
Abstract
Study Design
Cross-sectional observational study in a prospective cohort.
Objective
To analyze the cervical alignment characteristics and their chain of correlation in a sample of asymptomatic individuals.
Methods
Asymptomatic adults who had full spinal radiographs performed. Cervical radiographic parameters were measured, including upper cervical curvature (McGregor line-C2), lower cervical curvature (C2-C7), McGregor slope, and sagittal vertical axis from C2-C7 (CSVA) and T1-slope (T1S). Subjects were stratified by age into 3 groups (18-39 years, 40-59 years, and >60 years), and radiographic parameters were compared across age groups and based on sex.
Results
102 asymptomatic subjects (mean age, 50 years) were included. The T1S significantly increased with age, accompanied by an increase in C2-C7 lordosis. The cervical sagittal alignment, represented by CSVA, did not significantly differ based on age. There was a close correlation among the cervical sagittal parameters, such that the CSVA may be predicted based on the T1S and C2-C7 lordosis. Comparisons of the normative values identified in the present study with those reported in previous studies demonstrate variability in what constitutes normal in different populations.
Conclusion
This analysis of cervical alignment in a sample of asymptomatic volunteers revealed that with increasing age there is an observed increase in the sagittal inclination of the base of the cervical spine (T1S) that is accompanied by an increase in cervical lordosis as a means of maintaining cervical sagittal alignment (CSVA). The variability in what constitutes normal values for cervical parameters suggests that further study is warranted using standardized methodologies across diverse populations.
Introduction
The cervical spine is the most complex spinal region.1-3 The range of motion of the cervical spine enables it to facilitate the very fundamental function of keeping the head near the center of gravity with maintenance of horizontal gaze and with minimum energy expenditure.4,5 It is well established in the literature that cervical alignment correlates with and is impacted by the subjacent thoracolumbar regions and pelvic alignment as a means of providing compensatory changes that are ultimately intended to maintain functional horizontal gaze. 2
Historically, lordosis was viewed as the normal sagittal alignment for the cervical spine and loss of this lordosis, whether segmental or regional, was considered to be pathologic and potentially a form of deformity.6-8 However, recent studies have suggested that a straight or kyphotic cervical spine may also represent normal alignment in a significant proportion of asymptomatic individuals, depending on subjacent spino-pelvic alignment.9,10 Thus, the question of what constitutes “normal” cervical alignment and what defines the thresholds of cervical deformity remain unclear and are topics of ongoing research and debate. Although some kyphosis may be present in asymptomatic individuals, it is notable that kyphosis is also by far the most common cervical deformity11,12 and has been correlated with neck pain, spinal cord compromise, and myelopathy.13-15 Although its precise radiographic definition remains unclear, when present and symptomatic, cervical spine deformity is associated with severe negative effects on health-related quality of life, comparable to other very debilitating chronic conditions including blindness, emphysema, renal failure, and stroke.11,12
Over the last 2 decades, thoracolumbar and spino-pelvic radiographic parameters, including normative global and regional measures, have been extensively studied, and progress has been made in establishing what constitutes normal sagittal alignment and the thresholds for deformity. Fewer publications have studied normative cervical parameters and none has focused on an ethnic population from South America. Significant differences in thoracolumbar and spino-pelvic radiographic alignment have been reported across different geographic and ethnic populations and have enabled a better understanding of the diagnosis and treatment of deformities.16-19 The purpose of this study was to analyze the normative cervical alignment parameters and their chain of correlation in a sample of asymptomatic individuals from a Brazilian cohort.
