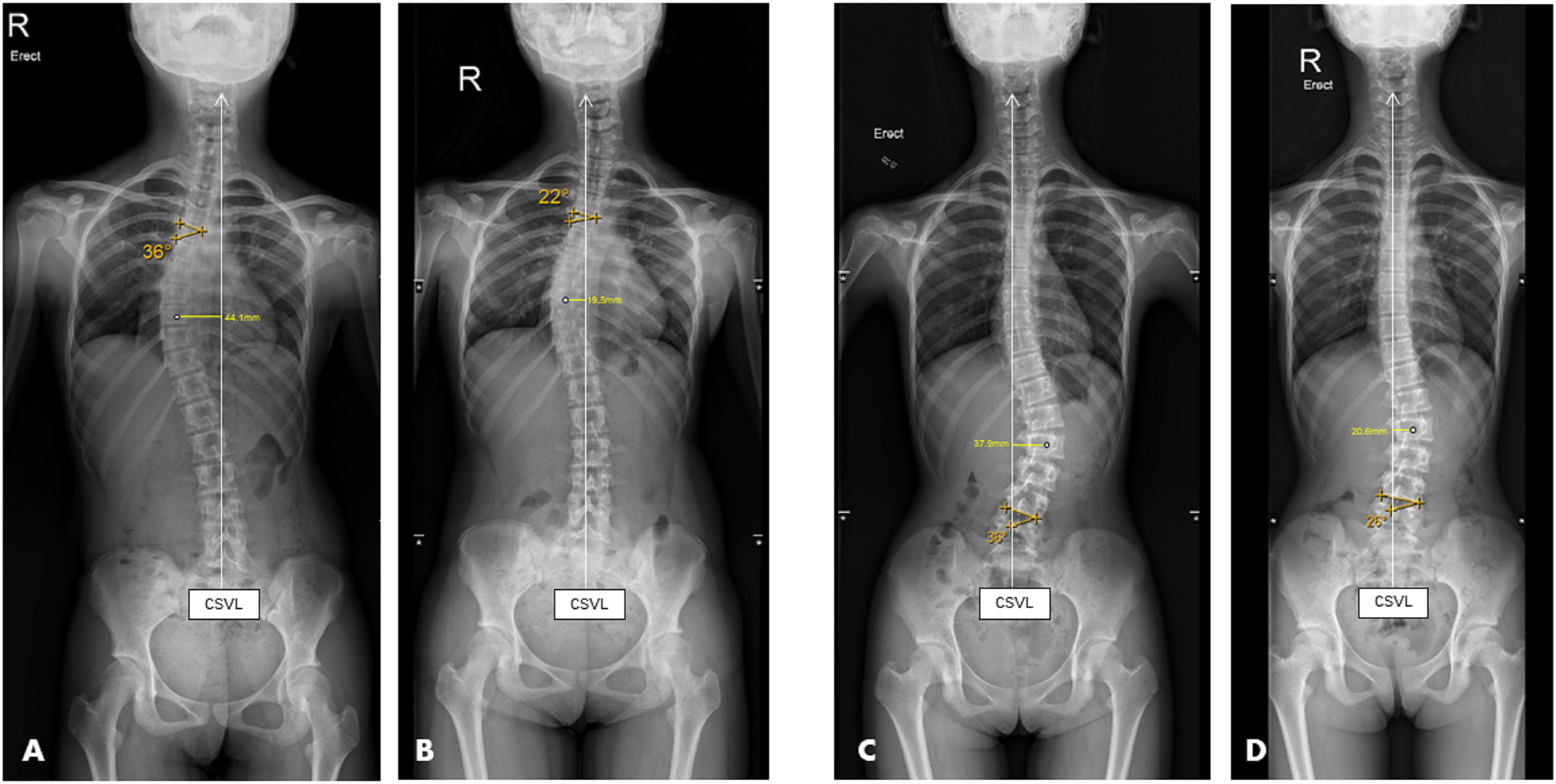
No curve deterioration was observed at the 1.5-year in patients with curve regression at the 6-month. Such regression had worn off and resulted in curve stabilization for 61 patients. This introduced a bouncing effect after PSSE. Nonetheless, 71.4% of patients, with curve regression at the 6-month, maintained curve regression and no one received operation at end of this study. This revealed a promising effect of 6-month PSSE in avoiding scoliosis deterioration.8,13 Like bracing in AIS, the rate of treatment success was 72% after bracing, as compared with 48% for observation only. 32 Thus, the efficacy of PSSE in alleviating scoliosis requires a prospective randomized trial with an observation only group as control to draw a conclusion. In the stabilization/deterioration group of this study, three patients, with a curve magnitude ≥ 42° at study initiation, received spinal fusion at the 2-year. This implies that a 6-month long of PSSE might not being effective in treating severe scoliosis. 3
Because of the retrospective nature of this study, baseline variances could not be completely controlled. Firstly, the initial Cobb angle was <30° and presented with progression risk < 50% in this study cohort. Hence, the threshold defined cannot be applied to patients with severe scoliosis or high progression risks. This might be caused by the exclusion of cases with orthotic treatment. Regarding the Scoliosis Research Society guideline, 2 moderate scoliosis with high progression risks should start orthosis at interventional initiation. In this study, we excluded patients with bracing, which eliminated the confounding effect of bracing. Secondly, self-compliance for PSSE can be uncertain like that of bracing and may lack accuracy. One study reported the bracing compliance rate to average 88% while the compliance monitor device only reported 33%. 33 Thus, reporting of compliance to HE can be variable according to the prescribed amount of time, what the patient reports, what the parents say, and the actual time of doing HE. Hence, self-reported compliance introduced internal recall bias in this study. However, given to the compliance was collected every 2-weeks, the recall bias was externally limited. Lastly, this study excluded numerous cases. Nonetheless, this was a controlled and homogeneous study, and confounding effects were eliminated; thus, the effect of PSSE was more accurately captured.
