
Abstract
Study Design
A retrospective cohort study.
Objectives
To determine the outcome and any differences in the clinical results of three different surgical methods for lumbar disk herniation and to assess the effect of factors that could predict the outcome of surgery.
Methods
We evaluated 148 patients who had operations for lumbar disk herniation from March 2006 to March 2011 using three different surgical techniques (laminectomy, microscopically assisted percutaneous nucleotomy, and spinous process osteotomy) by using Japanese Orthopaedic Association (JOA) Back Pain Evaluation Questionnaire, Resumption of Activities of Daily Living scale and changes of visual analog scale (VAS) for low back pain and radicular pain. Our study questionnaire addressed patient subjective satisfaction with the operation, residual complaints, and job resumption. Data were analyzed with SPSS version 16.0 (SPSS, Inc., Chicago, Illinois, United States). Statistical significance was set at 0.05. For statistical analysis, chi-square test, Mann-Whitney U test, Kruskal-Wallis test, and repeated measure analysis were performed. For determining the confounding factors, univariate analysis by chi-square test was used and followed by logistic regression analysis.
Results
Ninety-four percent of our patients were satisfied with the results of their surgeries. VAS documented an overall 93.3% success rate for reduction of radicular pain. Laminectomy resulted in better outcome in terms of JOA Back Pain Evaluation Questionnaire. The outcome of surgery did not significantly differ by age, sex, level of education, preoperative VAS for back, preoperative VAS for radicular pain, return to previous job, or level of herniation.
Conclusion
Surgery for lumbar disk herniation is effective in reducing radicular pain (93.4%). All three surgical approaches resulted in significant decrease in preoperative radicular pain and low back pain, but intergroup variation in the outcome was not achieved. As indicated by JOA Back Pain Evaluation Questionnaire–Low Back Pain (JOABPQ-LBP) and lumbar function functional scores, laminectomy achieved significantly better outcome compared with other methods. It is worth mentioning that relief of radicular pain was associated with subjective satisfaction with the surgery among our study population. Predictive factors for ineffective surgical treatment for lumbar disk herniation were female sex and negative preoperative straight leg raising. Age, level of education, and preoperative VAS for low back pain were other factors that showed prediction power.
Introduction
Back pain has been described in the Bible and the writing of Hippocrates and continues to be a major health problem.1 The international prevalence of low back pain vaires, 2 but estimations for lifetime prevalence of this condition have been reported between 49 and 80%. 3 Considering these rates, low back pain is a prevalent condition that has many direct and indirect costs in terms of pain and disability as well as the economic burden in terms of lost work days, health care interventions, and lost productivity time. 3 , 4 , 5 , 6 , 7 Herniated lumbar disk is the most common specific cause of low back pain. 8 Young and middle-aged individuals are the most frequent sufferers of this condition. 9 Except for cases that require immediate surgical intervention, the first-line treatment involves medical choices. Ninety percent of attacks of sciatica respond to conservative management. 10 Indications for surgical intervention include cauda equina syndrome (absolute emergency), morphine-resistant hyperalgesic sciatica, paralyzing sciatica, grade less than 3 for muscle power as indicated by the Medical Research Council (other than toe muscles, where isolated palsy is not an indication for surgery), and residual disabling pain despite 6 to 8 weeks of full medical treatment. 11
Surgery results in better outcome for cases with exclusive severe radicular pain in comparison with patients who suffer from moderate low back and leg pain. 12 Health-related quality of life improves after lumbar disk herniation (LDH) surgery. 13
The cost-effectiveness of LDH surgery is another area of debate. Although surgery has its own financial burden, 2-year health outcomes for operated cases were better than outcomes among conservatively managed cases. 14
Many approaches have evolved since the introduction of the first surgical method for treatment of ruptured intervertebral disk by Mixter and Barr. 15 Results for different surgical techniques used in treatment of LDH have been reported as follows:
Intradiscal procedures 16 , 17 have reported success rates of 70 to 80%.
With microscopically assisted procedures, such as microscopically assisted percutaneous nucleotomy (MAPN), 18 immediate postoperative pain relief was reported in 75% of cases.
Endoscopic procedures: in 81.8% of cases, according to the Macnab criteria, overall excellent or good outcomes were achieved, 19 and according to another study, 20 91% reported no leg pain at the time of follow-up examination.
Hemilaminoplasty led to significant improvements in Japanese Orthopaedic Association (JOA) scores and visual analog scale (VAS) for back and leg pain. 21
With spinous process osteotomy, 83% of patients were satisfied. 22
Standard diskectomy achieves an average recovery rate of 73.56 ± 21.7% as evidenced by JOA score. 23 Another study reported all but 23.4% of the patients were entirely satisfied. 24
Long-term comparative studies between surgically and nonsurgically treated cases have demonstrated greater relief of symptoms and improved function for cases that had surgery. 25 , 26 , 27 Success rates for LDH surgery have been reported between 56 and 90% in studies that evaluated patients from 2 to 32 years. 28 , 29 , 30 , 31 , 32 , 33 , 34 , 35 , 36
We aimed to study the following gaps in the literature. (1) Clinical results of spinous process osteotomy for the treatment of LDH is scarce in the literature. (2) Studies comparing clinical outcomes between laminectomy and osteotomy have not been reported. (3) Results of MAPN with open techniques have not been compared.
We sought to study the outcome of surgery for LDH by conducting a comparative study between three different surgical techniques; we aimed to find whether any of these approaches were more efficacious in reducing pain or improving patients’ quality of life. In addition, factors that could predict the outcome of LDH surgery were assessed.
Materials and Methods
This retrospective study was approved by the research and ethics committee of Shiraz University of Medical Sciences (SUMS), in Shiraz, Iran. From March 2006 to March 2011, 650 cases of spine surgery were performed at SUMS. Three hundred cases of LDH surgery were performed because of (1) persistent radicular pain after 8 weeks of medical and physical treatment, (2) episodes of radicular pain recurring for more than 6 months, (3) motor weakness (except dorsiflexion of big toe). In all, 208 cases were included in our study based on our inclusion criterion of single-level, unilateral LDH. Cases were excluded because of (1) previous history of spine surgery except recurrent cases where their primary surgery was done during the conduction period of this study (e.g., history of spondylolisthesis, spondylolysis, fractures, spinal stenosis, tumors); (2) coexistent pathology except focal stenosis at the level of LDH (e.g., spondylolisthesis, spondylolysis, spinal stenosis, juxtafacet cyst, any intradural pathology). We could not obtain follow-up data on 54 patients despite extensive attempts. Two had died (causes were unrelated to surgery: one had myocardial infarction 2 years postoperation and one had a car accident). We were left with 148 patients who were invited by phone to electively come for a follow-up visit as a part of a research study. They were informed about the nature of the study and its aims. Verbal consent was obtained. Patients were assessed by: (1) pre- and postoperative VAS for back and radicular pain; (2) Resumption of Activities of Daily Living (RADL) scale, 37 standardized Persian version; (3) Japanese Orthopedic Association Back Pain Evaluation Questionnaire (JOABPEQ) 38 ; and (4) a study-specific question that addressed patients’ subjective satisfaction with the operation, residual complaints, and job resumption.
