
Abstract
Study Design
Retrospective Cohort Study
Objective
To evaluate the accuracy of intraoperatively measured computed tomography (CT) Hounsfield unit (HU) values by comparison with preoperative CT HU values and to compare the radiation exposure between preoperative and intraoperative CT scans.
Methods
HU values of lumbar vertebrae were measured and compared between preoperative and intraoperative CT scans in patients undergoing lumbar interbody fusion. In patient group one, Canon CT scanners were used preoperatively and the AIRO CT scanner was used intraoperatively. In patient group two, Canon CT scanners were used preoperatively and the O-arm Cone Beam CT (CBCT) scanner was used intraoperatively. In a subgroup analysis of patient group one, radiation by means of CT Dose Index (CTDI) was compared between Canon and AIRO CT scanners.
Results
In the first patient group, a total of 250 vertebrae were analysed in 74 patients showing a strong Pearson correlation of >.94 between pre- and intraoperative HU values. Bland-Altman analysis indicated consistency and equivalence with a bias of 3.9 and 95% limits of agreement from −27.17 to 34.97 when comparing all pre- and intraoperative HU values of L1–5. In the second patient group, a total of 27 vertebrae were analysed in 10 patients showing weak Pearson correlation and Bland-Altman analysis indicated no equivalence. CTDI did not differ between Canon and AIRO CT scanners.
Conclusion
Correct and reliable CT HU measurement as mandatory key factor for the intraoperative assessment of bone quality and robotic-assisted surgery is feasible with intraoperative AIRO CT imaging without increase of radiation exposure.
Keywords
Introduction
The assessment of bone quality in the course of surgical lumbar interbody fusion is crucial, as alterations of the bone mineral density (BMD) due to diseases such as osteoporosis is an important risk factor for postoperative complications. When defined as implant pull-out in patients who underwent posterior spinal fusion, the prevalence of screw loosening was 9.6% (95% CI 5.6–15) with osteoporosis representing a significant risk factor (OR 7.49). 1 Osteoporosis is characterized by low bone mass, microarchitectural deterioration of bone tissue leading to enhanced bone fragility and a consequent increase in fracture risk. 2 Osteoporosis has become a global public health problem and the incidence of osteoporosis among patients aged ≥50 years undergoing lumbar fusion for lumbar degenerative diseases was reported to be 39.7% with higher prevalence in females than males (48.9% vs 27.1%). 3 In the last decades, the gold standard for diagnosing osteoporosis has been the dual-energy X-ray absorptiometry (DXA). However, because sclerotic lesions, scoliosis, spinal degeneration and abdominal aortic calcification can lead to an overestimation of BMD by DXA,4-6 new methods for the determination of BMD have been described. In recent years, assessing BMD by analysing Hounsfield unit (HU) measurements in computed tomography (CT) images as a complementary method has been proposed. By evaluating the BMD with CT HU values, above-mentioned disadvantages of DXA can be avoided. CT HU values strongly correlate with DXA BMD values and different CT HU thresholds for the diagnosis of osteoporosis in the lumbar spine have been proposed.7-16 The measurement of CT HU values is reliable, with excellent intra- and interobserver reliability. 9 HU measurements correlate with future osteoporotic fracture risk, 17 adjacent segment fractures after spinal fusion, 18 cage subsidence after transforaminal lumbar interbody fusion (TLIF), 19 pedicle screw loosening,20-22 symptomatic pseudarthrosis after posterolateral 23 and proximal junctional failure after posterior lumbar fusion. 24 When facing lowered bone quality in patients, the surgeon can anticipate osteoporosis-related complications by increasing the diameter and length of the screws, bi- or multi-cortical purchase, purposeful breach, cement augmentation of screws and others. 25 Thus, correct HU measurement is mandatory when assessing bone quality and CT HU values can make the best use of CT images at no extra cost since lumbar CT imaging is often a routine examination prior to spinal surgery. But if valid CT HU values could be determined intraoperatively when scanning for e.g. robotic (-assisted) surgical procedures, these values could be used to assess bone quality instead of the preoperative ones.
Subject
The aim of this study was to evaluate the use and accuracy of intraoperatively measured CT HU values in patients undergoing lumbar interbody fusion by comparison with preoperative CT HU values and to compare the radiation exposure between these preoperative and intraoperative CT scans.
