
Abstract
Study Design
Systematic review.
Objectives
Intraoperative neuromonitoring (IOMN) has become a standard practice in the detection and prevention of nerve damage and postoperative deficit. While multicenter studies have addressed this inquiry, there have been no systematic reviews to date. This systematic review identifies the leading causes of IONM alerts during adult spinal deformity (ASD) surgeries.
Methods
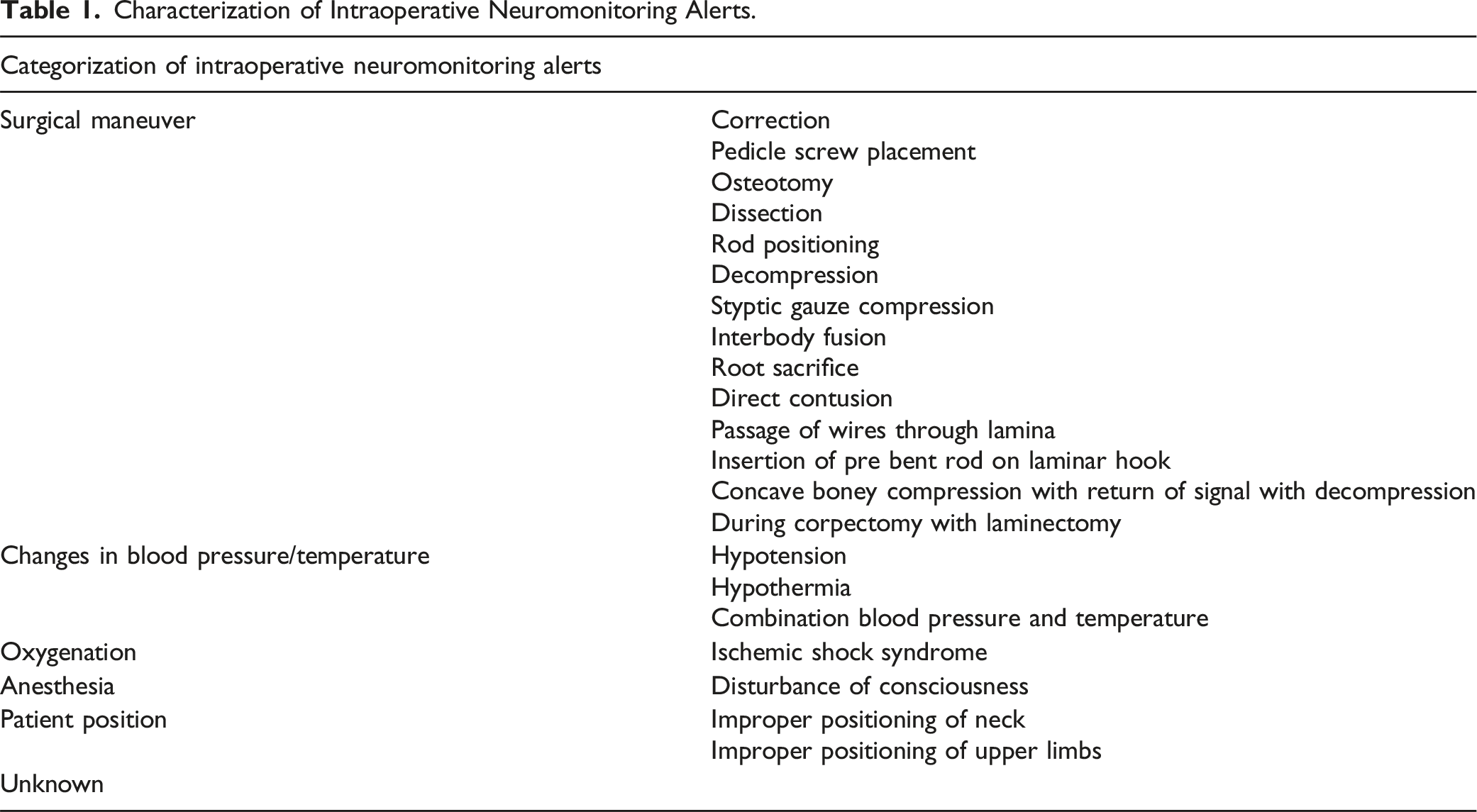
Following PRISMA guidelines, a literature search was performed in PubMed and Embase. IONM alert causes were grouped by equivalent terms used across different studies and binned into larger categories, including surgical maneuver, Changes in blood pressure/temperature, Oxygenation, Anesthesia, Patient position, and Unknown.