Some authors define recurrence as development of radicular pain after a symptom-free period, such as 6 months, 39 but in our series, we defined recurrence as lower extremity radicular pain 2 months after the surgery that was confirmed by contrast-enhanced magnetic resonance imaging (MRI). We defined failed surgery as symptoms continuing immediately after operation.
Surgical Methods
Laminectomy (74 cases, 48.6%) was performed by bilateral dissection of the paravertebral muscles, partial (one-third to one-half of the lamina's height) laminectomy of the upper and lower laminas, plus flavectomy and facet-saving, disk fragment removal, and unilateral diskectomy.
MAPN (20 cases, 13.2%) was performed with a percutaneous transmuscular approach. 18 A tube for the surgical corridor was used, and partial flavectomy and removal of the upper lamina edge were done. Disk fragments that were seen inside the disk space were unilaterally removed.
Muscle-sparing technique (Fraser) 40 or spinous process osteotomy (54 cases, 35.8%) was performed by unilateral dissection of the paravertebral muscles, osteotomy of the upper and lower spinous processes, flavectomy, laminectomy of one-third to one-half of the upper and lower laminas, along with unilateral fragmentectomy and removal of loose disk fragments.
Diskectomy was performed as fragmentectomy, and all loose or severely degenerated disk particles that were found inside the disk space were removed.
The choice of surgical technique was based on the surgeon and patient preferences.
Data Analysis
Data were analyzed with SPSS version 16.0 (SPSS, Inc., Chicago, Illinois, United States). Statistical significance was set at 0.05. Qualitative comparisons between groups were done with the chi-square test. Qualitative variables (that had two options) and quantitative variables (because they did not demonstrate a normal distribution as determined by Kolmogorov-Smirnov test) were compared by nonparametric test (the Mann-Whitney U test). Qualitative variables (that had more than two options) and quantitative variables were compared with the Kruskal-Wallis test. Repeated-measure analysis was performed for comparing pre- and postoperative change in VAS (ΔVAS) for surgical techniques (within and between groups). Variables studied for possible predictive significance are shown in Table 1. To determine the confounding factors, univariate analysis by the chi-square test was used (variables with p ≤ 0.25 were considered in logistic regression analysis) by performing logistic regression model; it seemed that sex was a confounding factor in comparison with other variables.
Description of outcome predictor variables
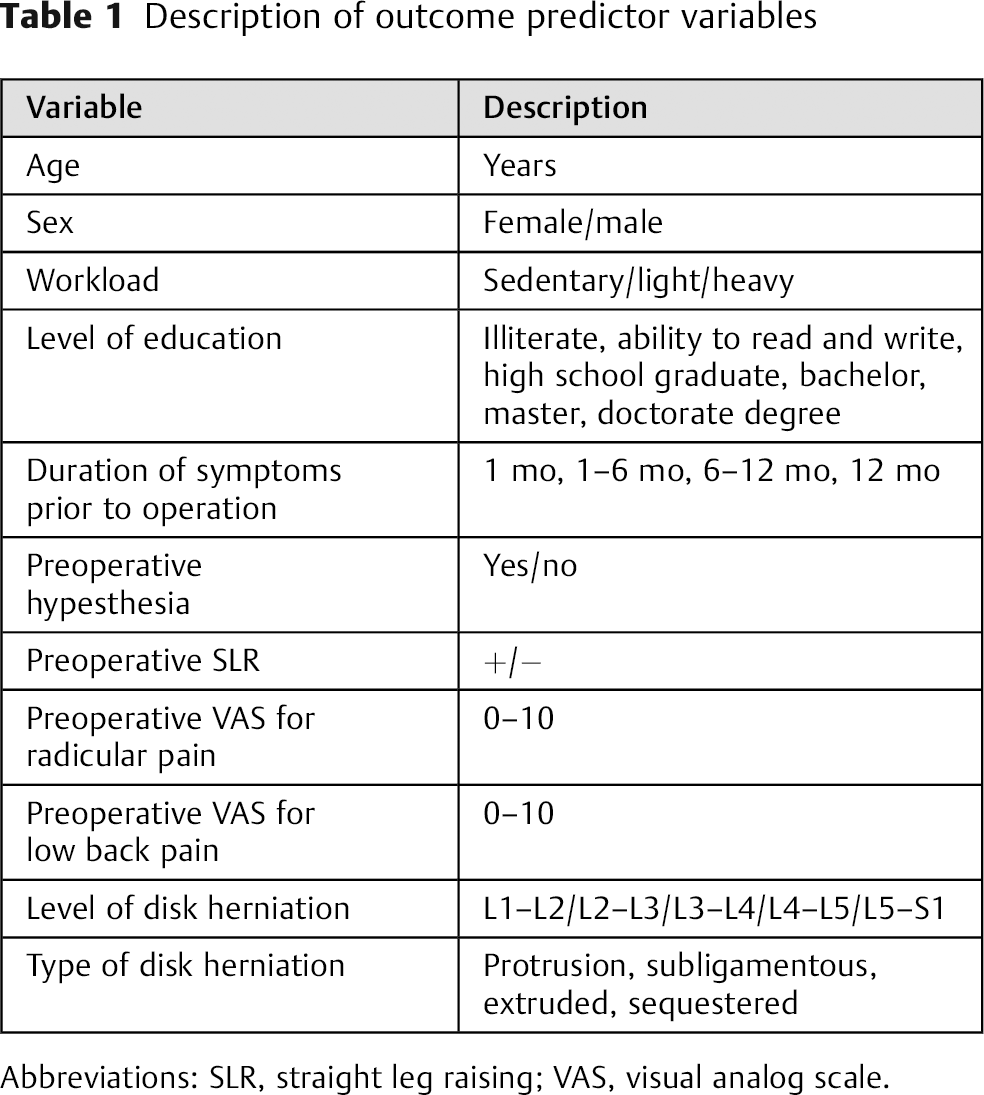
Abbreviations: SLR, straight leg raising; VAS, visual analog scale.
Results
Mean follow-up time of our study was 35.54 ± 15.60 months (minimum 12 months). Mean preoperative VAS for radicular pain and low back pain were 9.12 ± 1.87 (standard deviation [SD]) and 6.69 ± 4.31 SD, respectively. Mean preoperative VAS for back pain was higher in women than men (female = 7.26 ± 4.03 SD, male = 6.03 ± 4.54 SD, p = 0.125). However, the difference was not present on preoperative VAS for radicular pain (female = 9.09, male = 9.07, p = 0.35). Other patient data are shown in Table 2.
