
Abstract
Study Design:
Cross-sectional study.
Objectives:
Our aim was to describe age-dependent changes of lumbar paraspinal muscle endurance and morphology in Chinese healthy population. We also explored the relationship between paraspinals endurance and morphology.
Methods:
A total of 181 participants from Chinese community population without chronic low back pain were included. The participants were divided into three groups: young (20-39 years old, n = 29), middle (40-59 years old, n = 93), and elderly (≥ 60 years old, n = 59). The Ito test was performed to evaluate the isometric endurance of paraspinal muscles. The total cross-sectional area (TCSA) and fat infiltration (FI) of multifidus (MF) and erector spinae (ES) were measured at L1-L5 levels on magnetic resonance imaging. Physical activity level was evaluated using the physical activity index and comorbidities were assessed by the modified 5-item frailty index.
Results:
The elderly group had a shorter performance time of endurance test than the young group and middle-aged group. Correlation analysis showed that age had a significant correlation with endurance test, the average MF TCSA, MF FI, ES TCSA and ES FI of L1-5. In addition, PAI had a significant correlation with endurance test and MF FI. In multiple linear regression analysis, paraspinals endurance was associated with MF FI, ES FI, physical activity level and comorbidities.
Conclusion:
Age-related decreases in paraspinals endurance and TCSA, and an increase in FI were revealed. Besides, paraspinal muscles FI, but not TCSA, was negatively associated with the endurance of paraspinals.
Introduction
It is common that paraspinal muscle degeneration occurs in elderly population. 1 Sarcopenia, obesity, and osteoporosis are associated with the degeneration of paraspinal muscles with age. 2 Multiple studies have revealed that paraspinal muscle degeneration is implicated in degenerative lumbar pathologies.3-5 Besides, the relationship between paraspinal muscles deficits and several inferior complications after lumbar surgery has raised considerable attention. 6
Evaluating the endurance of paraspinal muscles can directly reflect the muscle function. Several studies have investigated the endurance of trunk extensor muscles in chronic low back pain (LBP) population.7-9 However, few studies evaluated it across the lifespan to provide the reference data. On the other hand, previous studies have evaluated paraspinal muscle morphology across the lifespan of healthy population,1,10-12 whereas few studies have reported on the reference data of healthy people with quantitative magnetic resonance imaging (MRI) in China. In addition, there still exists inconsistent results in whether paraspinal muscle morphology is correlated to muscle function.13-15
As paraspinal muscle degeneration is considered to be potential prognostic and diagnostic markers for spine health, depicting paraspinal muscle change in healthy people as a baseline is crucial. 16 The purpose of this study was to: (I) assess the age-dependent differences in the endurance test and paraspinal muscles morphology in healthy Chinese population to provide reference data of paraspinal muscle degeneration; (II) explore the relationship between paraspinal muscles endurance and morphology.
Methods
Participants
260 participants from the community were recruited via print advertisements posted in senior centers and physician offices and social media accounts related to Peking University. The included participants would be paid for their times as an incentive. Before included in this study, every subject had underwent a history taking and physical examination. The inclusion criteria were: (1) Age ≥ 18 years; (2) without chronic LBP. We defined chronic LBP as LBP of at least moderate intensity (3/10 or greater intensity on a numeric pain-rating scale) that occurred at least 4 days per week for a duration of greater than 1 year according to previous studies.17,18 The exclusion criteria were: (1) with previous spinal surgery or arthroplasty, spinal fracture, neurological or orthopaedic diseases; (2) pregnant; (3) other serious chronic diseases impacting daily life; (4) unsuitable for undergoing an MRI examine. Finally, 181 participants were included in our study. The participants were divided into three age groups: young (20-39 years old, n = 29), middle (40-59 years old, n = 93), and elderly (> 60 years old, n =59).
All participants received a participant information sheet and gave their written informed consent. This study was approved by Peking University Third Hospital Medical Science Research Ethics Committee (M2019400).