Results
Inclusion criteria were studies on adult patients receiving ASD correction surgery using IONM with documented alert causes. 1544 references were included in abstract review, 128 in full text review, and 16 studies qualified for data extraction. From those studies, there was a total of 3945 adult patients with 299 IONM alerts. Surgical maneuver led the alert causes (258 alerts/86.3%), with signal loss most commonly occurring at correction or osteotomy (101/33.8% and 95/31.8% respectively). Pedicle screw placement caused 35 alerts (11.7%). Changes in temperature and blood pressure were the third largest category (34/11.4%).
Conclusions
The most frequent causes of IONM alerts in ASD surgery were surgical maneuvers such as correction, osteotomy, and pedicle screw placement. This information provides spine surgeons with a quantitative perspective on the causes of IONM changes and show that most occur at predictable times during ASD surgery.
Introduction
Adult spinal deformity (ASD) is a common occurrence, with an estimated global prevalence ranging from 1% to 32%.1-3 This number may be significantly higher when looking exclusively at the elderly population. In a small cohort of asymptomatic individuals over 60 years of age, 68% (51/75) had radiographic evidence of scoliosis. 4 Operative management for these deformities is increasingly being favored over non-operative management due to multiple factors including advanced surgical techniques and decline in the rate of complications; from 2004 to 2011, the number of ASD surgeries more than doubled from 2137 to 5030 per year in the United States. 5 Significant spinal deformities are associated with increased morbidity and dissatisfaction in overall quality of life.6-11 This has ultimately led to the development of innovative surgical techniques to correct spinal deformities that have failed conservative management. 12
With the increasing prevalence of surgical intervention for ASD, it is important to understand the intraoperative complications associated with surgery. ASD surgeries are complex procedures due to the inherent heterogeneity present in deformity and the goal of achieving extensive correction. 13 When compared to other high risk procedures such as coronary artery bypass grafting, pancreatectomy and esophagectomy, ASD surgery was found to have a higher surgical invasiveness and morbidity score, and therefore be more risky. 14
One of the feared intraoperative complications is neurologic injury, resulting in a 296% increase in the use of intraoperative neuromonitoring (IONM) during spine surgery in the United States within the last decade. 15 Among IONM modalities, 3 main types prevail: somatosensory evoked potentials (SSEP), motor evoked potentials (MEP) and electromyography (EMG). SSEP tracks nerve conduction from extremity to central nervous system, providing monitoring of the sensory pathway. SSEP monitoring in continuous, but cannot distinguish between nerve roots, is somewhat susceptible to false positives and false negatives 16 Alarm thresholds are often set at a 50% loss of signal amplitude or a 10% increase in latency. MEP is monitored in the opposite direction, often from a transcranial electrode source and recorded at a peripheral extremity. This modality provides more immediate status of nerve pathways, but cannot be used continuously, and is susceptible to nerve blockade and inhaled anesthetics. Alert thresholds are often set around 50%–80% loss of amplitude or a loss of provoked response, barring other causes, for 10 minutes. EMG monitors muscle contractions from nerve root stimulation, and provides spontaneous and continuous feedback, but is susceptible to anesthesia, transient nerve root activity during surgery, 17 is more specifically suited for nerve root status, and has a high rate of false positives. 16 This study collected data on SSEP, MEP, and multimodal neuromonitoring. These various neuromonitoring modalities provide a convenient method to monitor a broader base of neural function, and can provide spontaneous warnings of neural deficit through signal loss. The use of IONM provides both high sensitivity and specificity for spinal cord injury during spinal surgery, allowing surgeons to identify intraoperative neural insult and intervene before damage is done.16,18
Despite the value of IONM and the increased surgical management of ASD, there is a paucity of literature examining the most common causes of intraoperative neuromonitoring changes. This systematic review seeks to describe and quantify the most common causes of IONM changes in ASD surgery, giving better insight into the relative risks of hazardous intraoperative events. Knowledge of when these occurrences will happen provides spine surgeons with the ability to prepare for them and work through established guidelines to ensure a successful surgery.
Methods
Screening and Data Collection
This systematic review was written in accordance with the Primary Reporting Items for Systematic Reviews and Meta-Analyses (PRIMSA) guidelines. 19 Our written protocol is registered on the PROSPERO website. The registration number is CRD42023395618.
The literature search was performed in 2 electronic databases, PubMed (1946-present) and Embase via Elsevier (1947-present). The searches were conducted in January 2023. Results were restricted to English language only and only full text articles. Results in Embase were limited to articles only. No restrictions were placed on the date of publication. Searches were not re-rerun prior to analyses. Due to the nature of this study, Institutional Review Board approval was not required and informed consent is not applicable.
