
Abstract
Study Design
Prospective single-center study.
Objective
This study aimed to investigate the muscle activity of the trunk, pelvis, and lower limb, which are used to maintain a standing posture in elderly patients with spinal deformities. We also elucidated the mechanism of compensation against spinal deformity in terms of muscle activity.
Methods
Any patient scheduled to undergo surgery for adult spinal deformity was included. Surface electromyography and radiography were performed preoperatively. The following four representative alignments were defined as compensations: 1. pelvic retroversion, 2. reduction in thoracic kyphosis, 3. hyperextension of the lumbosacral junction, and 4. knee flexion. Individual muscle activity was compared with and without compensation. The patients were stratified into three groups according to the severity of spinal compensation, and differences in muscle activity were compared.
Results
This study included 76 patients (7 men and 69 women, average age 69.4 years). Our results revealed that pelvic retroversion and knee flexion were compensations that required trunk muscle activity. In contrast, reduction of thoracic kyphosis and hyperextension of the lumbosacral junction did not require much trunk muscle activity. There was a significant difference in the muscle activity of the pelvis and lower limbs according to the severity of the deformity.
Conclusions
In terms of muscle activity, compensation for regional alignment changes in the adjacent spine is economical. However, extra-spinal compensations, such as pelvic retroversion and knee flexion, are non-economical. According to compensation recruitment, the muscle activity of the pelvis and lower limbs increased with the severity of the spinal deformity.
Keywords
Introduction
It has been reported that sagittal malalignment of the spine and pelvis is related to the quality of life (QOL),1,2 which is an essential issue in the research of spinal deformities in middle-aged and elderly patients. Recently, many authors have reported spinal malalignment, and the biological responses to this phenomenon have become clear. A compensatory function is recruited against spinal malalignment to maintain an upright posture. The main compensatory mechanisms for spinal malalignment include cervical hyperextension, reduction of thoracic kyphosis, and hyperextension of adjacent segments (e.g., hyperextension of the lower lumbar spine), and/or pelvic retroversion, knee flexion, and ankle dorsiflexion.3-5 However, the exact mechanism of compensatory function has not been elucidated. These mechanisms together are rarely observed in the same patient; however, they are usually present in various degrees, depending mainly on the stiffness of the spine, condition of the muscles, level of pain, and severity of the imbalance. 4 The compensatory mechanisms involving the spine, pelvis, and lower extremities are thought to be related to muscles, as there are several research reports on spinal deformity and muscle.6-8 The ideal way to evaluate muscles is to assess muscle strength, but it is challenging to accurately evaluate patients’ muscles with spinal deformity as dynamic review is not possible. Thus, imaging evaluations, such as cross-sectional muscle area, are often used as a substitute. Spinal malalignment and pelvic position are associated with the erector spinae and lower limb muscles.7,8
We hypothesize that when the compensation mechanism is working for spinal sagittal malalignment, the specific trunk and lower limb muscles contract, which may induce symptoms such as fatigue and pain. 9 It is necessary to study the muscles that maintain the standing position in patients with spinal deformities in real time. Surface electromyography (s-EMG) is a non-invasive physical test used to evaluate muscle activity in real time and has been used to evaluate limb and erector spinae muscles.9,10 However, various methods have been reported to evaluate muscle activity, this report describes the first real-time evaluation of muscle activity to maintain the standing posture using s-EMG. The objective of this study was to investigate the muscle activity of the trunk, pelvis, and lower limb in elderly patients with spinal deformities. Additionally, the mechanism of compensation against spinal deformity will be elucidated in terms of muscle activity.
Materials and Methods
The institutional review board at our institution approved this study (approval number 15-284), and written informed consent was obtained from all participants. This study was designed as a single-center prospective case series. Any patient who was scheduled to undergo surgery for adult spinal deformity (ASD) between September 2016 and March 2020 and who consented to electromyography was eligible for this study. We excluded patients with neuromuscular diseases, congenital and syndromic deformities, infections, and spinal tumors. Demographic variables included age, sex, weight, height, and body mass index. S-EMG and radiographic examinations were performed preoperatively. A standard lateral radiograph of the entire spine was obtained in a relaxed standing posture with the fingers on the clavicles. The spino-pelvic parameters measured on lateral radiographs were as follows: lumbar lordosis (LL), thoracic kyphosis (TK), sagittal vertical axis (SVA), sacral slope (SS), pelvic tilt (PT), pelvic incidence (PI), T1 pelvic angle (TPA), 11 lordosis in the lower lumbar vertebrae (L4/S lordosis), defined as the angle between the L4 and S1 superior endplates, and femoral oblique angle (FOA),12,13 defined as the angle between the femoral axis and vertical line, using the average of left and right sides in the analysis. Patient-reported outcomes (PRO) were assessed using the Oswestry Disability Index (ODI) and the Scoliosis Research Society–22 r (SRS-22r) questionnaire.