Data Collection
Age, height, weight, body mass index (BMI), physical activity level, smoking and comorbidity were collected for each participant. Physical activity level was evaluated using the physical activity index, which can provide an estimate of overall energy expenditure of daily activity based on self-report.19,20 A questionnaire was administered by the interviewers to determine the average number of hours per day a participant spent in each of five levels of physical activity (basal, sedentary, slight, moderate, and heavy). The hours for each activity level were multiplied by corresponding weighting factors (1.0, 1.1, 1.5, 2.4, and 5.0 respectively), and the results summed to determine the physical activity index. 20 The modified 5-item frailty index is a concise comorbidity-based risk stratification tool that was calculated based on the presence of the 5 co-morbidities: congestive heart failure within 30 days prior to surgery, insulin-dependent or noninsulin-dependent diabetes mellitus, chronic obstructive pulmonary disease or pneumonia, partially dependent or totally dependent functional health status at time of surgery, and hypertension requiring medication. 21 Each category was assigned a ‘0’ if the comorbidity is absent or ‘1’ if the comorbidity is present. The comorbidity score was then calculated based on the sum of each of the 5 categories.
Paraspinal Muscle Endurance Test
The Ito test was performed according to previous studies (Figure 1).7,22 The participants were in a prone starting position on an examination table with a 10-cm-high pad placed under the lower abdomen to decrease the lumbar lordosis. The participants were instructed to raise their upper body to an individual adjusted endpoint (by ∼15°). Simultaneously, the arms were kept parallel to the body axis, the cervical spine was held in a neutral position, looking down, and both feet remained on the examination table throughout the entire test. The test would cease until they felt voluntary fatigue or for a maximum of 5 min. Task failure was determined by a drop in the angle of trunk of greater than 10° at any point.
23
The test started with a trial for recognition, followed by 5 min rest for baseline data and then two recorded trials with 5 min rest in between. The result of endurance test was identified as the best record of two trials. The illustration of Ito test for measuring paraspinal muscle endurance.
Paraspinal Muscle Evaluation on MRI