Neuromonitoring keywords and subject headings were combined with spinal deformity terms. The full search strategies for PubMed and Embase can be found here (https://osf.io/563u8/?view_only=8b510d6c51f046e0965b7387ffd8833f). There were 951 results in PubMed and 1210 results in Embase, a total of 2161. References were deduplicated using a SR Accelerator tool called Deduplicator. There were 617 duplicates removed, which left 1544 unique references for review. These references were imported into Covidence for screening. All screening was performed utilizing Covidence software (version 2, Veritas Health Innovation). There were 2 stages of review, title/abstract and full text. References were independently screened using Covidence by 2 investigators, CC and DK. Any disagreements on paper eligibility, either in the title/abstract or full text screening phase, were resolved by a third independent reviewer, MS. A data extraction sheet was created in Covidence, outlining the variables to be collected. Data were extracted independently by investigators CC and DK. Any conflicts in data collection were reviewed by CC and rectified.
Our study population included adults with spine deformities that underwent corrective surgery utilizing neuromonitoring with documented events leading to neuromonitoring changes. An event was considered any patient physiological process or surgical maneuver that appeared causal to subsequent neuromonitoring change. Eligible spine deformity diagnosis included: idiopathic scoliosis, degenerative scoliosis, kyphosis, kyphoscoliosis, lordosis, sagittal deformities, coronal deformities, and nonspecific spine deformity. Eligible neuromonitoring modalities included somatosensory evoked potential (SSEP), motor-evoked potentials (MEP), transcranial motor evoked potential monitoring (Tc-MEP), cortical somatosensory evoked potentials (CSEP), descending neurogenic evoked potentials (DNEP), and multimodal intraoperative monitoring (MIOM). Papers were excluded if they exclusively included individuals under 18 years of age, had no diagnosis of spine deformity, spine deformity was due to acute trauma, infection, or tumor, intraoperative neuromonitoring was not used in surgery, or suspected causes of intraoperative neuromonitoring were not documented. Studies included were retrospective cohort studies, prospective cohort studies, and case series.
Characterization of Intraoperative Neuromonitoring Alerts.
Risk of Bias Assessment
The quality of each study included in the review was analyzed using the LEGEND evidence evaluation tool. This tool was selected because it offered multiple versions that align with a breadth of study designs that are all evaluated on the same scale. Studies that were deemed “not applicable or credible” were not included in the review. Studies were reviewed by CC.
Data Synthesis and Statistical Analyses
Suspected causes of intraoperative neuromonitoring causes were individually tabulated within each included paper. Data from each study was pooled, with each data point representing an adult patient who underwent corrective spine surgery for spine deformity who experienced a neuromonitoring event with a suspected cause. The nature of the data collected from each study did not require a statistical tool for synthesis. This data was considered raw data that was defined by the same diagnostic pool, procedure classification, neuromonitoring intervention group, and individualized event cause analyses.
Descriptive statistics were used for statistical analyses. A total number of recorded intraoperative neuromonitoring event causes were calculated. The total number of neuromonitoring event causes were then processed into percentages defined by the 6 broad classification categories: Surgical maneuver, changes in blood pressure/temperature, oxygenation, anesthesia, patient position, and unknown. Percentages for specific subclassification within each broad category were calculated.
