
Abstract
Study Design
Institutional review board-approved retrospective cohort study.
Objectives
Failure to achieve alignment goals may result in accelerated adjacent segment degeneration and poorer outcomes. In “open” spine surgery, intraoperative tools can fine tune alignment; minimally invasive spine surgery techniques may not allow for this type of intraoperative adjustment. The aim of this study was to identify pre-operative radiographic parameters that accurately predict post-operative alignment after minimally invasive lumbar spine surgery. We hypothesized that pre-operative supine and extension sagittal alignment would predict post-operative standing alignment.
Methods
50 consecutive patients underwent lateral or anterior lumbar interbody fusion with or without percutaneous posterior instrumentation by a single-surgeon. Sagittal alignment parameters were evaluated on pre-operative standing scoliosis radiographs, dynamic radiographs, supine CT scout, and 6-week post-operative standing radiographs. Demographic and perioperative data were analyzed.
Results
The mean age was 67.8 years. The mean BMI was 29.7. On average, 3 levels were instrumented (range, 2–6). Surgical time was 4.5 ± 1.8 hours. Following surgery, global lordosis increased from 44.7 ± 17° to 48.6 ± 16° (P = .001). However, there was no significant difference between the pre-operative supine (48.5 ± 15°), pre-operative extension (49.2 ± 18°), or 6-week post-operative standing radiographs (48.6 ± 16°). There were strong correlations between post-operative alignment and pre-operative supine (r = .825) and extension (r = .851) alignment.
Conclusions
Our results suggest that pre-operative supine and extension radiographs could be a gold standard for minimally invasive lumbar spine surgery alignment correction as they predict post-operative alignment. The extension alignment was the strongest predictor of post-operative alignment.
Introduction
Lumbar degenerative spine disease is a leading cause of morbidity and hospital visits. Globally, 266 million patients complain of symptomatic degenerative spine disease yearly. 1 Thus, when indicated, goals of surgically managed degenerative lumbar spine disease include reducing pain and improving functional status. While the pursuit of this is multifactorial, achieving appropriate sagittal alignment remains an essential aspect of spine surgery. Failure to achieve regional alignment goals may result in accelerated adjacent segment degeneration and poor clinical outcomes.2-6
With the progression and expanding indications for minimally invasive spine surgery (MISS), understanding the limitations and capabilities of these techniques is all the more important. In traditional “open” spine surgery, several intraoperative tools, including increased bony release, compression, distraction, etc., can be used to fine tune alignment. 7 Unfortunately, MISS techniques usually do not allow for this type of intraoperative adjustment. For this reason, surgeons must decide if their surgical plan will allow for appropriate correction pre-operatively. It is therefore critical for surgeons to be able to predict post-operative alignment based pre-operative data. Though guidelines for the use of MIS techniques have been previously published, 8 development of these tools will allow surgeons to more appropriately identify patients who may benefit from MISS procedures.
The goal of this study was to determine how pre-operative radiographic sagittal alignment parameters predict early post-operative standing alignment. Using pre-operative standing scoliosis films, dynamic radiographs, and the supine CT scout, we sought to correlate pre- and post-operative sagittal alignment measures. This would allow for surgeons to pre-operatively predict post-operative alignment.
Methods
Before initiation, the Hospital for Special Surgery Institutional Review Board approved the study (IRB Study #2020-0460). This retrospective, observational study was deemed exempt from requiring informed consent. The study included 50 consecutive patients with degenerative disc disease or spondylolisthesis (isthmic or degenerative) who underwent extreme lateral, oblique lateral, or anterior lumbar interbody fusion with or without percutaneous posterior instrumentation by a single-surgeon between November 2018 and February 2020. Patients who underwent open posterior surgery or osteotomies were excluded from the study.
Sagittal alignment parameters, including global lumbar lordosis, segmental lumbar lordosis, and pelvic incidence-lumbar lordosis (PI-LL) mismatch on pre-operative standing full-length scoliosis and dynamic (flexion and extension) radiographs, the pre-operative supine CT scout, and on standing radiographs at 6 weeks post-operative were evaluated. All parameter measurements were performed by 2 authors (L.A.B. and H.M.) using Sectra Ortho Toolbox (SECTRA Orthopaedics, Sweden) on de-identified imaging. The researchers were blinded to the pre-operative parameters when performing the post-operative measurements.