All enrolled participants had undergone MRI of lumbar area with Signa HDxt 3.0T (General Electric Company; repetition time, TR, of 3038 ms and echo time, TE, of 118 ms). The slice thickness was 3 mm with a 3-mm gap between each slice. Multifidus (MF) and erector spinae (ES) were measured bilaterally from T2-weighted images at the inferior endplate of the vertebral body of L1-L5 levels. The following parameters were measured on each level by the Image J software and mean values of bilateral parameters were calculated: total cross-sectional area (TCSA; including functional muscle and intramuscular fat; Figure 2A) of MF and ES; fat infiltration (FI) of MF and ES were measured by the previously reported thresholding technique.24,25 Thresholding technique can identify two different signal intensity peaks and classify the pixel areas with higher intensity peaks as intramuscular fat (Figure 2B). FI was calculated by the fraction of pixels representing fat/ (number of pixels representing fat + number of pixels representing muscle). We also calculated the mean values of TCSA and FI from L1 to L5. (A) Measurements of paraspinal muscular parameters on axial T2-weighted MRI. Regions of total cross-sectional area of multifidus (1), erector spinae (2) at L4 level were outlined by yellow lines. (B) Thresholding technique to highlight intramuscular fat area (red area).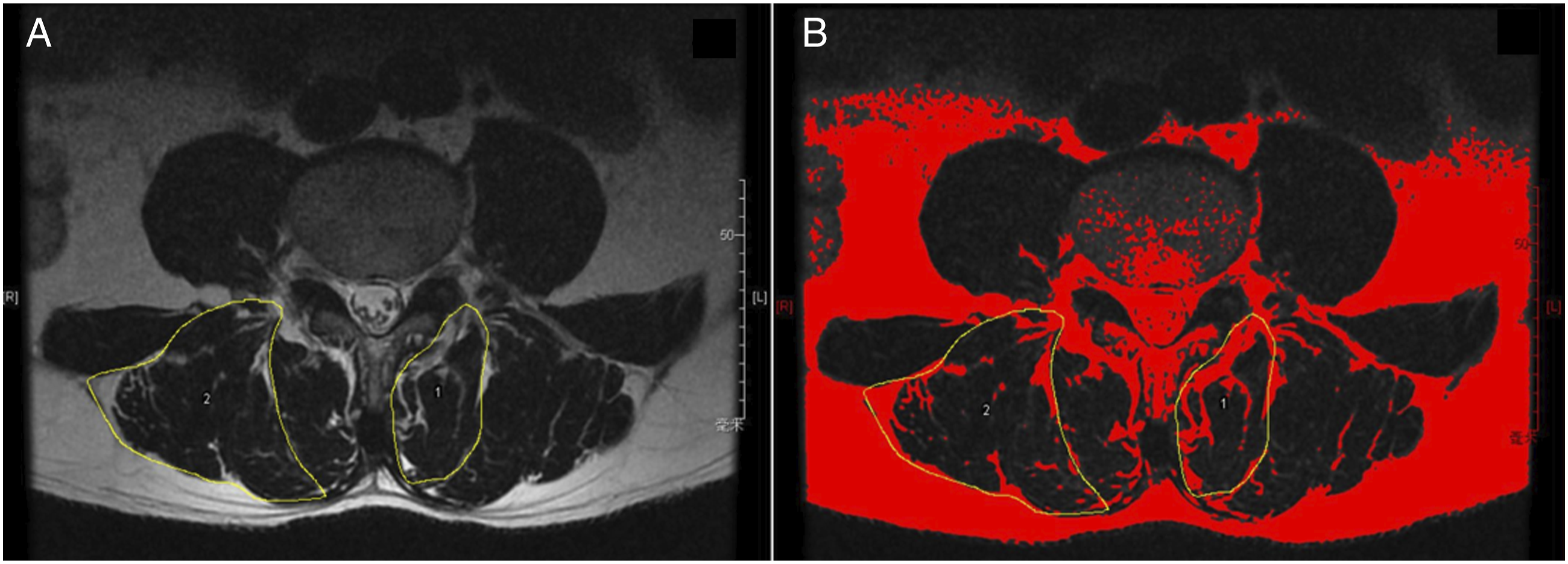
All muscular parameters of 20 participants were randomly selected and were measured by the two observers independently to test the reliability. After 3 weeks, the same measurements were performed by each observer. The ICCs for both intra-rater and inter-rater reliability of MF TCSA, ES TCSA, MF FI and ES FI were > .8.
Statistical Analysis
Statistical difference analysis of clinical characteristics, endurance test and paraspinal muscle parameters between the three groups (young, middle and elderly) were performed using Kruskal-Wallis H test, and P values were adjusted using Bonferroni correction. Chi-square test was also used for categorical data. The relationships between age, height, weight, BMI, physical activity index, performance time of endurance test and imaging parameters of paraspinal muscles were evaluated using Spearman correlations, depending on the distribution of the variables. Multiple linear regression analyses constructed by enter method were used to explore the relationship between the endurance test and muscular parameters. Sex, age, height, weight, BMI, physical activity index, comorbidity and muscular parameters were included in four models. Intraclass correlation coefficient (ICC) of the intra- and inter-reader reliability for muscle parameters was calculated (two-way random, absolute agreement, and single measures). Statistical significance was set at P value < .05. All statistical analyses were performed using SPSS 22.0 (IBM Corp).
Results
Clinical Characteristics and Paraspinal Muscle Function in the Young, Middle-Aged and Elderly Groups.
