
Abstract
Objective
To investigate whether intraoperative neuromonitoring (IONM) has a significant advantage in reducing the incidence of recurrent laryngeal nerve (RLN) injury.
Methods
Patients who underwent thyroid and parathyroid surgery from October 2012 to December 2017 at the Center for Thyroid and Breast Surgery of Xuanwu Hospital were retrospectively analyzed. They were divided into the IONM group and visualization alone group (VA group) according to whether IONM was used.
Results
In total, 1696 nerves at risk of injury (IONM group, n = 1104; VA group, n = 592) were included in the analysis. Among the high-risk nerves, permanent damage occurred in no cases in the IONM group but in one case in the VA group. Because the higher proportion of central lymph node metastasis caused difficulties in central cervical lymph node dissection and identification of the RLN, the patients undergoing lateral cervical lymph node dissection in the VA group had a significantly higher risk of postoperative RLN injury (11.76% vs. 0.00%).
Conclusion
IONM technology has advantages in protection of the RLN, especially in high-risk nerves and patients with a high proportion of central lymph node metastasis who require central and lateral cervical lymph node dissection.
Keywords
Introduction
Recurrent laryngeal nerve (RLN) palsy is a major complication of thyroid and parathyroid surgery. RLN dysfunction can cause postoperative hoarseness and even difficulty breathing, potentially requiring patients to undergo tracheotomy to relieve the symptoms. This not only greatly reduces patients’ quality of life but is also a main cause of medical litigation. Although the development of surgical instruments and standardization of surgical procedures have helped surgeons to identify and protect the morphological integrity of the RLN, these measures alone can hardly ensure good neurological function. Therefore, intraoperative neuromonitoring (IONM) based on electromyographic (EMG) signals was developed.
According to recent research, the overall incidence of RLN paralysis ranges from 0.5% to 20.0%, with a transient incidence of 0.6% to 9.6% and a permanent incidence of 0.0% to 2.0%.1–9 Several factors place patients at high risk of RLN injury, including thyroid reoperation, thyroidectomy for thyroid malignancy, Graves’ disease, giant thyroid goiters (>300 g), and goiters with a retrosternal component. 10 Undoubtedly, IONM technology has a significant advantage in identifying the RLN during high-risk surgery. However, applying IONM technology to reduce RLN damage is controversial. Some studies have shown that the use of IONM can help to reduce the incidence of RLN injury and shorten the surgery time,1,9 especially in patients undergoing complicated thyroid surgery. Nevertheless, other studies have suggested that the use of IONM results in no significant difference in the incidence of RLN injury.2–4
Considering these controversial results, we analyzed and summarized the clinical data of 1033 patients with 1696 RLNs at risk of injury for 5 consecutive years in our institution to determine whether the use of IONM helps to reduce the rate of RLN injury.
Materials and methods
Patients
We retrospectively analyzed consecutive patients diagnosed with thyroid and parathyroid diseases, including thyroid carcinoma, thyroid nodular goiter, thyroid adenoma, Graves’ disease, and parathyroid adenoma, who were admitted to the Center for Thyroid and Breast Surgery, Department of General Surgery, Xuanwu Hospital from October 2012 to December 2017. These patients’ clinicopathologic features were comprehensively recorded and analyzed. The patients were divided into an IONM group and visualization alone group (VA group) according to whether RLN monitoring technology was used during the operation. We excluded patients with neural paralysis as detected by laryngoscopic examination prior to thyroid and parathyroid surgery, patients requiring removal of malignant lesions invading the RLN as observed during surgery, and patients without a complete case record.
Establishment and implementation of IONM system
The NIM-Response 3.0 monitoring system (Medtronic Inc., Minneapolis, MN, USA) and a standard reinforced tracheal catheter were used to monitor the RLN during surgery. A non-depolarizing muscle relaxant (rocuronium, 0.3 mg/kg) was given during anesthetic induction, and no further muscle relaxant was used during the surgery. Tracheal intubation was performed through a visual laryngoscope to ensure good contact between the surface electrodes of the tracheal tube and the bilateral vocal cords. Intermittent IONM was used for RLN monitoring. The RLN and vagus nerve were stimulated directly with a handheld monopolar device during the operation.