In addition to the assessment of bone quality, correct intraoperative measurement of HU values has high relevance for robotic (-assisted) surgical procedures. CT-navigated screw implantation provides high accuracy and safety in spinal instrumentation26-29 and thus gains widespread application. Robotic (-assisted) surgical procedures based on computed tomography use complex image processing techniques based on artificial intelligence and machine learning applications to correctly plan and place screws in spinal surgery. However, bone must be automatically and reliably identified and entry points as well as trajectories must be planned precisely. For this purpose, an orientation according to structures with specific HU values appears essential. Therefore, intraoperative CT HUs must be measured correctly, which has not been analysed before.
Summarized, the measurement of CT HU values is a simple, rapid and reliable method 9 to assess bone quality and precise intraoperative CT HU measurement is mandatory for robotic (-assisted) surgical procedures. However, the accuracy of intraoperatively measured CT HU values for the purpose of addressing both of the above-mentioned subjects within one scan has not been analysed yet. Therefore, the aim of this study was to evaluate the hypothesis of accurate intraoperative CT HU measurement in patients undergoing lumbar interbody fusion by correlation analyses and Bland-Altman plots of preoperative and intraoperative CT HU values as main objective and to compare the radiation exposure between these preoperative and intraoperative CT scans as secondary objective.
Design and Methods
Patient Cohort
The study was approved by the ethics committee of the Charité – Universitätsmedizin Berlin, Germany (EA4/046/16). This study included patients who underwent lumbar interbody fusion at the Department of Neurosurgery at the Charité – Universitätsmedizin Berlin because of lumbar degenerative diseases, tumours, spondylodiscitis or spinal trauma. Informed consent was waived due to the retrospective nature of the study. Between the 01.01.2019 and 31.12.2020, 407 patients underwent lumbar interbody fusion for the above-mentioned indications. Out of these patients, two main patient groups were formed for this study: Patient group one included patients in which Canon CT scanners were used preoperatively and the mobile AIRO CT scanner was used intraoperatively. Patient group two included patients in which Canon CT scanners were used preoperatively and Cone Beam CT (CBCT) using the O-arm scanner was used intraoperatively. Patients with pre-instrumented vertebrae were excluded. Only unenhanced CT scans with pre-defined protocols focussing on the lumbar spine were included, see below. CT HU values of lumbar vertebral bodies were measured, analysed and compared between preoperative and intraoperative scans.
The first patient group included 74 patients who met the inclusion criteria. The mean age was 65.38 ± 12.28 years (range 29–89 years), including 36 women and 38 men. The mean age was 64.67 ± 11.45 years (range 29–83 years) in the female subgroup and 66.05 ± 13.14 years (range 35–89 years) in the male subgroup. The age difference between these subgroups was not significant (p = .6308).
The second patient group included 10 patients who met the inclusion criteria. The mean age was 70.4 ± 10.56 years (range 47–80 years), including five women and five men. The mean age was 70.2 ± 14.2 years (range 47–80 years) in the female subgroup and 70.6 ± 7.021 years (range 63–79 years) in the male subgroup. The age difference between these subgroups was not significant (p = .9564).
CT-Scanning
All subjects of patient group one and two underwent a preoperative CT scan at the Department of Neuroradiology at the Charité – Universitätsmedizin Berlin with a mean interval ± standard deviation (SD) of 6.47 ± 9.89 days (range 1–45 days) before the operation. Patients with pre-instrumented vertebrae were excluded. Only unenhanced CT scans with pre-defined protocols focussing on the lumbar spine were included. This preoperative CT examination was performed using a Canon CT Aquilion PRIME/ONE (Canon Medical Systems Corporation, Otawara, Tochigi, Japan. According to the producer, HU values and radiation doses are comparable between Aquilion PRIME and ONE, thus values were pooled). All Canon devices were calibrated on a regular basis to ensure accuracy. The CT scan was performed following the standardized breathing instructions with the following parameters: tube voltage: 100–135 kVp, tube rotation time: 0.5 s and scanning slice thickness: 1 mm. Intraoperatively, patients of group one underwent unenhanced CT scans and patients of group two underwent unenhanced CBCT scans at the department of Neurosurgery at the Charité – Universitätsmedizin Berlin. Of the intraoperative images, only the scan before screw implantation was analysed. Intraoperative CT in patient group one was performed using the AIRO Mobile CT scanner (Mobius Imaging, Shirley, MA, USA). The AIRO CT device was calibrated on a regular basis to ensure accuracy. The CT scan was performed under apnoea following pre-oxygenation to reduce motion artefacts with the following parameters: tube voltage: 120 kVp, tube rotation time: 0.8 s and scanning slice thickness: 1 mm. Intraoperative CBCT examination in patient group two was performed using the O-arm scanner (Medtronic Inc., Louisville, CO, USA). The CBCT scan was performed under apnoea following pre-oxygenation to reduce motion artefacts with the following parameters: tube voltage: 120 kVp, tube rotation time: 1.92 s and scanning slice thickness: 1 mm. CT images were transferred to the Phönix-PACS MERLIN Diagnostic Workcenter software to evaluate HU values.