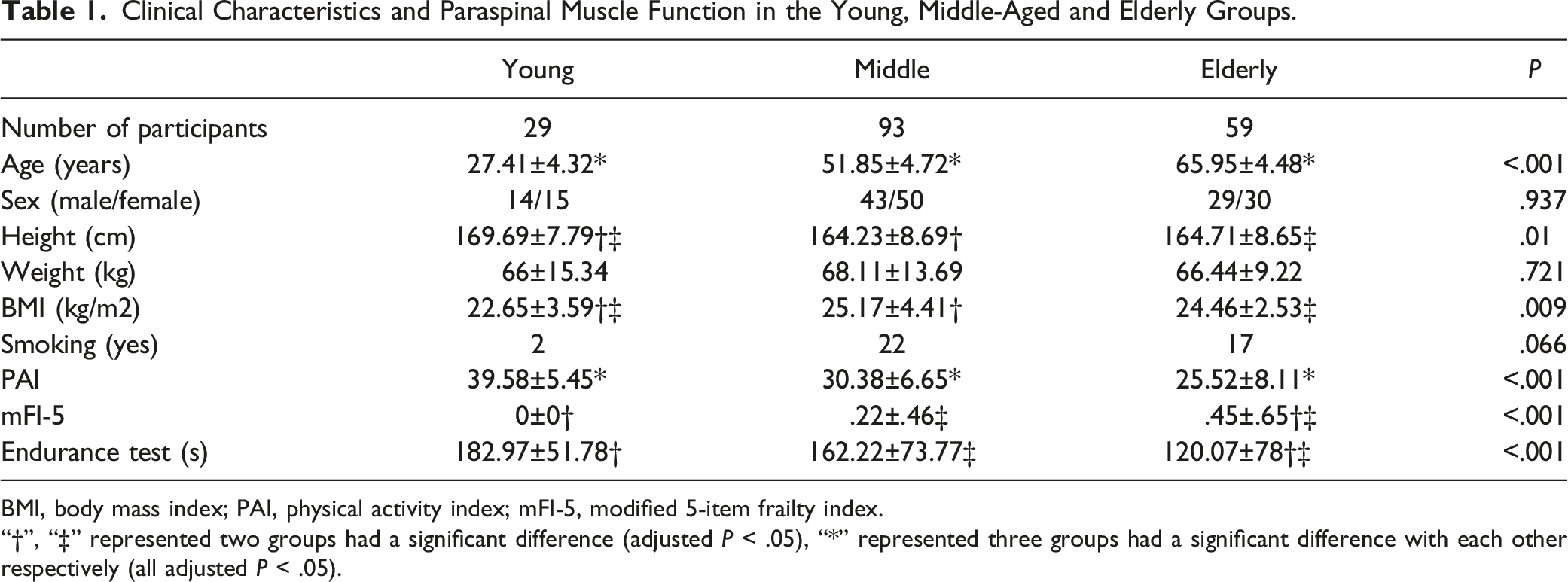
BMI, body mass index; PAI, physical activity index; mFI-5, modified 5-item frailty index.
“†”, “‡” represented two groups had a significant difference (adjusted P < .05), “*” represented three groups had a significant difference with each other respectively (all adjusted P < .05).
The results of the endurance test in the young, middle-aged and elderly groups were 182.97±51.78, 162.22±73.77 and 120.07±78, respectively. The elderly group had a shorter performance time of endurance test than the young group and middle-aged group (all adjusted P < .05; Table 1).
Distribution of Cross-Sectional Area and Fat Infiltration of Paraspinal Muscles in Young, Middle-Aged and Elderly Groups.