Patient data
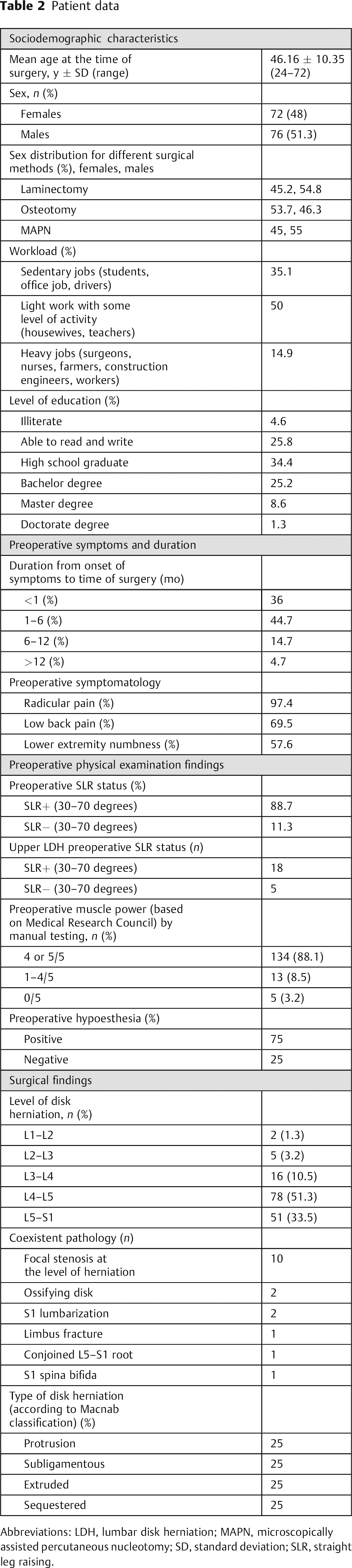
Abbreviations: LDH, lumbar disk herniation; MAPN, microscopically assisted percutaneous nucleotomy; SD, standard deviation; SLR, straight leg raising.
Hospital Stay
A significant correlation (p = 0.001) was seen between duration of hospital stay and surgical approach. The majority of our cases were discharged 24 to 48 hours after the operation. Hospital stays are shown in Table 3.
Duration of hospital stay
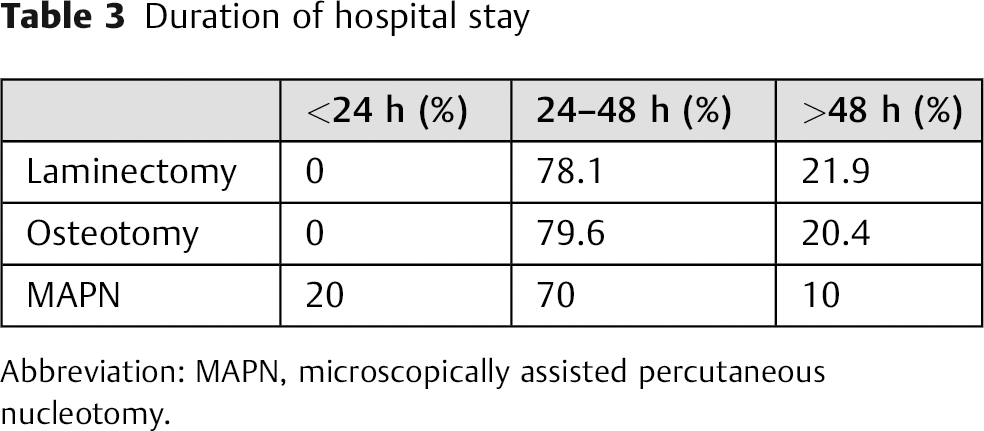
Abbreviation: MAPN, microscopically assisted percutaneous nucleotomy.
Overall Success Rate for Surgery
Overall success rates for LDH surgery as assessed by patient satisfaction with the surgery, ΔVAS for low back pain and radicular pain, RADL, and JOABPEQ are shown in Table 4. As demonstrated in Table 4, success with regard to patient subjective satisfaction with the operation (94%) is almost equal to the success rate with radicular pain, which suggests that the most troublesome symptom for the patient was the radicular pain and its relief brought about satisfaction.
Overall success rate for LDH surgery
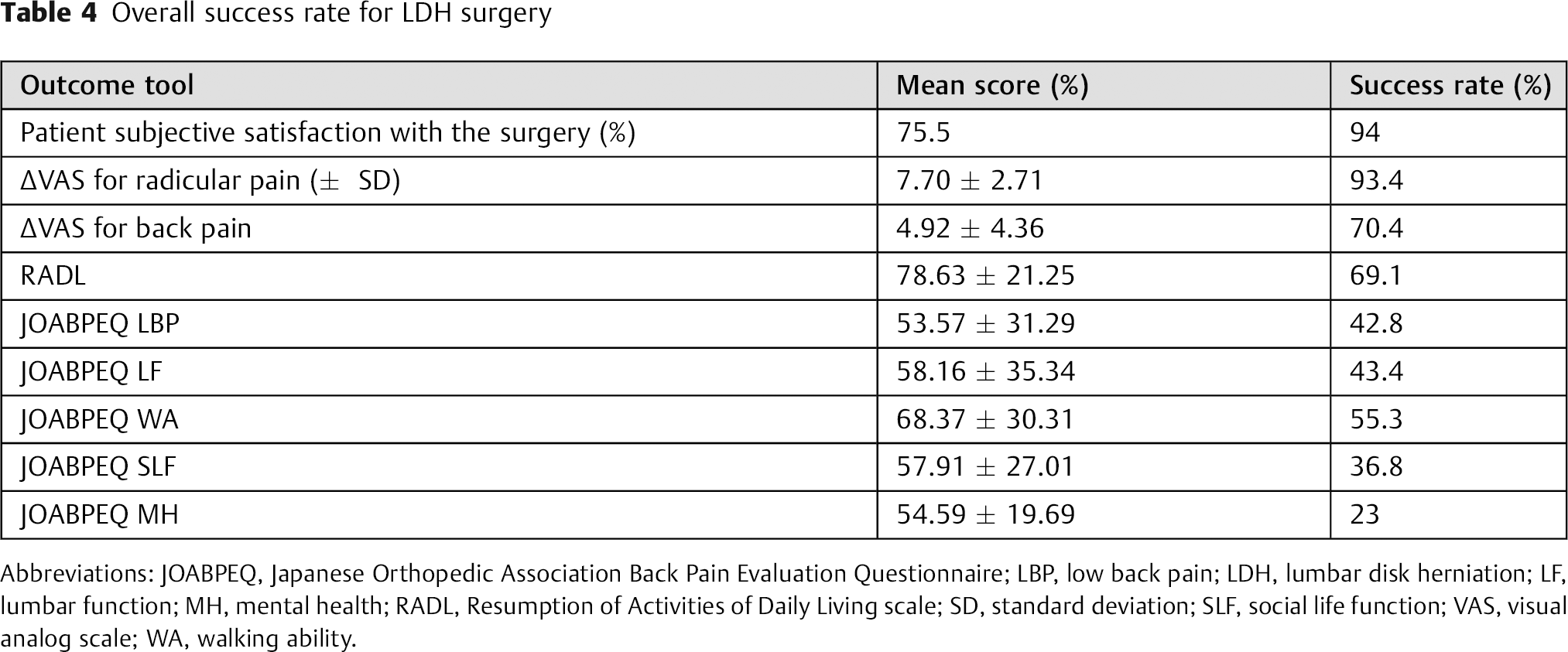
Abbreviations: JOABPEQ, Japanese Orthopedic Association Back Pain Evaluation Questionnaire; LBP, low back pain; LDH, lumbar disk herniation; LF, lumbar function; MH, mental health; RADL, Resumption of Activities of Daily Living scale; SD, standard deviation; SLF, social life function; VAS, visual analog scale; WA, walking ability.
