
Abstract
Study Design
Retrospective multicenter cohort study
Objectives
We aimed to clarify the efficacy of multimodal intraoperative neuromonitoring (IONM), especially in transcranial electrical stimulation of motor-evoked potentials (TES-MEPs) with spinal cord-evoked potentials after transcranial stimulation of the brain (D-wave) in the detection of reversible spinal cord injury in high-risk spinal surgery.
Methods
We reviewed 1310 patients who underwent TES-MEPs during spinal surgery at 14 spine centers. We compared the monitoring results of TES-MEPs with D-wave vs TES-MEPs without D-wave in high-risk spinal surgery.
Results
There were 40 cases that used TES-MEPs with D-wave and 1270 cases that used TES-MEPs without D-wave. Before patients were matched, there were significant differences between groups in terms of sex and spinal disease category. Although there was no significant difference in the rescue rate between TES-MEPs with D-wave (2.0%) and TES-MEPs (2.5%), the false-positivity rate was significantly lower (0%) in the TES-MEPs-with-D-wave group. Using a one-to-one propensity score-matched analysis, 40 pairs of patients from the two groups were selected. Baseline characteristics did not significantly differ between the matched groups. In the score-matched analysis, one case (2.5%) in both groups was a case of rescue (P = 1), five (12.5%) cases in the TES-MEPs group were false positives, and there were no false positives in the TES-MEPs-with-D-wave group (P = .02).
Conclusions
TES-MEPs with D-wave in high-risk spine surgeries did not affect rescue case rates. However, it helped reduce the false-positivity rate.
Introduction
Although the rate of neurological complications is overall 1.0% in spinal surgery, 1 perioperative neurological complications are more frequent, ranging from 13% to 31% in high-risk surgeries, such as those involving spinal deformity, spinal-cord tumors, or ossification of the posterior longitudinal ligament (OPLL).2-7 Therefore, neurological complications should be avoided as much as possible, especially in high-risk surgeries. Currently, intraoperative neuromonitoring (IONM) can detect these neurological changes promptly, and the primary aim of IONM is to identify neurological complications before they become permanent.
IONM has many modalities, such as transcranial electrical stimulation of motor-evoked potential (TES-MEPs),8,9 somatosensory-evoked potentials,
10
spinal cord-evoked potentials after transcranial stimulation of the brain (epidural MEP, D-wave),11,12 spinal cord-evoked potentials after spinal cord stimulation,
13
and spontaneous electromyography.
14
Of these, TES-MEPs and D-wave are important for monitoring the motor tracts during spinal and spinal-cord surgery. To evaluate TES-MEPs, compound muscle action potentials (CMAPs) are measured using needle or disc electrodes placed on the muscles of the upper and lower limbs. D-wave is recorded directly from the epidural space
We hypothesized that the combined use of these modalities would provide high prevention ability against neurological complications and prevent permanent sequelae, as well as highlight the high validity of this diagnostic tool. Therefore, the purpose of this study was to clarify the efficacy of this modality combination use in high-risk spine surgeries with regard to: (1) the rate of prevention (termed “rescue” in this study) and (2) validity outcomes, such as true-positive, false-positive, true-negative, and false-negative cases.
Materials and Methods
Patients
This study was a retrospective multicenter cohort study of the Spinal Cord Monitoring Working Group of the Japanese Society for Spine Surgery and Related Research (JSSR). A total of 3625 patients who underwent TES-MEP monitoring during spinal surgery at 14 spine centers between April 2017 and March 2020 were included. The exclusion criterion for TES-MEP monitoring was a history of epilepsy.
Based on a previous study, 7 we defined high-risk surgeries for spinal deformity, cervical OPLL, thoracic OPLL, extramedullary spinal cord tumor (EMSCT), and intramedullary spinal cord tumor (IMSCT). We compared two groups in this study: one was a solo TES-MEP group, and the other was a combined TES-MEP with D-wave group, both using IONM. We further excluded patients who underwent surgery at the cauda equina level because D-wave cannot be applied at that level.
All surgeries were performed by JSSR-board-certified spinal surgeon instructors. The study protocol was approved by the Institutional Review Board of our hospital (research approval no. 3026), and all patients provided written informed consent before enrollment.
TES-MEP Monitoring
Corkscrew-type stimulating electrodes or silver-silver chloride electrodes were bilaterally and symmetrically placed 5 cm lateral and 2 cm anterior to Cz (international 10-20 system of electrode placement). Constant-voltage or constant-current stimulators were used in this study. For constant-current stimulators, the transcranial stimulus parameters were the following: 5-10 train stimuli, a stimulus interval of 2 ms, stimulus intensity 100-200 mA, stimulus duration .5 ms, filter 2-3 kHz, and recording time 100-200 ms. In contrast, the transcranial stimulus parameters for constant-voltage stimulators were the following: 5 train stimuli, a stimulus interval of 2 ms, stimulus intensity 300-600 V, stimulus duration .05 ms, filter 2-3 kHz, and recording time 100-200 ms.