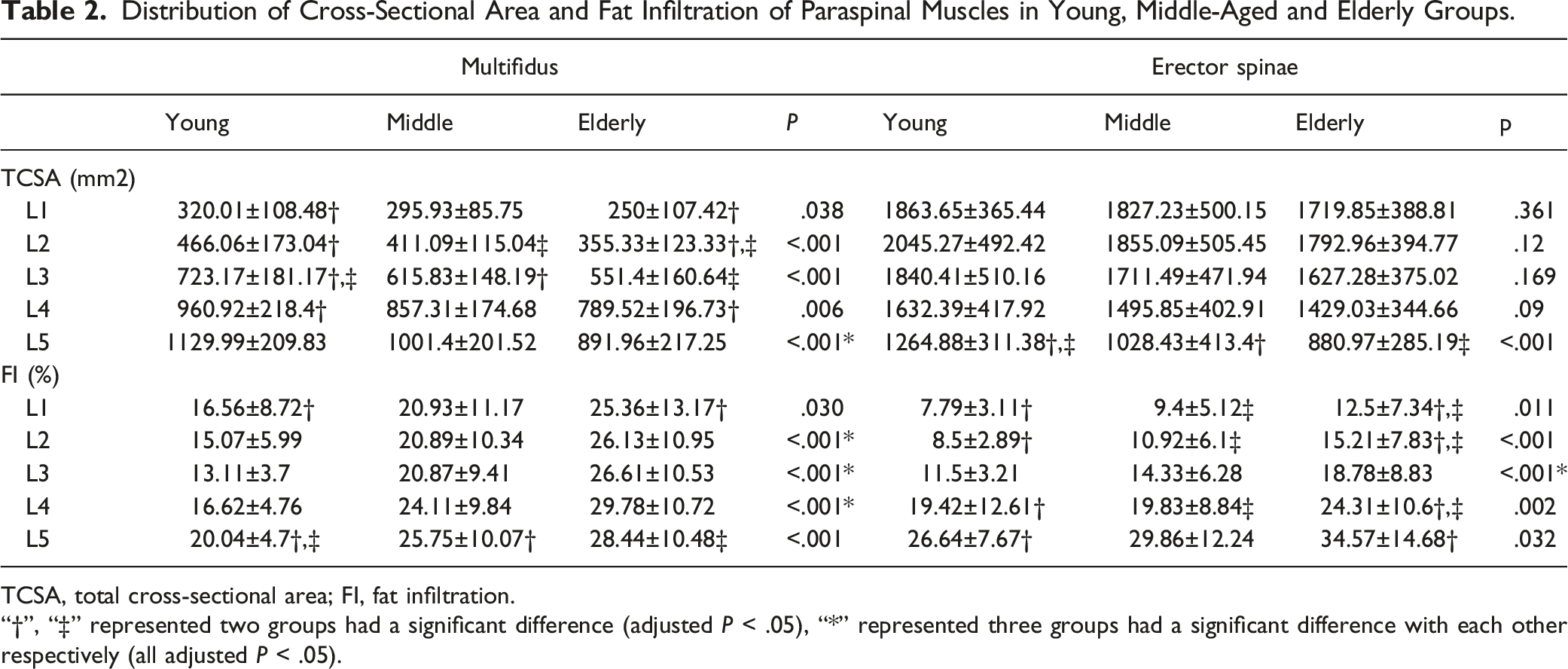
TCSA, total cross-sectional area; FI, fat infiltration.
“†”, “‡” represented two groups had a significant difference (adjusted P < .05), “*” represented three groups had a significant difference with each other respectively (all adjusted P < .05).
Spearman Correlation Coefficient between Clinical Characteristics, Endurance Test and the Mean Values of Paraspinal Muscle Parameters from L1 to L5.
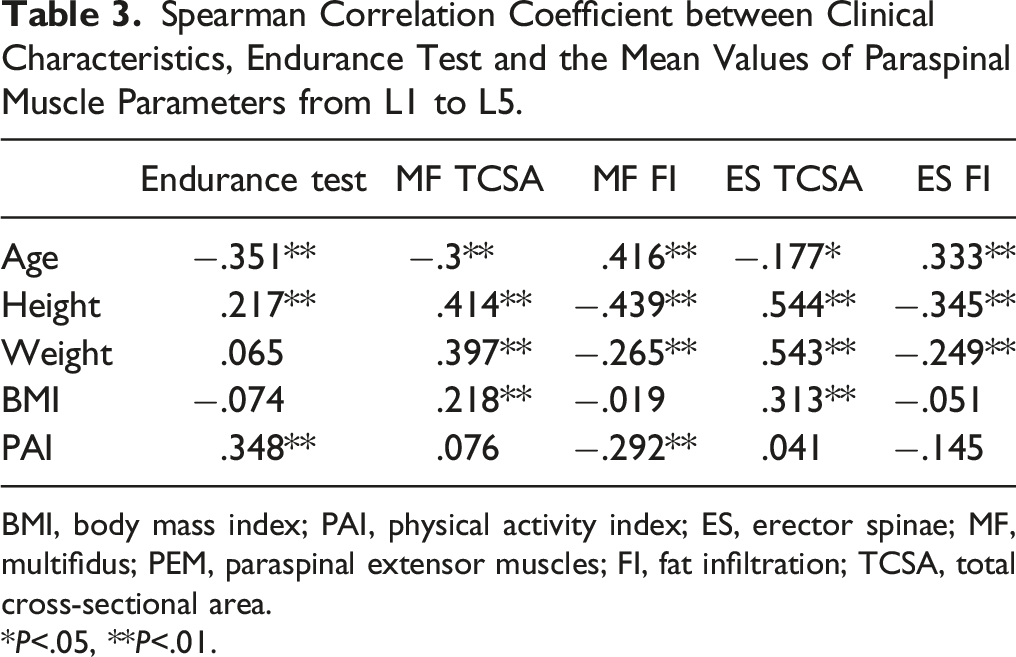
BMI, body mass index; PAI, physical activity index; ES, erector spinae; MF, multifidus; PEM, paraspinal extensor muscles; FI, fat infiltration; TCSA, total cross-sectional area.