Surgical Complications
Surgical complications were classified into three categories: intraoperative, immediate postoperative, and late. We had a 5.9% complication rate for durotomies. A statistically significant relation (p = 0.007) was found between complications and surgical techniques. Dural tears were reported in one case of laminectomy and four cases operated on with osteotomy and MAPN. Except for one case with evident cerebrospinal fluid leak, in others pinpoint dural tears were sutured with muscle patch and covered with gel foam. One patient developed postoperative chin blister.
Cases with Recurrence
To find out the true rate of recurrence in this study, we excluded cases whose first operation was done before March 2006 and whose revision surgeries were performed during the period of this study. Three patients experienced recurrence (1.98%). The minimum time from primary surgery to revision surgery was 70 days. Two had ipsilateral same-level and one had contralateral different-level recurrences. One of our recurrent cases underwent two revision surgeries. Two had MAPN as their primary surgery. For revision surgeries, laminectomy was done for two. The patient who required two revision surgeries was a 31-year-old man at the time of the primary surgery; the first revision surgery was osteotomy and the second was decompression, fixation, and interbody fusion. Outcome of revision surgeries was assessed by ΔVAS (for back radicular pain) and patient subjective satisfaction with the surgery. We could not use the JOABPEQ and the RADL scale for evaluating the outcome of revision surgeries because one patient underwent revision surgery 70 days after the primary surgery; in those 70 days, the patient was modestly active and had not completely returned to normal activities. Baseline data and outcome of revision surgeries are as follows: mean preoperative VAS for leg pain (±SD) was 9.33 ± 1.15, mean preoperative VAS for back pain (±SD) was 4.66 ± 1.15, mean postoperative VAS for leg pain (±SD) was 2.66 ± 1.15, mean postoperative VAS for back pain (±SD) was 0.66 ± 1.15, mean ΔVAS for leg pain (±SD) was 6.66 ± 2.30, and mean ΔVAS for back pain (±SD) was 4 ± 2. A 100% success rate was achieved for radicular pain according to ΔVAS, and a 66.7% success rate was achieved for back pain as indicated by ΔVAS and subjective satisfaction with the operation.
Precipitating factors like lifting heavy objects and doing heavy exercises were identified in two patients. Of the nine patients suspected of having recurrence, contrast-enhanced MRI revealed adjacent-level disease in three. Medical treatment and strengthening exercises for abdominal and paravertebral muscles were recommended. No statistical significance was achieved between level of herniation, intraoperative complications (durotomy), and recurrence.
Foot Drop Cases
Foot drop is defined as a decrease in ankle dorsiflexion power to 0 to 3/5 (according to Medical Research Council Classification) evaluated by manual testing. There were four cases of foot drop. Three were men and one was a woman. The youngest was 46 years old and the oldest was sixty-six years at the time of operation. Preoperative complaints were back pain, radicular pain, numbness, and inability to walk. Disks involved were at the level of L3–L4, L4–L5 (two cases), and L5–S1. Duration between the symptom of “being unable to walk because of ankle joint weakness” to the time of surgery for two patients was less than 1 month and for two others was between 1 and 6 months. All cases had positive straight leg raising (SLR). Two individuals achieved recovery with surgical decompression. One was a 66-year-old man with L3–L4 disk herniation, with bilateral muscle power for ankle dorsiflexion of 0/5. Laminectomy was performed less than 1 month after the onset of weakness, and his ankle dorsiflexion muscle weakness recovered to 4/5. The second patient was a 46-year-old woman with L3–L4 LDH who had preoperative muscle power of 2/5. She underwent lumbar diskectomy (muscle-sparing technique) within 1 month of onset of weakness and regained her power (4/5) by the first follow-up in 2 months.
Recovery of Symptoms
For 105, 145, and 86 cases, preoperative low back pain, radicular pain, and hypoesthesia were documented, respectively. Rates of recovery (symptom-free individuals) for these symptoms were achieved in 54 (51.4%) of low back pain cases, 102 (70.34%) of radicular pain cases, and 58 (67.44%) with hypoesthesia.
Residual Complaints
We found an overall rate of 71.1% for residual complaints of back and radicular pain and various sensory complaints alone or in combination. Subjectively, the severity of these symptoms did not impair return of these patients to their previous jobs. There was a direct, significant relation between the severity of back pain and leg pain (r = 0.509, p = 0.001), which means those with more intense residual back pain reported more severe residual leg pain. A significant correlation (p = 0.016) was present between surgical techniques and residual symptoms. Among individuals with residual complaints, 48.1% were operated on by laminectomy, and 39 and 12.7% of individuals who reported residual complaints underwent osteotomy and MAPN, respectively. No association was present between preoperative hypoesthesia, type of disk herniation, age, sex, preoperative VAS score for back/radicular pain, duration of symptoms from the onset to the time of surgery, job, preoperative symptoms, level of herniation, or durotomy and residual complaints. Although some patients did not have access to physiotherapy or aqua therapy, 18 and 13 cases who complained of residual back and radicular pain, respectively, did not benefit from these measures when compared with those who had similar complaints but did not use physiotherapy. Fifteen cases with negative preoperative back pain reported back pain in follow-up visits. Most sufferers (nine cases) were operated by osteotomy (mean VAS for back pain: 4.93, mean age: 45). A significant relation (p = 0.001) was present between presence and severity of residual symptoms and JOABPEQ mental health functional score. Individuals with lower scores reported higher degrees of back pain, radicular pain, and lower extremity numbness. Table 5 demonstrates additional data regarding residual complaints.