Methods
Design, Setting, Participants, and Ethics
This is an observational cross-sectional study of asymptomatic adult volunteers, conducted with institutional review board approval. A total of 146 volunteers were recruited from March 2014 through June 2015. Written informed consent was obtained from all study individuals. Adults over 18 years of age without significant spine symptoms (visual analog scale less than 2 out of 10) were included. Exclusion criteria were: previous spinal or neurological surgery, underlying neurological or neuromuscular conditions, history of spinal trauma or neoplastic disease, and/or complaint of hip/knee/ankle/foot disability that could potentially alter the ability to obtain accurate standing radiographs. During the radiographic evaluation, we excluded volunteers who were found to have thoracolumbar scoliosis (Cobb angle ≥20°)
Variables and Measurements
Demographic data was collected, including sex and age. All radiograph images were acquired following an established protocol: coronal and sagittal full-length spinal radiographs, with volunteers standing with a comfortable posture, fingers on their clavicles or on their face and their shoulders at a 45° forward position. 21 Radiographic parameter measurements were performed using Surgimap software (Nemaris Inc, New York, USA), a validated tool for spinal analysis. 22
Assessed radiographic parameters were: (1) total sagittal cervical alignment, measured as the Cobb angle from the occiput to C7; (2) upper cervical angle (UCA), Cobb angle between McGregor’s line (line between the hard palate and the opisthion) and lower endplate of C2
9
; (3) lower cervical angle (LCA), Cobb angle between the lower endplate of C2 and the lower endplate of C7
3
; (4) T1-slope (T1S), angle between the horizontal plane and T1 endplate
3
; (5) McGregor’s slope (McG-Slope), angle between McGregor’s line and the horizontal
4
; and (6) the cervical sagittal vertical axis (CSVA), measured as the distance between a plumb line dropped from the centroid of C2 and the posterior superior corner of C7
3
