
Abstract
Study Design
Case report.
Objective
Describe a case of intradural disk herniation and a method for intraoperative localization.
Methods
Intradural disk herniations are uncommon but well described. The diagnosis of these lesions is often difficult, and sometimes they may be diagnosed only through an intradural exploration after an expected disk fragment cannot be located. We report the case of an intradural disk herniation with an additional diagnostic difficulty—a migrated intradural disk.
Results
We present the first intraoperative imaging evidence of disk migration and propose a strategy to locate intradural disk fragments prior to durotomy.
Conclusion
Intradural disk herniations should be suspected when intraoperative findings are not congruent with imaging findings. An intraoperative myelogram may be helpful.
Introduction
Intradural disk fragments were first described by Dandy in 1942, 1 and since then, more than 100 cases have been presented in the literature. 2 However, despite improved imaging techniques, the diagnosis of intradural disk fragments is often made only during surgical intervention, which can present a surgical dilemma regarding intradural exploration, particularly for a surgeon unprepared to open the thecal sac. This procedure may be further complicated by the rare event of intradural migration of the disk fragments. We report a patient who presented with cauda equina syndrome due to a migratory intrathecal disk herniation, and we describe a means to diagnose an unsuspected intradural disk intraoperatively.
Case Report
History and Presentation
The patient was a 68-year-old woman with a history of mild chronic intermittent back pain and a known degenerative lumbar scoliosis who presented to a referring institution with worsening low back pain, sensory changes in the L3–S1 distribution, lower extremity pain, weakness of the right greater than left lower extremities (right tibialis anterior 1 to 2/5 and extensor hallucis longus 3/5; left lower extremity 4/5 tibialis anterior and extensor hallucis longus), as well as perineal sensory changes and urinary retention consistent with cauda equina syndrome. Magnetic resonance imaging (MRI) demonstrated a large disk herniation at the L2–3 level causing severe central canal impingement, more prominent on the right side (Fig. 1). Urgent surgical intervention was recommended and accomplished the same day as the MRI.
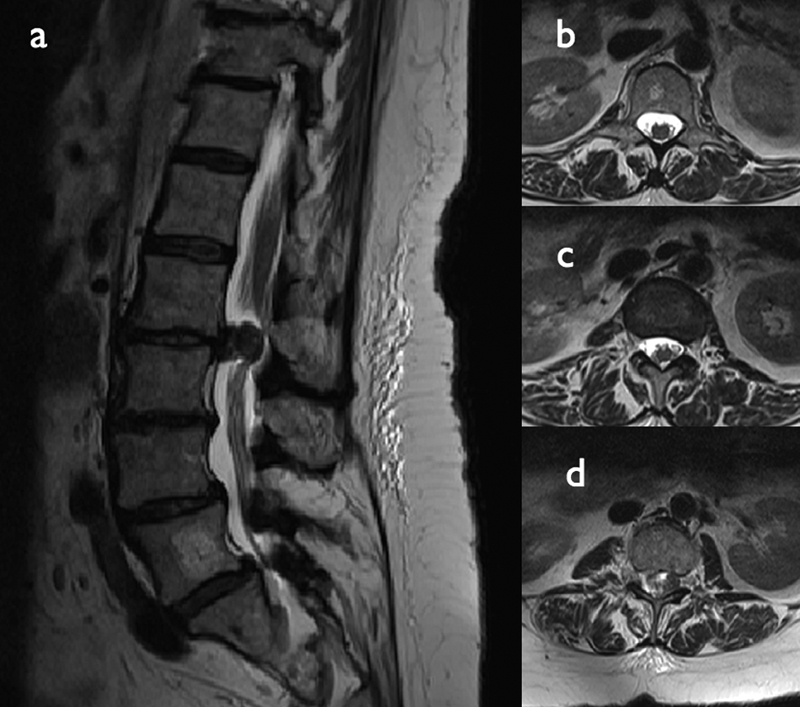
Preintervention magnetic resonance imaging (MRI). (a) Sagittal T2-weighted MRI demonstrating a large extruded disk at the L2–3 interspace. (b) Axial T2-weighted MRI at the level of the L1 vertebral body, without evidence of disk extrusion. (c) Axial T2-weighted MRI at the level of the L1–L2 disk space, without evidence of disk extrusion. (d) Axial T2-weighted MRI at the level of the L2–3 disk space demonstrating disk extrusion.