*P<.05, **P<.01.
Correlation analyses showed that age had significant correlations with the performance time of endurance test, the average MF TCSA, MF FI, ES TCSA and ES FI of L1-5 (r = −.351, P < .01; r = −.3, P < .01; r = .416, P < .01; r= −.177, P < .05; r= .333, P < .01, respectively; Table 3). We also found positive relations of BMI with the average MF TCSA and ES TCSA of L1-5 (r = .218, P < .01; r = .313, P < .01, respectively; Table 3), but no relations of BMI with FI (all P > .05). In addition, physical activity level was significantly correlated with the performance time of endurance test and the average MF FI of L1-5 (r = .348, P < .01; r = −.292, P < .01, respectively; Table 3).
Multiple Linear Regression Analysis of the Relationship between Endurance Test and Paraspinal Muscle Parameters.
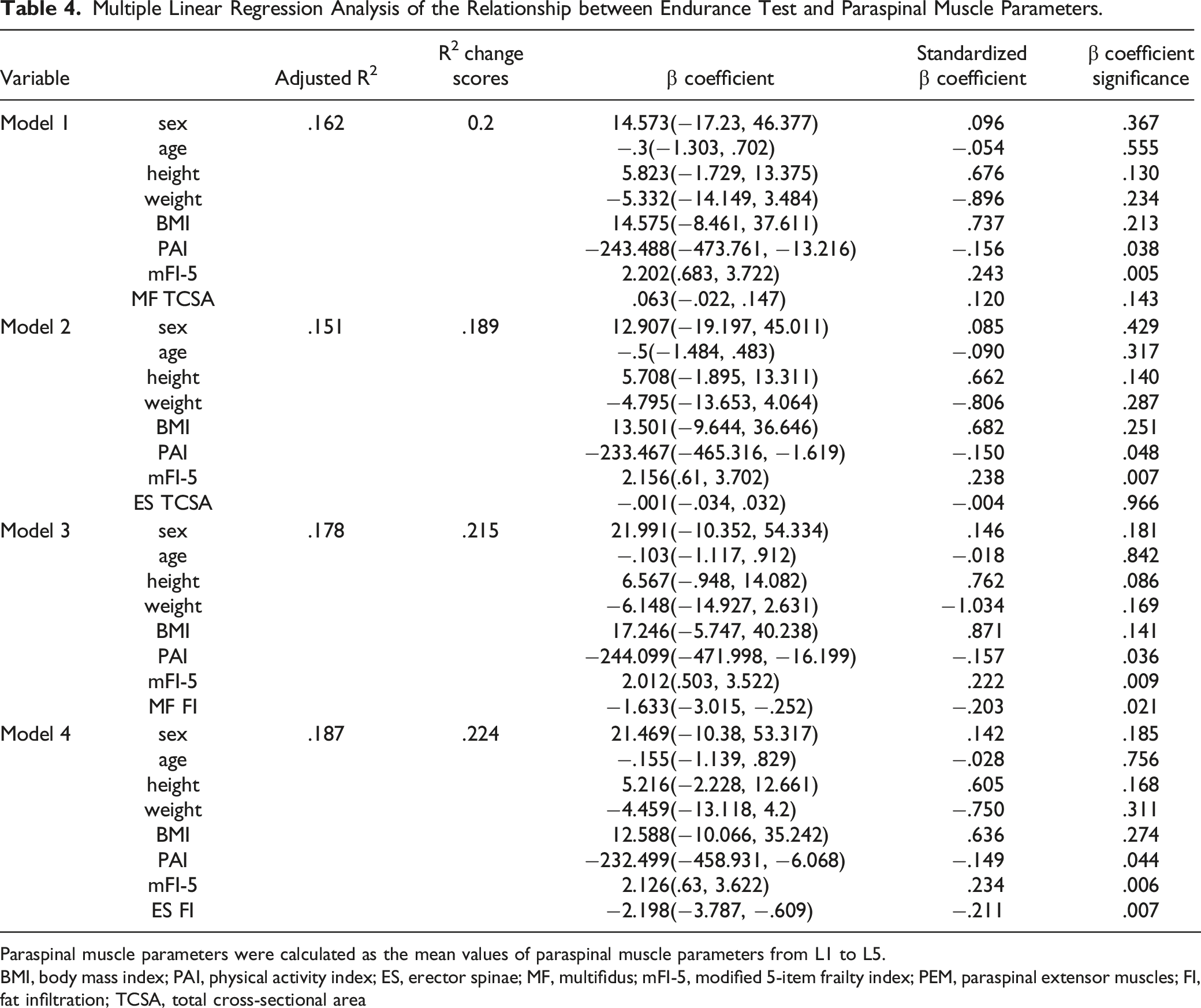
Paraspinal muscle parameters were calculated as the mean values of paraspinal muscle parameters from L1 to L5.
BMI, body mass index; PAI, physical activity index; ES, erector spinae; MF, multifidus; mFI-5, modified 5-item frailty index; PEM, paraspinal extensor muscles; FI, fat infiltration; TCSA, total cross-sectional area
Discussion
In this study, we evaluated the endurance of paraspinal extensor muscles with Ito test and quantified cross-sectional area (CSA) and FI of paraspinal muscles using MRI in 181 men and women aged 20-80 years-old. This healthy Chinese population-based study have examined the age- and level-dependent distributions of function and morphology in paraspinal muscles, which is important as a reference for future comparative studies and to find the cut-off values as prognostic factors. Several studies have proposed some cut-off values of paraspinal muscle degeneration to predict the prognosis of clinical outcomes in patients with degenerative lumbar diseases.26-28,29 However, determining a reasonable cut-off value needs the data of normal people as the reference since it calculated only through receiver-operating curve might be impractical. Besides, few studies have examined the relationship between quantitative paraspinal muscle evaluation on MRI and muscle endurance.