(Figure 1). The mismatch between cervical lordosis (CL; C2-C7 Cobb angle) and T1S (CL-T1S) was also calculated for all volunteers. For the CL, a negative value was adopted for lordosis and positive for kyphosis. Lateral cervical radiograph illustrating the parameters considered in the present study. UCA: upper cervical angle; LCA: lower cervical angle; McG: McGregor; CSVA: cervical sagittal vertical axis. (A) Extracted image from Surgimap software (Nemaris Inc., New York, USA). (B) Illustration of the measurement of the considered parameters.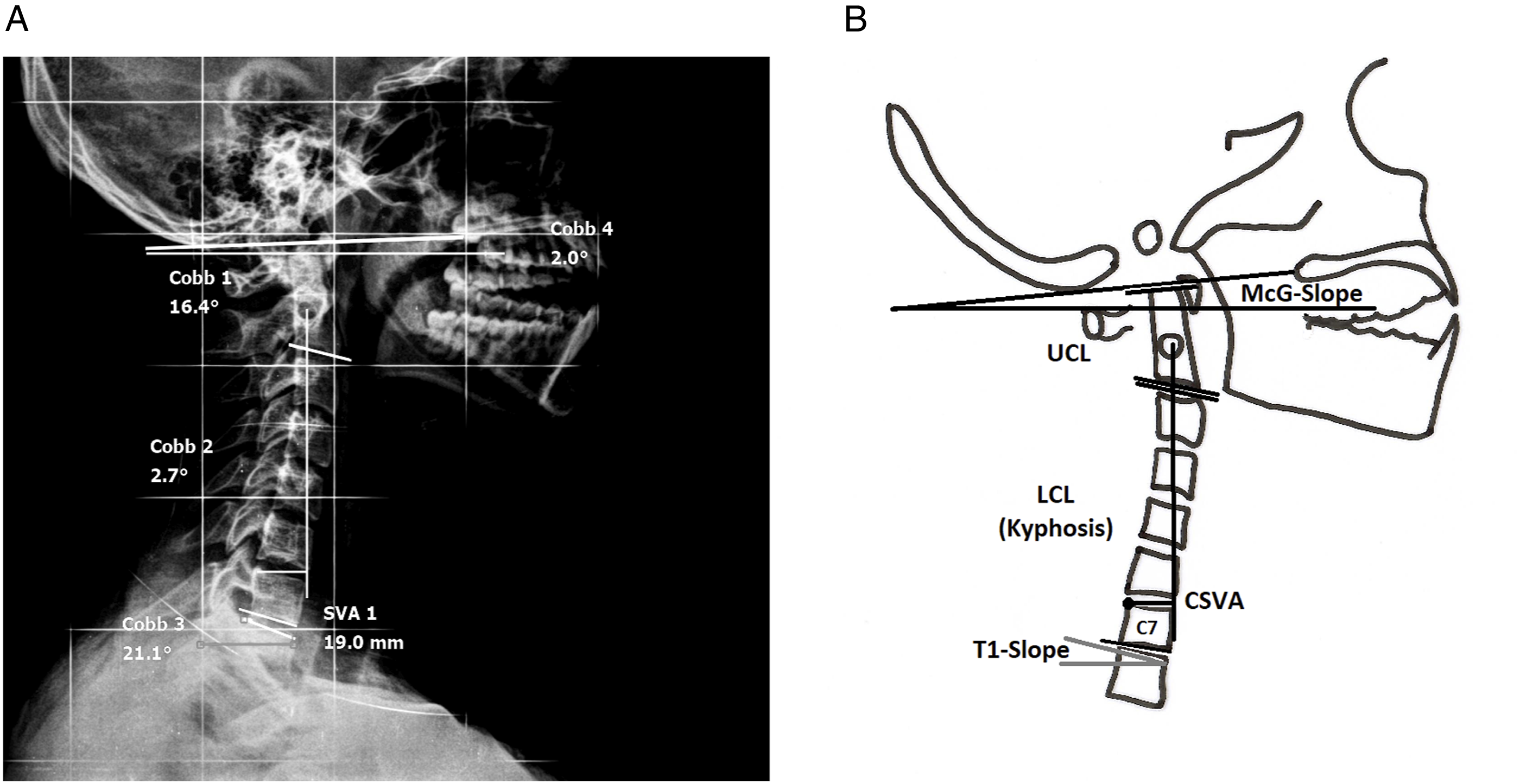
All radiographic measurements were performed by the senior author, an experienced spinal surgeon in practice, twice with an interval of 2 weeks. The concordance between the measurements was almost perfect (intraclass correlation coefficient >.85).
Statistical Analysis
Statistical analysis was performed using SPSS, version 20.0 (IBM Corp, Armonk, NY, USA). The normality of the data was investigated using the Kolmogorov–Smirnov test. The subjects were stratified by age into 3 groups: 18-39 years, 40-59 years, and ≥60 years. The mean, standard deviation (SD), and range for each parameter in each group were calculated. Radiographic parameters were compared based on sex using Student’s t-test, and radiographic parameters were compared based on age group using ANOVA. Pearson product-moment correlation coefficients were calculated to identify potential relationships between various radiographic parameters, and a multilinear regression model was subsequently created to predict CSVA using other parameters. The level of statistical significance was set at .05.
Results
Population Data
A total of 102 (70% of the patients enrolled) volunteers met study criteria and were included in this study. The mean age of the cohort was 49.9 years (SD= 14; range, 18-77 years). 84 volunteers (82%) were women. The mean TPA was 5.4° (SD: 5.9°), with no significant difference based on sex or age group (P>.05). The 3 age groups included: 24 subjects (24%) in the 18-39-year-old group, 46 (45%) in the 40-59 year-old group, and 32 (31%) in the ≥60 year-old group.
Radiographic Values
Mean, Standard Deviation, and Range for radiographic parameters for the entire cohort.
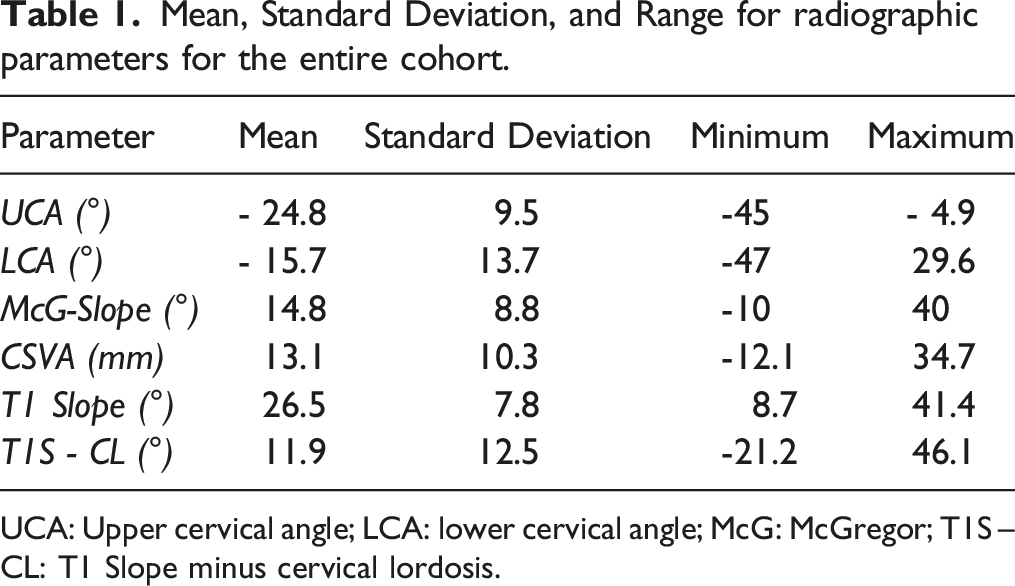
UCA: Upper cervical angle; LCA: lower cervical angle; McG: McGregor; T1S – CL: T1 Slope minus cervical lordosis.
