
Abstract
Study Design
Randomized controlled trial
Objective
Percutaneous transforaminal endoscopic discectomy (PTED) was introduced as a less invasive procedure to treat sciatica. Even though the PTED has a small scar size, it is unknown if PTED also leads to better scar-related patient-reported outcomes. Therefore, we aimed to compare scar-related outcomes between patients undergoing PTED vs open microdiscectomy.
Methods
Patients with at least 6 weeks of radiating leg pain were randomized in a 1:1 ratio to PTED or open microdiscectomy. Scar-related patient-reported outcomes were measured using the Body Image Score (BIS), Cosmesis Scale (CS) and a 0-10 numeric rating scale (NRS) on scar esthetic.
Results
Of the 530 included patients, 286 patients underwent PTED and 244 underwent open microdiscectomy as allocated. At 12 months of follow-up, 95% of the patients had data available. At 12 months, the BIS was 6.2 ± 1.7 in the PTED-group and 6.6 ± 1.9 in the open microdiscectomy group (between-group difference .4, 95% CI .2 to .7). CS was 21.3 ± 3.0 in the PTED-group and 18.6 ± 3.4 in the open microdiscectomy group (between-group difference −2.7, 95% CI −3.1 to −2.3). Average NRS for scar esthetic was 9.2 ± 1.3 and 7.8 ± 1.6 in the PTED and open microdiscectomy groups, respectively (between-group difference −1.4, 95% CI −1.6 to −1.2)
Conclusions
PTED leads to a higher self-rated scar esthetic as compared to open microdiscectomy, while self-reported body image seems to be comparable between both groups. Therefore, from an esthetic point, PTED seems to be the preferred technique to treat sciatica.
Background
Even though leg pain caused by lumbar disc herniation often resolves with conservative treatment, the high prevalence of sciatica in the general population makes lumbar discectomy a frequently performed procedure.1,2 Conventional transflaval open microdiscectomy is considered to be the standard surgical procedure to treat lumbar disc herniation.3,4 Due to the development of surgical endoscopes and due to attempts to reduce the surgical invasiveness of lumbar discectomy, full-endoscopic procedures were developed to treat sciatica. 5 Percutaneous Transforaminal Endoscopic Discectomy (PTED) is one of these techniques that was proposed as a less invasive alternative to open microdiscectomy. As an endoscopic procedure, PTED was expected to be associated with advantages as less postoperative low back pain, shorter duration of hospitalization, faster resumption of work and a smaller skin incision.6,7 The evidence in favor of most of these advantages, however, is scarce or of low quality.
Although the formation of a scar is adherent to performing surgery, scars can negatively affect patients’ body image and related quality of life.8,9 Previous studies conducted in other surgical fields have shown that patients in general desire smaller scars, but that minimally invasive surgery may not always lead to better body image and cosmesis compared to conventional surgical techniques.10,11 As minimally invasive surgery is rising in popularity among patients and surgeons and a small scar size is often proposed as an advantage of minimally invasive surgery, an evaluation of scar-related patient-reported outcomes between these techniques and conventional surgery seems appropriate. 12 Therefore, the aim of the current study was to assess whether PTED had superior scar-related outcomes compared to open microdiscectomy.
Methods
Trial Design
This study was conducted alongside the PTED-study. 13 The PTED-study was a multicenter, open-label, non-inferiority, randomized controlled trial that was conducted at four clinics in the Netherlands among patients with sciatica caused by lumbar disc herniation. The PTED-study was funded by ZonMw, The Netherlands Organization for Health Research and Development. The institutional review boards of all participating hospitals approved the study protocol (METc VUmc: 2015.029). Prior to enrollment, all patients provided written informed consent.
Sample Size Calculation
The primary aim of the PTED-study was to show non-inferiority in leg pain reduction of PTED compared to open microdiscectomy. Based on a non-inferiority margin of 5 on the 0 to 100 visual analogue scale (VAS) for leg pain, an assumed standard deviation of 14.9, an alpha of .05 and a power of 90%, the sample size was calculated set at 306 patients. 14 With an attrition rate of 20% the sample size for the actual study was 382. Prior to the PTED-study, three of the participating surgeons did not perform PTED. Based on an educated guess and the literature, we estimated them to have a learning curve of 50 cases. 14 To account for an estimated learning curve of 50 patients per surgeon, 150 patients were added to the PTED-arm and was matched by adding 150 patients to the microdiscectomy-arm. Therefore, the PTED-study aimed to enroll 682 patients.
Participants
From February 2016 to April 2019 patients were screened and enrolled by neurosurgeons and orthopedic surgeons, during the outpatient clinic visit. Patients were eligible for enrollment in the PTED-study, if they were between 18 and 70 years of age; had more than 10 weeks of radiating pain with or without motor or sensory loss in the leg, or with more than 6 weeks of excessive radiating pain and no tendency for any clinical improvement; had an indication for surgery; had magnetic resonance imaging demonstrating a herniated disc with nerve compression with or without concomitant spinal or lateral recess stenosis or sequestration; and had sufficient knowledge of the Dutch language in order to complete forms and follow instructions independently. Exclusion criteria were previous surgery on the same or adjacent disc level; cauda equina syndrome; spondylolytic or degenerative spondylolisthesis; pregnancy; severe comorbid medical or psychiatric disorder (American Society of Anesthesiologists classification >2); severe caudal or cranial sequestration of disc fragments; contraindication for surgery and moving abroad on short notice.
Study Endpoints
The primary endpoint of the trial was the difference in VAS for leg pain at 12 months after surgery. The published study-protocol gives an overview of all the outcome measures assessed during the PTED-study. 13 For this study, four outcome measures were used to assess body image, cosmesis, scar esthetic and scar satisfaction. These outcomes were measured 6 weeks, 12 weeks and 52 weeks after surgery.