The six-step procedure for IONM was performed as follows. First, the bilateral vocal cord function was examined with a laryngoscope prior to surgery. Second, the ipsilateral vagus nerve signal was detected to determine whether the monitoring system had been successfully set up or whether a non-RLN mutation was present. Third, the ipsilateral RLN signal was recorded before thyroidectomy. Fourth, the RLN signal was recorded after the thyroid gland resection. Fifth, the vagus nerve signal was recorded to confirm the nerve function. Finally, the movement of the bilateral vocal cords was examined and assessed by laryngoscopy after surgery.
Surgical procedure
Patients diagnosed with benign thyroid goiters underwent subtotal thyroidectomy or unilateral lobectomy according to the size and location of the lesion. Patients with thyroid carcinoma underwent thyroid lobectomy or total thyroidectomy with central or lateral lymph node dissection based on the presence of a malignant lesion and lymph node metastasis. All resected specimens were confirmed by pathological examination.
Loss of signal
Loss of signal (LOS) was defined as a reduction in the amplitude of the EMG signal by >50% compared with the initial baseline value or to <100 µV under the condition that an EMG signal above the threshold (usually set at 100 µV) could be elicited by stimulating the RLN with a 1- or 2-mA current in a clean surgical field. When LOS occurred during the surgery, the RLN was carefully checked for any visible damage. In such cases, stimulating the contralateral vagus nerve may help to determine whether real LOS is present rather than equipment failure. 11 If the occurrence of LOS was believed to have been caused by nerve injury, laryngoscopy was performed at 2 days and 1, 3, and 6 months after the operation. Vocal cord paralysis that could not be recovered 6 months after surgery was defined as permanent RLN injury.
Statistical analysis
Data were analyzed with SPSS version 23.0 (IBM Corp., Armonk, NY, USA). The statistical significance of categorical variables was evaluated using Pearson’s chi-square test, and that of continuous variables was calculated using the unpaired two-tailed Student’s t-test. A p value of <0.05 was considered statistically significant.
Ethics
This study was approved by the Ethics Committee of Xuanwu Hospital, Capital Medical University based in Beijing, China (20 April 2020, ID [2020]055). The requirement for informed consent was waived because of the retrospective nature of the study. The patients’ data were kept confidential, and the details were presented such that the identity of the patients cannot be ascertained. All procedures were performed in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
Patients’ general characteristics
Of 1059 consecutive patients who were diagnosed with thyroid and parathyroid diseases, 1033 patients (280 men and 753 women with 478 malignant tumors and 555 benign tumors) were included in this study. Nineteen patients underwent parathyroid surgery and 85 underwent secondary thyroid surgery. In total, 1696 at-risk nerves were included in the analysis; of these, 597 nerves were found to be at risk during central lymph node dissection, and 92 nerves were found to be at risk during lateral lymph node dissection. The at-risk nerves were divided into a high-risk and low-risk group according to the following risk factors for RLN injury proposed by Dralle et al. 10 and Barczynski et al.: 9 recurrent benign and malignant goiters, primary surgery for thyroid malignancy, Graves’ disease, giant thyroid goiters (>300 g), and goiters with a retrosternal component. The differences in age and sex were not statistically significant between the two groups, but significantly more malignant lesions were present in the IONM group than in the VA group (p < 0.001) (Table 1).
Clinical characteristics in IONM group and VA group.

Data are presented as median (lower quartile, upper quartile) or n (%).
IONM, intraoperative neuromonitoring; VA, visualization alone.
Incidence of RLN palsy
The overall incidence of postoperative RLN paralysis was 2.00%, while the incidence of transient and permanent injury was 1.83% and 0.17%, respectively. There were 1104 and 592 at-risk nerves in the IONM and VA group, respectively. No significant difference was present in the incidence of overall, transient, or permanent RLN injury between the IONM and VA groups (Table 2).
Incidence of RLN palsy in IONM group and VA group.

Data are presented as n (%).
RLN recurrent laryngeal nerve; IONM, intraoperative neuromonitoring; VA, visualization alone
The effects of different surgical procedures and risk factors on the incidence of RLN injury were also compared. The use of IONM reduced the risk of permanent injury of high-risk nerves (p = 0.047), and the incidence of RLN paralysis was higher in patients undergoing lateral cervical lymph node dissection in the VA group than IONM group (p = 0.003) (Table 3).
Incidence of RLN palsy in different surgical procedures and risk classification.

Data are presented as n (%).