Residual complaints
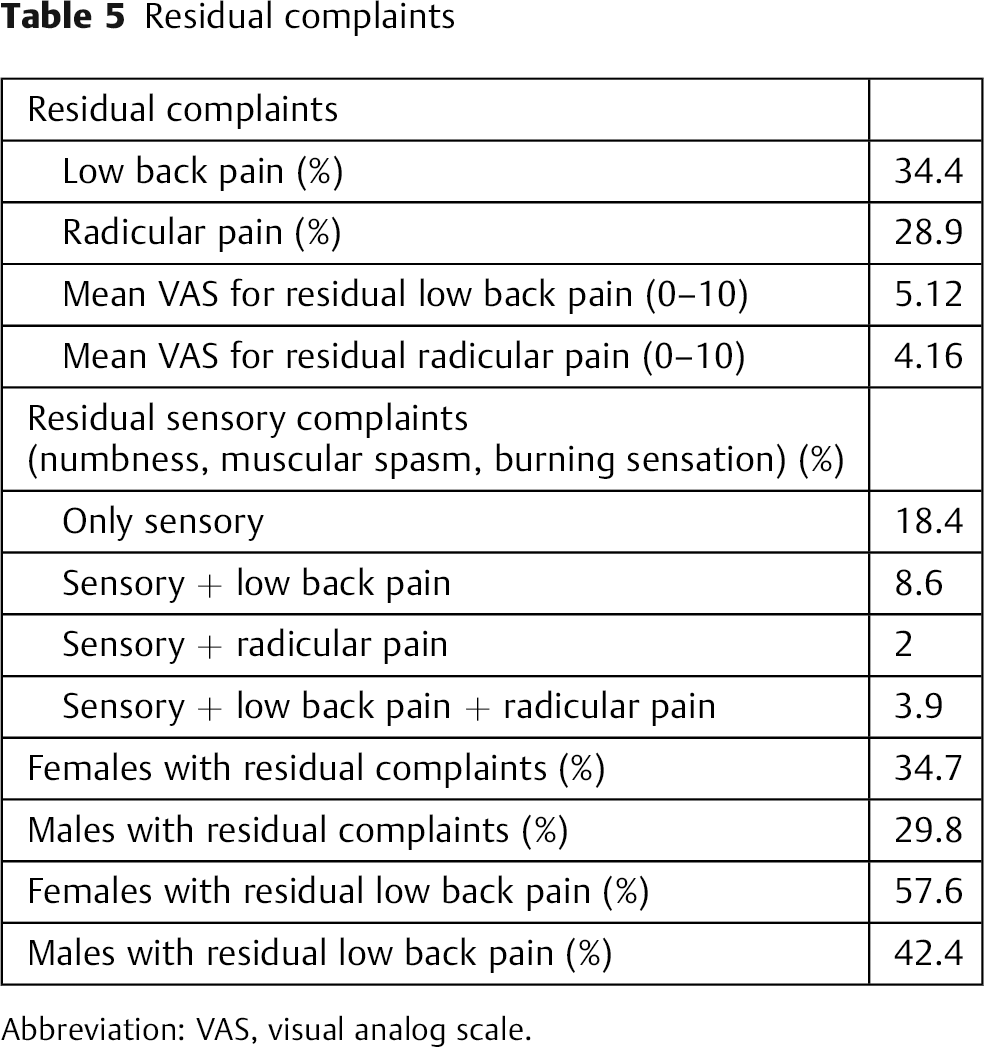
Abbreviation: VAS, visual analog scale.
Results in Elderly Cases
Sixteen cases were above 60 years of age. No significant statistical difference was achieved when we compared outcome of surgery between individuals older versus younger than 60 years of age. Twelve cases had negative SLR. No association was present between the type of herniation and age over 60 years.
Upper LDH Cases
With no statistical significance, surgery for upper LDH cases (L1–L2, L2–L3, and L3–L4) yielded better results when compared with L4–L5 and L5–S1. Of 23 cases with L1–L2, L2–L3, and L3–L4 disk herniation, none had coexisting pathologies. No correlation was demonstrated between upper LDH and workload. There was a significant statistical relation between age and three upper LDH (p = 0.001). The mean age for cases with L1–L2, L2–L3, and L3–L4 disk herniation was 57.50 ± 4.03 SD and 52.43 ± 11.01 SD, respectively (in comparison with L4–L5 with mean age of 46 and compared with L5–S1 cases with mean age of 42). This finding suggests that lower lumbar disks are more vulnerable to mechanical loads, which make them more susceptible to herniation about a decade earlier than upper LDH.
Mental Health
To determine the influence of mental status on outcome, the relation between JOABPEQ mental health functional score and other outcome instruments was studied. Results showed that subjective satisfaction with the surgery (p = 0.001), four JOABPEQ functional scores (p = 0.001 for low back pain, lumbar function, walking ability, and social life function), and RADL scores (p = 0.001) were poorer in cases that had less satisfying JOABPEQ mental health functional score, a finding that draws attention to the influence of psychological status on other outcome measures.
Type of Disk Herniation
Patients with protrusion-type herniation had lower (poorer) outcome by means of JOABPEQ low back pain functional score (p = 0.046). Extruded-type herniation cases showed statistically significant higher (better) score (p = 0.052) for JOABPEQ low back pain functional score. Other than the aforementioned results, no statistically significant relation was found between type of disk herniation and our outcome instruments.
Pregnancy
With each pregnancy, JOABPEQ low back pain functional score decreased by 0.228 points (p = 0.052). No relation existed between number of pregnancies and type of LDH.
Return to Job
Ninety-four percent of our subjects resumed their jobs.
Results of Surgical Techniques
All three surgical approaches resulted in a significant decrease (p = 0.001) in the intensity of preoperative radicular pain and low back pain, but intergroup variations in the outcome with regards to the aforementioned outcome tools were not achieved. As indicated by JOABPEQ low back pain and lumbar function functional scores, laminectomy achieved significantly (p = 0.001) better outcomes in comparison with other methods. Comparisons between different surgical techniques in terms of outcome tools scores and success rates are shown in Tables 6, 7, and 8. Outcome of surgery did not significantly differ by age, sex, level of education, preoperative VAS for back pain, preoperative VAS for radicular pain, return to previous job, or level of herniation.