The body image score (BIS) measures the patient`s body perception and their attitude toward their appearance on a scale ranging from 5 (best body image score) to 20 (worst body image score). 8 The cosmesis score (CS) measures the patient`s satisfaction with their scar appearance, ranging from 3 (worst cosmetic result) to 24 (best cosmetic result). 8 Furthermore, scar esthetic was scored on a 10-point NRS score with 1 indicating a ‘revolting’ scar and 10 a ‘most appealing scar’. Scar satisfaction was measured using a 7-point Likert scale. In case of reoperations, patients were instructed to only judge the scar of the original surgical procedure on cosmesis.
In addition to the patient-reported outcome measures, data regarding the patient`s demographics, the surgical procedure, complications, discharge and reoperations were collected.
Data Collection and Statistical Methods
Questionnaires were sent to patients by email or regular mail at 6 weeks, 3 months and 12 months after surgery. In addition to these patient-reported outcome measures, a trained research nurse would inspect the scar for any signs of infection and would measure the length of the scar. Prior to the commencement of the PTED-study, the expected difference in the NRS for scar esthetic was <1.0 and a non-inferiority margin of .5 was established. 13
Primary analysis for this study was a per-protocol analysis. As it was hypothesized that the esthetic result of the scar was not dependent of the learning curve, the analyses were conducted on the total sample size including the learning curve. A separate sensitivity analysis, excluding the patients of the learning curve, was conducted to support this hypothesis.
Baseline characteristics were presented using percentages for categorical variables and means and standard deviations (SD’s) for continuous variables. Mixed model analyses with random intercepts on the patient level were used to account for dependency of measurements over time within patients. Linear mixed models were used to analyze BIS, CS and the NRS for scar esthetic. Logistic mixed models were used to analyze self-reported scar satisfaction. Crude and fully adjusted models are presented. The latter was presented as sensitivity analysis and included the baseline score, the VAS for leg pain at that time point, age, gender, duration of complaints, smoking status, body mass index, treatment preference of the patient and psychopathology as measured on the Four-dimensional symptom questionnaire.15,16 Mean differences and odds ratio’s (OR’s) are presented with their 95% confidence intervals (95% CI). CI’s from linear mixed model analyses were estimated using a 1000 bootstrap samples according to the bias accelerated procedure to take into account skewness of residuals. A P-value< .05 was considered to be statistically significant. SPSS version 25.0 (IBM) was used for all analyses.
In addition to these analyses, six post-hoc subgroup analyses were conducted to identify groups of patients who might benefit more from an endoscopic treatment in the context of scar esthetic. 17 These subgroups were based on (1) gender; (2) an age ≤ 40 vs > 40 years; (3) a BMI ≤ 30 vs > 30; (4) Caucasian ethnicity vs other ethnicities; (5) being an active smoker vs not; and (6) having a preference to undergo PTED vs having a preference to undergo open microdiscectomy or no preference. Interaction P-values were calculated to determine if the treatment effect varies across the levels of the subgroups.
Randomization and Blinding
Patients were randomized in a 1:1 ratio to PTED or open microdiscectomy using computer-generated variable block sizes (4, 6 or 8), stratified by enrolling center. Blinding of patients was not feasible because of the substantial differences between both procedures (eg PTED being performed under conscious sedation and an 8 mm incision lateral of the spine and open microdiscectomy being performed under general anesthesia with an incision of 2-5 cm dorsal of the spine in the midline).
Surgical Techniques
All trial surgeons were spine-dedicated surgeons who had 8 to 11 years’ experience in performing degenerative lumbar surgery. During this study, PTED was temporarily reimbursed and three surgeons (one per center) were trained in PTED. Each surgeon attended a hands-on workshop on PTED and performed 10 to 20 procedures under supervision of the senior surgeon.
The PTED procedure was performed under local anesthesia. 18 The amount of administered sedation allowed the patient to still respond to nerve root manipulation. Fluoroscopy in two planes, was used to verify the level of the disc herniation. An incision was made just above the dorsolateral side of the pelvis, where a needle was set from the incision to the superior articular process of the lower involved vertebrae of the herniated disk. After the needle had reached the superior articular process, a guidewire was inserted. Subsequently conical rods were introduced followed by a drill to enlarge the neuroforamen. Hereafter, an endoscope was introduced within the working channel using an 8 mm cannula. A forceps was used to remove the disc fragments. After removal of the loose disc fragments, the endoscope and working channels were removed and the wound was closed in a single layer with a dissolvable intracutaneous suture. Patients were treated on an outpatient basis.
Open microdiscectomy was conducted under general anesthesia. Fluoroscopy was used to verify the level of disc herniation. The use of loupe or microscope magnification was optional. A paramedian incision was performed. Following the identification of the lamina, the ligamentum flavum was removed to identify the nerve root and disc herniation. Laminotomy, as well as foraminotomy, was performed, if necessary. For foraminal herniated discs a partial medial facetectomy was performed while for extraforaminal herniated discs, a parafacetal approach was used. The wound was closed in multiple layers. The skin could be closed in two manners, depending on the surgeon. On one hand, the subcutis was closed with dissolvable sutures and wound closure strips would be applied to the cutis. On the other hand, after closure of the subcutis, a dissolvable intracutaneous suture would be used to close the cutis. Patients were discharged as soon as medically responsible, which was usually one day after surgery.
Pain medication was offered to all patients and the use of cointerventions was monitored using questionnaires.