RLN recurrent laryngeal nerve; IONM, intraoperative neuromonitoring; VA, visualization alone; LN, lymph node.
The RLN is generally believed to be minimally damaged during lateral neck lymph node dissection. The data of the present study suggest that the application of IONM significantly reduced the risk of RLN injury during lateral cervical lymph node dissection (p < 0.05). We believe that the probable cause of this phenomenon is that patients requiring lateral neck lymph node dissection often have severe central lymph node metastasis. The metastatic lymph nodes may have an indistinguishable tissue structure or may even show adhesion to or invasion of adjacent nerves, resulting in RLN injury during central lymph node dissection. The rate of central lymph node metastasis in patients undergoing lateral neck lymph node dissection was 0.49 in our clinical data. Therefore, we analyzed the correlation between central lymph node dissection and RLN palsy in all 1696 at-risk nerves. The results confirmed that central lymph node dissection significantly increased the risk of RLN injury (p < 0.05) (Table 4) and that RLN injury was significantly associated with the number of positive lymph nodes (p < 0.05) (Table 5), especially when the rate of central lymph node metastasis reached 0.4808 based on the receiver operating characteristic curve (p < 0.001) (Figure 1).
Effects of CLND on risk of RLN injury.
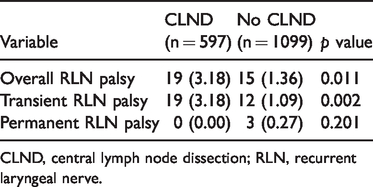
CLND, central lymph node dissection; RLN, recurrent laryngeal nerve.
Spearman correlation analysis of lymph node metastasis and recurrent laryngeal nerve injury.
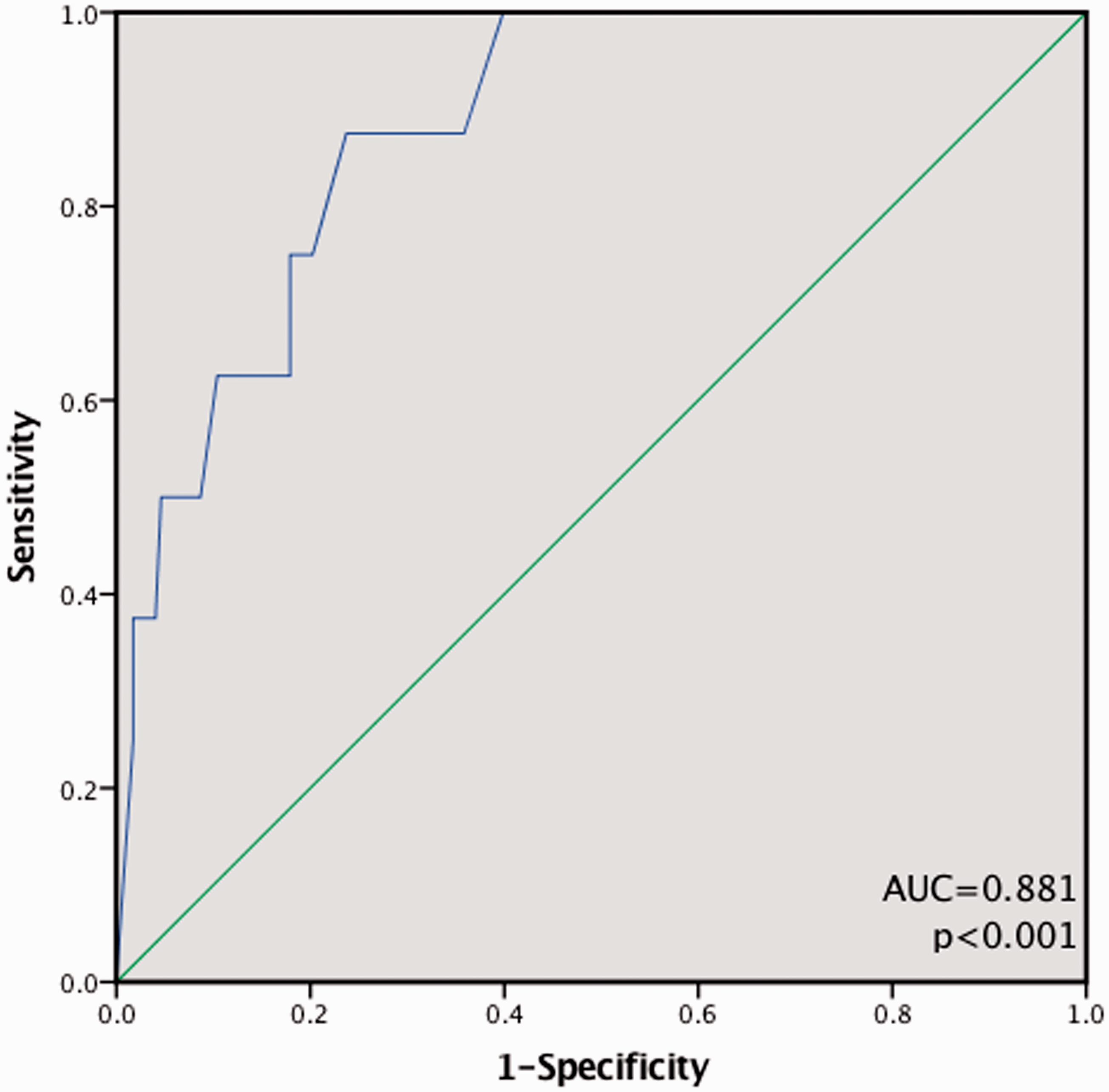
Receiver operating characteristic curve for predicting recurrent laryngeal nerve injury by ratio of central lymph node metastasis. AUC, area under the curve.
LOS and vocal cord paralysis
Of the 34 cases of RLN injury, traction injury occurred in 28 cases (82.4%), clamping injury in 2 (5.9%), thermal injury caused by a monopolar or energy-based device in 2 (5.9%), and transection injury in 2 (5.9%). LOS occurred in 52 at-risk nerves, and ipsilateral vocal cord paralysis was confirmed by laryngoscopy in only 34 cases. The positive predictive value of intraoperative LOS in cases of