CMAPs were recorded from the deltoid, biceps, triceps, abductor pollicis brevis, quadriceps femoris, hamstrings, tibialis anterior, gastrocnemius, and abductor halluces muscle groups via needle or disc electrodes. The amplitudes of CMAP were measured as baseline-to-first negative peak voltages, with amplitudes before invasive procedures regarded as baseline values.
In this study, we set an acute decrement in the amplitude of the CMAP response of ≥70% from baseline as the alarm threshold, based on a previous study. 19 For stimulus safety standards, the guidelines reported by McDonald et al. were followed. 20
D-Wave Monitoring
A bipolar catheter electrode was placed into the epidural space caudal to the surgical lesion for the recording electrode. A single TES stimulus was applied to elicit a D-wave. TES with a single pulse duration (.5 ms) and a stimulus of 50-200 mA, through the same transcranial stimulation sites as TES-MEPs, were used in this study.
We set an acute decrement in the amplitude of the D wave response of ≥50% from baseline as the alarm threshold. 11
Anesthesia
All patients underwent surgery under total intravenous anesthesia (TIVA) using propofol (3-4 mg/mL), fentanyl (2 mg/kg), and vecuronium (.12-.16 mg/kg) for induction, and propofol (100-150 mg/kg/min with target-controlled infusion), remifentanil (1 mg/kg/h), and vecuronium (0-.04 mg/kg/h) for maintenance of anesthesia. Systolic blood pressure was carefully controlled at >90 mmHg to maintain adequate perfusion, as low blood pressure may reduce TES-MEPs.
Clinical Assessment
We chose sex, age, body mass index (BMI), surgery time, blood loss, motor deficit before surgery, and category of high-risk spinal disease as clinical assessment factors in this study. Motor deficits were based on manual muscle testing (MMT) grade and the results of neurologic examinations documented in the database. Preoperative muscle weakness of MMT <4 was defined as a motor deficit.
Monitoring Outcomes
TES-MEPs group
Surgery was invariably and immediately stopped when CMAPs dropped by >70%. A true positive case was defined as a TES-MEP alert with a persistent decrease in the number of potentials at the end of the surgery, followed by observing a new neurological motor deficit after the surgery. A false-positive case was defined as an alert with a persistent decrease in the number of potentials at the end of the surgery and the absence of any new postoperative deficit. A true-negative case was defined as the absence of any TES-MEP alerts during surgery and no new postoperative deficits. A false-negative case was defined as the absence of an alert in a patient with a new postoperative motor deficit. A TES-MEP alert that normalized after some maneuvering in a patient who emerged without new motor deficits was defined as a rescue case.
TES-MEPs-With-D-Wave Group
Surgery was invariably and immediately stopped when CMAPs dropped by >70%, and the D-wave dropped by >50%. A true-positive case was defined as an alert of at least one of the two modalities with a persistent decrease in the number of potentials at the end of the surgery, followed by observing a new neurological motor deficit after the surgery. A false-positive case was defined as both alerts with a persistent decrease in the number of potentials at the end of the surgery and the absence of any new postoperative deficit. A true-negative case was defined as the absence of an alert of at least one of the two modalities with no new postoperative deficits. A false-negative case was defined as the absence of both alerts in a patient with a new postoperative motor deficit. A rescue case was defined as any kinds of alerts from TES-MEPs only or D-wave only or both that normalized after some maneuvering in a patient who emerged without new motor deficits.