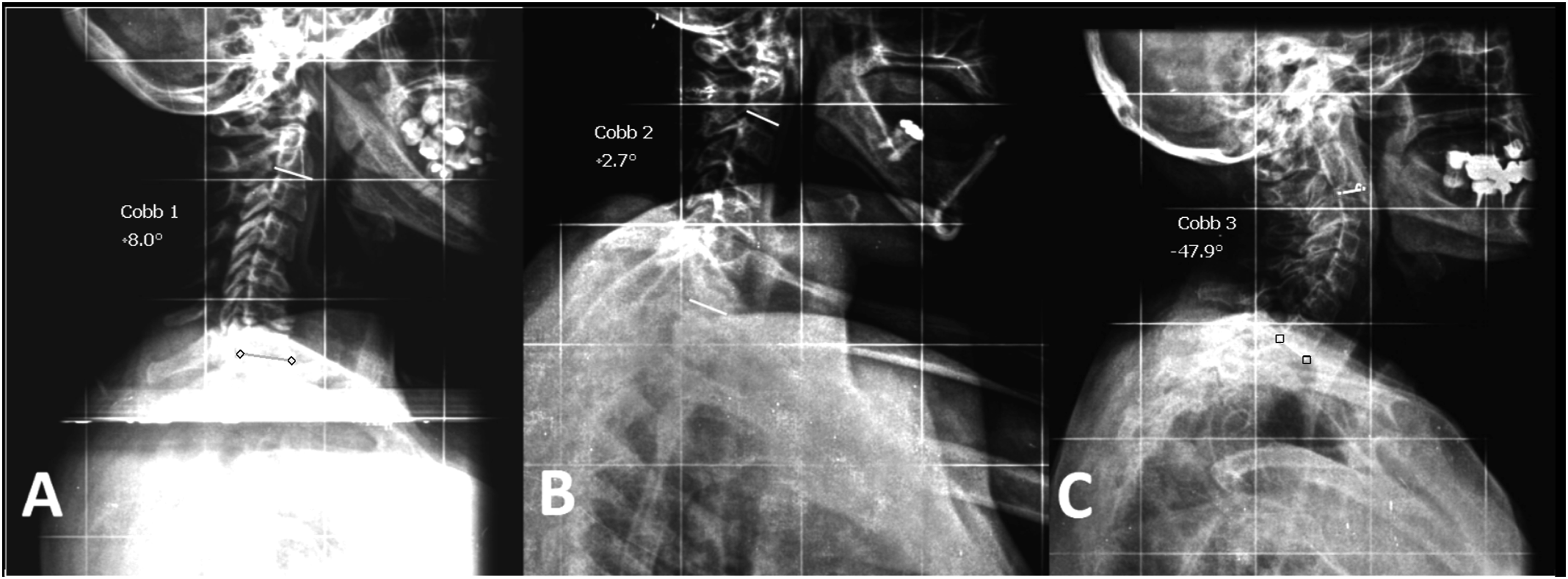
Example of the range of cervical sagittal alignment: (A) kyphotic cervical alignment; (B) relatively straight alignment; and (C) high cervical lordosis (>10° of lordosis).