postoperative vocal cord paralysis was 65.38%. Paralysis of the right vocal cord was found in one patient by postoperative laryngoscopy but no LOS was detected during surgery, possibly because of the surrounding tissue edema that compressed the RLN after the surgery. With the adoption of IONM, the negative predictive value of postoperative RLN palsy reached 99.90%.
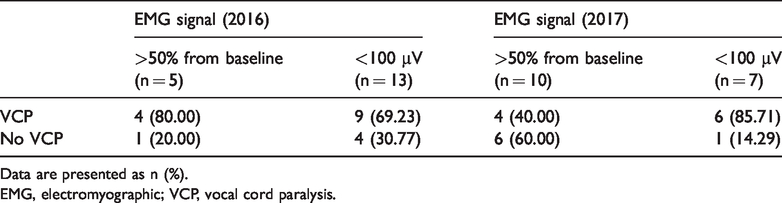
To further explore the correlation between changes in EMG signals and postoperative vocal cord function, we analyzed the patients who underwent laryngoscopic examinations before and after surgery with recording of the intraoperative EMG signals in 2016 and 2017. Compared with 2016, the number of patients with EMG amplitudes of <100 µV dropped by 57% in 2017. Beyond that, a decrease in the EMG amplitudes by >50% from baseline were detected in 10 patients, but vocal cord paralysis was found by postoperative laryngoscope in only four patients (40%). In 2016, among the patients with EMG amplitudes that had decreased by >50%, the proportion of those with vocal cord paralysis was twice that in 2017 (80%) (Table 6). Thus, when a significant reduction in the amplitude of the EMG signal is observed, immediate cessation of high-risk surgical operations is an effective way to avoid more serious injuries.
EMG signal changes in 2016 and 2017.

Data are presented as n (%).
EMG, electromyographic; VCP, vocal cord paralysis.
Discussion
Early in 1938, Lahey and Hoover 12 reported that exposing and identifying the RLN during surgery can effectively reduce the incidence of RLN injury. Routine visualization of the RLN has gradually been accepted as the gold standard for reducing the incidence of RLN injury. The RLNs are vulnerable during thyroid and parathyroid surgery because of various anatomic anomalies. 13 IONM during thyroid and parathyroid surgery was proposed by Shedd and Durham 14 in 1966 and by Flisberg and Lindholm 15 in 1969. To date, 90% of thyroid surgeons have accepted the IONM technique for RLN identification and protection, and 71% of surgeons routinely apply IONM. 16 However, whether the application of IONM technology can reduce the risk of RLN injury during thyroid and parathyroid surgery remains controversial.