Statistical Analysis
We compared data between the TES-MEPs group and TES-MEPs-with-D-wave group as analysis 1 (Figure 1). A one-to-one matching-model analysis using propensity scores was performed because of significant differences in the observed baseline and category of high-risk spinal disease between both groups (analysis 1). Age, sex, BMI, surgical time, blood loss, motor deficits before surgery, and category of high-risk spinal disease were included in the multivariable logistic regression model to calculate the propensity score for the use of D wave. C-statistic was calculated to evaluate the goodness of fit. We compared baseline data, monitoring results between matched TES-MEPs group and TES-MEPs-with-D-wave group as analysis 2. Study design.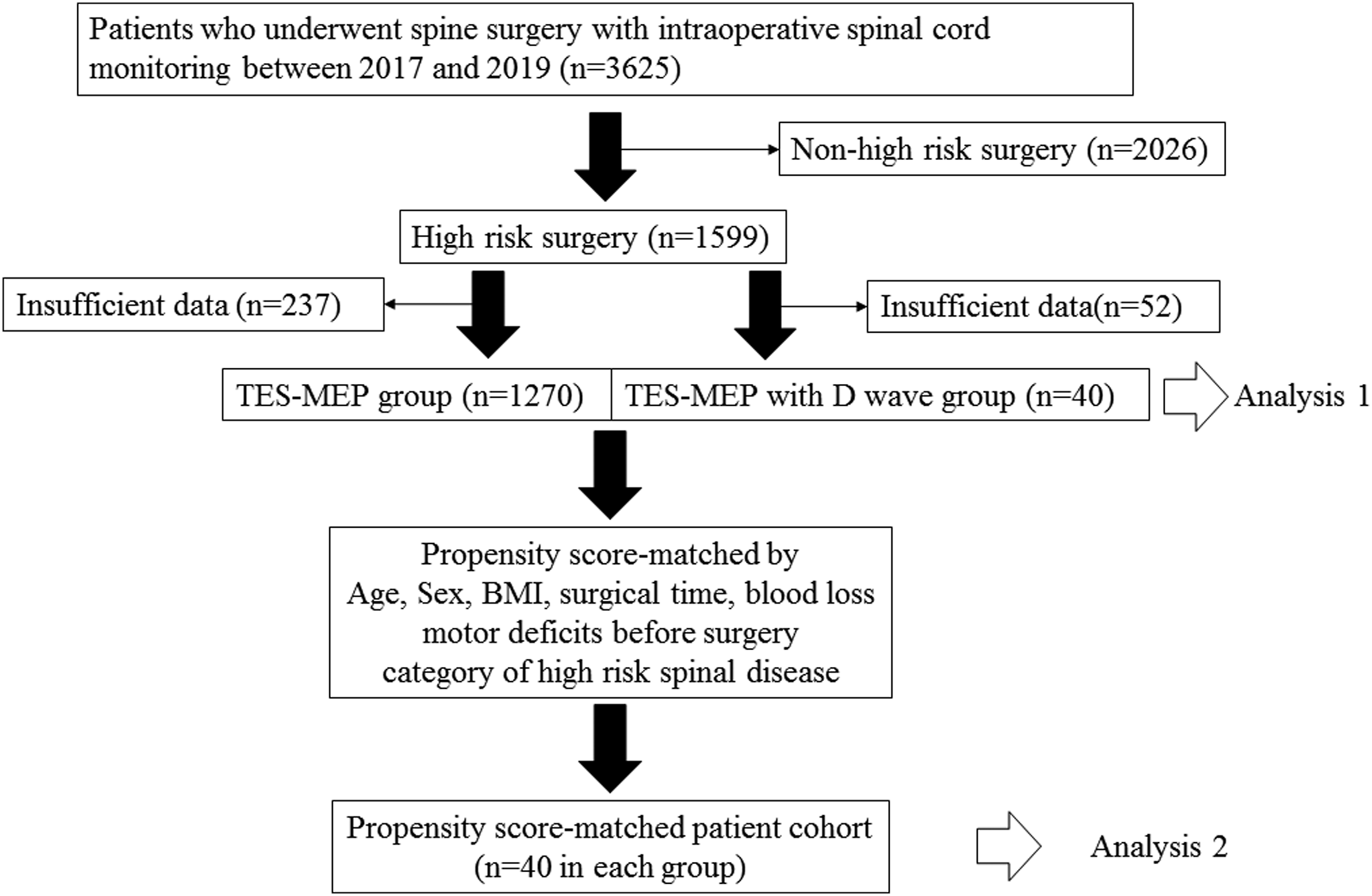
Unpaired continuous variables were compared using the Mann–Whitney U test, and categorical data was evaluated using the χ2 test or Fisher’s exact test.
Data was analyzed using SPSS Statistics ver. 26.0 (IBM Corp, Chicago, IL, USA) software, with P < .05 considered statistically significant.
Results
A total of 1599 (44%) patients underwent high-risk surgery for spinal deformity, cervical OPLL, thoracic OPLL, EMSCT, and IMSCT among the 3625 patients. Of these, 1507 underwent TES-MEPs, and 92 underwent TES-MEPs with D-wave. We excluded inadequate data, such as cauda equina level surgery or poor baseline waveform derivation, in the TES-MEPs group (n = 237) and TES-MEPs with D-wave group (n = 52) (Figure 1).
Analysis 1 (before Propensity-Score Matching)
Comparison of cases between TES-MEPs without D-wave and TES-MEPs with D-wave.