Demographic and perioperative data including procedure performed, surgical time, hospital length of stay, and complications were analyzed. Repeated measures ANOVA, combined with the Bonferroni correction for multiple comparisons, was used to compare sagittal alignment parameters on pre-operative standing, pre-operative supine, pre-operative dynamic, and 6-week post-operative standing imaging. Tukey post hoc testing was used when applicable for pairwise comparisons after ANOVA analyses. Multilinear stepwise regressions were performed to identify strongest predictor of post-operative alignment between pre-operative supine, pre-operative extension, and cage implant. The regression coefficient and R values were reported. Statistical tests were all two-tailed and a α level of .05 was determined to be statistically significant.
Results
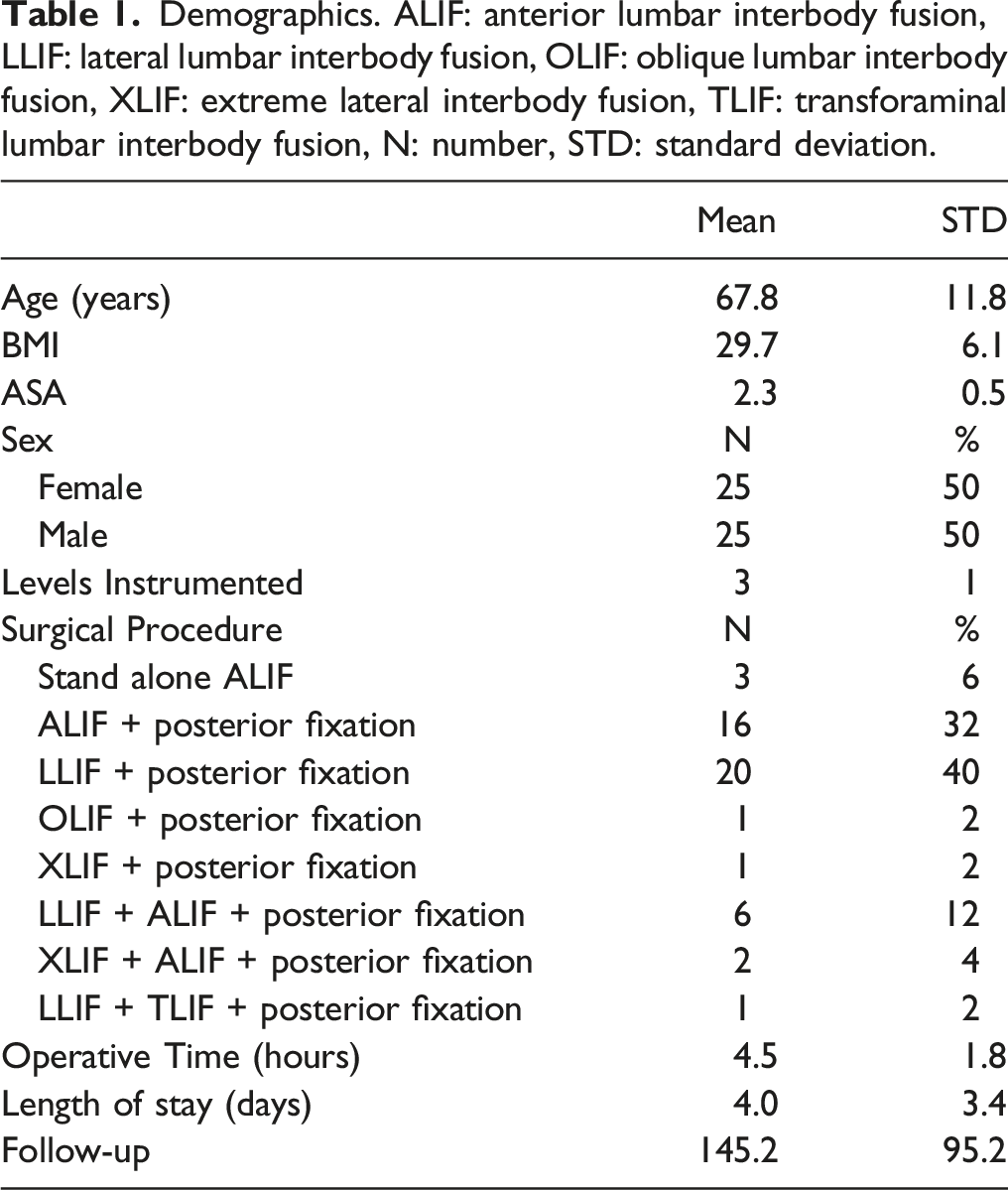
Demographics. ALIF: anterior lumbar interbody fusion, LLIF: lateral lumbar interbody fusion, OLIF: oblique lumbar interbody fusion, XLIF: extreme lateral interbody fusion, TLIF: transforaminal lumbar interbody fusion, N: number, STD: standard deviation.