Results
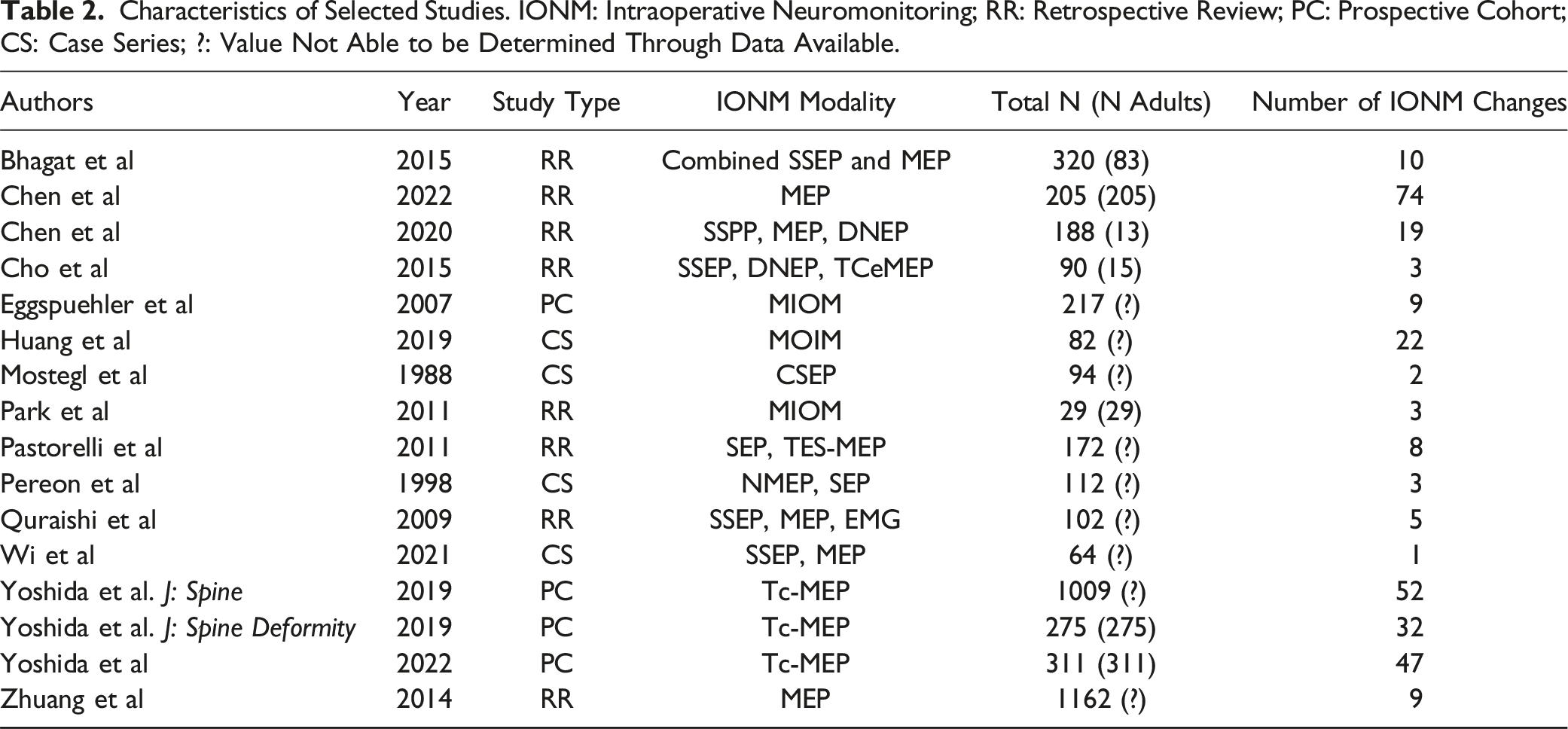
See Figure 1 for the literature selection flow chart. After independently screening 1544 articles, 16 were ultimately included. See Table 1 for characteristics of included articles. The 16 articles consisted of 8 retrospective reviews, 4 prospective cohort studies, and 4 case series that ranged in publication date from 1988 to 2022.17,20-34 PRISMA flow chart.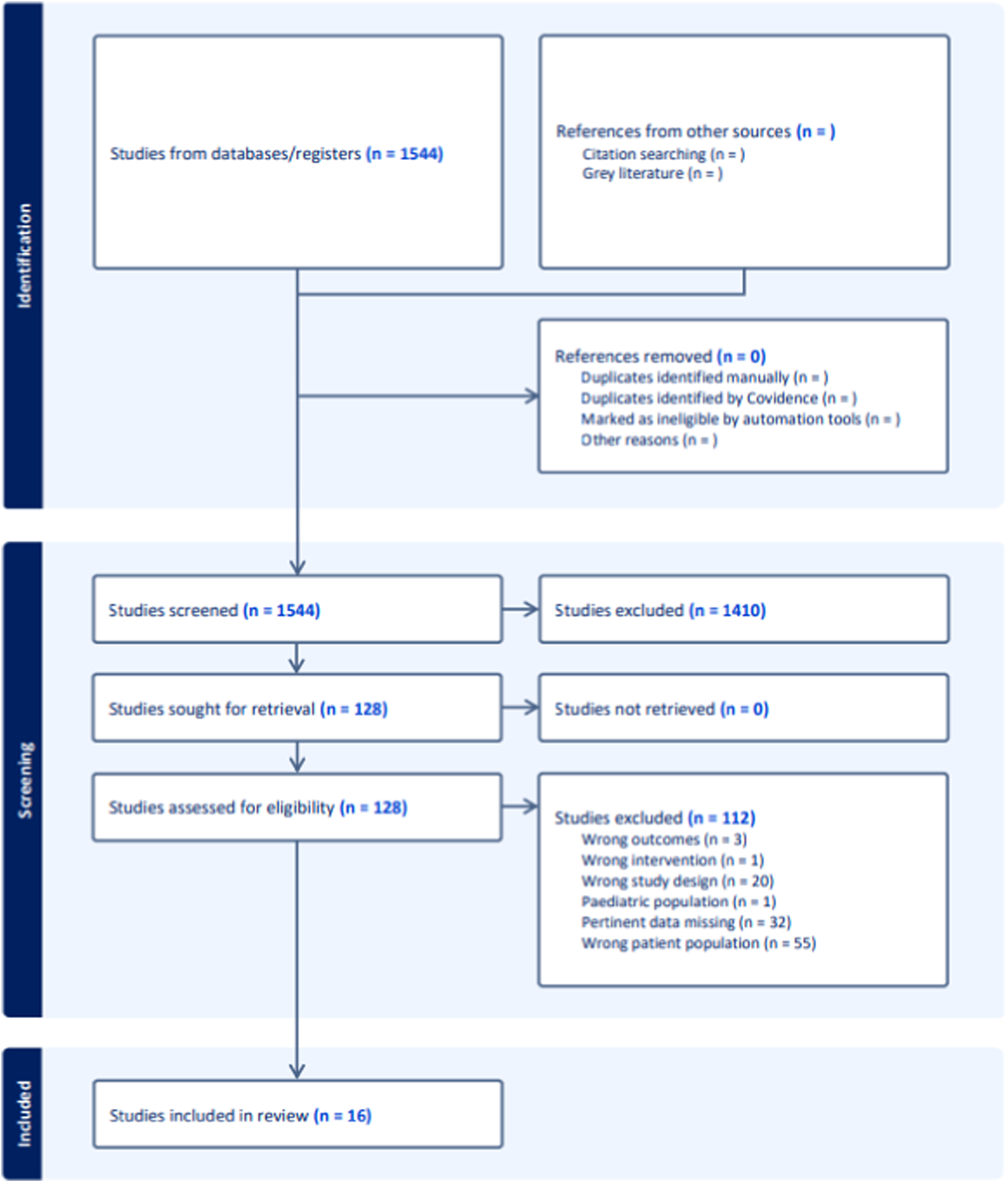
The total number of adult subjects was not able to be determined in some included articles that consisted of both pediatric and adults in their study population. In these cases, IONM events were reported in table format, including patient age, which allowed us to exclude any patient under 18 from data collection. However, when reporting cohort demographics, articles did not explicitly report the number of pediatric vs adult subjects with age characteristics. Average number of adult subjects included in each paper is 133, calculated only from those in which data was provided on the number of adults included. Average age of adult subjects could not be calculated due to numerous studies lumping pediatric and adult subjects in demographic analyses.
Characteristics of Selected Studies. IONM: Intraoperative Neuromonitoring; RR: Retrospective Review; PC: Prospective Cohort; CS: Case Series; ?: Value Not Able to be Determined Through Data Available.
Combined Tabulation for Causes of Intraoperative Neuromonitoring Events.