Results
Patients
During the enrollment period of the PTED-study, from February 2016 to April 2019, 711 patients were assessed for eligibility (see Figure 1). Eventually, 613 patients were assigned to PTED or open microdiscectomy. Of the 304 patients that were assigned to PTED, 286 eventually underwent PTED and were included in the per-protocol analysis, while of the 309 patients that were assigned to open microdiscectomy, 244 underwent open microdiscectomy and were included in the per-protocol analysis. Reasons for protocol violation were spontaneous recovery, conversion of the procedure, cauda equina syndrome, logistic reasons or not accepting the treatment allocation. At 12 months of follow-up, 95% of the patients included in the per-protocol analysis, had follow-up data available. Wounds and scars of PTED and microdiscectomy at different moments with the upper row showing PTED and the lower microdiscectomy. (A) and (E) give an overview of the position of the scar, (B) and (F) show the wound before closure, (C) and (G) show the sutured wound and (D) and (H) show the wound three months after surgery. PTED, Percutaneous transforaminal endoscopic discectomy.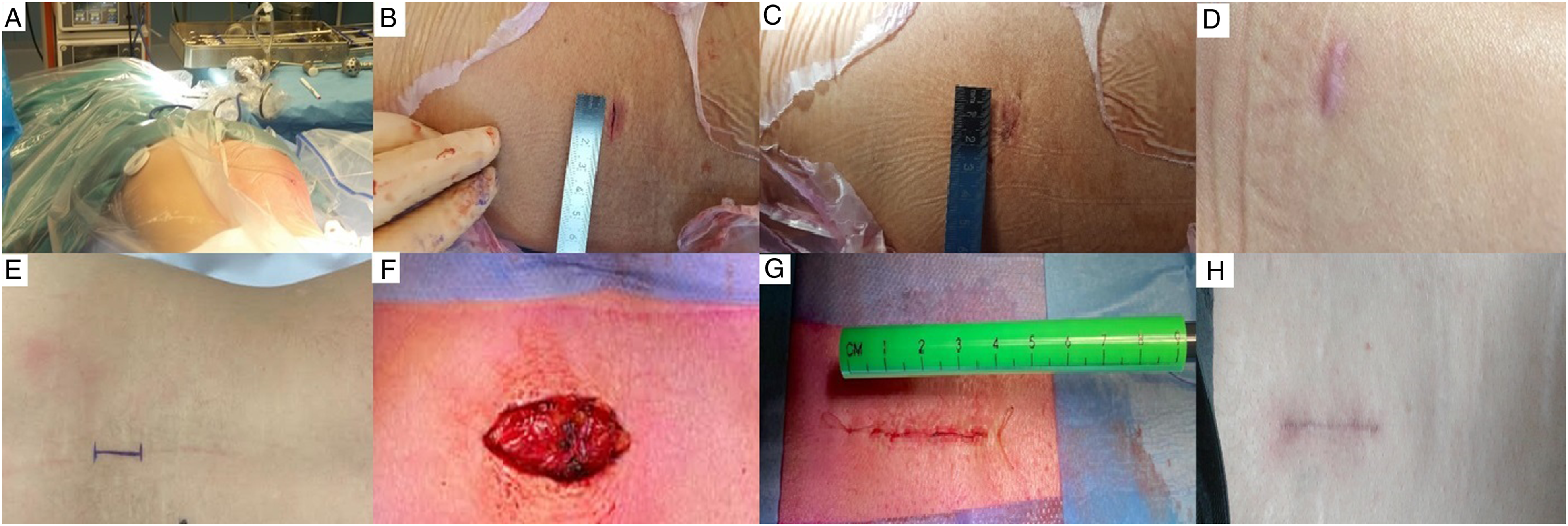
Baseline Characteristics of the Patients.
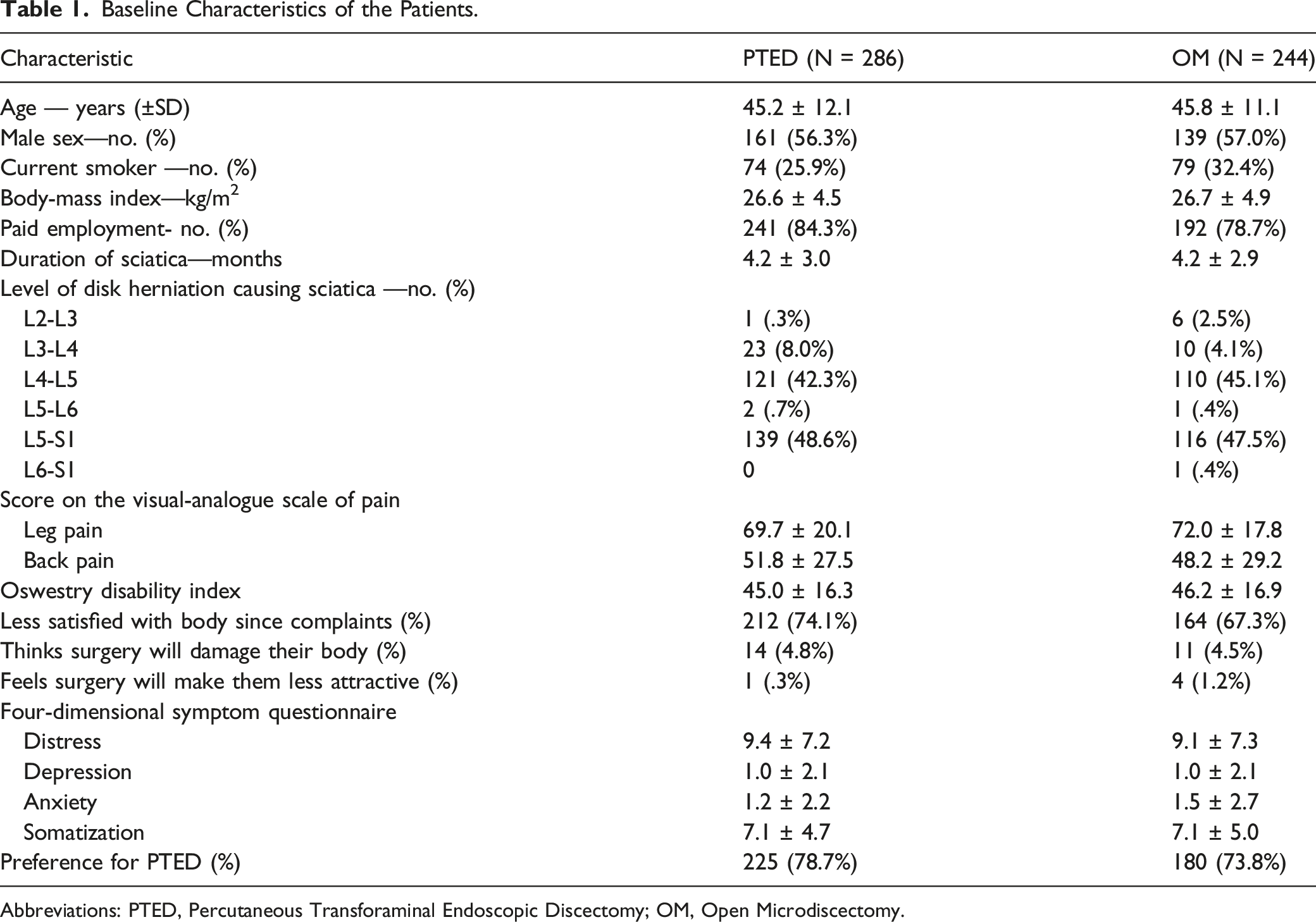
Abbreviations: PTED, Percutaneous Transforaminal Endoscopic Discectomy; OM, Open Microdiscectomy.