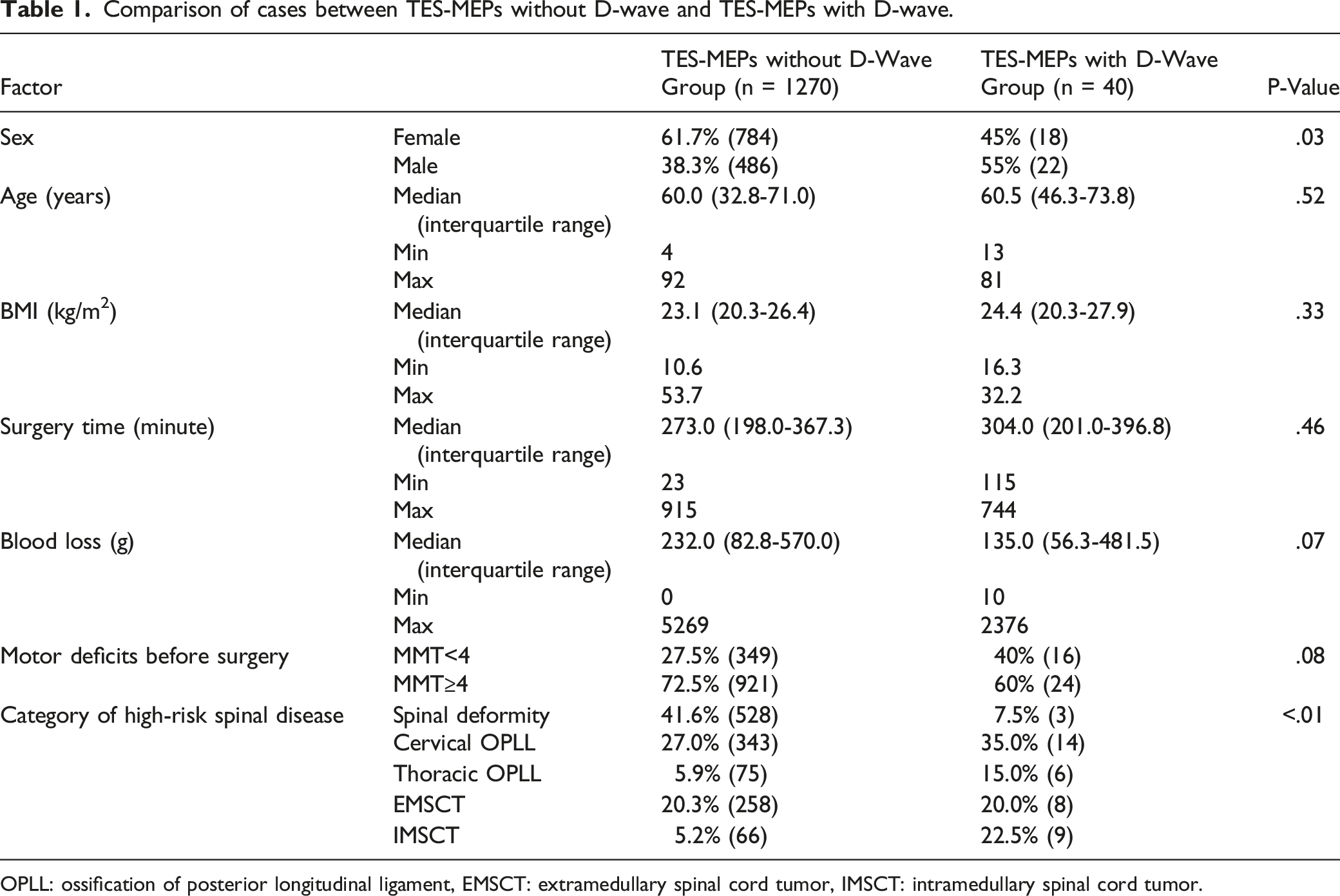
OPLL: ossification of posterior longitudinal ligament, EMSCT: extramedullary spinal cord tumor, IMSCT: intramedullary spinal cord tumor.
Comparison of cases between TES-MEPs without D-wave and TES-MEPs with D-wave group regarding monitoring outcomes.

Analysis 2 (after Propensity-Score Matching)
Comparison of cases between TES-MEPs without D-wave and TES-MEPs with D-wave after propensity matching.
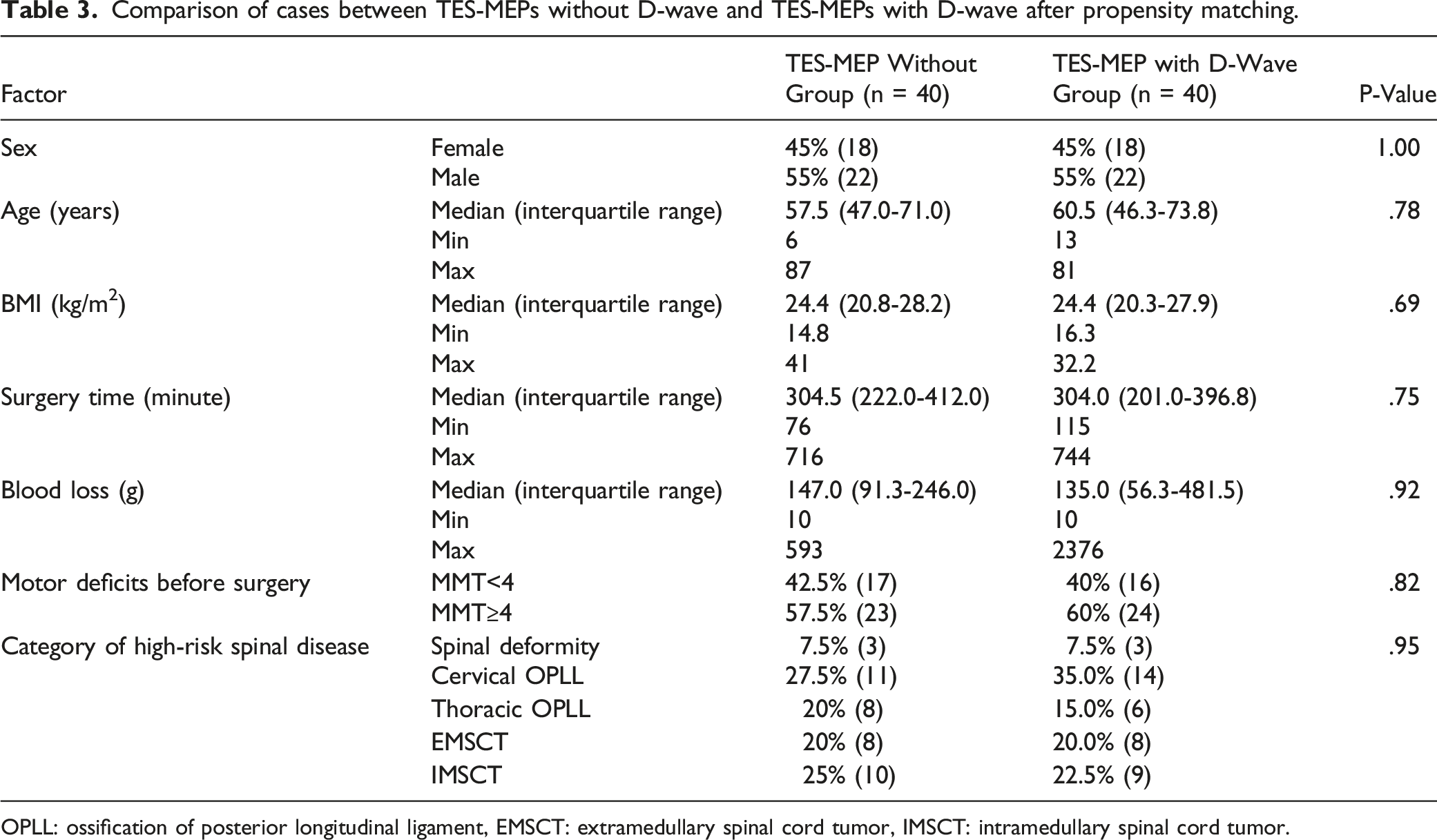
OPLL: ossification of posterior longitudinal ligament, EMSCT: extramedullary spinal cord tumor, IMSCT: intramedullary spinal cord tumor.