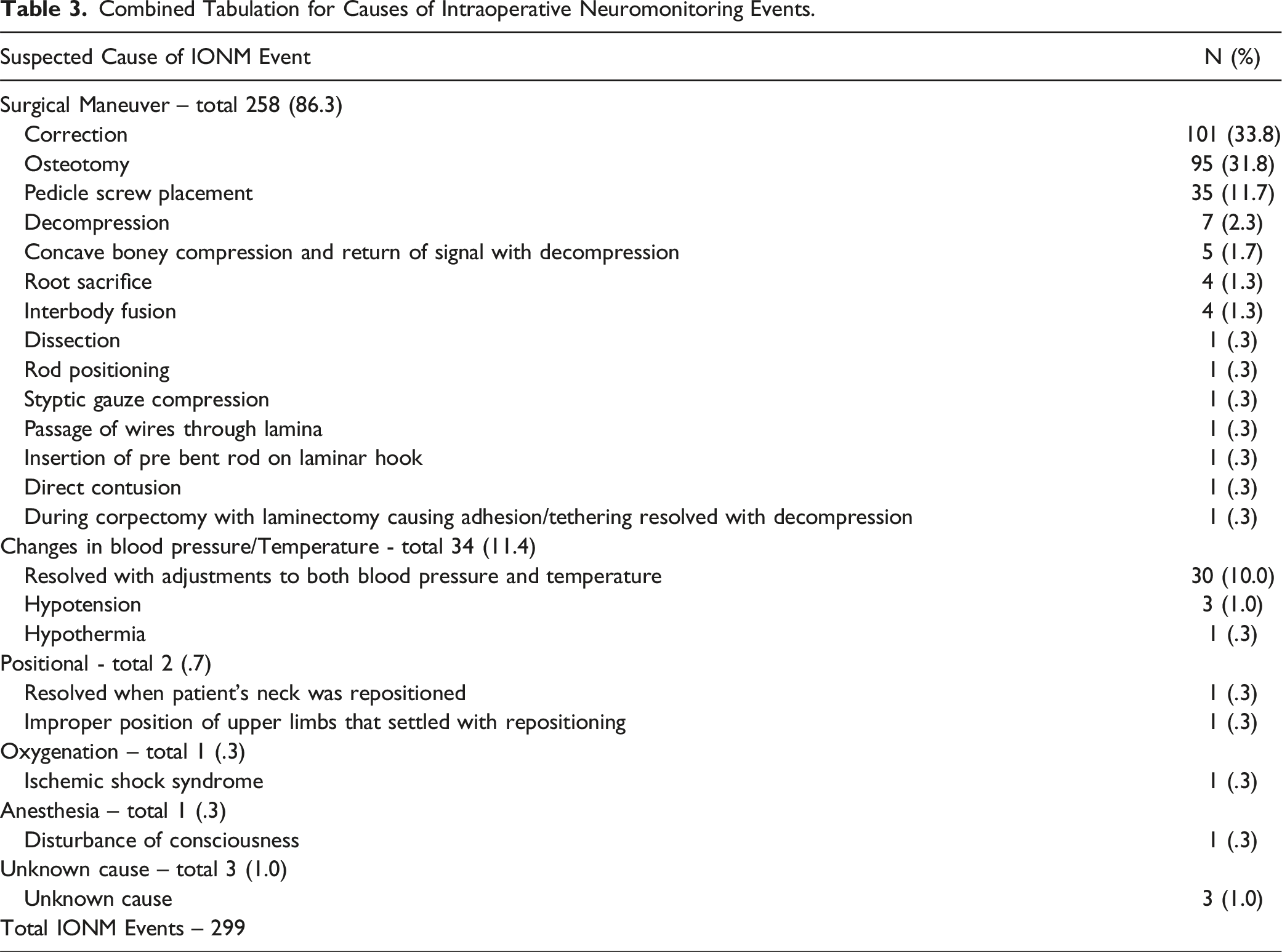
Within the changes in blood pressure/temperature group, 88.2% of such events were thought to be caused by both changes in blood pressure and temperature. Changes in blood pressure alone were thought to cause 8.8% of events and changes in body temperature alone to cause 2.9% of events (Table 3).
Changes in IONM due to patient positioning only occurred in 2 subjects, one of which resolved after repositioning the patient’s neck and the other with repositioning of the patient’s limbs. There were 3 reported unknown causes. The oxygenation group yielded one instance of ischemic shock as cause for an IONM change. The anesthesia group also yielded one subject, who was reported to have a change in consciousness as their suspected cause for a IONM change (Table 3).