Complications and Surgical Outcomes
Surgical Outcomes.
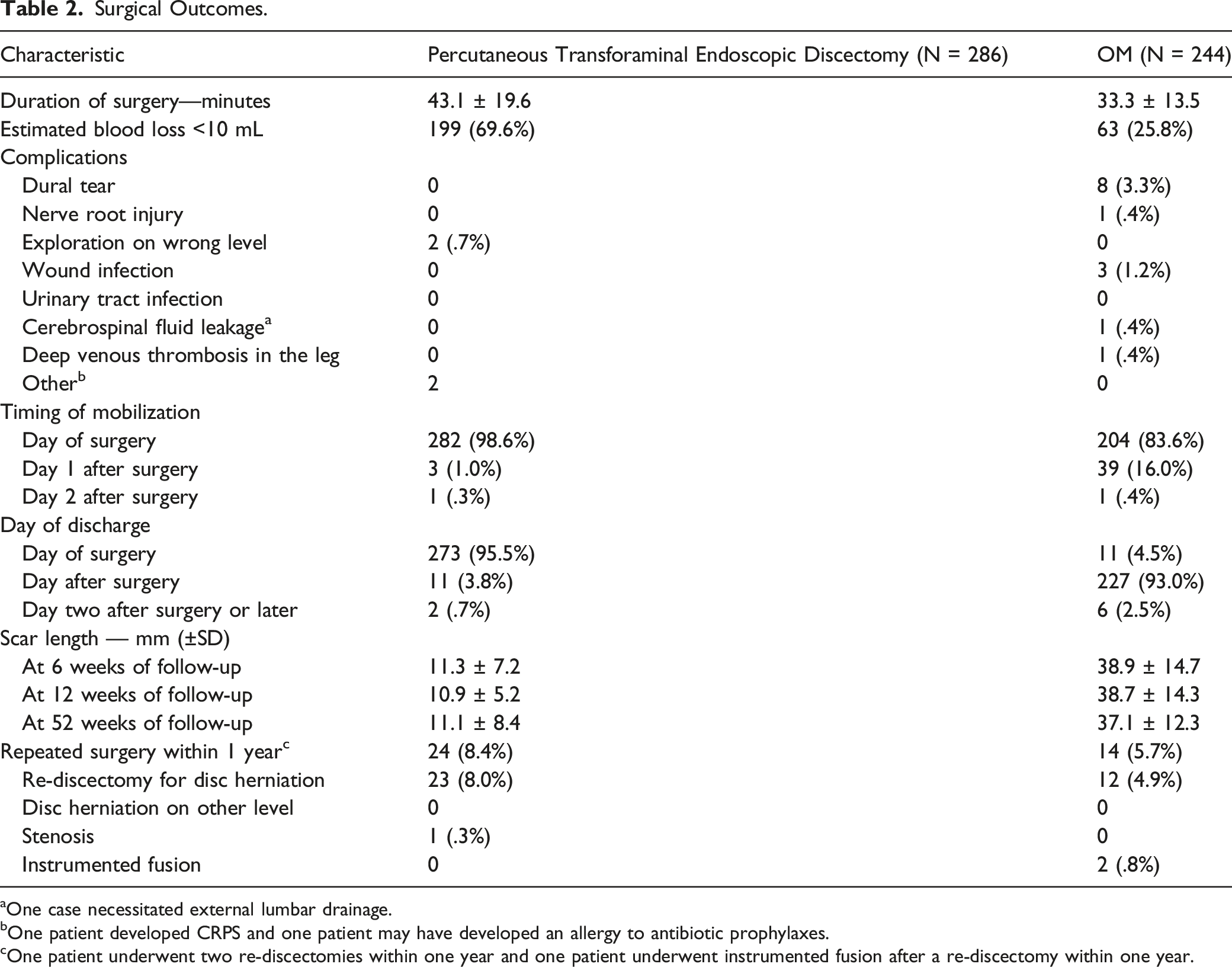
aOne case necessitated external lumbar drainage.
bOne patient developed CRPS and one patient may have developed an allergy to antibiotic prophylaxes.
cOne patient underwent two re-discectomies within one year and one patient underwent instrumented fusion after a re-discectomy within one year.