Bone Density Evaluation (HU Measurement)
Phönix-PACS MERLIN Diagnostic Workcenter software was used to determine HU values. The type of CT window did not change the HU value. 1mm slices were analysed. CT HU values of each vertebrae were measured by placing an oval region of interest (ROI) over an axial image of the middle of the vertebral bodies L1-5 (Figure 1). When an oval ROI was placed, Phönix-PACS MERLIN Diagnostic Workcenter software automatically calculates the mean CT HU of this ROI. If the vertebral body was scanned at an angle, the cutting plane was aligned horizontally to the vertebral endplates. The ROI had to include as much trabecular bone as possible. Cortical bone and heterogeneous areas, such as bone islands, posterior venous plexus and compressed bone were avoided. Vertebrae that were found to be the focus of degeneration/tumor/infection/trauma were excluded and values were only included if pairwise intraoperative and preoperative values per vertebra were available. CT scan of the lumbar spine with demonstration of HU measurement in the sagittal (left) and axial (right) plane using an oval region of interest (ROI). When an oval ROI is placed, Phönix-PACS MERLIN Diagnostic Workcenter software automatically calculates the mean CT HU for this ROI.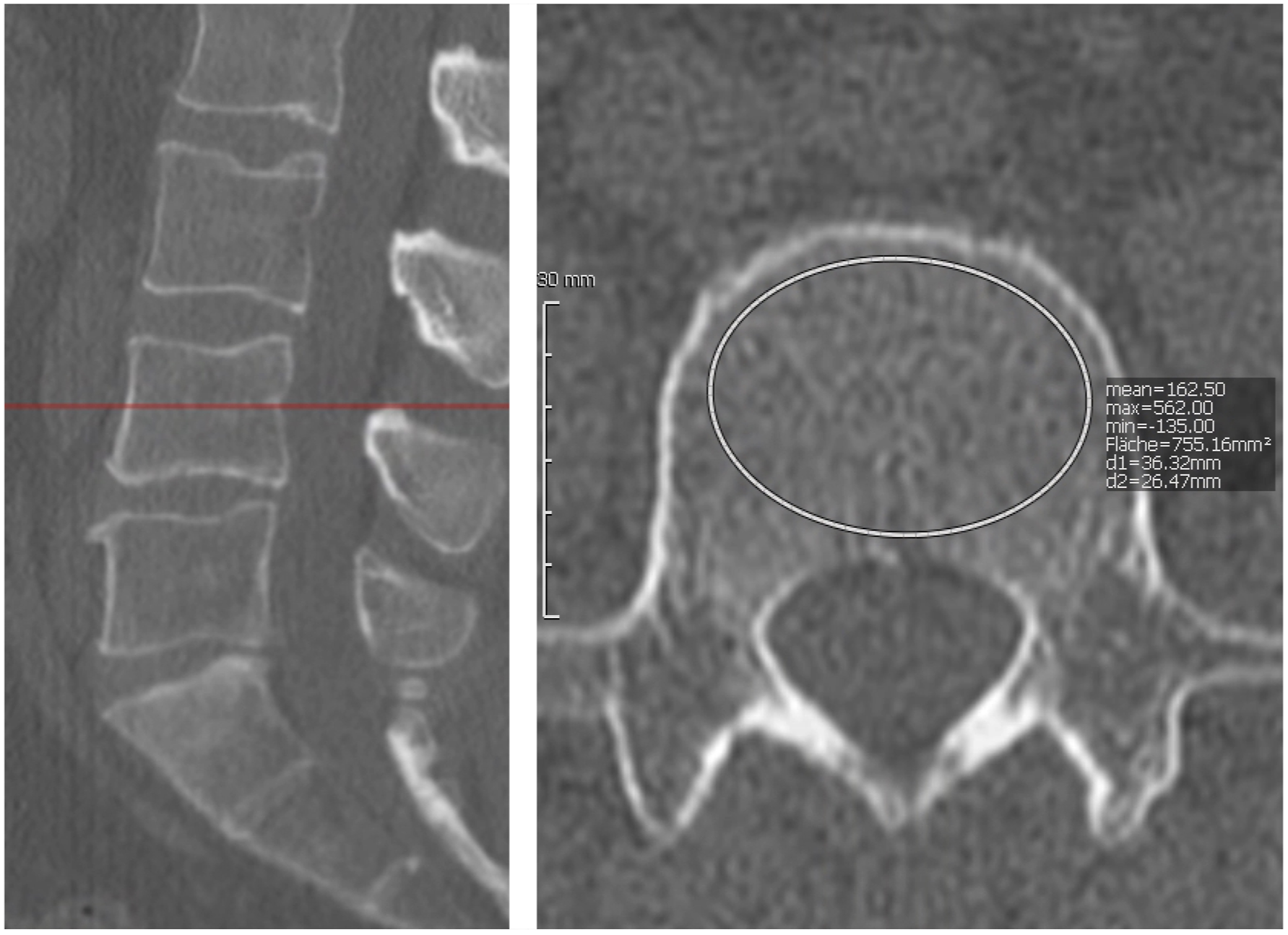
Radiation Dose
CT Dose Index (CTDI) values were analysed and compared in a subgroup analysis including all 35 patients of the first patient group (35 of 74 patients) who underwent surgery between the 01.01.2020 and 31.12.2020. After imaging, CTDI values were automatically transferred to the Phönix-PACS MERLIN Diagnostic Workcenter software and then used for further analyses.