LEGEND Bias Analyses
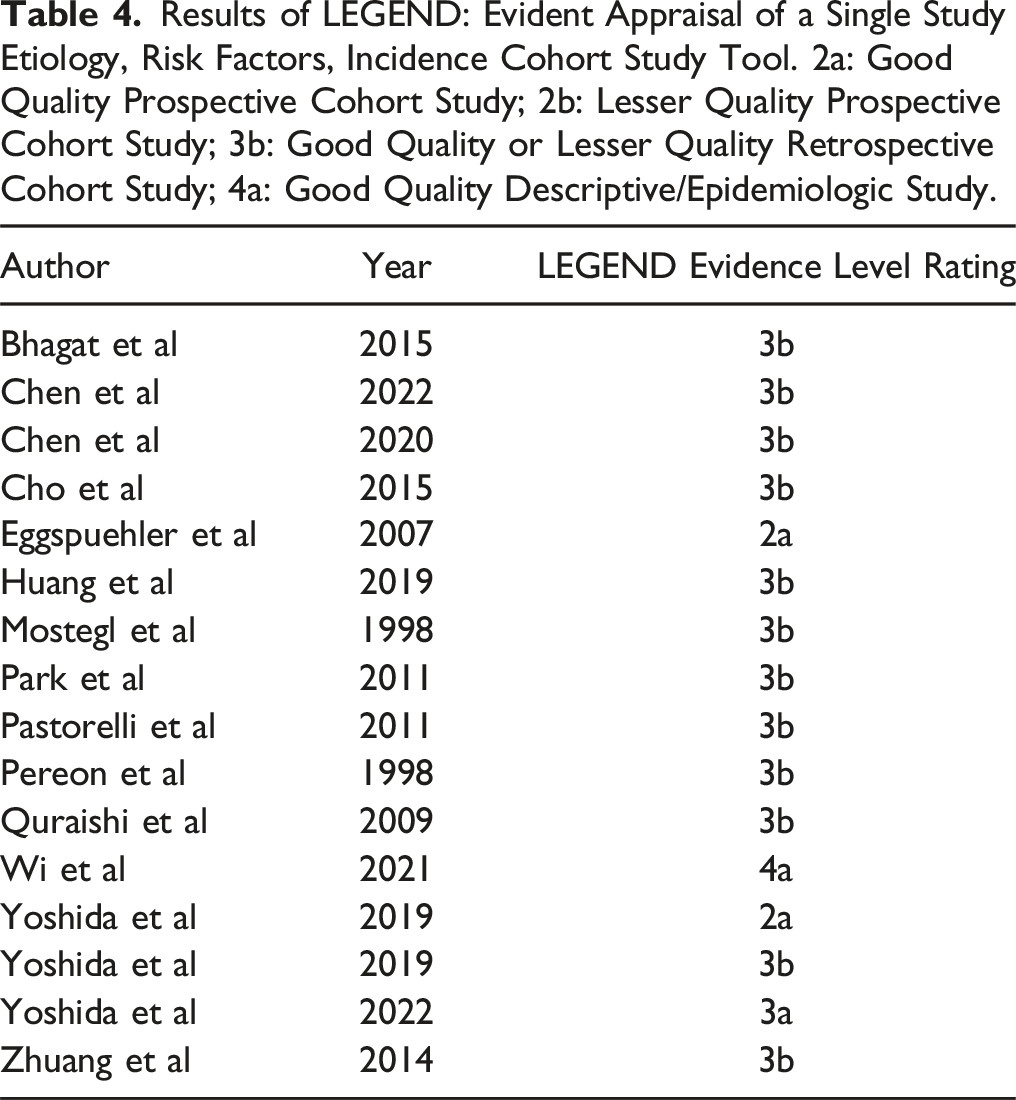
See Table 3 for LEGEND evidence level ratings for each article. No articles were deemed not valid, reliable, or applicable.
Discussion
Results of LEGEND: Evident Appraisal of a Single Study Etiology, Risk Factors, Incidence Cohort Study Tool. 2a: Good Quality Prospective Cohort Study; 2b: Lesser Quality Prospective Cohort Study; 3b: Good Quality or Lesser Quality Retrospective Cohort Study; 4a: Good Quality Descriptive/Epidemiologic Study.
The most prevalent causes of IONM alerts were related to surgical maneuvers. Of these maneuvers, correction made up 33.8% (101) of all alerts. Spinal correction involves adjustments in vertebral alignment, rotation, and translation, which can introduce tension on the spinal cord and nerve roots. Altered tension of neuronal tissue contributes to changes in signal conductivity and propagation, leading to IONM changes. 35 Lewis et al. found that the degree of angular correction is an independent predictor of developing IONM alerts. 36 Additionally, angular deformity correction can lead to IONM changes though impingement of bony structure into the spinal cord or vascular injury from stretching of the anterior spinal artery. 37 Detecting these IONM changes is critical, as previous studies have shown high rescue rates and avoidance of long-term neurological deficits if the correction is released in a timely fashion.32,36
Our systematic review found the next greatest cause of IONM alerts occurred during osteotomies, accounting for 95 out of 299 alerts (31.8%). Osteotomies introduce significant angular corrections to the spinal cord. In the more drastic pedicle subtraction osteotomy, corrective angles as high as 30˚-40° can be introduced through just one resection. 38 As previously discussed, these angular corrections can lead to IONM changes through various mechanisms of mechanical insult. Additionally, osteotomies require extensive exposure of the vertebral body, introducing further risk of IONM signal changes. For example, spoon retractors can compress nerve roots and contribute to signal changes. 39 Lastly, osteotomies such as pedicle subtraction osteotomies have estimated blood losses of up to 2 Liters. 40 The resultant transient ischemia from excessive blood loss can be another source of IONM alerts as neural conductivity is altered. IONM changes during osteotomies are common and likely occur due to a wide variety of mechanisms. As such, surgeons should pay close attention to IONM during osteotomies and prepare for possible changes.