Comparison of radiographic parameters between individual’s sex.
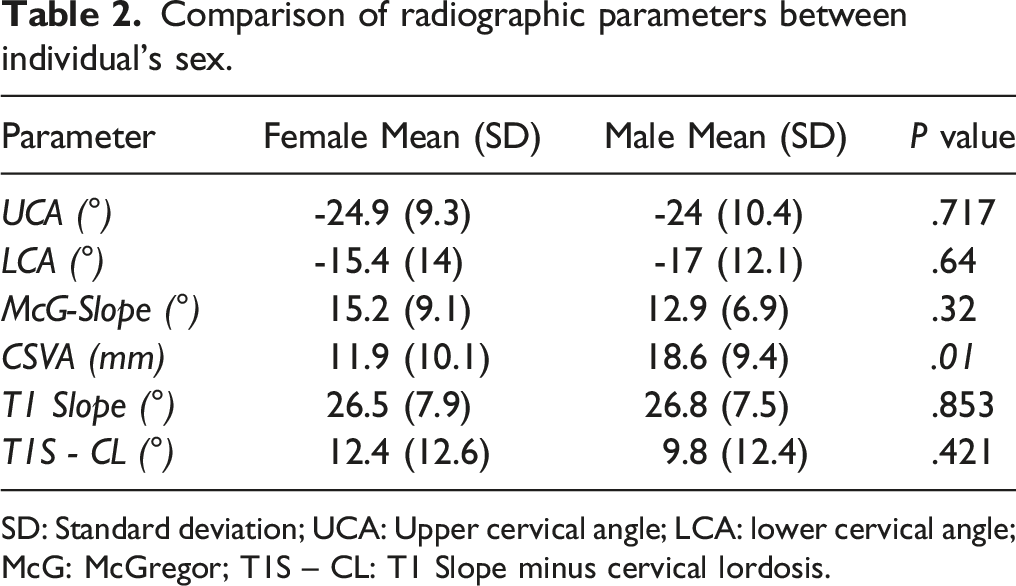
SD: Standard deviation; UCA: Upper cervical angle; LCA: lower cervical angle; McG: McGregor; T1S – CL: T1 Slope minus cervical lordosis.
Comparison of radiographic parameters based on patient age group.
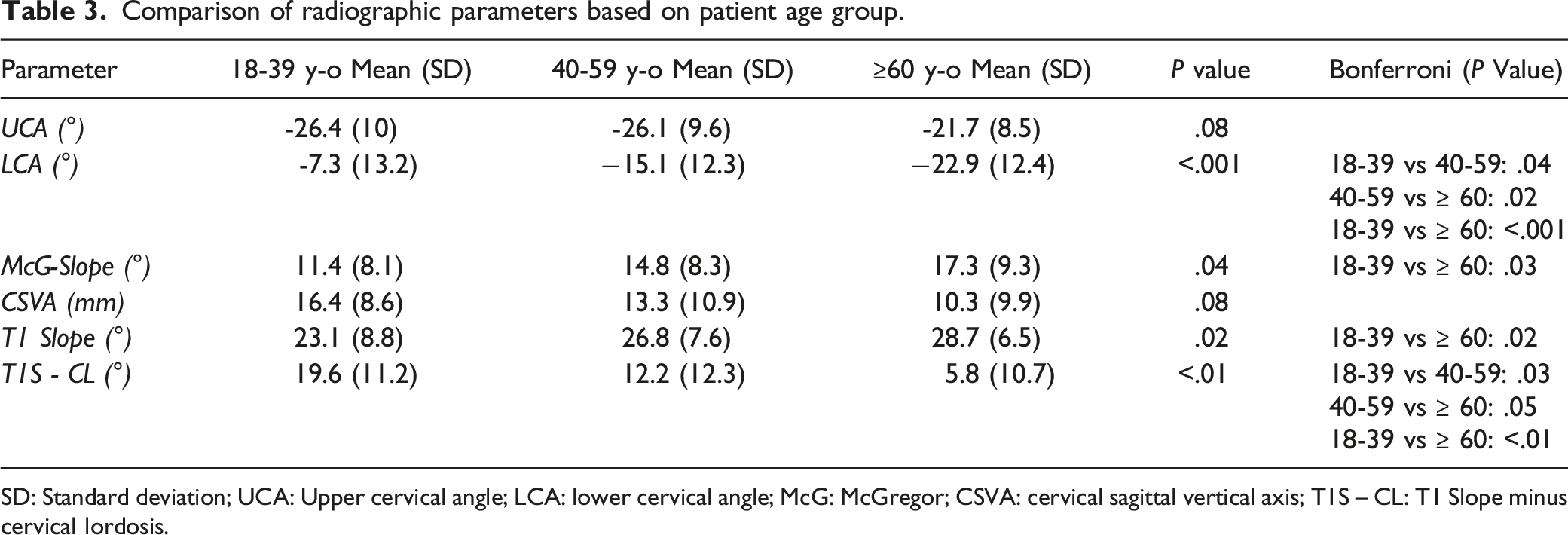
SD: Standard deviation; UCA: Upper cervical angle; LCA: lower cervical angle; McG: McGregor; CSVA: cervical sagittal vertical axis; T1S – CL: T1 Slope minus cervical lordosis.