Mean scar size after PTED was 11 mm vs 39 mm after open microdiscectomy, measured at 6 weeks of follow up. Scar sizes showed no relevant change during follow-up moments at 3 and 12 months. During the follow-up period 3 superficial wound infections occurred, all three in the open microdiscectomy-group. At 12 months of follow-up, 24 (8.4%) reoperations occurred in the PTED-group in contrast to 14 (5.7%) reoperations in the open microdiscectomy-group (Figure 2). Flowchart of study eligibility, enrollment, procedures and completeness of outcomes.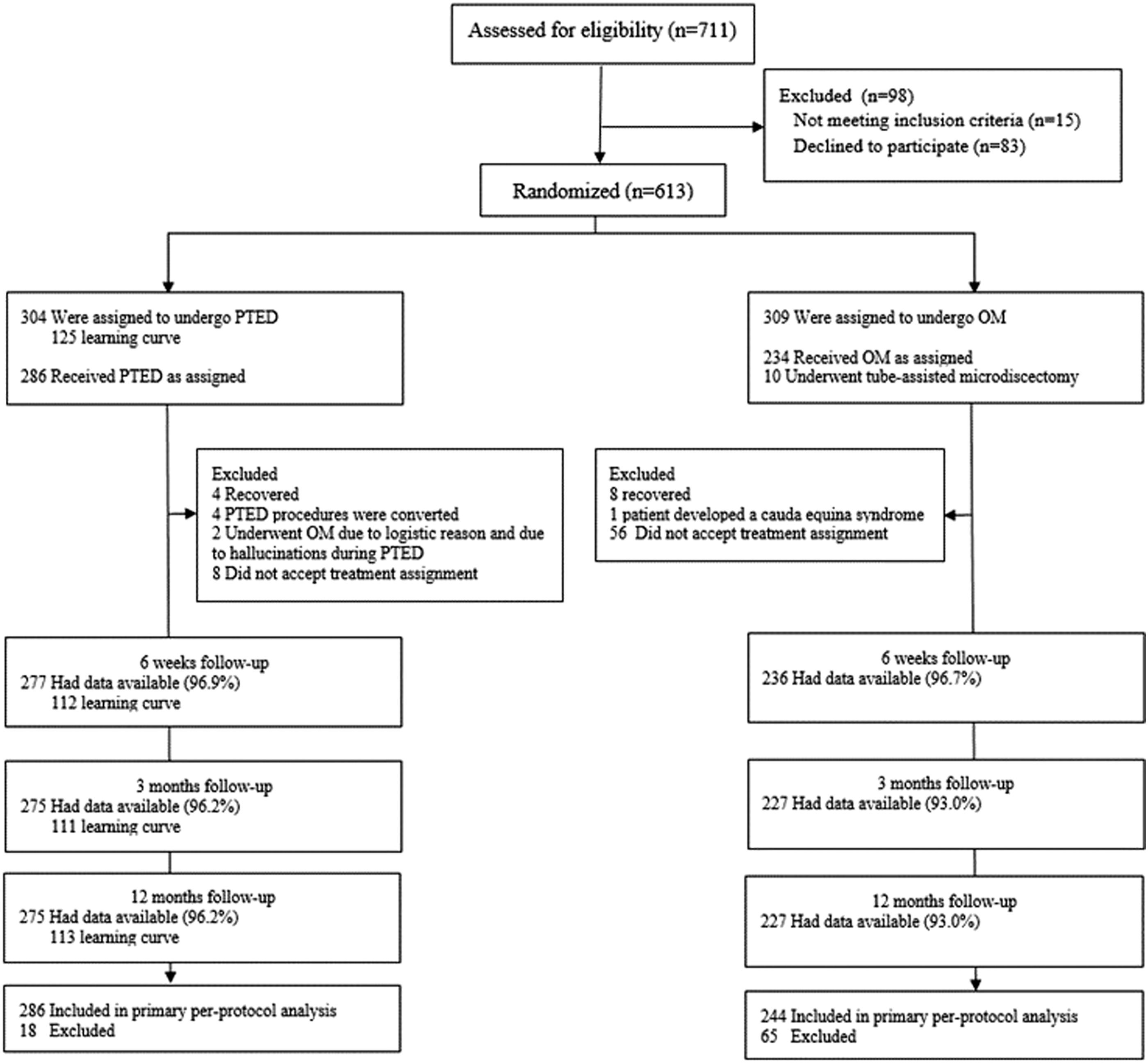
Body Image and Cosmesis Score
Curves of mean scores on the body image, cosmesis score, NRS for scar esthetic are shown in Figure 3, together