Statistical Analysis
IBM SPSS statistical software version 27.0 and GraphPad Prism version 9.0 were used for statistical analyses and graphs, and P values less than .05 were considered statistically significant. Descriptive statistics of the patient groups were presented as proportions for categorical variables and means plus standard deviations for continuous variables. Shapiro–Wilk test and Anderson–Darling test were used as normality tests. Age differences were analysed using an unpaired t-test as the values passed normality tests. The correlation between preoperative CT HU values and intraoperative CT HU values was analysed by Pearson correlation coefficient. Bland-Altman plots were applied to compare the consistency and equivalence of CT HU values measured pre- and intraoperatively, whereby the bias was computed as average of the differences between the HU values determined by preoperative CT minus the HU values determined by the intraoperative CT. The 95% limits of agreement were computed as the mean difference (bias) plus or minus 1.96 times its standard deviation. To compare CTDI values between pre- and intraoperative CT, Wilcoxon test was performed as the values did not pass normality tests.
Results
Correlation and Consistency of HU Values
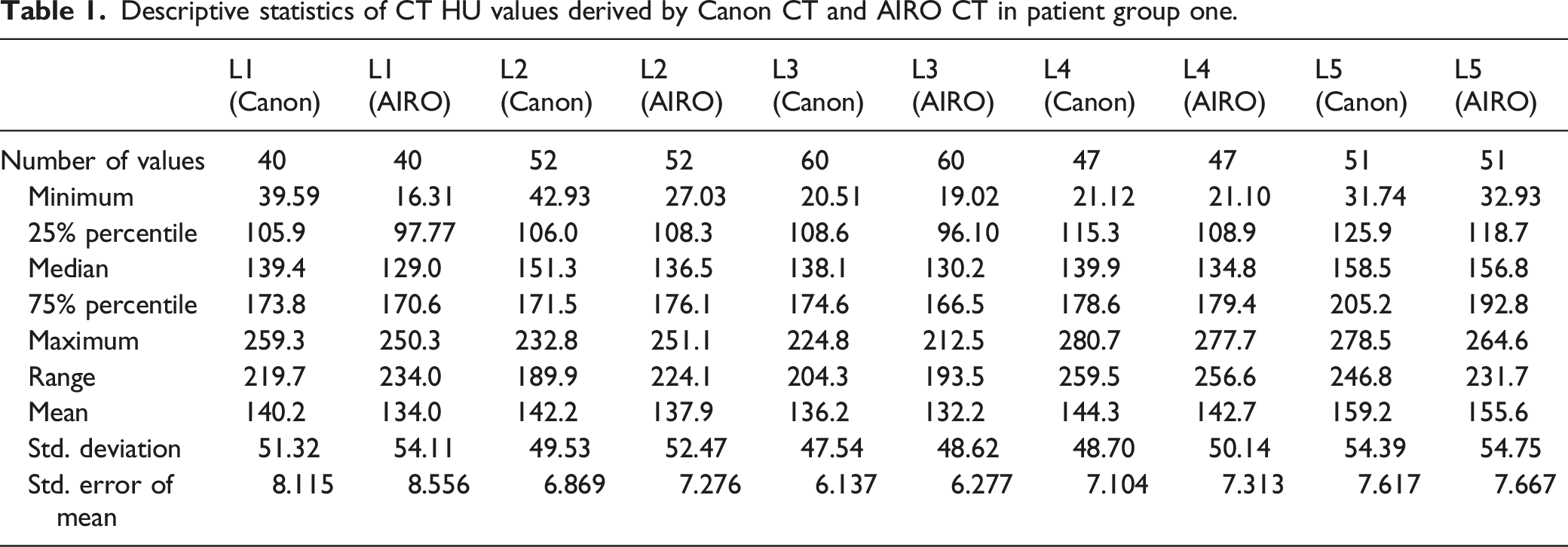
Descriptive statistics of CT HU values derived by Canon CT and AIRO CT in patient group one.