Outcome measures scores and success rate for individual surgical technique
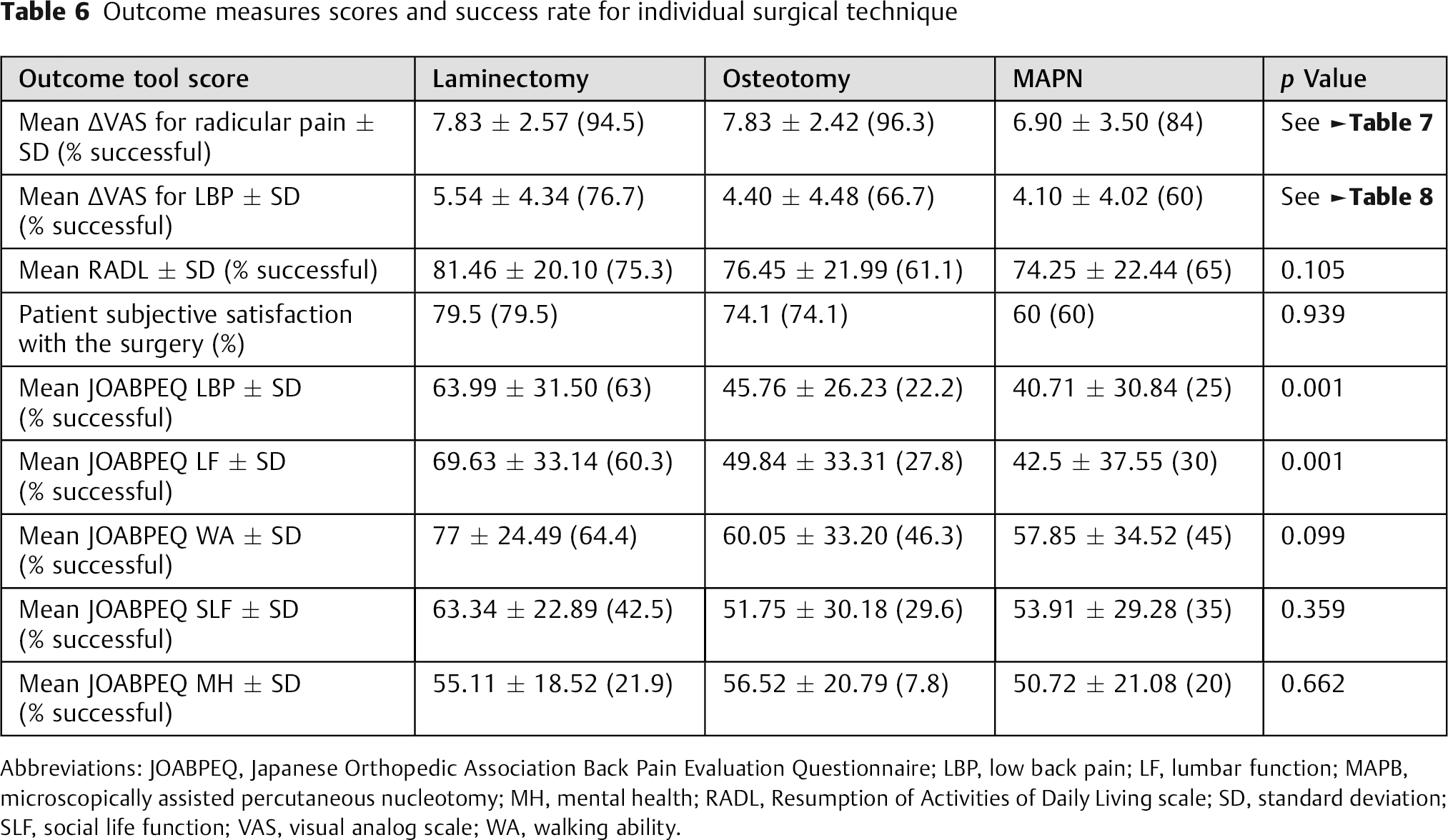
Abbreviations: JOABPEQ, Japanese Orthopedic Association Back Pain Evaluation Questionnaire; LBP, low back pain; LF, lumbar function; MAPB, microscopically assisted percutaneous nucleotomy; MH, mental health; RADL, Resumption of Activities of Daily Living scale; SD, standard deviation; SLF, social life function; VAS, visual analog scale; WA, walking ability.
VAS for radicular pain (comparison between and within surgical techniques)
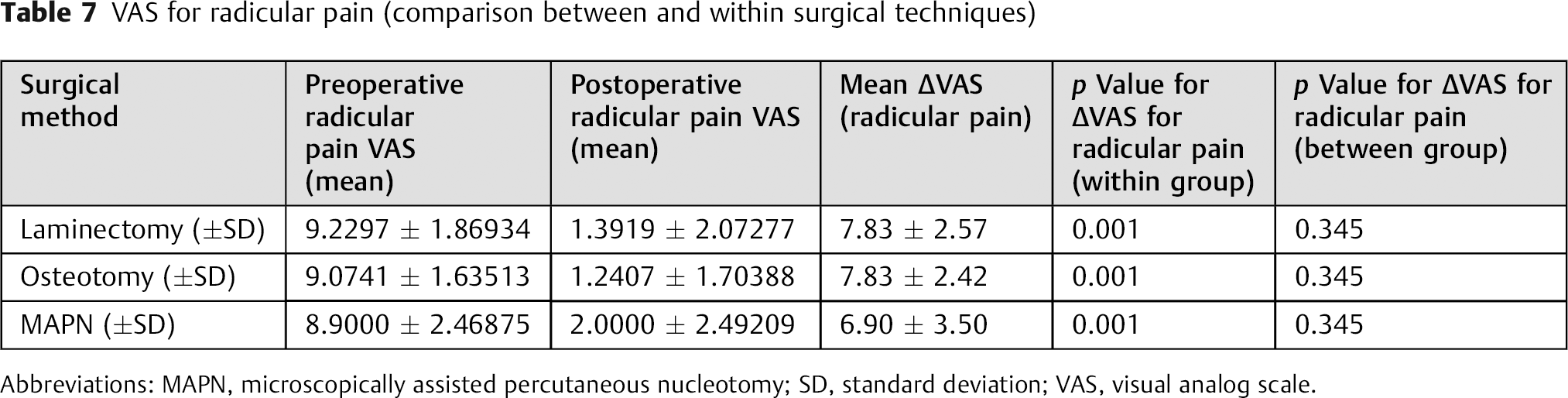
Abbreviations: MAPN, microscopically assisted percutaneous nucleotomy; SD, standard deviation; VAS, visual analog scale.
VAS for back pain (comparison between and within surgical techniques)
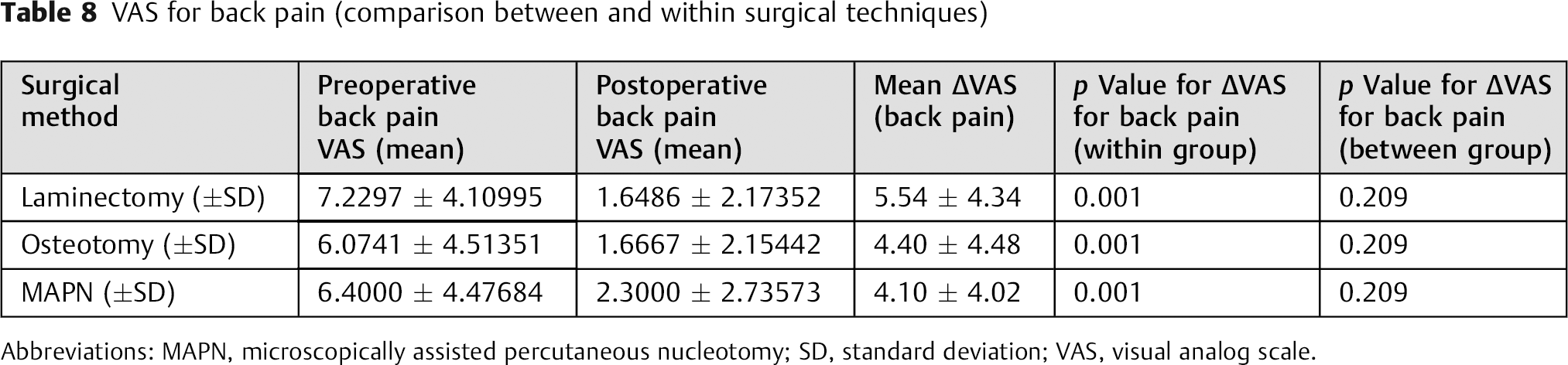
Abbreviations: MAPN, microscopically assisted percutaneous nucleotomy; SD, standard deviation; VAS, visual analog scale.