Comparison of cases between TES-MEPs without D-wave group and TES-MEPs with D-wave group regarding monitoring outcomes after propensity score matching.
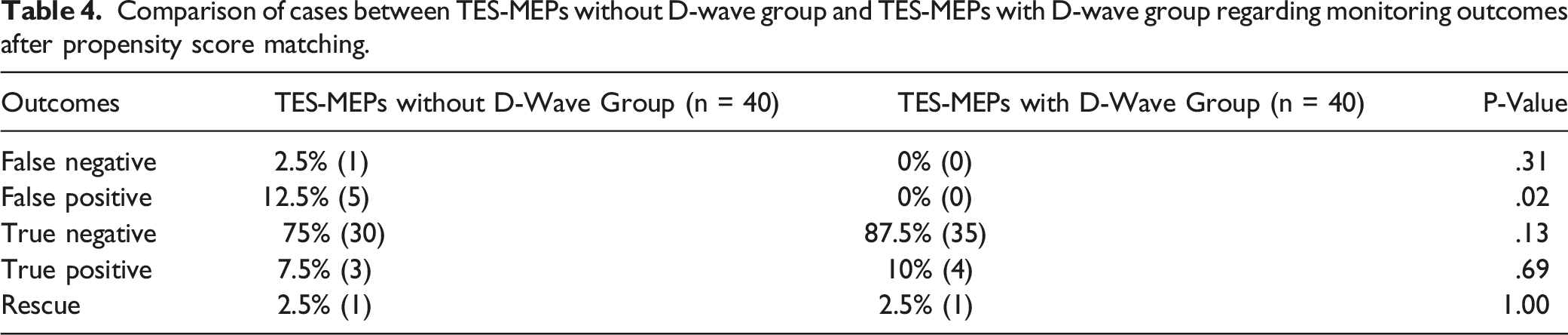
Based on our outcome monitoring, we calculated the sensitivity, specificity, positive predictive value, and negative predictive value in both groups. In the TES-MEPs-without-D-wave group, the sensitivity was 75%, specificity 85.7%, positive predictive value 37.5%, and negative predictive value 96.8%. Meanwhile, all parameters were 100% in the TES-MEPs-with-D-wave group.