First Operation
Intraoperatively, the L2–3 interspace was approached and a midline laminectomy was performed. Upon exposure of the dura, no displacement was noted and no disk fragment was discovered. The L2–3 disk space was initially approached from the right but no disk material was found. The left side of the L2–3 disk space was also explored without localizing any extruded disk material. Lacking any extruded disk, no diskectomy was performed at that time. The operative level was reconfirmed with fluoroscopy. Palpation with a Woodson superiorly, inferiorly, medially, and laterally as well as out into the L2–L3 and L3–L4 foramina bilaterally confirmed no extraneous disk material as far cephalad as the L1–2 interspace. We then elected to perform an intraoperative myelogram. Omnipaque 180 (10 mL) was injected through a 25-gauge needle into the dural space at the L2–L3 level. No filling defects were observed at the level of L2–3; however, a filling defect was present behind the vertebral body of L1 (Fig. 2). Because of the discrepancy between these findings and the preoperative MRI, we elected to awaken the patient and obtain an additional MRI for confirmation of the myelogram findings. Following this procedure, the patient experienced some improvement in her weakness and lower extremity sensory changes but with residual perineal numbness, possibly suggestive of a conus medullaris syndrome. Repeat MRI indeed confirmed the findings suspected following the myelogram with several extruded disk fragments behind the body of L1 (Fig. 3).

Intraoperative fluoroscopy, lateral projection, demonstrating a lack of contrast filling behind the L1 vertebral body.
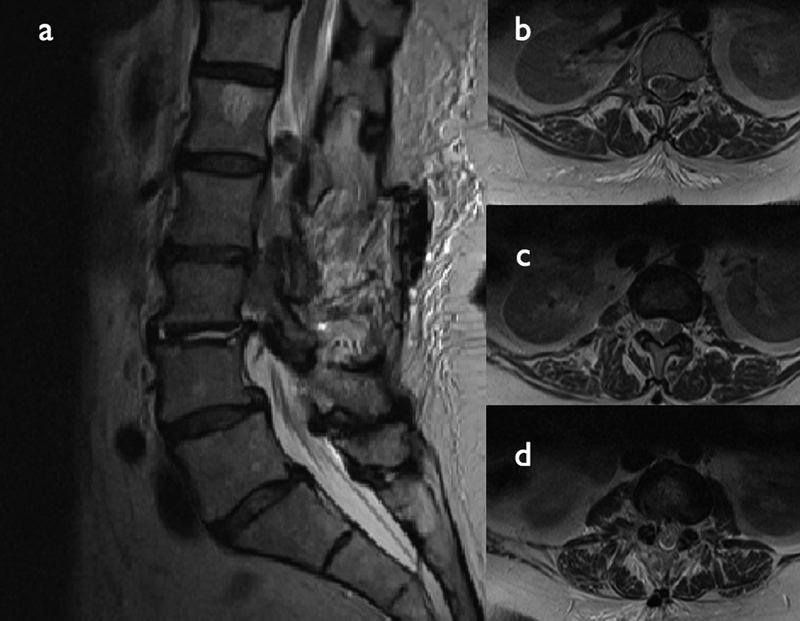
Post–first intervention magnetic resonance imaging (MRI). (a) Sagittal T2-weighted MRI demonstrating postoperative changes and confirming presence of the migrated disk to the L1 level. (b) Axial T2-weighted MRI demonstrating disk material at the level of the L1 vertebral body. (c) Axial T2-weighted MRI at the level of the L1–L2 disk space demonstrating further disk material. (d) Axial T2-weighted MRI at the level of the L2–3 disk space showing diminished or absent disk material at this level.
Second Operation and Postoperative Course
The patient returned to the operating room and an L1 laminectomy was performed. Again finding no extradural disk material, a surgical durotomy was performed. Several large pieces of disk material were found ventral and lateral to the conus medullaris, and this material was removed piecemeal (Fig. 4). The dura was repaired, the wound closed, and the patient taken to recovery. The remainder of her hospitalization was unremarkable. Postoperatively, she experienced good relief of her pain and good recovery of her neurologic function, particularly her motor symptoms and bowel and bladder function. She still had some residual numbness in the right foot. Two years postoperatively, she demonstrated 5/5 motor strength in her bilateral lower extremities and intact sensation; bowel and bladder function was normal.
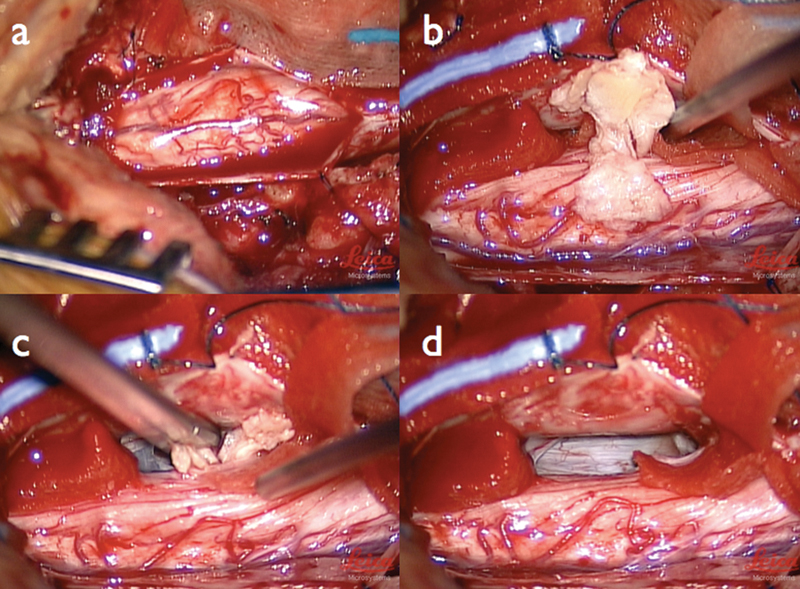
Intraoperative findings. (a) The dorsal displacement of the spinal cord is evident. (b) A large disk fragment is removed. (c) Additional disk material is removed piecemeal. (d) After removal of all disk material, the spinal cord assumes a more normal position.