Factors Predictive of Outcome
The second part of our study was aimed to determine predictive factors in outcome of LDH surgery. A description of the variables is given in Table 1. As demonstrated in Table 9, predictive factors for ineffective surgical treatment for LDH were female sex and negative preoperative SLR. Female sex compared with male sex had two to four times more risk of unsuccessful results, whereas positive preoperative SLR was a predictor for successful treatment. Age, level of education, and preoperative VAS for low back pain were other factors that showed prediction power. The risk of unsuccessful surgical treatment was shown to increases with age. Other factors associated with ineffective surgical management were lower educational level and higher scores for preoperative VAS for low back pain.
Significant outcome predictors
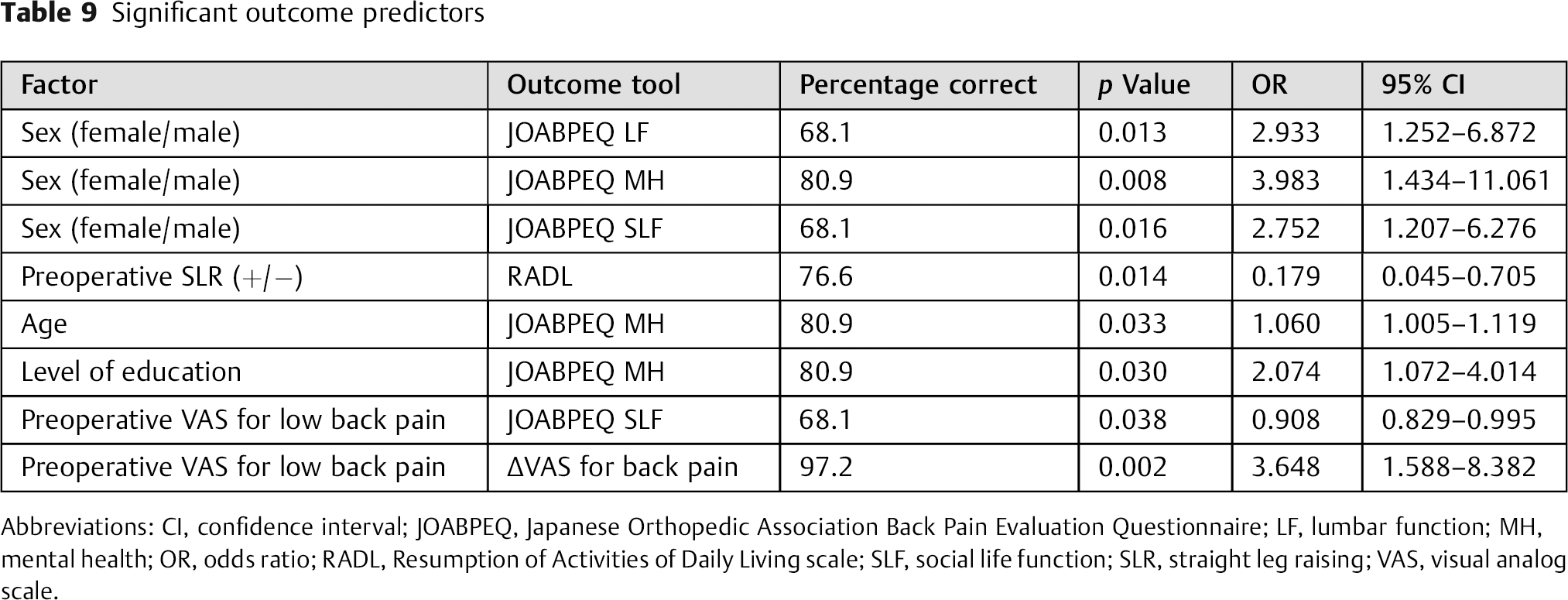
Abbreviations: CI, confidence interval; JOABPEQ, Japanese Orthopedic Association Back Pain Evaluation Questionnaire; LF, lumbar function; MH, mental health; OR, odds ratio; RADL, Resumption of Activities of Daily Living scale; SLF, social life function; SLR, straight leg raising; VAS, visual analog scale.
Discussion
Outcome
There have been several studies on the long-term outcome of LDH surgery. 26 , 29 , 32 , 33 , 35 , 41 , 42 , 43 Few studies have addressed the results of LDH surgery in Iran. 44 , 45 To the best of our knowledge, this is the first study among the Iranian population about the outcome of different surgical techniques and the effect of various factors on the results.
The success rate for LDH surgery despite various outcome measures has been reported to be 56 to 90%. 28 , 30 , 32 , 41 , 46 , 47 , 48 The recurrence rate in our study was 2.6%, which is lower than the rates reported in the literature (7.1 to 12.7%). 49 , 50 , 51 , 52 , 53
The rate of residual postoperative complaints in our study population was 71.1%. Residual back pain occurred in 43.3% of cases, which was higher than one study that reported a 17% rate for backache at the time of follow-up. 54 Naylor in a study conducted on 204 cases of laminectomy reported 32 patients with postoperative lower extremity numbness, cramps, and paraesthesia. 54 In that study, 15.68% of cases had postoperative sensory deficits, which is less than our rate for the group with only sensory complaints (18.4%). Also in that study, 5 of 32 cases with sensory symptoms were in the backache group. We had 13 patients (8.6%) who reported sensory deficits and back pain together. Different causes of back pain following LDH surgery have been proposed. 55 Although Ostelo et al evaluated residual complaints at 3- and 12-month follow-up, they demonstrated that baseline back and leg pain predicted residual back and leg pain. 56 In our series, we did not note this relation.
Although we did not find a relationship between type of herniation and postoperative residual back pain, we found that cases with extruded-type disk herniation had better JOABPEQ low back pain functional score. Another study reported that the degree of low back pain was relatively lower for extruded cases as compared with that for protruded or sequestered cases. 57
Recovery of foot drop has been documented in some literature. 58 , 59 , 60 , 61 Ghahreman et al suggested that severity of motor deficit prior to surgery and the age of the patient were important prognostic predictors of the recovery of ankle dorsiflexion weakness. 58 Girardi et al found no statistically significant relation between extent of recovery and age, diagnosis (herniated nucleus pulpous, lumbar canal stenosis), or severity of preoperative weakness. 59 The severity of preoperative weakness has been found to be an important prognostic factor in two studies. 60 , 61 Although Ghahreman et al found no relation between duration and outcome, 58 other studies noted the importance of preoperative symptom duration as a factor in recovery of foot drop. 60 , 61 We had a small study population of four foot drop cases, but we could not find any relation between preoperative duration of weakness, preoperative weakness severity, or age and recovery.