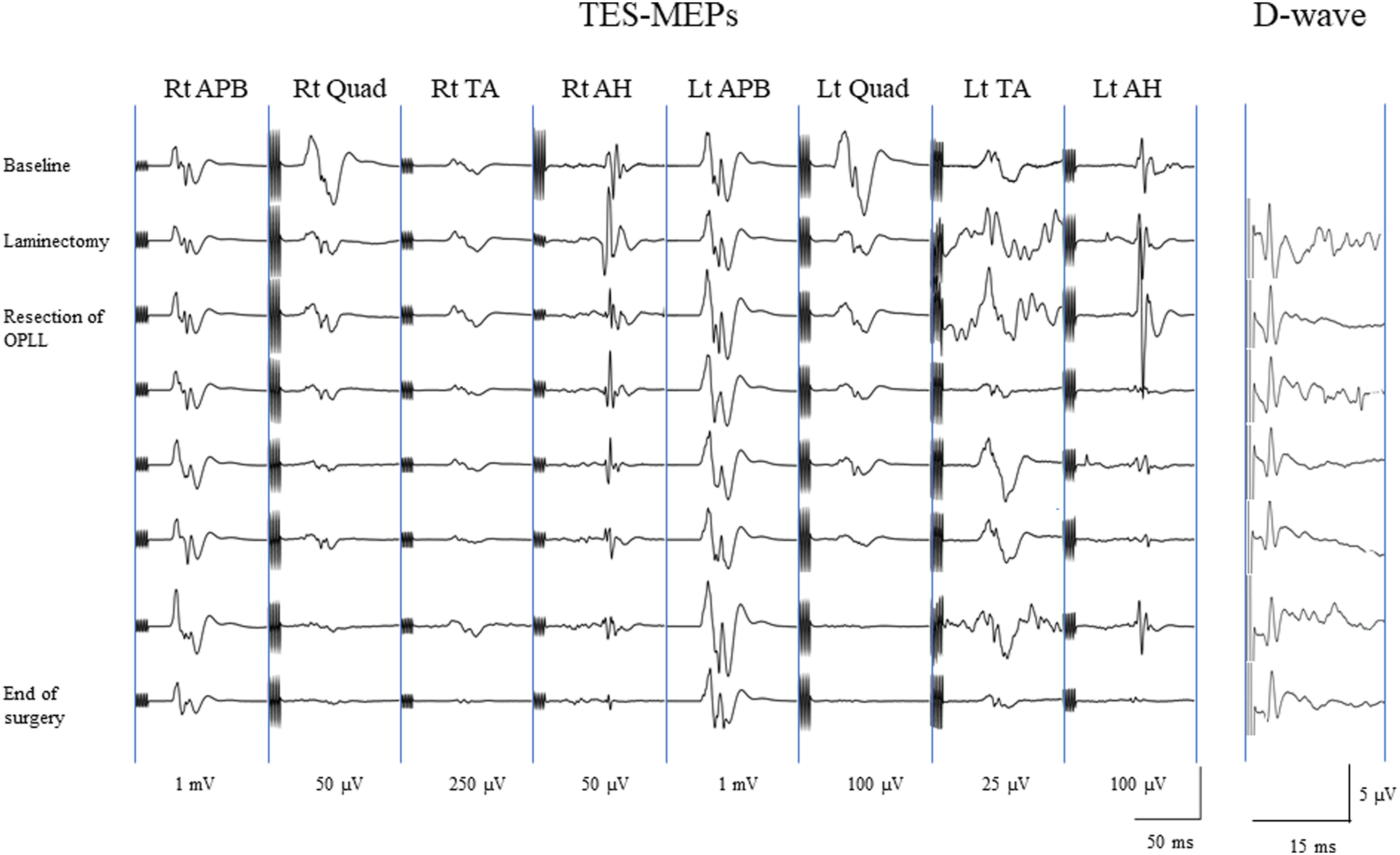
Illustrative Case (TES-MEPs With D-Wave, a True-Negative Case)
Case: A 51-year-old man with T1-2 thoracic OPLL was treated by posterior approach (Figure 2). He underwent laminectomy and resection of OPLL. During the OPLL resection, the patient’s TES-MEPs from bilateral lower limbs dropped by >70%, except right abductor halluces. Meanwhile, his D-wave remained unaltered and was maintained throughout the surgery (Figure 3). His motor function showed no deterioration after surgery. Although this may have been a false-positive case based on TES-MEPs, the final monitoring outcome confirmed it as a true negative because his D-wave did not change during the surgery. a: Sagittal computed tomography (CT) view shows OPLL at T1-2; b: Axial CT view of T1-2 thoracic vertebrae shows OPLL on the left side; c: Axial T2-weighted magnetic resonance imaging view of T1-2 thoracic vertebrae shows cord compression due to OPLL from left anterior lesion. Wave amplitudes of transcranial electrical stimulation motor-evoked potentials (TES-MEPs) and D-wave during surgery. AH: abductor halluces; APB: abductor pollicis brevis; Lt: left; OPLL: ossification of the posterior longitudinal ligament; Quad: quadriceps femoris; RT: right; TA: tibialis anterior.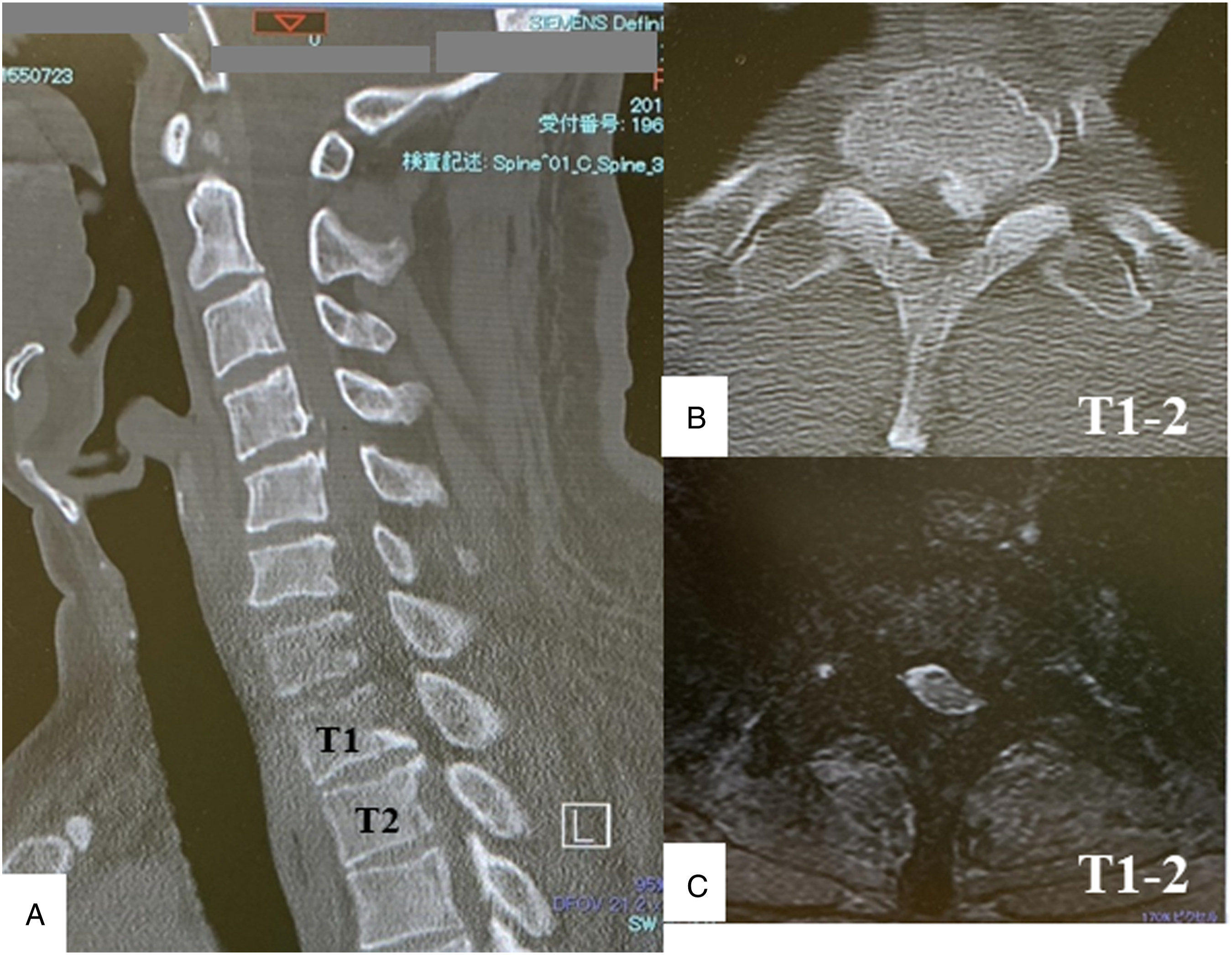
Discussion
Our results showed that the number of false-positive cases significantly decreased in the TES-MEPs-with-D-wave group before and after propensity-score matching. The TES-MEPs with D-wave reduced the number of false positives to zero (Table 2). However, the number of rescue cases did not change significantly between the two groups, regardless of propensity-score matching.
TES-MEPs and D-Wave as IONM
IONM is an essential tool to avoid intraoperative spinal cord injuries in high-risk spinal surgery. TES-MEPs are widely used for IONM and have become the standard because of their high sensitivity, the importance of intraoperative monitoring of motor function, and the effectiveness of TES-MEP monitoring to prevent postoperative neurological deficits. Although TES-MEPs have high sensitivity and specificity, the false-positive rate of this device is relatively high. 21 TES-MEPs may compel surgeons to take unreasonable risks or unnecessarily change the operative plan based on a potentially false-positive alert.