Measurement of Surface Electromyography
A telemetric EMG system (Telemyo™ DTS, Noraxon, Scottsdale, USA) was used to measure the s-EMG. Six muscles were assessed: the thoracic and lumbar erectors (TES and LES), and abdominal external oblique (AEO) as the trunk muscles; gluteus maximus (GM) as the pelvic muscle; rectus femoris (RF), and biceps femoris (BF) as the lower extremity muscles. Only the right side of the muscle was measured because of the lack of channels in the measuring equipment. The TES and LES were assessed 5 cm to the right of the midline of the level at the angulus inferior scapulae and the spinous process of the fourth lumbar vertebra, respectively. The skin of the measurement site was cleaned using alcohol cotton to ensure low impedance. Subsequently, the s-EMG electrodes were attached to the muscle belly of each muscle at a distance of 2 cm in the direction of the muscle fibers. The s-EMG conditions were 500 Hz, low-pass filtered, and sampled at 1500 Hz, and the measurements were wirelessly sent to a computer. The examinee stood comfortably and gazed forward, and the s-EMG was recorded for 3 s after the waveform had stabilized (Figure 1A). The integrated value of this EMG waveform for 3 s was calculated and used as the average value per second. To determine the maximal voluntary contraction (MVC) of these muscles, participants were asked to perform a maximal isometric movement against the resistance applied by the researcher (Figure 1B). We use a device that can immobilize the lower limbs and pelvis to evaluate the MVC of trunk muscles (Figure 1C). The average MVC value was an integrated value of .5 seconds before and after the maximum muscle activity (as per second). EMG waveform data was analyzed using the myoRESEARCH® 3 (Noraxon, Scottsdale, USA). The average muscle activity during 3 s