with the proportion of patients that are satisfied with their scar. In general, the body image and scar-specific outcomes were more favorably scored in patients that underwent PTED compared to those that underwent open microdiscectomy at all follow-up moments. Curves of mean (±SE) scores on (A) the Body Image scale, (B) the Cosmesis score and (D) the numerate rating scale for scar esthetic are shown. Self-reported satisfaction with the scar is also depicted (C).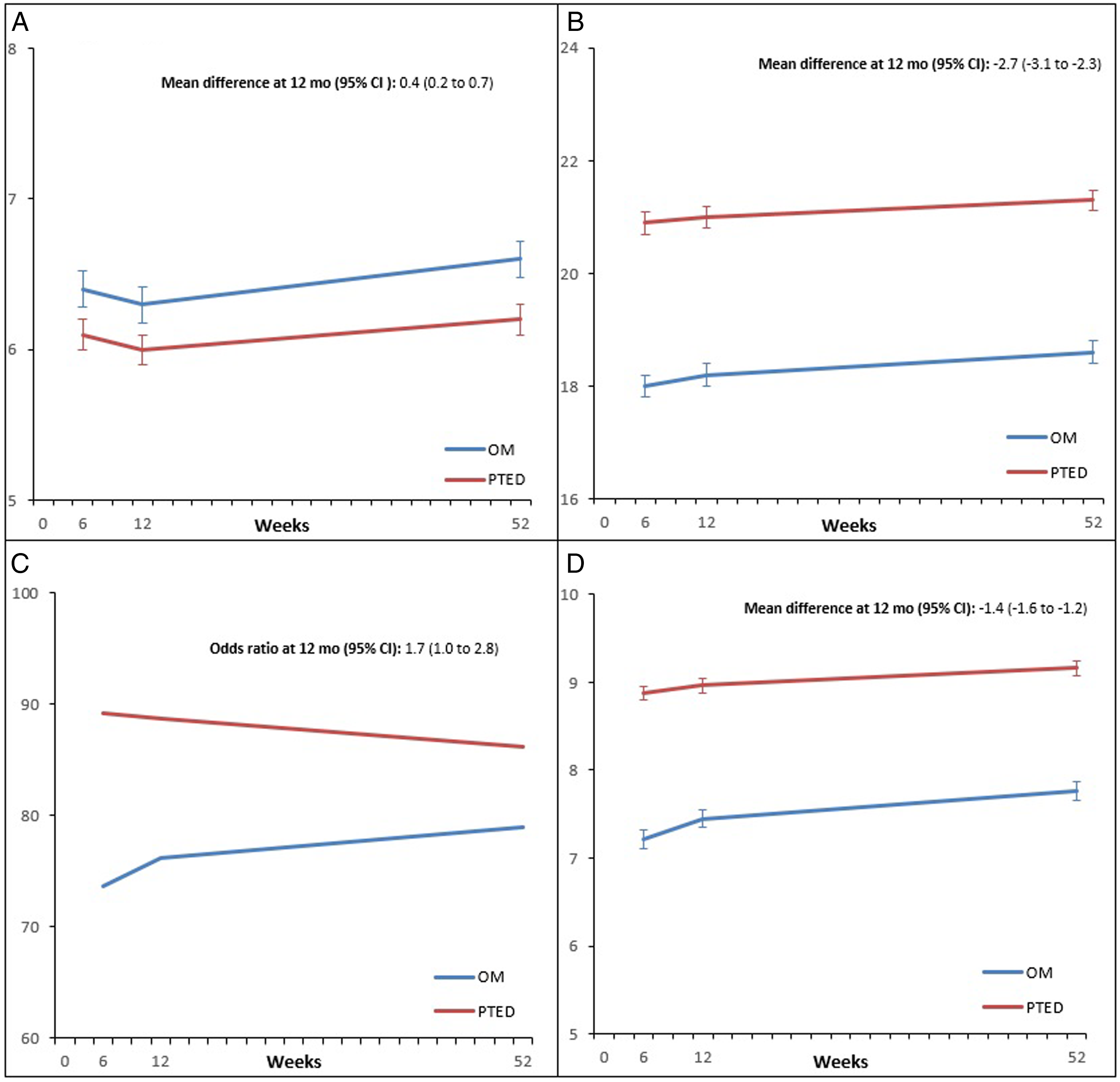
Body Image Score, Cosmesis Score and Other Scar-Related Outcomes 6 Weeks, 3 Months and 12 Months After Surgery.
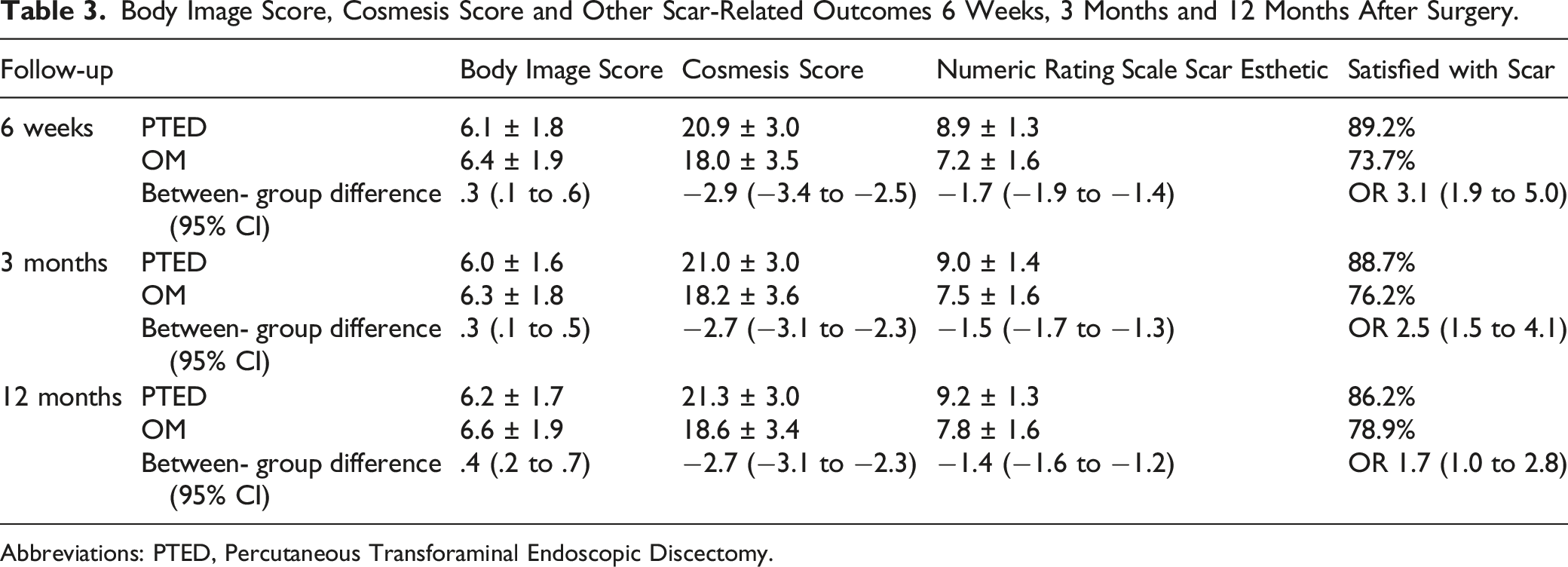
Abbreviations: PTED, Percutaneous Transforaminal Endoscopic Discectomy.