Several studies have reported that evaluating the muscle endurance has greater discriminative validity than maximal voluntary contractile force.30,31 Ito test was designed for evaluating isometric endurance of the trunk extensor muscles, which has been improved on the basis of Sorensen test. 7 With a high reproducibility and safety, multiple studies have applied it into clinical practice and used it to discriminate between healthy people and patients with LBP.7,8,23 However, the age-dependent distributions and influencing factors of the endurance test are still indistinct. In our study, we found that the elderly group had a less position-holding time than both the young group and the middle group, indicating 60 years might be a potential age where a significant change of endurance occurs. Our finding was in accord with previous study that the fatigue of back muscle was correlated to age. 32
Magnetic resonance imaging is the gold standard for estimating muscle mass among numerous measuring techniques applied in research and routine clinical practice. 33 For muscular morphology, we found an age-related decrease in TCSA and an increase in FI of paraspinal muscles in most levels in the Chinese population, suggesting progressive degeneration of muscle quantity and quality could be a part of the normative aging process. These findings were consistent with previous studies.1,10-12 Some plausible explanations including immobility and reduced levels of and responsiveness to growth hormone and androgens have been reported as the mechanisms of muscle degeneration. 34 It seems that Chinese population have a smaller CSA but a lower FI of paraspinals when compared with Caucasian population, 35 and have a higher FI than Japanese population. 36 We also found that MF and ES TCSA in the young, middle and elderly groups were all greater than those in Peng et al’s study. 1 The reason might be that Peng et al’s study only included Chinese female participants. It has been proved that back muscle mass is larger in men than women. 36 Besides, MF and ES FI in the young and middle group were slightly lower but in the elderly group was higher than those in Peng et al’s study.