In recent years, there has been marked variation in the results of individual newly published clinical studies, which has prevented a consensus on IONM application. Several studies have suggested that IONM technology can reduce the risk of RLN injury and effectively protect the RLN,9,17 but other studies have shown that IONM technology cannot substantially reduce the risk of RLN injury.6,18–23 Although several meta-analyses have been performed in an attempt to increase the statistical power by a combination of several published individual studies, 24 few high-quality randomized controlled trials (RCTs) were included. 3 Therefore, well-designed RCTs with a larger number of cases and longer follow-up are needed. 25 Among the published studies, Barczynski et al. 9 observed 2000 at-risk nerves in an RCT and concluded that the adoption of IONM can significantly reduce the incidence of transient RLN palsy in high-risk nerves (p = 0.011). The results of a multicenter study conducted by Thomusch et al. 26 involving 45 hospitals and 4382 patients with thyroid benign goiters revealed that the use of IONM decreased the incidence of transient (p = 0.008) and permanent (p = 0.004) RLN injuries. In addition, three meta-analyses recently published by Zheng et al., 27 Yang et al., 28 and Wong et al. 1 supported the above findings. In the present study, the incidence of permanent RLN injury in the high-risk VA group was 0.67% compared with 0.00% in the IONM group. Although this difference was statistically significant, whether it represents a truly meaningful clinical significance is unclear. A larger number of cases and longer follow-up are still needed to draw a more convincing conclusion.
A meaningful finding in our study is that IONM might be recommended for patients with a high positive rate of lymph node metastasis requiring extensive central and lateral cervical lymph node dissection. From an anatomical point of view, the RLN is minimally damaged directly during lateral neck lymph node dissection unless the vagus nerve is injured during the dissection. However, no vagus nerve injury occurred in our study. As we mentioned above, the requirement for lateral neck lymph node dissection is associated with more central lymph node metastases, and a higher ratio of positive central lymph nodes leads to a greater risk of RLN injury. Accordingly, we consider that central lymph node dissection and extensive lateral lymph node dissection remain certain risk factors for RLN injury because of the indirect effects of lateral lymph node dissection on the RLN. A study conducted by Moritani 29 showed that RLN invasion by positive lymph nodes occurred more often on the right than left side; moreover, the paratracheal lymph nodes in the central area of the right neck could be divided into two parts by the right RLN. 30 Patients with thyroid papillary carcinoma often have metastatic lymph nodes posterior to the right RLN, which increases the risk of RLN injury during lymph node dissection. Consequently, our experience suggests that IONM might be actively used to reduce the risk of RLN injury in patients with severe central lymph node metastasis, especially on the right side, who are highly susceptible to the need for extensive cervical lymph node dissection during the operation.
The development and application of continuous IONM technology in recent years has provided a new method for monitoring and protecting the RLN. In our study, only intermittent IONM technology was used to observe the advantage of this technique in intraoperatively protecting the RLN. However, intermittent IONM technology can detect suspicious injury only after the injury has occurred. Continuous IONM enables timely intervention for impending RLN injury by regular intermittent stimulation of the vagus nerve and real-time signal variation. When surgeons notice changes in amplitude and latency during an operation that may cause RLN injury, immediately stopping the operation may effectively reduce the risk of postoperative voice cord paralysis. 31 Continuous IONM is being actively carried out in our department in preparation for further research of the advantages of this technique.
Our study has two main limitations. First, this was a single-center retrospective study; a multicenter study with a larger number of cases and longer follow-up is necessary to further confirm the advantages of IONM technology. Second, because retrospective studies have inherent inclusion bias, patients with risk factors for RLN injury were more likely to choose IONM technology during the operation. Therefore, the protective effect of IONM on the RLN still needs to be confirmed by high-quality RCTs.
Conclusions
The adoption of IONM
Footnotes
Acknowledgement
We would like to thank all colleagues who were involved in the data collection for this study.
Authors' contributions
Conception and design: H Kang; administrative support: H Kang; provision of study materials or patients: J Zhao, Y Zhao, and Y Wang; collection and assembly of data: Y Ling and K Li; data analysis and interpretation: Y Ling; manuscript writing: all authors; final approval of manuscript: all authors.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by the Beijing Municipal Health System Academic Leaders of High-level Health Personnel Program, P.R. of China (No. 2011-2-28).