Pre-operative Standing Compared to Post-operative Standing Radiographs
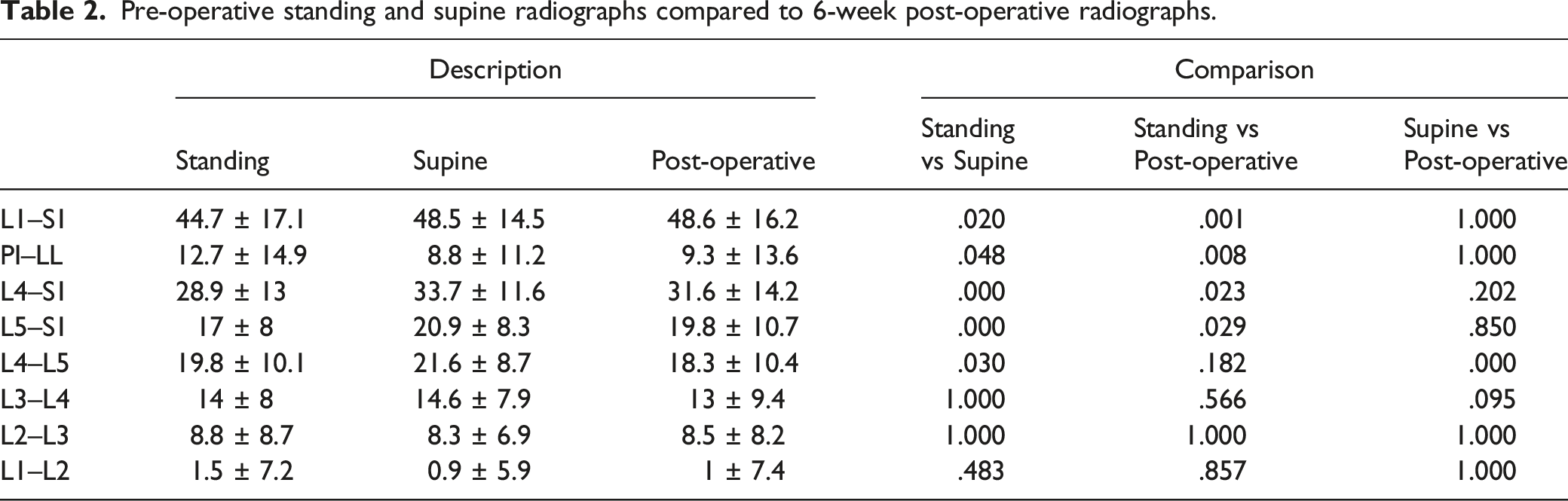
Following surgery, global lordosis increased from 44.7 ± 17 to 48.6 ± 16° (P = .001). Statistical significance can also be seen when evaluating PI-LL mismatch, L4–L5, L4–S1, and L5–S1 segmental lordosis between pre-operative standing and early post-operative radiographs (Figure 1, Table 2). Pre-operative standing, supine, and extension radiographs compared to 6-week post-operative global lordosis. Pre-operative standing and supine radiographs compared to 6-week post-operative radiographs.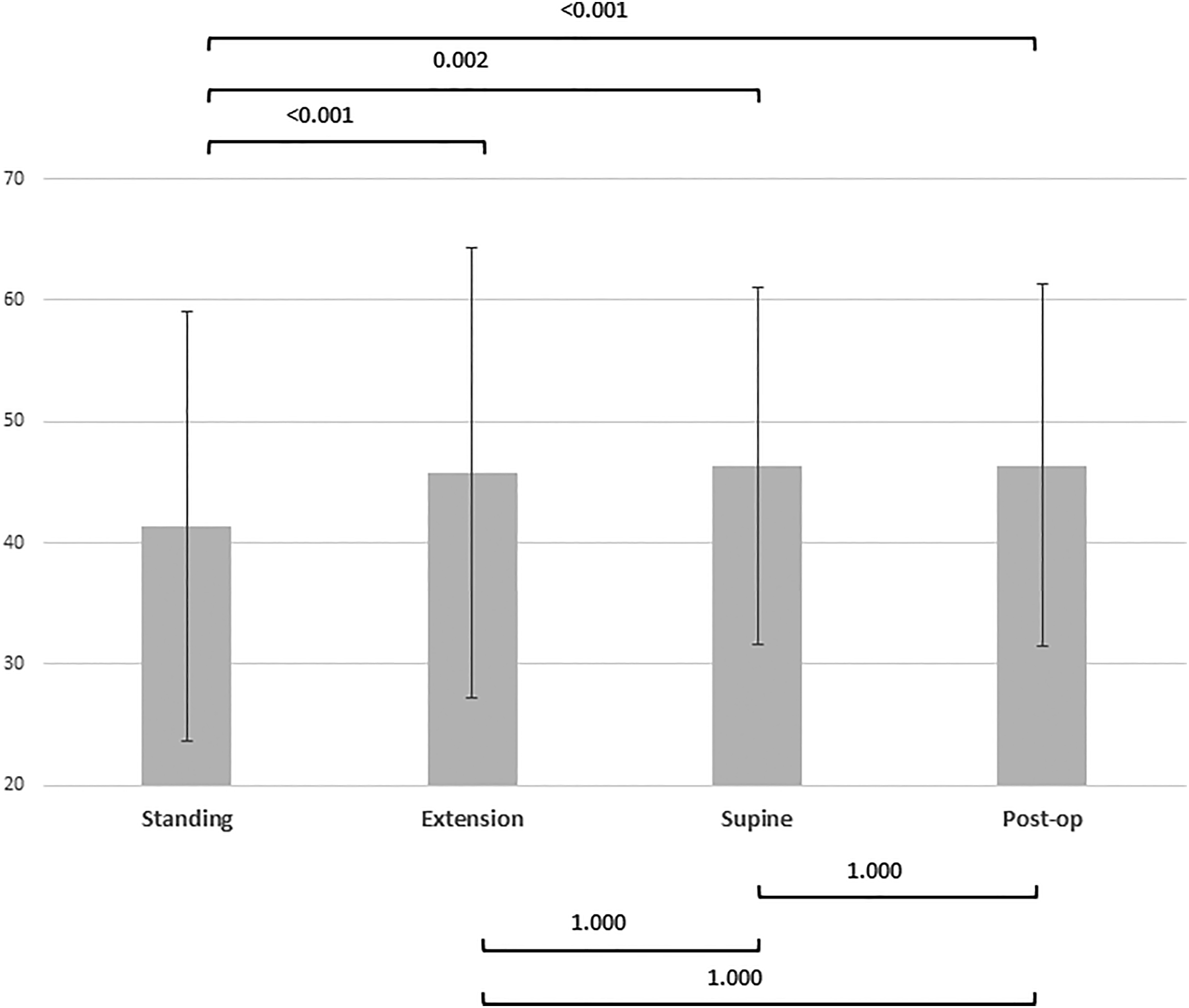
Pre-operative Supine Compared to Post-operative Standing Radiographs
There was no significant difference between the pre-operative supine global lumbar lordosis (48.5 ± 15°) and that on the 6-week post-operative standing radiographs (48.6 ± 16°). There were strong correlations between post-operative standing and pre-operative supine (r = .825, P = .001) alignment as found through repeated measures ANOVA. In contrast to the comparison between pre- and post-operative standing alignment, there was no significant difference between pre-operative global lumbar lordosis on supine imaging and 6-week post-operative radiographs (48.5 ± 15° vs 48.6 ± 16°, P = 1.000; Table 2).