in the resting standing position was calculated and normalized (%MVC) by the maximum isometric contraction of each muscle.14,15 We measured the values at the same site twice, and the average value was used as the measurement value. Surface electromyogram waveform and simultaneous photograph. (A). Resting standing position. (B). Maximum muscle activity of rectus femoris. The examiner manually applied an antagonistic force to the rectus femoris. Surface EMG shows a large waveform at the rectus femoris. (C). Maximum muscle activity of trunk muscles.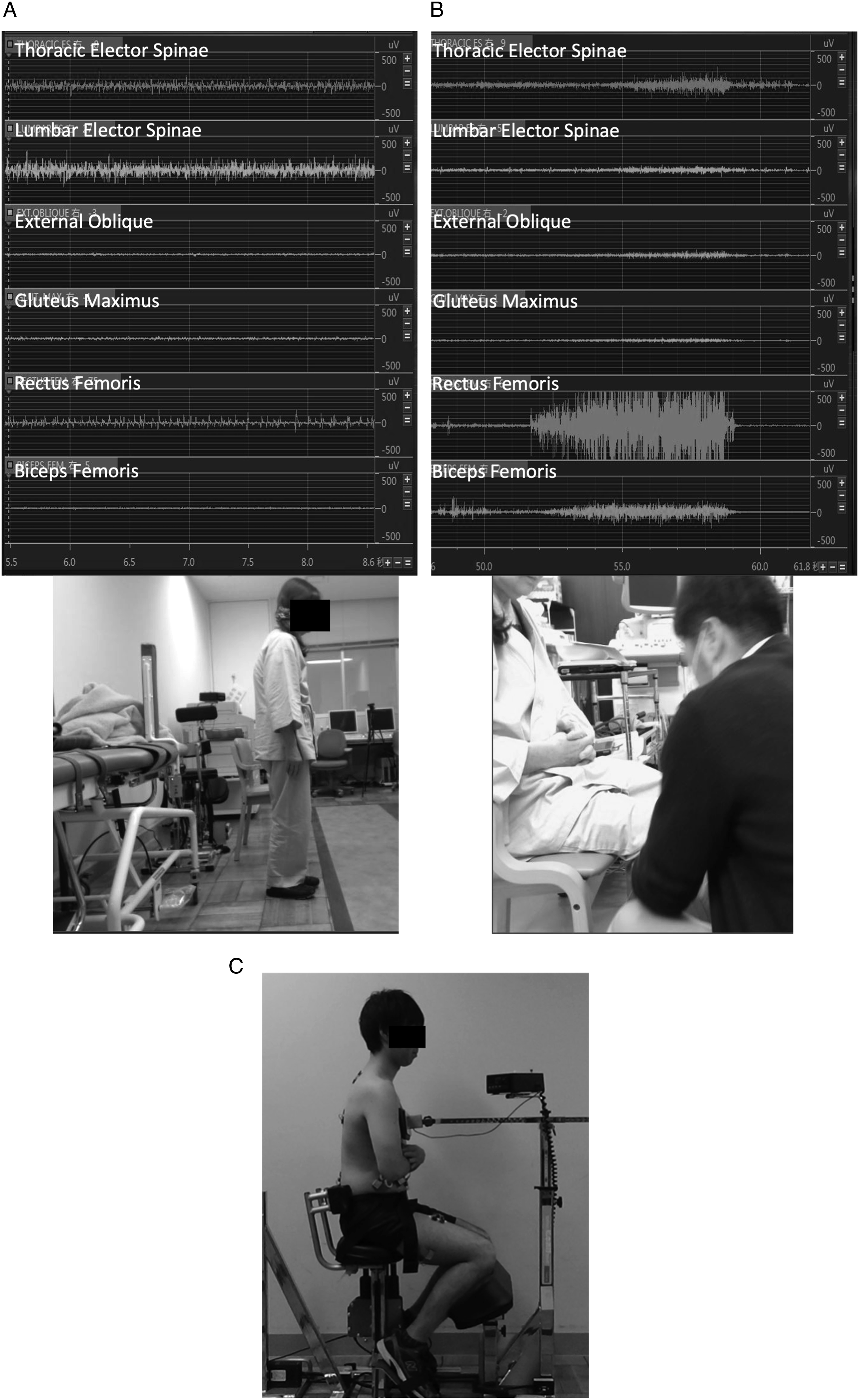
Definition of Compensatory Mechanisms
Types of Compensation
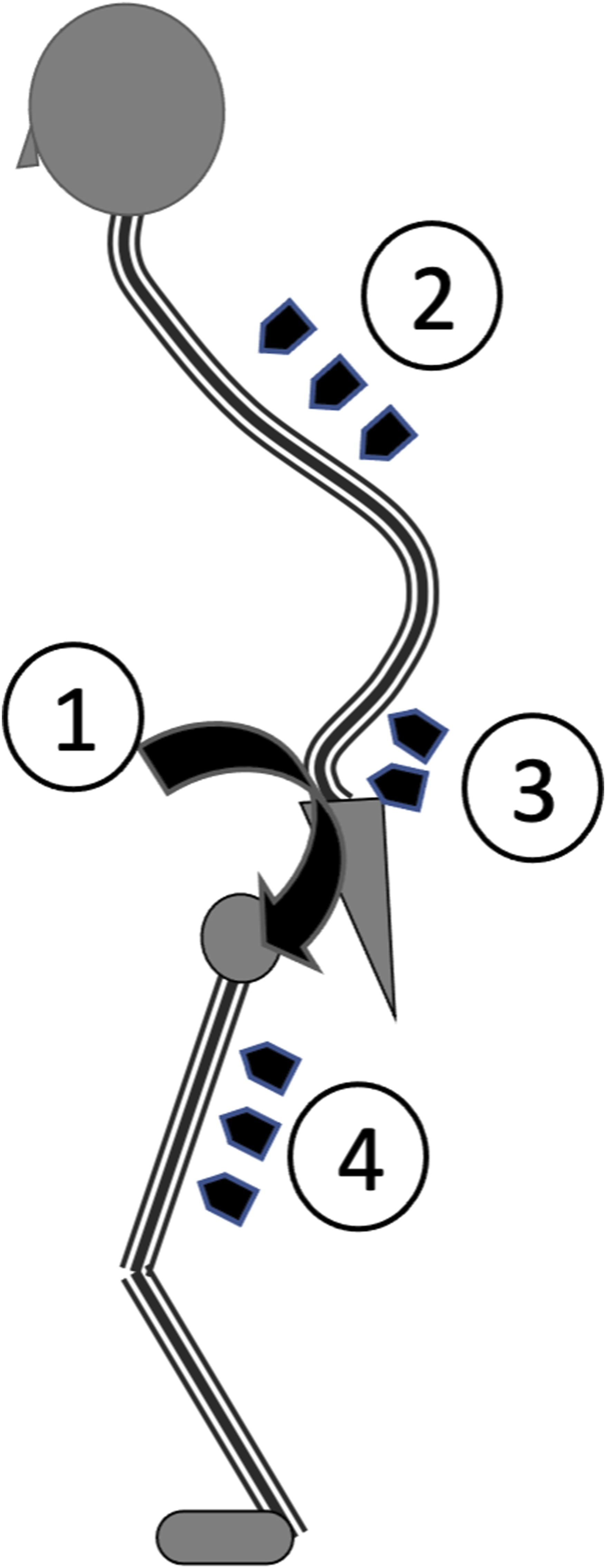
Substantial compensatory mechanisms have been reported to work against the poor sagittal alignment of the spine. However, previous reports have not clearly defined or provided cutoff values for each of the compensations. Among these, the following four representative alignments are defined to indicate compensation (Figure 2). 1. Pelvic retroversion (PT > 30°): Referring the sagittal modifiers of the SRS-Schwab classification.
16
2. Reduction of thoracic kyphosis (TK ≤ 10°): Referring to this definition in adolescent idiopathic scoliosis, a reduction of thoracic kyphosis was defined as TK ≤ 10°.
17
3. Hyperextension of the lumbosacral junction (L4/S lordosis ≥30°): Two-thirds of the LL is formed at L4/S, and the average LL of elderly volunteers is 40°–45°18,19 Considering the above, L4/S of 30° or more is considered to be an unusual pathological condition. 4. Knee flexion (FOA >10°): Referring to the report that preoperative FOA of 10 degrees or more is a factor for poor clinical and functional outcomes.
20
Illustration of the four types of compensation. 1. Pelvic retroversion, 2. reduction in thoracic kyphosis, 3. hyperextension of the lumbosacral junction; 4. knee flexion.