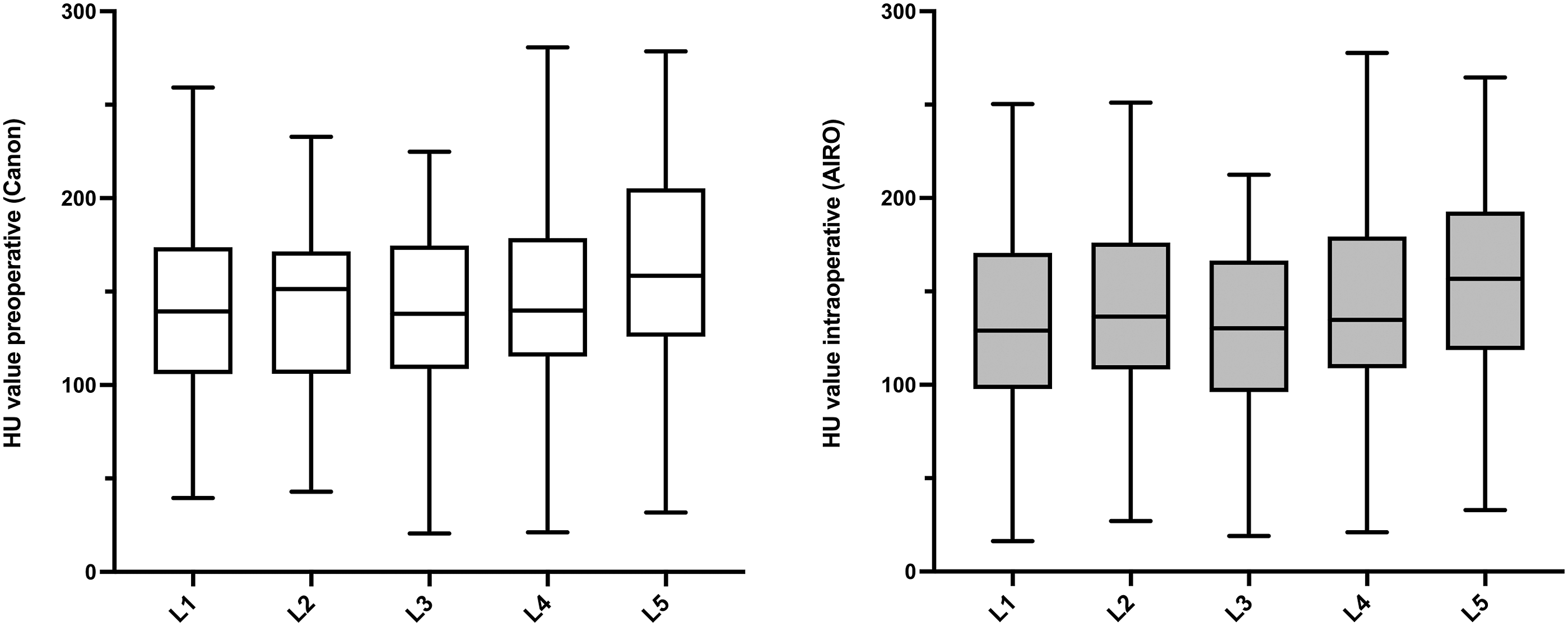
CT HU values of L1–5 in patient group one, shown as box and whiskers (box extends from the 25th to 75th percentiles, the line in the middle of the box is plotted at the median. Whiskers represent minimum and maximum). CT HU values showed an increase from the cranial to the caudal lumbar vertebrae in both preoperative Canon (left) and intraoperative AIRO (right) CT imaging. L1: n = 40; L2: n = 52; L3: n = 60; L4: n = 47; L5: n = 51.