Notably, MF showed wider and earlier muscular atrophy than ES in our study. This phenomenon seems to be interpreted by the relationship between stress loading and muscle degeneration. Some studies have reported that MF showed higher stress and fatigue than ES during back extension. 37 Moreover, our findings exhibited that the atrophy of both MF and ES at L5 were most remarkable when compared with any other levels. A specific pattern of degeneration starting at L5 and extending to the upper levels has been showed in our study, which was accordant with previous studies.10,36
In terms of muscle composition, we found a prominent age-dependent change of MF FI and ES FI at all levels. Besides, the degeneration pattern of MF and ES were similar. Lee et al 10 have reported that the age-dependent fatty degeneration appeared wider in ES than MF on computed tomography. They also found that the level-dependent FI of ES showed a similar pattern with MF, but the change of ES seemed to start earlier in age than MF at L5-S1. Furthermore, it seemed that FI showed more significant age-related differences than TCSA. The similar results have been reported by Dallaway et al 38 and Maryse et al. 35 It is likely that increase in non-contractile tissue size may mask age-related muscular atrophy of the paraspinals.
In our study, extensor muscle endurance was positively associated with physical activity level. Previous studies have demonstrated that exercise could facilitate paraspinals function.39,40 They emphasized that exercise in the early postoperative period contributed to improvements in clinical status and muscle function. In addition, we found that physical activity was negatively associated with MF FI, which was consistent with previous studies.41-43 Physical activity significantly decreases in older age resulting in the deterioration of muscle function and the accumulation of intramuscular fat.
Whether paraspinals morphology was associated with muscle function remained inconsistent in previous studies.15,13,44 We found a negative correlation between paraspinal muscles FI and the endurance time in multivariate analysis. Several studies have revealed that increased FI was correlated to poorer function and weakness.13,14 Our findings indicated that the relationship between TCSA and muscle endurance was not as significant as that of FI. This result was in line with Schlaeger et al 13 and Gibbons et al. 15 They found that ES FI, but not CSA, remained a statistically significant predictor of relative extensor strength in multivariate regression models. Gibbons et al found that the position-holding time of back extension endurance test was unrelated to the cross-sectional area of paraspinal muscles. 15 When surgeons find a high FI of paraspinals on preoperative MRI, they may associate it with a poor muscle function. The patients with poor muscle function may have sagittal imbalance and a higher risk of screw loosening.27,45 Consequently, surgeons can adjust surgical plan in advance, like using screws with greater fixation strength.
The present study has several limitations. First, the study population may not be representative of the general population because participants were recruited from only one area of China. Besides, the included participants might tend to be more active in their health given the way we recruited. However, our study investigating a reference data with a relatively large sample size is conducive to explore the cut-off value as well. Several studies have proposed some cut-off values of paraspinal muscle degeneration to predict the prognosis of clinical outcomes in patients with degenerative lumbar diseases.26,27 Second, combining with lumbar degeneration could aggravate the degeneration of paraspinal muscles. Whereas in this study all participants were without chronic LBP and obvious degenerative lumbar diseases, thus we considered the study population could demonstrate age-related physiological changes. Third, the absence of a standardized test procedure of Ito test might limit the use of it and influence the results. However, we have performed the endurance test with a detailed procedure according to previous studies.
Conclusion
In conclusion, we measured the isometric endurance using Ito test and TCSA and FI of paraspinal muscles using MRI in the Chinese population ranging in age from 20 to 80 years-old, providing a normal reference data of paraspinal muscle function and morphology. There was a tendency toward progressive decrease in the endurance of paraspinal muscles with age. Our study also showed an age-related decrease in TCSA and an increase in FI in both MF and ES. Besides, physical activity level had a significant correlation with the endurance test and MF FI. Moreover, the isometric endurance was associated with paraspinal muscles FI, physical activity level and comorbidity in multivariate analysis. Future studies are required to investigate the cut-off values of paraspinal muscle degeneration for predicting the clinical outcomes for surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Clinical Cohort Construction Program of Peking University Third Hospital, China National Key Research and Development Program (2018YFB1307700) and the Accurate Diagnosis and Treatment Technology of Bone and Joint Diseases Research.