The muscle activities (%MVC) of each muscle were compared with or without compensation.
The Severity of Compensation and Imbalance
Barrey et al. and Hasegawa et al.4,21 classified the patients into three groups according to the severity of compensation. We also classified into three groups, referring the sagittal modifiers of SRS-Schwab classification,
16
with PT > 30° for compensation presence and SVA > 95 mm for global imbalance as follows: “Aligned”, SVA ≤ 95 mm and PT ≤ 30°; “Compensated”, SVA ≤ 95 mm and PT > 30°; and “Decompensated”, SVA>95 mm (Figure 3). Radiographic parameters and %MVC were compared among the three groups to identify differences in the trunk and lower extremities’ muscle activity depending on the degree of compensation. Classification of global alignment according to the severity of spinal compensation.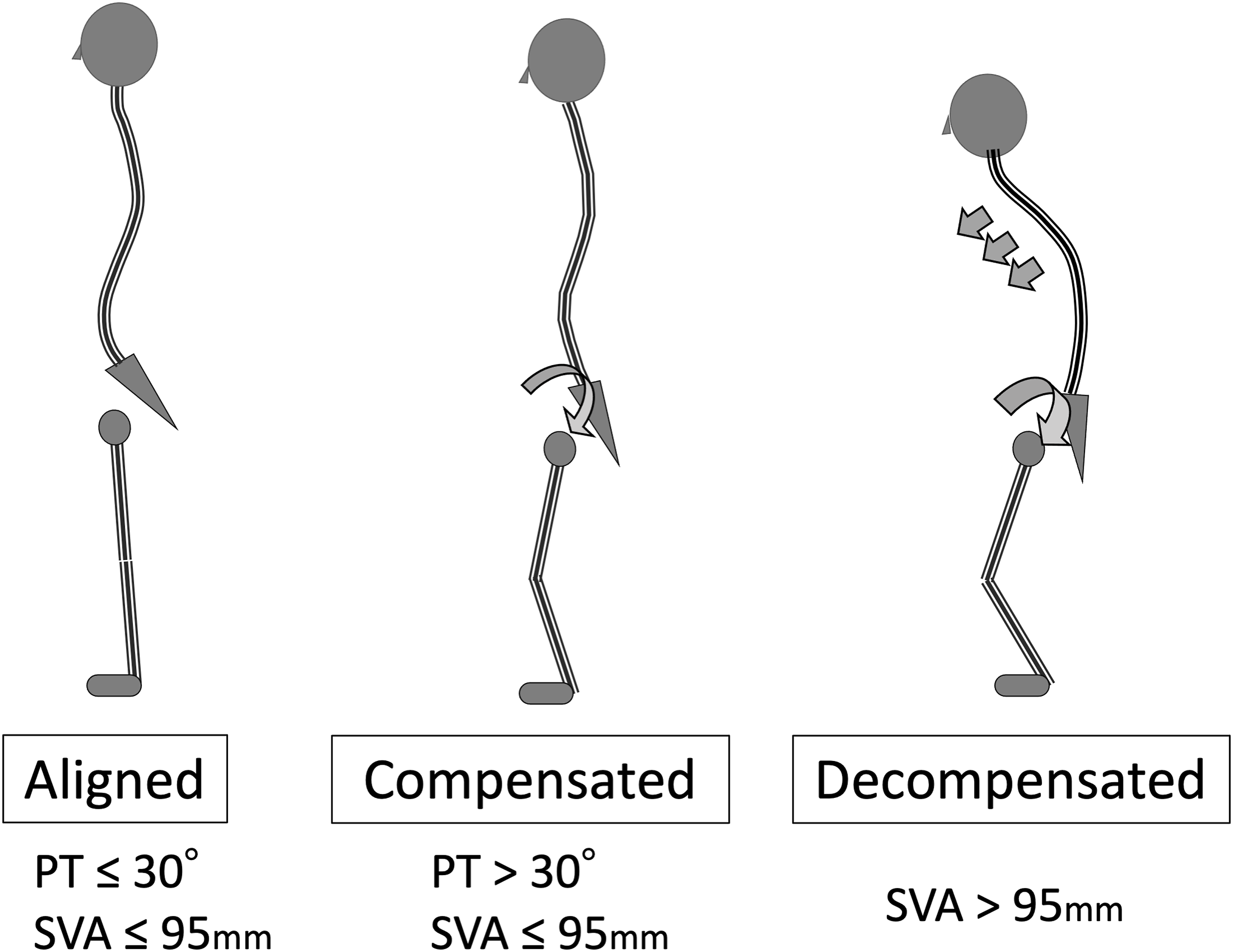
Statistical Analysis
Descriptive statistics, including means and standard deviations, were calculated for the demographic data. The Kolmogorov–Smirnov test was used to verify normality. Differences in %MVC with or without each compensation alignment were examined using unpaired t-tests. Differences in radiographic parameters and %MVC among the three compensation stages were analyzed using one-way analysis of variance, followed by Tukey’s post-hoc test. All statistical analyses were performed using EZR (Saitama Medical Center, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). More precisely, it is a modified version of R commander designed to add statistical functions frequently used in biostatistics. 22 A p-value <.05, was considered statistically significant.
Results
Demographics of patients.
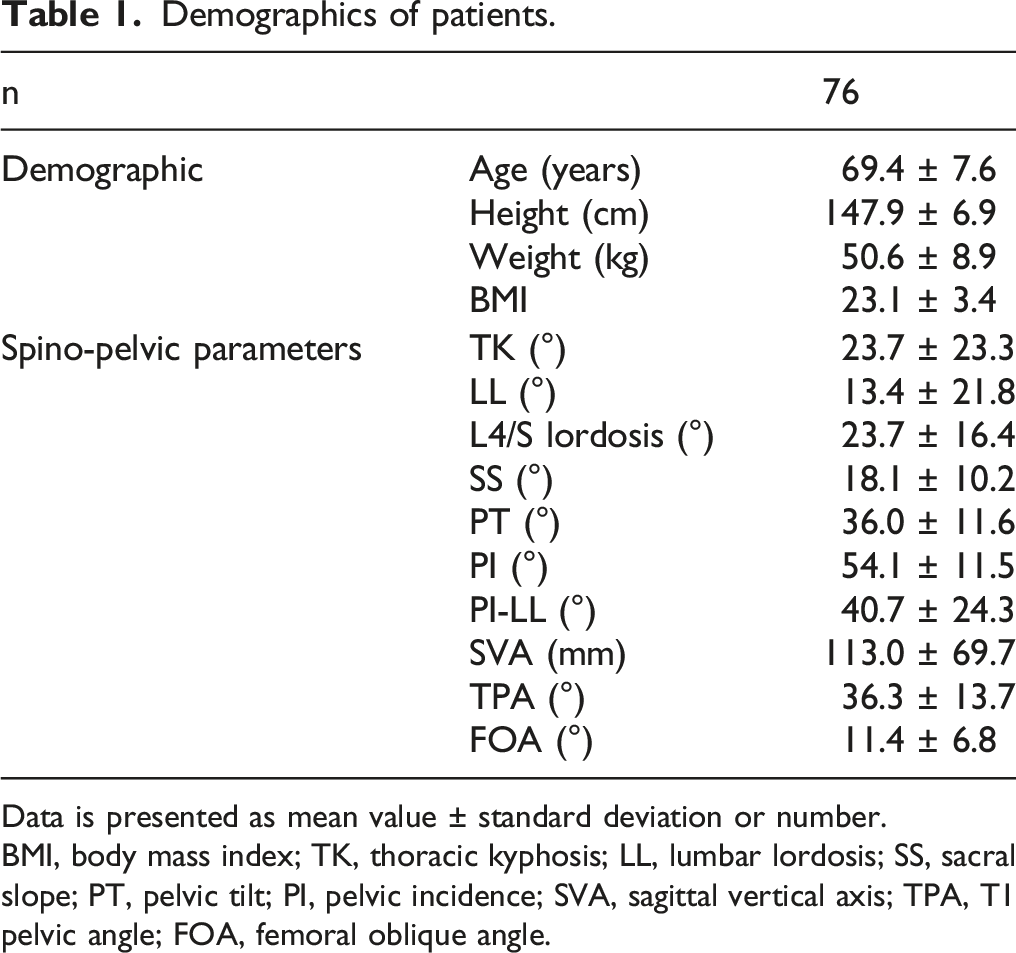
Data is presented as mean value ± standard deviation or number.