The same lack of statistical significance can be seen when evaluating PI-LL mismatch, L1–L2 to L5–S1 segmental lordosis between pre-operative supine imaging and 6-week post-operative radiographs (Table 2). The only exception is for the L4–L5 segmental lordosis (P < .05).
When stratified by operative segment, there was a statistically significant increase in lordosis by 2.6°. The supine segmental angle was the most important predictor of post-operative segmental angle, more so than pre-operative standing angles or cage angle.
Individual linear regression between pre-operative supine and post-operative standing sagittal alignment demonstrated strong correlation. Figure 2 shows the scatter plot specifically for global lordosis where r = .996 (P < .001). PI-LL mismatch was also closely correlated pre-operative supine and post-operative standing (data not shown) with r = .967 (P < .001). The stepwise elimination also showed that segmental lordosis of the operated level on pre-operative supine imaging was found to be a stronger independent predictor of post-operative sagittal alignment than implant geometry (data not shown). Pre-operative Supine and Early Post-operative Standing Global Lordosis Regression Model. There was a strong correlation between the pre-operative supine and post-operative alignment (r = .825). The stepwise regression demonstrated a coefficient of almost 1 with no constant between supine and post-operative alignment.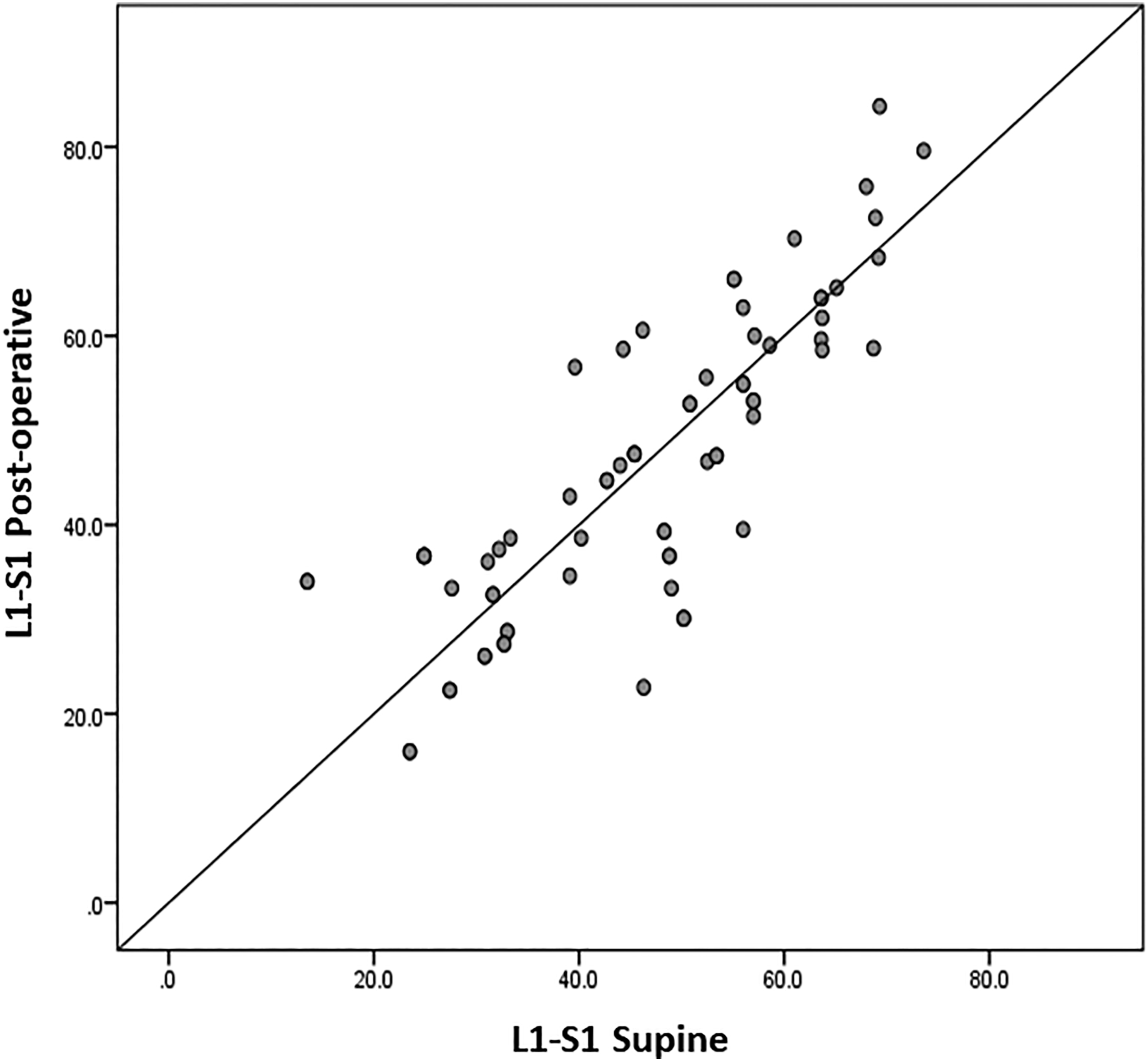