Correlation Between Radiographic Parameters
Coefficients of Correlation (Pearson product-moment correlation coefficients, All With P value <.01).
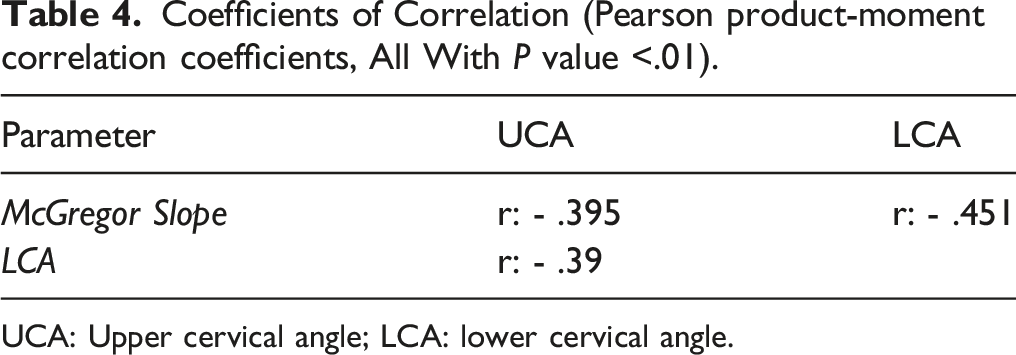
UCA: Upper cervical angle; LCA: lower cervical angle.
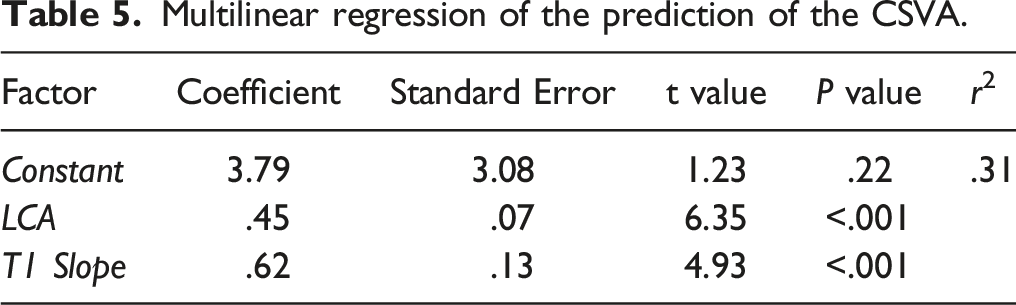
Multilinear regression of the prediction of the CSVA.