BMI, body mass index; TK, thoracic kyphosis; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence; SVA, sagittal vertical axis; TPA, T1 pelvic angle; FOA, femoral oblique angle.
Differences in Muscle Activity With and Without the Compensatory Status
1. Pelvic retroversion: PT > 30° (Figure 4A) Muscle activity with and without compensation box-and-whisker diagram. (A). Pelvic retroversion. (B). Reduction of thoracic kyphosis. (C). Hyperextension of lumbosacral junction. (D). Knee flexion.
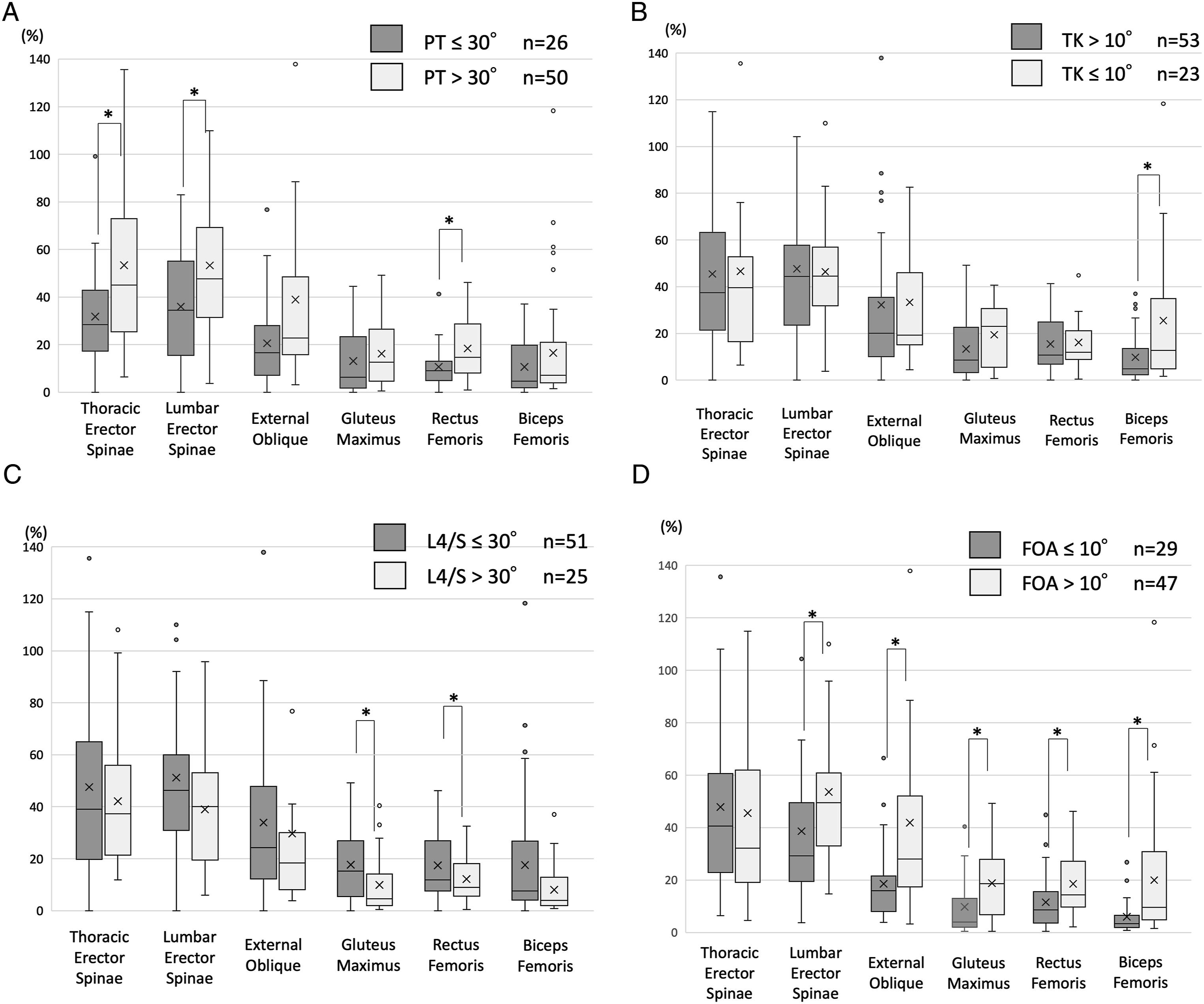
Pelvic retroversion was observed in 50 of the 76 patients. The mean %MVC of patients with pelvic retroversion was significantly higher in the TES, LES, and RF than those in the PT ≤ 30° groups: TES (mean ± SD) (PT > 30°; 53.4 ± 37.8, PT ≤ 30°; 33.1 ± 21.2), LES (53.3 ± 31.9, 37.4 ± 21.0), and RF (18.4 ± 12.5, 11.1 ± 8.7). 2. Reduction of Thoracic Kyphosis: TK ≤ 10° (Figure 4B)
A reduction in thoracic kyphosis was observed in 23 patients. There was no difference in the muscle activity of the trunk muscles with and without reduction of thoracic kyphosis, and only %MVC in the BF was significantly higher in the group with reduction of thoracic kyphosis: BF (TK ≤ 10°; 25.5 ± 29.2, TK > 10°; 10.0 ± 10.6). 3. Hyperextension of the lumbosacral junction: L4/S lordosis ≥30° (Figure 4C)
Hyperextension of the lumbosacral junction was observed in 25 patients. There was no apparent difference in trunk muscle activity between patients with and without this compensation. However, muscle activity in the lower limbs tended to be more significant in the hyperextension group: RF (L4/S ≥ 30°;12.2 ± 9.0, L4/S < 30°;17.8 ± 12.6), BF (8.0 ± 9.1, 17.9 ± 22.3), and GM (9.9 ± 11.1, 18.0 ± 13.5). 4. Knee Flexion: FOA > 10° (Figure 4D)
Knee flexion was observed in 47 patients. All muscle activities except TES were significantly higher in the FOA > 10° group than those in the FOA ≤ 10° group: LES (FOA > 10°; 53.6 ± 27.0, FOA ≤ 10°; 38.7 ± 31.5), EO (41.9 ± 44.6, 18.6 ± 14.5), RF (18.6 ± 11.9, 11.6 ± 10.5), BF (20.0 ± 22.7, 6.0 ± 6.5), and GM (18.8 ± 13.0, 9.8 ± 11.9).