Discussion
Intradural disk herniations are uncommon but well described. They are most common at the L4–5 level, although intradural disks at other lumbar levels, as well as in the cervical and thoracic regions, have also been described. 3 The clinical presentation and demographics of patients with intradural disk herniation are indistinguishable from those of patients with more standard disk herniations, although cauda equina syndrome may be more common in individuals with an intradural disk herniation. 4 , 5 Despite improved imaging techniques in spine surgery, the location of the disk material or exact diagnosis may be unknown until the time of surgery, presenting an intraoperative dilemma for the surgeon.
Pathophysiology
Although the exact mechanism for transdural migration of disk fragments is unknown, the leading hypothesis relates to the formation of ventral dural and posterior longitudinal ligament adhesions, which have been confirmed on cadaveric studies, 6 as well as previous intradural disk case reports. 2 These conditions may lead to thinning of both the annulus and the dura, allowing migration of disk fragments into the dural space when herniation occurs. 7 Additional theories relating to an inflammatory response or previous surgery have also been postulated. 8 One reported case was related to a traumatic injury. 9 Our patient had neither previous surgery nor any related traumatic event.
Imaging Evidence
The imaging characteristics of intradural disks are variable. Some initial cases were discovered on myelography, where a total or subtotal block of contrast was often seen. 10 An irregular filling defect has also been suggested to point to an intradural disk herniation. 11 Computed tomography has been utilized in the past to diagnose intradural disk herniations. Hidalgo-Ovejero and colleagues suggested that the presence of epidural gas bubbles may indicate an intradural disk herniation. 12 , 13 MRI is currently the most common method of radiologic evaluation in the nontraumatic lumbar spine and is likely the most reliable for diagnosing intradural disk herniations. Both a “hawk-beak” sign (loss of continuity and beaking of the posterior longitudinal ligament) and rim enhancement of the disk material have been described in intradural disk cases, 14 , 15 but may not be commonly found. 16 Although not an absolute indicator, the location of the herniation in relation to the disk may suggest an intradural location. Kim and colleagues reported on a dorsally extruded extradural disk located just beneath the lamina and posterior to the thecal sac; based upon imaging characteristics, an intradural herniation was suspected. 17 Furthermore, disks that are obviously intradural may mimic intradural spine tumors. 7 This diagnostic difficulty was experienced in our case, and the absence of extradural disk material noted intraoperatively was the only clear indication that the herniation may be intradural.
Disk Migration
Migration of intradural disk herniations has rarely been reported. Sarliève and colleagues described an unfruitful disk surgery for cauda equina syndrome, with incomplete recovery and subsequent MRI demonstration of disk material one level above the operated level 2 months after surgery. 5 Although this event was postulated by the authors to have occurred either prior to or during intraoperative manipulation, the lack of imaging evidence until 2 months after surgery obscured this picture. 5 Bloom and Maurice-Williams described what they believed to have been a transdural migration during surgery in one case, although the disk material remained at the original lumbar level. 18 To our knowledge, our case represents the first documented intraoperative evidence of migration of an intradural disk. Upon retrospective review of our imaging studies, we believe that the disk herniation in our patient was likely always intradural; however, the migration cephalad may have been due to several factors: first, positioning the patient prone with some flexion on a Wilson frame may have forced the disk fragments cephalad. Alternatively, retraction on the thecal sac to visualize the disk space may have caused the cephalad displacement.
Intraoperative Strategy
Ultimately, intraoperative findings may be the only way to determine the intradural location of the disk fragments. Schisano and colleagues have advocated that “tense dura and palpation of an intradural mass associated with observation of an empty intervertebral disk” is suggestive of an intradural location. 10 However, because of the additional risk of intradural exploration, the possibility of disk resorption, 19 and possible migration to a higher level as presented in our case, intraoperative confirmation of intradural disk material would be preferable prior to intradural exploration. We have described a technique for intraoperative myelogram using Omnipaque, a 25-gauge needle, and fluoroscopy. We feel that this is a viable option for determining an intradural location of pathology, and if the level of the filling defect coincides with preoperative MRI level of the disk herniation, then the intraoperative myelogram alone may justify intradural exploration. Because of the unexpected finding of a filling defect at a level above the originally visualized disk herniation in our case, intradural exploration at the lower level was avoided and an MRI was chosen to confirm our findings. This technique is useful for both confirming intradural disk location, as opposed to disk resorption (another possible explanation for absent disk material), as well as identifying migration of the intradural disk.
Disclosures
Scott D. Daffner, none
Cara L. Sedney, none
Charles L. Rosen, none