Sensitivity and Subgroup Analyses
The results of the sensitivity analysis with adjusted between-group differences are shown in Supplementary Table 1. In general, the crude results were not significantly altered in the adjusted between-group differences. Furthermore, results excluding patients from the learning curve (N = 115) are shown in Supplementary Table 2. Again, omitting the results of the learning curve patients, did not alter the results.
The results of the subgroup analyses are shown in Figure 4. All subgroups show that the patients that underwent PTED had a higher mean score in scar esthetic compared to patients that underwent open microdiscectomy. The subgroups based on gender and body mass index had between-group differences of at least .5 point on the NRS for scar esthetic. Of both of these groups only the subgroup based on gender seemed to have a statistically significant interaction P-value (P = .01). Female patients that underwent discectomy had a larger mean difference (−1.7, 95% CI −2.1 to −1.4) in NRS for scar esthetic compared to male patients (−1.0, 95% CI −1.3 to −.7) in favor of PTED. The other subgroups based on age, ethnicity, smoking status and preference for surgical procedure did not reveal any statistically significant differences in NRS for scar esthetic. Subgroup-analysis of the NRS for scar esthetic. The subgroups are presented with their sample size, the mean difference in NRS with their respective 95% confidence interval and the interaction P-value. NRS, numeric rating scale.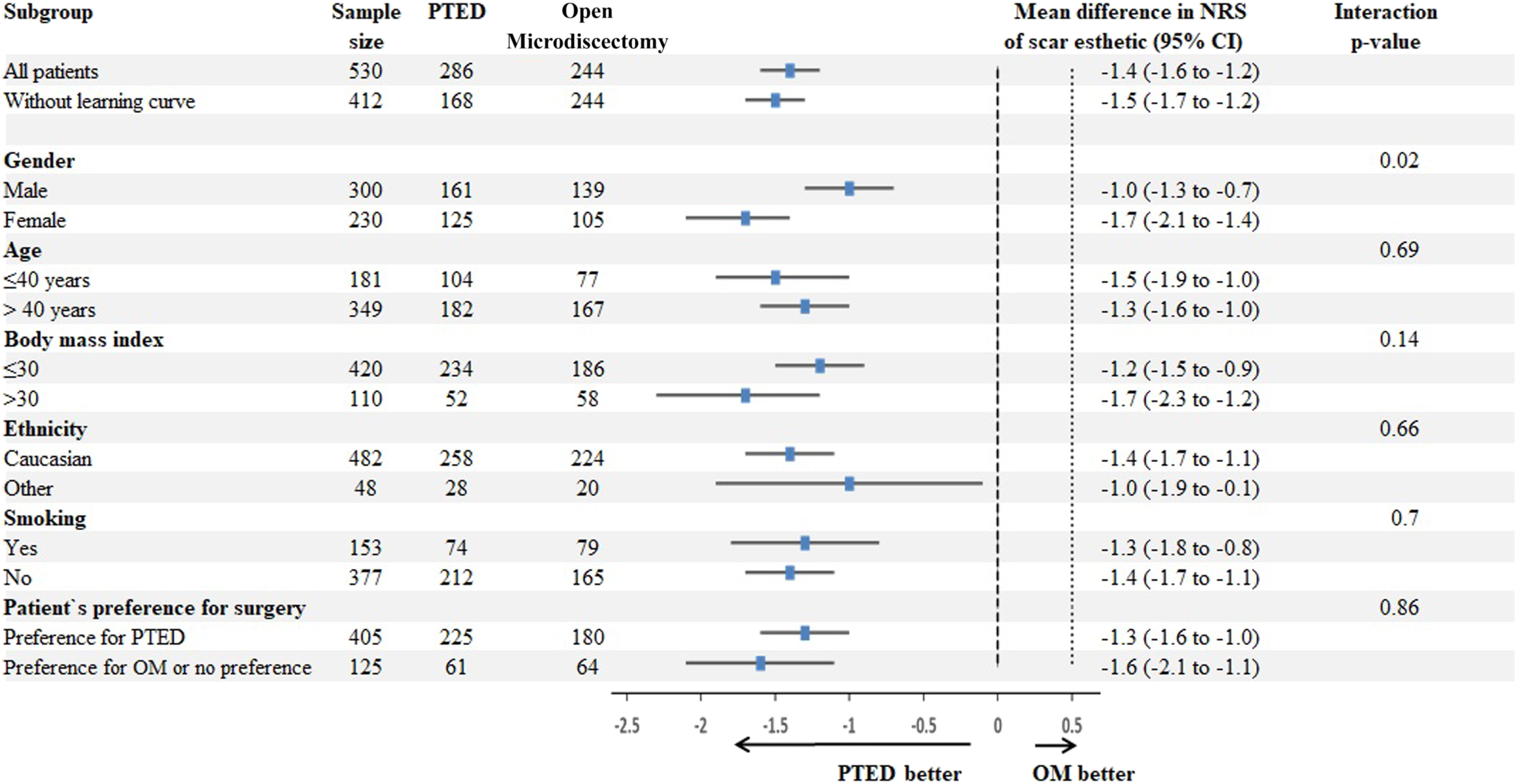
Discussion
The current study is the first to assess and compare scar-related patient-reported outcome measures after spine surgery, based on data of a randomized controlled trial. In the per-protocol analysis including 530 patients, patients that underwent PTED had more favorable scar-related outcomes at 12 months. Compared to open microdiscectomy, the scar size was smaller and wound infections did not occur, while the cosmesis score and scar esthetic had higher scores. Even though of statistical significance, body image scores seem comparable between both groups during follow up. Scar satisfaction was higher in the PTED-group at 6 weeks and 3 months but was comparable between both groups at 12 months. A priori, it was hypothesized that the scar esthetic would differ 1 point, which was exceeded in the current study. However, no clinically important differences were defined a priori. In the literature, there is a paucity on data of minimally clinically important differences in scar-related patient-reported outcomes, but for the body image and cosmesis scores a clinically relevant improvement of 20% is commonly used. 19 For a 0 to 100 mm VAS on scar cosmesis, a minimal clinically important difference of 15 mm seems appropriate. 20 From the viewpoint of these established minimal clinically important differences, patients from the PTED-group seem to only have a clinically relevant benefit in NRS for scar esthetic at 6 weeks and 3 months, compared to patients who underwent open microdiscectomy.