Differences in Muscle Activity According to the Severity of Compensation and Imbalance
Radiographic parameters among three compensated stages.
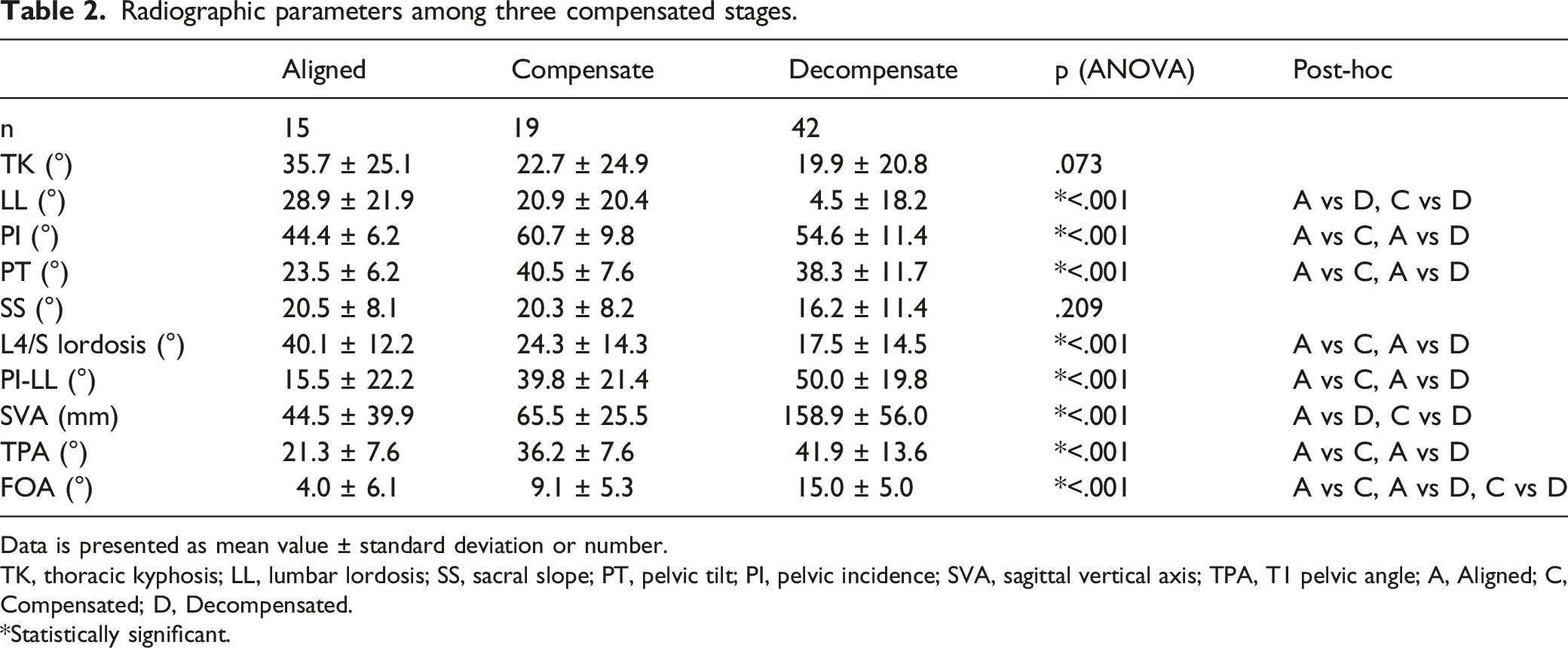
Data is presented as mean value ± standard deviation or number.
TK, thoracic kyphosis; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence; SVA, sagittal vertical axis; TPA, T1 pelvic angle; A, Aligned; C, Compensated; D, Decompensated.
*Statistically significant.