In our series, 23 cases with upper LDH were identified. Sanderson et al concluded that surgical outcome in terms of postoperative back and radicular pain was worse for herniated disks at L1–L2 and L2–L3 compared with those at L3–L4. 62 Our results do not support the previously mentioned result. None of our cases had coexisting or preexisting pathologies in upper LDH, a finding that is not in agreement with another study. 63 The mean age for this kind of disk involvement in our study (53 years) is slightly higher than other studies (40.7 and 50 years). 63 , 64 Gutterman and Shenkin reported that 78% of their cases had satisfactory relief of pain. 65 Satisfactory operative results were achieved in 90% of patients in a study conducted by Wei et al. 66 Seventy-eight percent (18/23) of our patients having upper LDH were completely satisfied with their surgery.
Fujii et al suggested that outcome of lumbar diskectomy in elderly patients was as good as in younger patients. 67 Our findings are in line with this study by Fujii et al.
Although one study found that sequestered-type herniation was more common in elderly patients, 67 we did not find a relationship between age and type of herniation. Our findings agree to some extent with those of Jönsson and Strömqvist, 68 , 69 who reported that with increasing age there was a decreasing prevalence of highly restricted positive SLR test results, and the prevalence of severe reduction of walking capacity increased.
Dural tear incidence has been reported to be 2.7% for LDH surgery 70 and 3.2% for spine surgery. 71 In our series, we encountered a 5.9% rate of incidental durotomies. It has been suggested that durotomy predicts poor outcome of surgery. 71 In our series, cases with durotomy demonstrated poorer outcome as indicated by JOABPEQ walking ability functional score (p = 0.001).
Predictors
One study demonstrated longer duration for preoperative sensory deficits among predictors of poor outcome. 72 In our study, preoperative hypoesthesia did not show sufficient statistical power to be included in the analysis of predictive factors.
Effect of age on outcome of LDH surgery has been reported to be a statistically significant short-term predictor, 73 but Graver et al, who had 7-year clinical follow-up, suggested that age had no statistically significant prognostic value. 32 We found that risk of unsuccessful surgical treatment increased with age.
Den Boer et al found that lower level of education was a predictor of unfavorable outcome. 74 Oslon et al found that surgical outcomes did not differ by level of education. 75 However, in our series, we found higher educational level to be a predictor of success.
Several studies have reported that depression and psychological condition of patients undergoing LDH surgery play a role in the outcome. 47 , 74 , 76 , 77 , 78 , 79 , 80 , 81 , 82 , 83 Edwards et al 76 found that distress and anxiety had a negative effect on pain and function. Den Boer et al supported the relation between unfavorable outcome and psychological complaints. 74 Arpino et al 81 also demonstrated a negative prognostic effect of depression. Our finding by means of JOABPEQ mental health functional score is consistent with previous studies and confirms that psychological status is important in outcome evaluation studies for LDH surgery. Studies addressing results of LDH surgery should encompass the psychological status of individuals as well.
Duration of preoperative radicular pain has been suggested to influence the outcome of LDH surgery in several studies. 46 , 72 , 73 , 84 , 85 , 86 , 87 , 88 Ng et al 89 found less favorable outcome in patients with duration of leg pain more than 12 months. Rothoerl et al 72 found duration of leg pain more than 60 days to be among negative outcome predictors. Duration of pain in our study did not attain the statistical qualification to be included in the logistic regression analysis, but with no statistically significant relation, we found preoperative pain duration of 6 to 12 months yielded satisfactory results compared with durations of less than 1 month, 1 to 6 months, and more than 12 months.
In our series, female sex was associated with unsuccessful clinical outcome. Peul et al suggested that female sex was a strong predictor of unsatisfactory outcome at 1 year for patients with sciatica. 90 Strömqvist et al also found that at 1-year follow-up, females reported a higher rate of consumption of analgesics, a higher degree of postoperative back and leg pain, and less improvement regarding disability and some aspects of quality of life. 69 Although the previously mentioned study reported patient outcome at 1-year follow-up, we also found a higher rate for females with residual back pain (female = 57.6%, male = 42.4%). Sex was not a statistically significant predictor for outcome in one short-term study, 73 but was reported to have a minor influence on the 1-year outcome in another short-term study. 32
Loupasis et al did not suggest a relationship between poorer results and the level of surgery. 33 Generally, our findings are in line with Loupasis et al. 33
We found positive preoperative SLR to be a predictor for success in the outcome of surgical management for LDH. Kohlboeck et al found Lasegue sign to be a high risk factor for poor outcome. 47 Moranjkic et al reported that preoperative tension sign was not a statistically significant predictor of short-term outcome. 73 Positive SLR association with poor outcome was demonstrated by Vroomen et al. 91
Hurme and Alaranta evaluated patients at 1 and 6 months postoperatively and reported that the operative finding of protrusion predicted a poor result. 85 Moranjkic et al 73 found that extrusion-type disk implied better outcome. Folman et al 87 reported better outcome for noncontained herniation as compared with contained herniation. Although type of disk herniation in our study did not show a predictive power, we found significantly poorer results for protrusion-type herniation in JOABPEQ low back pain functional score, and extruded-type herniation cases showed statistically significant higher score by means of JOABPEQ low back pain functional score.
To the best of our knowledge, severity of preoperative low back pain has not been reported as an outcome predictor. As indicated by two of our outcome instruments, higher preoperative VAS for low back pain was a risk factor for not achieving success with surgical management of LDH.
Conclusion
Surgery for LDH is an effective treatment in terms of reducing radicular pain (93.4%). All three surgical approaches resulted in significant decrease in the intensity of preoperative radicular pain and low back pain, but intergroup variations in the outcome were not achieved. As indicated by JOABPEQ low back pain and lumbar function functional scores, laminectomy achieved significantly better outcomes compared with other methods. Relief of radicular pain was associated with subjective satisfaction with the surgery among our study population, as evidenced by the decrease in radicular pain and the subjective satisfaction with the operation. Factors associated with poor success in our surgeries were female sex, negative preoperative SLR, age, and level of education.
Disclosures
Mahsa Sedighi, none
Ali Haghnegahdar, Board membership: Iranian Board of Neurosurgery; Consultant: Shiraz University of Medical Sciences
Footnotes
Acknowledgment
We deeply appreciate Mohsen Akparpour (SUMS) for his efforts in performing the statistical analysis of this study and also Esmaeil Ghaedsharaf (SUMS) for his guidance on some of the digital aspects related to this work.