Discussion
Interest in spinal sagittal alignment has been growing over the past several years, and multiple studies have presented significant correlations between radiographic measures of sagittal alignment and overall patient quality of life.23-25 Initial studies focused on the thoracolumbar and spino-pelvic segments, but more recently, cervical sagittal alignment parameters have been increasingly studied, and thresholds of cervical malalignment at which there is adverse impact on health-related quality of life have been suggested.2-4,12,26,27
The importance of determining normative values for radiographic spinal alignment has been demonstrated for thoracolumbar spinal deformity through both the ability to better define what constitutes thoracolumbar deformity and also to aid in surgical planning for realignment goals. In contrast, there are fewer numbers of studies in the literature reporting normative sagittal values for the cervical spine9,28 in order to similarly define the thresholds of cervical deformity and guide realignment objectives. In addition, for thoracolumbar and spino-pelvic alignment, several variables, such as age, sex and BMI, can affect normative radiographic alignment.16,17,19 Furthermore, there are some publications reporting lack of uniformity in normative radiographic sagittal alignment across different populations,18,19 suggesting the need to investigate and understand these normative values across geographic regions and ethnicities.
The radiographic parameters considered in this study were selected based on the most relevant literature, including the Ames-ISSG cervical deformity classification, 11 studies showing the correlation between CL and T1S,3,9,11,29 a study showing correlation between McGregor’s slope and the chin-brow vertical angle (CBVA), 4 and also publications that assessed asymptomatic populations.9,28 Similar to available normative values for thoracolumbar and spino-pelvic alignment parameters, there is considerable variability in the normative values of cervical sagittal parameters in the current literature.
In the series published by Le Huec et al, 9 the mean lordosis between C2-C7 was 4.9°, while in our series it was 15.7°. However, the mean age of their subjects was 38 years (half of the sample was under 30 years old), while in the present study the mean age was 51 years, which is consistent with the finding in both studies that the magnitude of CL was positively correlated with age. In a systematic review, Kuntz et al 30 reported a mean of 17° of C2-C7 lordosis, among a population with a mean age of 42 years. Interestingly, although the individuals in the series from Le Huec were younger than the present series, 34% of their asymptomatic subjects had kyphotic alignment between C2-C7, 9 while in the present sample, only 10% had C2-C7 kyphosis. Park et al 28 analyzed cervical sagittal alignment in asymptomatic Korean adults based on 2 age groups: younger (20-29 years) and older (>60 years). The mean C2-C7 lordosis in the older group was 14° and in the younger group was 9°, representing a significantly greater lordosis with aging (P = .03). 28 The present study identified a mean UCA, measured as the angle between the McGregor line and the inferior endplate of C2, of −25°, while Le Huec et al 9 and Kuntz et al 30 found mean UCA values of −16° and −14°, respectively.
In their series, Le Huec et al 9 investigated the C7-slope as a foundation of overall cervical alignment and found a mean of 20°, while in the present study we focused on the T1S for which the mean was 26°. Several studies have suggested that the amount of the C2-C7 lordosis, or even kyphosis, is related to the T1S, in a relationship similar to that observed between the pelvic incidence and lumbar lordosis. 11 Increasing the sagittal inclination of the base of the cervical spine (i.e., the T1 superior endplate) must in turn be compensated by increasing cervical lordosis in order to help maintain overall cervical sagittal vertical alignment and an upright head. Le Huec et al 9 did not measure the C2-C7 SVA, but their spino-cranial angle (defined between the C7-slope and a line joining the middle of the C7 endplate and the middle of the sella turcica) was intended to reflect the cervical sagittal alignment and there was significant correlation of this parameter with both the C7-slope and C2-C7 lordosis. Similarly, in the present study, a multivariate regression found significant correlation of CSVA with T1S and C2-C7 lordosis, allowing prediction of the CSVA with the following the equation: CSVA = 3.79 - .45xCL +.62xT1S.
It was observed in the present study that there was a greater mean sagittal inclination of T1 (T1S) in older subjects, and this was accompanied by a greater degree of C2-C7 lordosis (LCA). However, the increase in CL overcame the T1S and resulted in a significant decrease in the mean of the mismatch between T1S and CL (TS-CL) with aging. In the Park et al 28 series, they also observed an increase in the amount of lordosis in older individuals that was associated with a decrease in the T1S. However, they did not consider the T1S-CL mismatch parameter in their study. 28 In the present study, CSVA was not significantly different across the age groups, suggesting the efficacy of the ability to adjust cervical sagittal alignment through an increase of the lower cervical lordosis. Park et al 28 found the same maintenance in the CSVA comparing younger and older subjects.