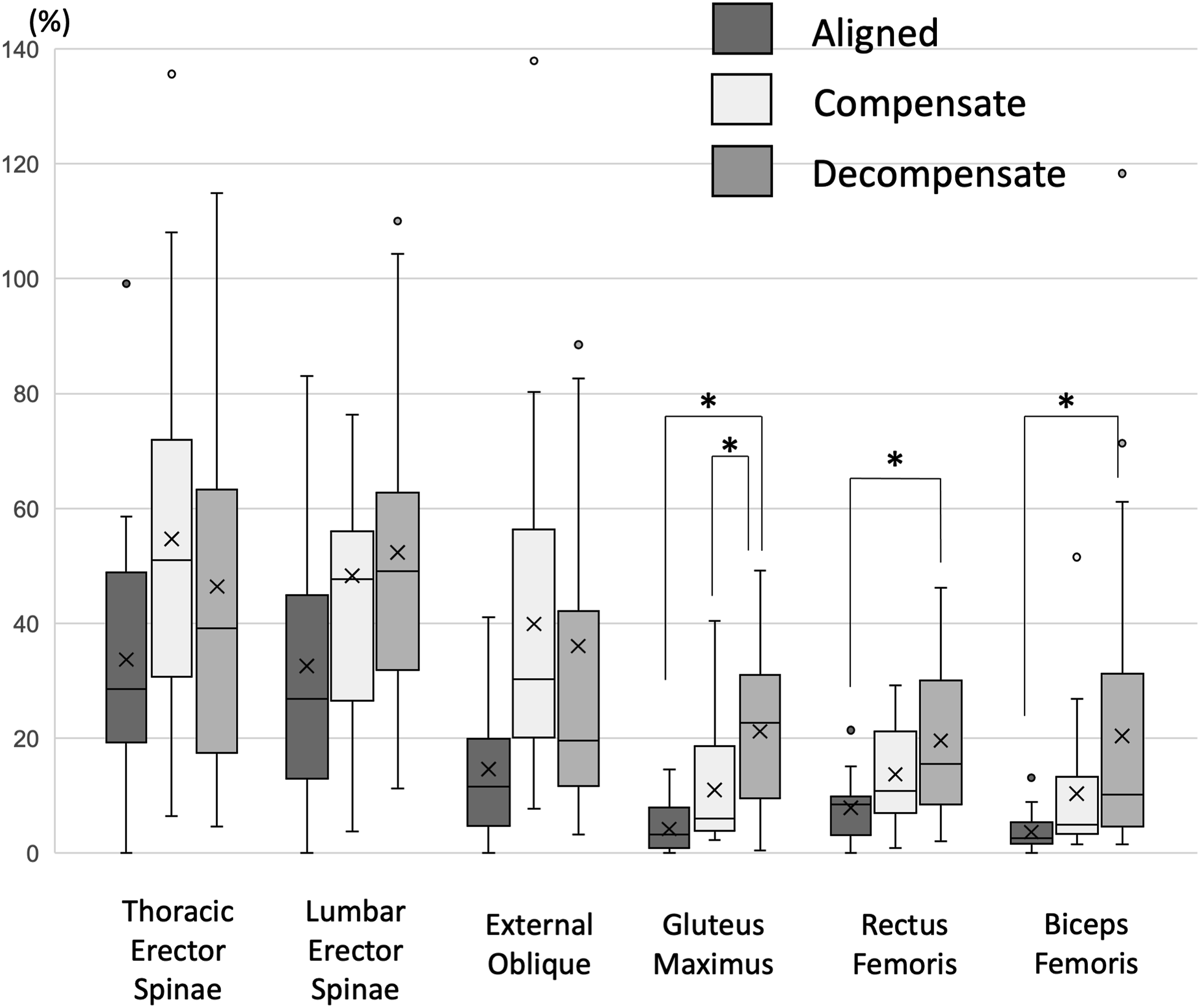
Muscle activity among three compensated stages. Box-and-whisker diagram.
Patient-reported outcome in three compensated stages.
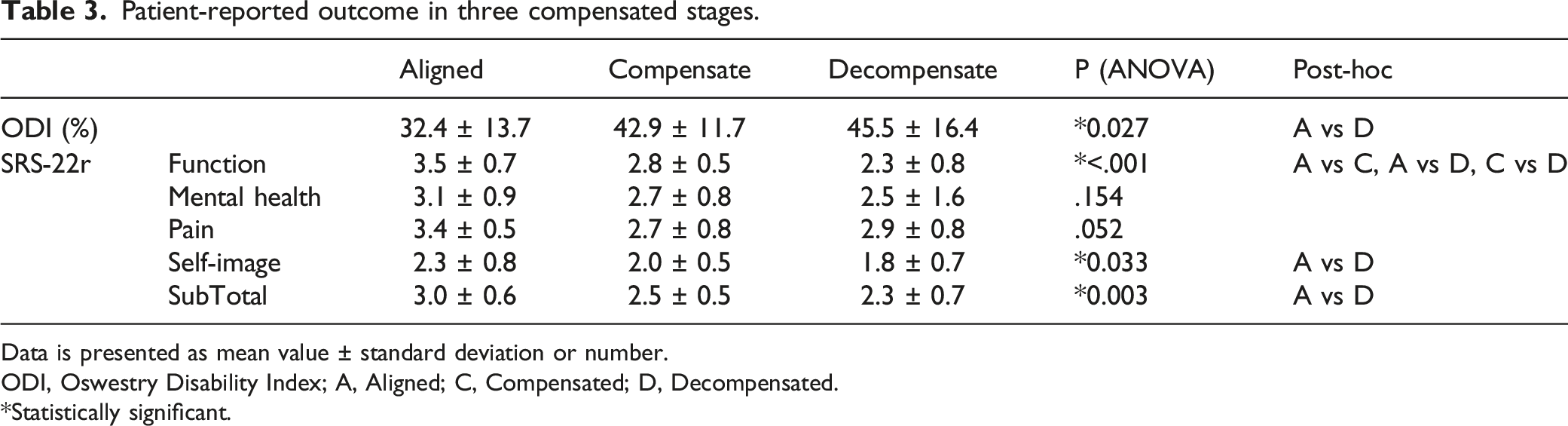
Data is presented as mean value ± standard deviation or number.
ODI, Oswestry Disability Index; A, Aligned; C, Compensated; D, Decompensated.
*Statistically significant.
Discussion
This study investigated which functional compensation status requires muscle contraction of the trunk, pelvis, and lower limbs in patients with spinal deformity. This report is the first to describe the real-time evaluation of muscle activity to maintain the standing posture using s-EMG, although various methods of muscle assessment have been reported. In studies that measured cross-sectional muscle area using CT or MR imaging, patients with spinal deformities had smaller cross-sectional regions of the extensor muscles.7,23,24 The cross-sectional muscle area of the multifidus and erector spinae muscles was found to be related to spinal pelvic sagittal plane alignment.6-8,25 MRI can also assess fatty infiltration within the muscle and, thus, evaluate the occurrence of fatty degeneration in the back muscles of patients with spinal deformity or degeneration.23,26 However, the assessment of muscle area on these images is a morphological assessment in the supine position. Some studies27-29 have assessed trunk extensor strength and reported that trunk extensor strength correlates with lumbar lordosis or PROs.