Pedicle screw placement was another common cause of IONM alerts, accounting for 35 out of 299 alerts (11.7%). Pedicle screws are a valuable tool in spine surgery, allowing surgeons to safely apply greater corrective forces to the spine than previous hook-based constructs.41,42 However, placing pedicle screws in close proximity to neural tissue introduces risk of direct compression in the form of malpositioned screws. 43 As with the previously discussed causes of IONM alerts, timely detection of pedicle screw malpositioning is critical in order to reposition the screw and prevent long term neurological injury.
Fluctuations in temperature and blood pressure were also responsible for a significant amount of IONM alerts, causing 34 out of 299 alerts (11.4%). Many anesthetic agents of induction and maintenance have vasodilatory effects that result in significant fluctuations in blood pressure. 44 Additionally, patients who experience excessive blood loss during their procedure are more susceptible to hypotensive episodes. These fluctuations, especially hypotension, can have profound effects on neurological function resulting from spinal cord ischemia. 45 Detecting these neurological deficits through IONM is critical as they can often be easily reversed. Yang et al. performed a prospective analysis of four hundred fifty two spinal deformity patients who experienced an IONM change and found that 20% of all IONM changes may be reversed with a simple raise in mean arterial pressure (MAP) to 85mmHg. 46 As such, IONM may be a useful tool for preventing hypoperfusion of the spinal cord and long-term neurologic injury.
Our paper also highlights the lack of information regarding IONM changes. The exclusion of sources during full text review was, in fact, largely due to studies not providing details on IONM causes. There were more papers that mentioned changes, however, these often had both pediatric and adult populations. While these are valuable, descriptions are needed that isolate and describe pediatric or adult populations independently. This will provide more information to surgeons and ultimately allow for better individualized patient care.
Additionally, our study demonstrates that IONM alerts often occur during predictable aspects of ASD surgery, and there were few reported instances of IONM that were not attributable to one of the aforementioned major causes. Repositioning, ischemic shock, and unknown or other reasons only accounted for 7 out of 299 alerts (2.3%). As such, surgeons should understand most changes occur during correction, pedicle screw placement, osteotomy, or hypoperfusion so that the risk of IONM alerts can be accounted for in surgical planning.
This project had various limitations. While we identified potential causes for IONM changes, we did not collect data on how many of these alerts were reversed. This information would further enrich the surgeon’s perspective on the priority of certain hazardous events over others. Tracing documented postoperative neurological deficit to alert causes would similarly enrich our perspective on relative intraoperative hazards. Additionally, we were unable to definitively discriminate true vs false positive IONM alerts. Follow-up studies reviewing true vs false positive alerts in this population would be useful. Deficits undetected by IONM would also be valuable data to analyze (though the pool of studies with such broad and consistent data would be smaller). While PubMed and Embase are the 2 largest searchable databases, there may remain some relevant studies indexed elsewhere. Our review was also limited to literature published in English. Abstracts that did not make it to publication in either database in our searches might also have added data, or at least perspective to our study. The large studies with n sample values that were magnitudes greater, such as Yoshida (2019b) or Zhuang, had proportionally greater representation. Differences in the methods of these large studies would skew the results. There were also variations in how studies set alert criteria, such as inconsistencies in MEP thresholds amongst the included studies: Peron 60%, Pastorelli 65%, Yoshida 70%, and Zhuang 80%. If certain event causes tend to reduce amplitude less than others, they could be underrepresented in studies with lesser alert thresholds. As the data came from different surgery centers, differences in alert causes would be a likely consequence of certain centers practicing on patients of more or less morbidity, varying levels of fusion or angular correction, different levels of risk, or different instrumentation.
Conclusion
IONM is an important tool for monitoring neurologic function during ASD surgery and preventing long-term neurologic injury. The purpose of this systematic review was to evaluate and quantify the most common causes of IONM alerts during ASD surgery. Our data shows the majority of IONM alerts are related to surgical maneuvers. Correction, osteotomies, and pedicle screw placement were all significant sources of alerts. A minority of alerts were related to changes in body temperature or blood pressure. These aforementioned causes were responsible for nearly 98% of all alerts, with repositioning, ischemic shock, and unknown or other reasons accounting for the remainder. In conclusion, it is important that surgeons are aware of the described and predictable causes of IONM alerts, as they introduce significant risk of long-term neurologic injury if they are not reversed in a timely manner.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.