The D-wave amplitude is a direct measure of the number of functioning fast-conducting fibers within the corticospinal tracts. 22 Since no synapses are involved between the stimulating and recording sites (the proximal axon of the cortical motoneuron is stimulated and the recording site is located below the lesion site but above the synapses at the alpha-motoneuron), the D-wave is robust even under general anesthesia and is unaffected by muscle relaxants. 23 However, D-wave can only be applied at the spinal cord level. Therefore, we believe that combining TES-MEPs and D-wave is essential to complement each other’s shortcomings when monitoring motor function during spinal surgeries.
TES-MEPs With D-Wave
Ito et al. 24 reported that a combination of TES-MEPs and D-wave may be the best multimodality method for motor function monitoring in various spinal diseases, including non-high-risk surgeries, based on a high sensitivity of 90%. Sala et al. 11 also recommended that combining TES-MEPs and D-wave was the gold standard for intramedullary spinal cord tumor surgery. On the other hand, Ulkatan et al. 25 reported that epidural D-wave may be contraindicated for spinal deformity surgeries such as scoliosis because of false D-wave amplitude changes after spinal straightening, possibly due to altered spinal cord–recording electrode distance. Because spinal deformity surgery using TES-MEPs with D-wave was rare in our series (Table 1), it may not have affected our results. Further studies are needed to clarify the use of D-wave, especially in spinal deformity surgery, in the future.
Why did the Rescue Case Number Not Change and the False-Positive Rate Decrease When Combining TES-MEPs With D-Wave?
As mentioned above, although the number of false-positive cases decreased in the TES-MEPs with the D-wave group, the number of rescue cases did not change. Although the D-wave remains or drops insignificantly despite complete TES-MEP loss, the disappearance of TES-MEPs usually precedes changes in the D-wave. 17 Therefore, the reaction of TES-MEPs should be faster than that of the D-wave. Regarding rescue cases, we speculated that most alerts occurred in advance, based on TES-MEPs (>70% decrease in amplitude), and the surgeon performed the corresponding intervention immediately. We could preserve motor function before permanent spinal cord injury with this pattern. Meanwhile, regarding false-positive cases, we could evaluate motor function during surgery with two IONM methods in the case of TES-MEPs with D-wave. Even if TES-MEPs clearly decreased, if the D-wave was not decreased, the case was not recognized as a false positive. Therefore, we speculated that the total number of false positives was reduced by TES-MEPs with D-wave.
In this study, we clarified the utility of TES-MEPs with D-wave. Although this was not the focus of our study, spinal surgeons who participated in this study preferred the use of TES-MEPs in spinal deformity surgery among several high-risk spinal surgeries (Table 1). In addition, they did not prefer to use D-wave in spinal deformity surgeries (Table 1).
There are several limitations to this study. First, although we focused on high-risk spine surgeries, we included a variety of spinal disorders for which various surgical procedures were performed by different surgical teams using different methods. In addition, spinal cord compression and preoperative symptoms differed among high-risk surgeries; these clinical heterogeneities may have influenced the results. Second, although we decided on a common timing for TES-MEP or D-wave, it might have been difficult to completely unify the data because of the multicenter study design; this induced bias into the evaluation of alarms. Third, the number of TES-MEPs with D-wave was relatively small and might not be sufficient to draw proper conclusions. This small number of subjects might affect the monitoring of the results such as sensitivity, specificity, positive predictive value, and negative predictive value of 100% in the D-wave group. Fourth, there is no consensus on the definition of differentiation from multimodal IONM. For instance, a previous paper 26 used the following definition for a true positive: at least one alert with a persistent decrease in the number of potentials at the end of the surgery, followed by observing a new neurological motor deficit after the surgery. A false-positive case was defined as at least one alert with a persistent decrease in the number of potentials at the end of the surgery and the absence of any new postoperative deficit. A true-negative case was defined as the absence of an alert of all modalities in a patient with no new postoperative deficits. A false-negative case was defined as the absence of all alerts in a patient with a new postoperative motor deficit. However, we believe that the use of IONM should avoid false-positive as well as false-negative results. Therefore, as we mentioned before, we used our definition in this study.
Despite these limitations, a key feature of this study was that the D-wave could compensate TES-MEP false-positive drops to preserve motor function. That is, TES-MEPs with D-wave reduced the number of false-positive cases, although the false positives on TES-MEP were relatively high. The multicenter design was also a strength of this study. The results contribute to further understanding of the usefulness of TES-MEPs with D-wave monitoring for high-risk spinal surgery, which has a high chance of neurological complications and has rarely been studied prospectively.
Conclusion
TES-MEPs with D-wave did not affect rescue-case counts in high-risk spinal surgery. However, this combination reduced false-positive case rates compared with TES-MEPs without D-wave. Furthermore, the sensitivity and specificity of this combination showed an apparent increase compared with that of TES-MEPs without D-wave. Hence, we recommend the combined use of TES-MEPs and D-wave because it can reduce the number of false positives, which will minimize surgeon anxiety in high-risk spine surgeries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB Approval
Institutional ethical approval for this prospective study was obtained from Nara Medical University, Nara, Japan, and all patients provided informed consent prior to enrollment.