Cervical deformity can be a very disabling condition compared with other very impactful chronic diseases. 12 However, normal sagittal cervical alignment has been shown to be very heterogenous. 31 An adult cervical deformity classification was recently published that includes a qualitative description of cervical deformity and 5 modifiers, 3 of which reflect sagittal cervical radiographic parameters: CBVA, T1S-CL, and CSVA, and cutoffs for these parameters allow classification of subjects into grades 0, 1, or 2. 11 Bakouny et al 31 indicated that the cervical anomalies described in the Ames-ISSG classification have some overlap with observed variations in cervical alignment in asymptomatic subjects, such that abnormal modifier grades of CBVA and TS-CL can occur in some asymptomatic subjects.
In the present sample, all subjects had a CSVA measurement <4 cm, which corresponds to grade 0 in the Ames-ISSG classification, similar to that observed by Bakouny et al, 31 in which 99.3% of individuals also had grade 0. Considering the T1S-CL mismatch, in the present series 21% of the subjects had >20° (grade 2 of the classification), 18% had 15°-20° (grade 1) and 61% had <15° (grade 0), while in the Bakouny et al 31 sample, the majority (70%) of the subjects were classified as grade 2, 19% as grade 1, and 11% as grade 0.
The CBVA, an assessment of horizontal gaze, is a clinically assessed parameter or may be measured based on radiographs that include the skull.4,11 Lafage et al 4 have shown a strong correlation of the McGregor slope, a more reliable radiographic measurement, with the CBVA as an alternative means to assess horizontal gaze and proposed an equation to predict the CBVA from the McG-Slope: McG-Slope = −1.495 + .896 × CBVA. 4 In the present study, the mean of the McG-Slope was 14.8° that, applying the formula above, corresponds to a CBVA of 18°, a value surprisingly high (grade 1 in the Ames-ISSG classification). In the Lafage et al 4 series, the mean of the McG-Slope was −.9°, despite their assessment being based on a group of symptomatic patients, and their results suggested that patients with low disability should have CBVA in a range of −5° to 18°. Kuntz et al 30 presented a mean CBVA of −1°, and in a different series, Bao et al 32 analyzed 64 asymptomatic subjects and found a mean McG-Slope of 6.7°, which corresponds to a CBVA of 7.3°.
The main limitation of the present study is its cross-sectional design, which does not allow assessment of individual changes across the aging process. Another important limitation to consider is the relatively small sample size that may not be reflective of the broader Brazilian population, although it may serve as a basis for future larger population-based studies and provides at least initial normative reference values. The comparisons with other publications showing the heterogeneity of cervical sagittal alignment parameters among different series and ethnicities 33 are interesting, but readers should consider that the methodology, especially concerning image acquisition and measurement techniques, could differ across studies. 34 More definitive assessments of differences in normative cervical alignment parameters across ethnic groups would benefit from a single study that employs standardized image acquisition and measurement methodologies.
Conclusion
This analysis of cervical alignment in a Brazilian sample of asymptomatic volunteers revealed that with increasing age there is an observed increase in the sagittal inclination of the base of the cervical spine (T1S) that is accompanied by an increase in cervical lordosis as a means of maintaining cervical sagittal alignment (CSVA). Comparisons of the normative values identified in the present study with those reported in previous studies demonstrate variability in what constitutes normal and suggests that further study is warranted using standardized methodologies across diverse populations.
Footnotes
Declaration of Conflicting Interest
The author Justin S Smith declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Smith has received grants as Speaking/teaching arrangements from Zimmer Biomet, NuVasive and K2M; as Consulting from Zimmer Biomet, Nuvasive, and K2M; Research Study group founding from DePuy Synthes; and fellowship funding from NREF and AOSpine.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Note
This work was performed at Hospital do Servidor Público Estadual de São Paulo and at Ribeirão Preto Medical School of University of São Paulo, Brazil.
Ethical Approval
Institutional review board approval from the responsible service: Plataforma Brasil/Instituto de Assistência Médica ao Servidor Público Estadual - IAMSPE (opinion number 951.141).