Pre-operative Dynamic Compared to Post-operative Standing Radiographs
72% had pre-operative flexion/extension radiographs available for review. The mean arc of motion from L1–S1 between flexion and extension was 13.5 ± 9.3°. There was no significant difference between the pre-operative extension (49.2 ± 18°) and the 6-week post-operative standing radiographs (48.6 ± 16°). Again, there were no significant differences in PI-LL mismatch between pre-operative extension and post-operative standing alignment (Figure 1).
There were strong correlations between post-operative and extension alignment (r = .851). Furthermore, pre-operative extension alignment is a stronger predictor of post-operative alignment than supine alignment or cage size.
Post-Operative Course
The most common post-operative complications were anterior thigh/groin numbness or pain (seen in 4 patients) and radiculopathy (4 patients). Two patients had iliopsoas weakness likely due to the approach, which improved. One patient had 3 retained k-wire tips within the vertebral bodies. Two patients required post-operative blood transfusions. One patient had a superficial wound dehiscence, which improved with local wound care.
The mean hospital length of stay was 4.0 ± 3.4 days (range, 1–20 days) with an average follow-up of 145.2 ± 95.7 days (range, 34–386 days). Two patients underwent revision surgery (1 revision decompression and fusion 7 months post-operatively for persistent radiculopathy and 1 revision fusion 4 months post-operatively for symptomatic cage subsidence).