The use of EMG allowed us to evaluate the muscle in real time.15,25 Using s-EMG, Enomoto et al. 10 revealed that patients with thoracolumbar kyphosis had significantly increased muscle activity in the lower back in the resting standing position and increased severe muscle fatigue in the upper lumbar spine. We determined four compensations based on standing sagittal alignment in the whole spine radiograph and examined the differences in real-time muscle activity with and without these compensations. Our results demonstrated that pelvic retroversion and knee flexion were compensations that required trunk muscle activity. In contrast, reduction of thoracic kyphosis and hyperextension of the lumbosacral junction were compensations that did not require much trunk muscle activity. Barrey et al.3,4 described compensatory mechanisms in the spine, pelvis, and/or lower limb. Reduction of thoracic kyphosis and hyperextension of the lumbosacral junction were found to be the regional compensations for extension adjacent to the region with malalignment. Barrey et al. also reported that the value of PI affects the severity and compensation of the deformity.3,4 In this study, PT and PI were not different between “compensated” and “decompensated” groups. This is due to the definition of the three groups using parameters in this study. In contrast, pelvic retroversion and knee flexion involve extra-spinal compensation. Regional spinal compensation requires less muscle activity because the spinal alignment itself is altered and stabilized, and from the perspective of muscle activity, it is an economical compensation. However, extra-spinal compensation requires significant muscle activity in the trunk and lower limbs to support malalignment.
In recent years, several reports have described the use of full-standing axis stereography to evaluate the alignment of the whole body and describe compensation.5,21,30,31 Hasegawa et al. 21 classified spinal deformities into three categories: normal, compensated, and decompensated, with the decompensated stage being the non-economical stage. Jalai et al. 31 revealed that more severe sagittal deformities required differential recruitment of lower limb extension, which varied significantly with age. Diebo et al. 5 discussed the recruitment of compensation for sagittal spinal malalignment. As the PI-LL mismatch increased, the TK and PT contributions to the compensation cascade decreased, and the knee flexion angle and pelvic shift contribution increased. Pelvic retroversion and flattening of the TK got exhausted with an increasing mismatch. At that point, there has seemed to be a steady transfer of compensation toward significant participation of the lower limb.
In this study, we examined the severity and compensation of spinal deformities in muscle activity rather than alignment. There was a difference in the muscle activity of the pelvis and lower limbs according to the severity of the deformity. The more severe the deformity, the more muscle activity of the pelvis and lower limb was required to maintain the standing position. This result indicates that patients with severe deformity and sagittal decompensation cannot maintain an upright posture without muscle strength in the lower limbs, and muscle training from the pelvis to the lower limbs and joint function improvement may help maintain ADL. The function domain of SRS-22r also worsened in the order of aligned, compensated, and decompensated, suggesting that compensated and decompensated dysfunction was more evident than the domains of mental health and pain. Functional impairment can be particularly pronounced because of the immense load on the muscles that are contributing to compensations.
Several authors have reported the relationship between sagittal spinal deformity and posture and muscle fatigue. 32 Abboud et al. 9 indicated that combined muscle fatigue and creep deformation of spinal tissues lead to increases in muscle activity amplitude, as well as increases in muscle activity distribution. Bae et al. 33 postulated that the loss of compensatory mechanisms is due to fatigue of the pelvic and spinal extensor muscles after patients walk for 10 minutes. The extended walking unmasked any hidden sagittal imbalance in compensated deformities. In this study, trunk muscle activity increased in extra-spinal compensations, such as knee flexion and pelvic anteversion. This may be related to the fact that spinal deformations in the sagittal plane produce muscle fatigue and the creep phenomenon. In this study, the pain score of the SRS-22r was not correlated with the status of compensation. The pain domain in the SRS-22r may not reflect pain with muscle fatigue and was not compared directly with muscle activity.
This study has several limitations, including a single-center setting, small number of patients, small number of evaluated muscles due to equipment limitations, lack of age-adjusted controls, and no assessment of contractures in hip and knee joint. The PI affects the severity and compensation of the deformity.3,4 However, it is difficult to determine the threshold of compensation in each parameter according to the value of PI, because the decisive factors that determine the threshold of compensation have not been clearly defined. This is one of significant limitations of our study. Moreover, we used the normalization method using MVC as a reference, which is difficult to measure accurately in elderly patients with spinal deformities. Although this method may not be suitable for the elderly, we adapted it because it is widely used.14,15 Another limitation is that this study did not evaluate muscle strength itself, so it is unclear how much muscle output was being produced. However, it was useful to evaluate the muscle activity required to compensate for the spinal deformity in real time.
Conclusions
Many compensatory mechanisms are involved in the sagittal malalignment of the spine. In terms of muscle activity, regional alignment changes for compensation are economical in the adjacent spine. However, compensations outside the spine, such as pelvic retroversion and knee flexion, are non-economical. According to compensation recruitment, the muscle activity of the pelvis and lower limbs increased with the severity of the spinal deformity.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Ms. Nao Kuwahara, Tomoe Mabuchi and Mrs. Taku Nagao and Tomokazu Suzuki, secretaries in the Department of Orthopedic Surgery, for their excellent contribution in data collection. The authors also would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Yu Yamato and Shin Oe work at a donation-endowed laboratory and are funded Medtronic Sofamor Danek Inc., Japan Medical Dynamic Marketing Inc., and Meitoku Medical Institution Jyuzen Memorial Hospital. For the remaining authors, none were declared. The manuscript submitted does not contain information about medical device(s)/drug(s).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Funding sources of Yu Yamato and Shin Oe Medtronic Sofamor Danek Inc., Japan Medical Dynamic Marketing Inc., and Meitoku Medical Institution Jyuzen Memorial Hospital.
Data Availability
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Ethical Approval
This study was approved by the institutional review board of Hamamatsu University School of Medicine (approval number 15-284).
Informed consent
Written informed consent was obtained from all participants.