Supplemental Material
Supplemental Material - The Relationship Between Compliance of Physiotherapeutic Scoliosis Specific Exercises and Curve Regression With Mild to Moderate Adolescent Idiopathic Scoliosis
Supplemental Material for The Relationship Between Compliance of Physiotherapeutic Scoliosis Specific Exercises and Curve Regression With Mild to Moderate Adolescent Idiopathic Scoliosis by Yunli Fan, Michael KT To, Guan-Min Kuang, and Jason Pui Yin Cheung in Global Spine Journal
Footnotes
Acknowledgments
We would like to thank Helen Zhi, the senior statistician of our university, who was blinded to this study and final checked on the data analysis. We also thank all patients with their parents. Reviewer’s comments are also gratefully acknowledged.
Author Contributions
Yunli Fan: Manuscript draft and editing. Michael KT To and Guan-Ming Kuang: Imaging assessor and data collection. Jason PY Cheung: Performed the operation, manuscript editing, conceptualization, funding receiver.
Author Note
This study was performed in the University of Hong Kong – Shenzhen hospital, Shenzhen, Guangdong province, China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the high level – hospital program (HKUSZH201902042) of the HKU - SZH in Shenzhen, Guangdong Province, China. This study was partially supported by Hong Kong Research Grant Council Research Impact Fund (R5017-18).
Ethics Approval
The University of Hong Kong- Shenzhen Hospital Ethics Committee(s) approved this study. (IRB reference No.: 伦 [2020]08)
Content to Participate
All participants/patients and parents signed consent form before data collection, agreed with analyzing their radiographic parameters and documented treatment compliance.
Content to Publish
All authors approved the final manuscript before submitting to this journal. Individuals in this manuscript have given written informed consent to publish these case details.
Trial Registration
Availability of Data And Material
Raw data will be saved using the online electronic management database -Redcap. Data will be set as open access within 6 months after manuscript published.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.