Discussion
We performed a retrospective analysis of lumbar fusions using circumferential minimally invasive spine (cMIS) techniques. While lumbar lordosis increased post-operatively, there was no significant difference between sagittal parameters on pre-operative supine or extension imaging and post-operative standing radiographs. These results suggest that the lordosis measured on pre-operative supine or extension radiographs determines the degree of correction that can be expected post-operatively (Figure 3). If additional correction is required (e.g., rigid curves or significant sagittal malalignment), surgeons should consider additional releases or an open approach. Case example: 61-year-old female presenting with 2 months of lower back pain with radiation to her anterior thigh and motor weakness in the L4/L5 nerve distribution. Imaging confirmed a grade 2 spondylolisthesis at L4–L5 with disc height loss and collapse. Additionally, she has central canal stenosis, bilateral recess stenosis, and bilateral left greater than right foraminal stenosis (not shown). She underwent an L4–L5 lateral lumbar interbody fusion with posterior instrumentation and had an unremarkable post-operative course. Images above are sagittal radiographs (from left to right): pre-operative standing, pre-operative supine, pre-operative extension, and early post-operative timepoints. Measurement shown is the global lumbar lordosis (L1 to S1).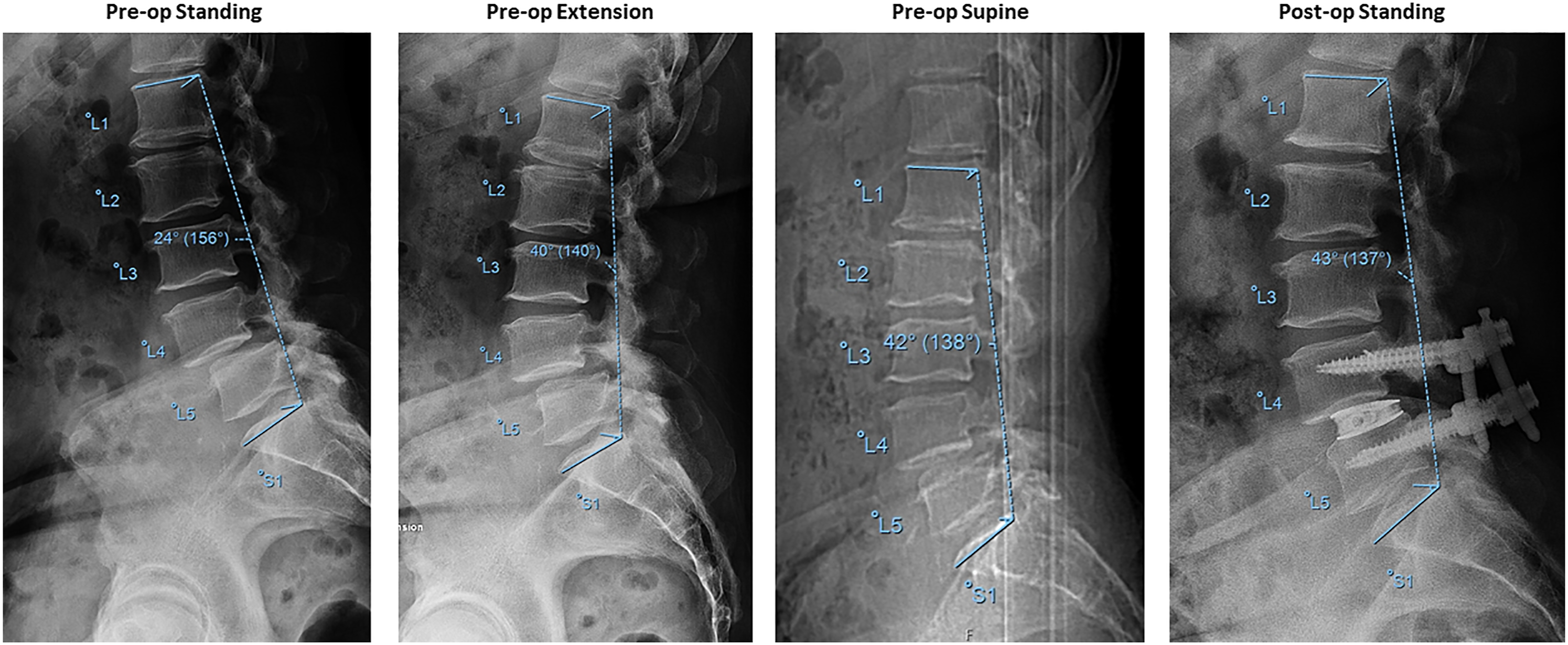
Minimally invasive lumbar spine surgery has several advantages. The ability to decrease complication rates while maintaining clinical outcomes has been shown in several prior studies.9-12 However, as with any technique, there are limitations. With regards to sagittal alignment, minimally invasive techniques prevent surgeons from using intraoperative tools available in traditional “open” spine surgery to achieve alignment. Given the risks of inadequate correction, including accelerated adjacent segment disease and poorer clinical outcomes, it is imperative to pre-operatively understand the possibilities and limitations of cMIS. Thus, prediction of post-operative alignment based on pre-operative data is critical.