To the best of our knowledge, only one study could be identified that compared aesthetic outcomes between minimally invasive and open surgical techniques to treat lumbar degenerative disease. 21 In that prospective study, 74 patients were enrolled at a single center and were followed during one year with outcomes such as a VAS on scar aesthetic. During the follow-up period, patients that underwent minimally invasive surgery consistently scored 1 to 2 points higher on the VAS which ranged from 1 to 5 (with “1” being very poor and “5” being excellent). Some differences can be discussed. At first the between-group differences in the former study, seem to be larger than was be shown in the PTED-study. This difference may be explained by the remarkably low scores on the VAS for scar aesthetic, by patients that underwent open surgery. For instance, at 1-year follow-up, the mean score for the open surgery group was a 2 which was defined as poor. Another difference between both studies, is that the former was not randomized and therefore selection bias and confounding by indication cannot be ruled out. Nevertheless, both studies show that minimally invasive spine surgery has some aesthetic advantages over open procedures.
The current study has some limitations that need to be acknowledged. Some of these limitations are adherent to the design and conduction of the PTED-study.13,22 For instance, the study had a non-inferiority design and was also not blinded as it was not feasible due to the nature of the procedures. By calculating adjusted between-group differences, we aimed to correct for the patients’ preferences for PTED. Another limitation might be that the estimated the sample size of 682 patients was not reached. However, the sample size of 682 included 150 patients that underwent PTED as learning curve cases, which was considered to be relevant in the treatment of leg pain but not for scar-related patient-reported outcome measures. Therefore, the current analysis might rather be overpowered then underpowered. Another limitation is that it was not feasible to control for scar diathesis. Other limitations maybe introduced in the choices made for data analysis. While the PTED-study was designed to perform a primary intention-to-treat analysis, it was deemed to be less appropriate for the analysis of scar-related outcomes. This mainly due to the immediate drop-out of patients in the open microdiscectomy-group after randomization. Proportions of these patients would undergo surgery by other minimally invasive techniques or would not undergo surgery at all. The inclusion of their scar-related outcomes, which were mostly missing due to not undergoing surgery, would only increase the chance of introducing bias in the analysis. Therefore, only the results of the per-protocol analysis are shown. Another possible limitation might be related to the BIS and CS. Both scales have been widely used in the assessment of scar-related outcomes in abdominal surgery, but not yet in lumbar spine surgery.8,19 Hence its validity in this patient population is unknown. Furthermore, the differences on the BIS, that were statistically significant, would not have been detected when we would have rounded up the scores to whole numbers as it was intended to in the original BIS. Therefore the detected differences on the BIS are likely not clinically relevant. Nevertheless, the BIS and CS seems to have a good correlation with the numeric scale on scar esthetic which has been previously been used. 21 Finally, the interpretation of the exploratory subgroup analyses also warrants some caution as subgroup analyses are frequently underpowered or prone to multiplicity. 17 As these subgroup analyses were posthoc, no attempts were made to adjust the P-value for multiplicity.
Based on the current randomized controlled trial, both PTED and open microdiscectomy have favorable scar-related outcomes. PTED, however, leads to a smaller scar size, less wound-related complications and higher self-rated scar esthetic as compared to open microdiscectomy, while self-reported body image and scar satisfaction seems to be comparable between both groups. Therefore, from an esthetic point of view, PTED seems to be the preferred technique to treat lumbar disc herniation.
Supplemental Material
Supplemental Material - Body Image and Cosmesis After Percutaneous Transforaminal Endoscopic Discectomy Versus Conventional Open Microdiscectomy for Sciatica Caused by Lumbar Disc Herniation: Results of a Randomized Controlled Trial
Supplementary Material for Body Image and Cosmesis After Percutaneous Transforaminal Endoscopic Discectomy Versus Conventional Open Microdiscectomy for Sciatica Caused by Lumbar Disc Herniation: Results of a Randomized Controlled Trial by Pravesh S. Gadjradj, Paul R. Depauw, Pieter J. Schutte, Arnold V. Vreeling, and Biswadjiet S. Harhangi in Global Spine Journal.
Footnotes
Acknowledgments
We gratefully acknowledge the support of the Dutch Health Insurance Board, ZonMw, the participating patients, the patient organization ‘de Wervelkolom (nvvr)’, the enrolling physicians and the research nurses. Aside from the authors, members of the PTED-study group are dr. J. van Susante, dr. S. Rubinstein, dr. W. Peul and Prof.dr. M. van Tulder.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by ZonMw, The Netherlands Organization for Health Research and Development (project number 837004013)
Authors’ Note
Funded by ZonMw, The Netherlands Organization for Health Research and Development; PTED-study ![]() number NCT02602093. ZonMw did not participate in the study design and conduct of the study, in the collection, analysis, and interpretation of the data, or in the preparation, review or approval of the manuscript.
number NCT02602093. ZonMw did not participate in the study design and conduct of the study, in the collection, analysis, and interpretation of the data, or in the preparation, review or approval of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.