In this study, pre-operative standing sagittal alignment demonstrated a significant difference when compared to post-operative standing alignment. Importantly, pre-operative supine and pre-operative extension imaging were not significantly different from post-operative standing sagittal alignment. As such, these 2 pre-operative modalities were both strong predictors of post-operative alignment. Regression analyses demonstrated that pre-operative extension sagittal alignment was the best predictor of post-operative alignment, outranking competing variables such as implant geometry and choice of approach.
The importance of attaining sagittal balance has been established within the traditional “open” literature.13-15 Given the fundamental importance of restoring this alignment, this principle is also applied in cMIS techniques. 8
As described by Park et al., 16 cMIS through oblique lateral interbody fusion (OLIF) successfully corrected marked sagittal deformity, as defined by SVA >9.5 cm, PI-LL mismatch >20°, or PT > 30°, in adult spinal deformity patients. In their retrospective review of 23 patients, they found a statistically significant increase in lumbar lordosis and PI-LL mismatch at 2 years post-operatively as measured on plain film. In agreement with Park et al., the present study in adult patients with degenerative lumbar disease demonstrates a significant increase in lumbar lordosis after cMIS. However, Park et al.’s, study did not evaluate for predictors of post-operative alignment and focused on adult deformity patients undergoing fusion utilizing one MIS technique (OLIF).
Similarly, in their retrospective review of 35 patients who underwent primary lateral interbody fusion, Blizzard et al. found a statistically significant increase in global lumbar lordosis, 17 similar to that found in our study. However, their study was again focused on adult spinal deformity patients and did not evaluate for post-operative alignment predictors.
Nevertheless, cMIS is limited by the minimally invasive nature of the approach. Mummaneni et al. and the Minimally Invasive Surgery Section of the International Spine Study Group identified these limitations and created a minimally invasive spinal deformity surgery algorithm as a decision framework for MIS vs open spine surgery. With substantial inter- and intra-observer reliability, their algorithm takes into account the possibility of suboptimal sagittal plane correction with MIS in adult spinal deformity. 8 Generally speaking, these algorithms recommend MIS techniques for flexible curves with mild or moderate degrees of deformity. This approach is largely in keeping with our current findings. However, we believe our study adds to this data because it provides information on extent of the correction that might be achieved via MIS techniques.
Therefore, predicting which patients would benefit from MIS techniques without the complications of inadequate sagittal correction is critical. To our knowledge, this is the first study to use pre-operative radiographic alignment as a predictor of post-operative sagittal alignment. In this study, we demonstrated that pre-operative supine and extension alignment are strong predictors of early post-operative alignment in circumferential minimally invasive lumbar spine fusions.
The strength of this study is the robust data collection. All patients in the study had pre-operative standing radiographs and supine imaging as well as 6-week post-operative radiographs. 50 consecutive patients were reviewed and each patient served as their own control.
However, a weakness of this study is the short-term follow-up and subsequent lack of associated clinical outcomes. Though pre-operative supine alignment is a predictor of early post-operative alignment, it is unclear if this continues with longer-term evaluation. Further studies are needed to evaluate loss of or change in lordosis with longer follow-up. Another potential limitation of this study is the generalizability. Overall, patients included in this study had a pre-operative lordosis of 44.7 ± 17°. Findings in patients with more sagittal plan deformity may have differing findings. Additionally, this study is limited by the retrospective and observational nature. Though all patients who met criteria were included, there is a risk of selection bias with initial patient selection and indications for cMIS. Furthermore, patients were limited to those with degenerative conditions of the lumbar spine who underwent MISS fusion procedures; these findings may not be applicable to other populations. Another limitation is the smaller sample size and grouping of multiple MISS techniques. Due to the limited number of patients available, stratification by surgical approach, levels, or diagnoses was not possible.
Conclusion
We sought to identify predictors of post-operative alignment after minimally invasive lumbar spinal fusions. Pre-operative alignment measures on supine and extension radiographs were the most important predictors of post-operative alignment after MISS. Our results suggest that the supine and extension radiographs could be considered the “gold standard” when planning MISS alignment correction in the lumbar spine. If more correction is required, surgeons should consider additional releases (e.g., anterior longitudinal ligament release) or an open approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.