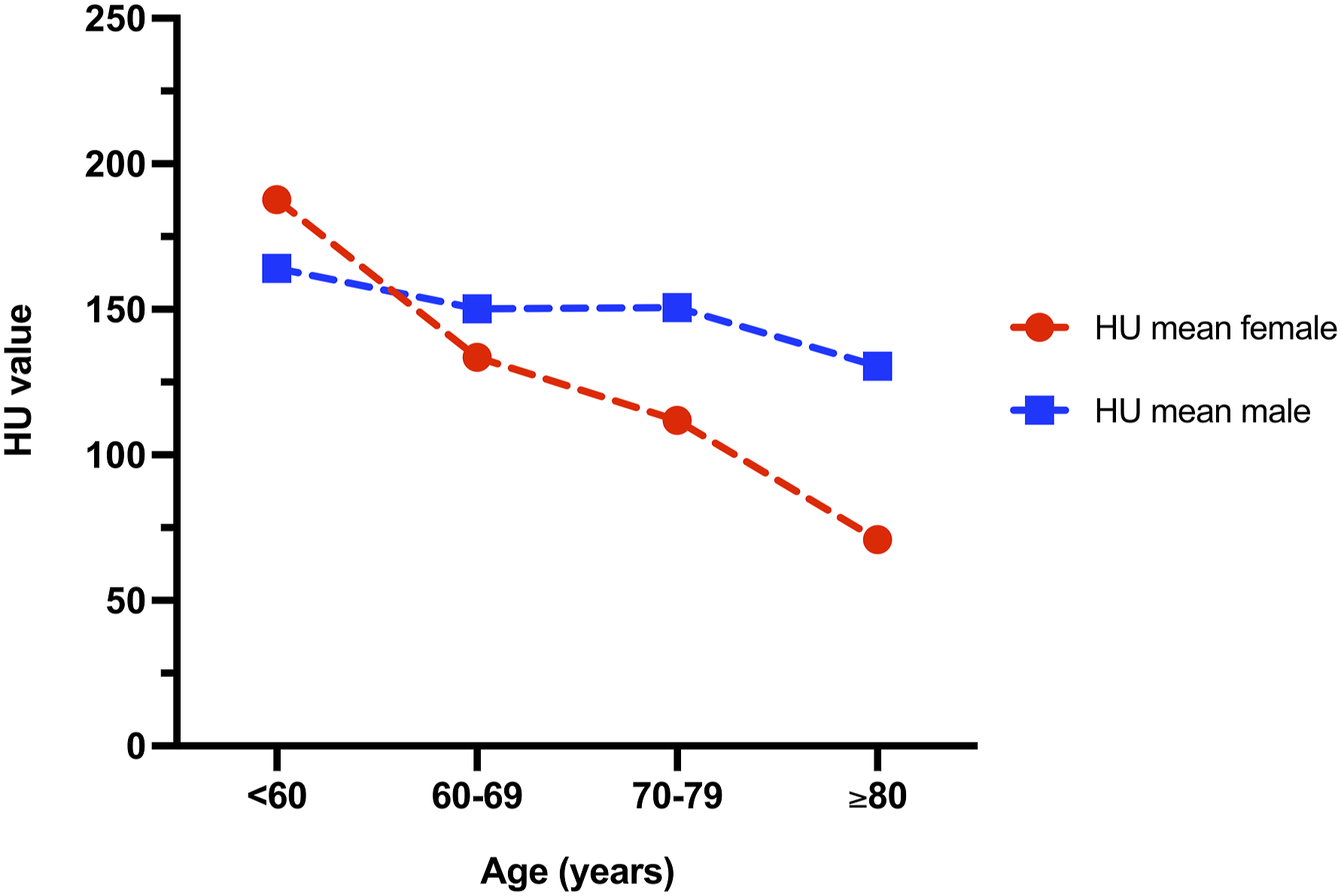
HU values changed with age in males and females (mean intraoperative AIRO CT HU values of all vertebrae per person of patient group one were calculated. Plot shows mean of these values per age group).
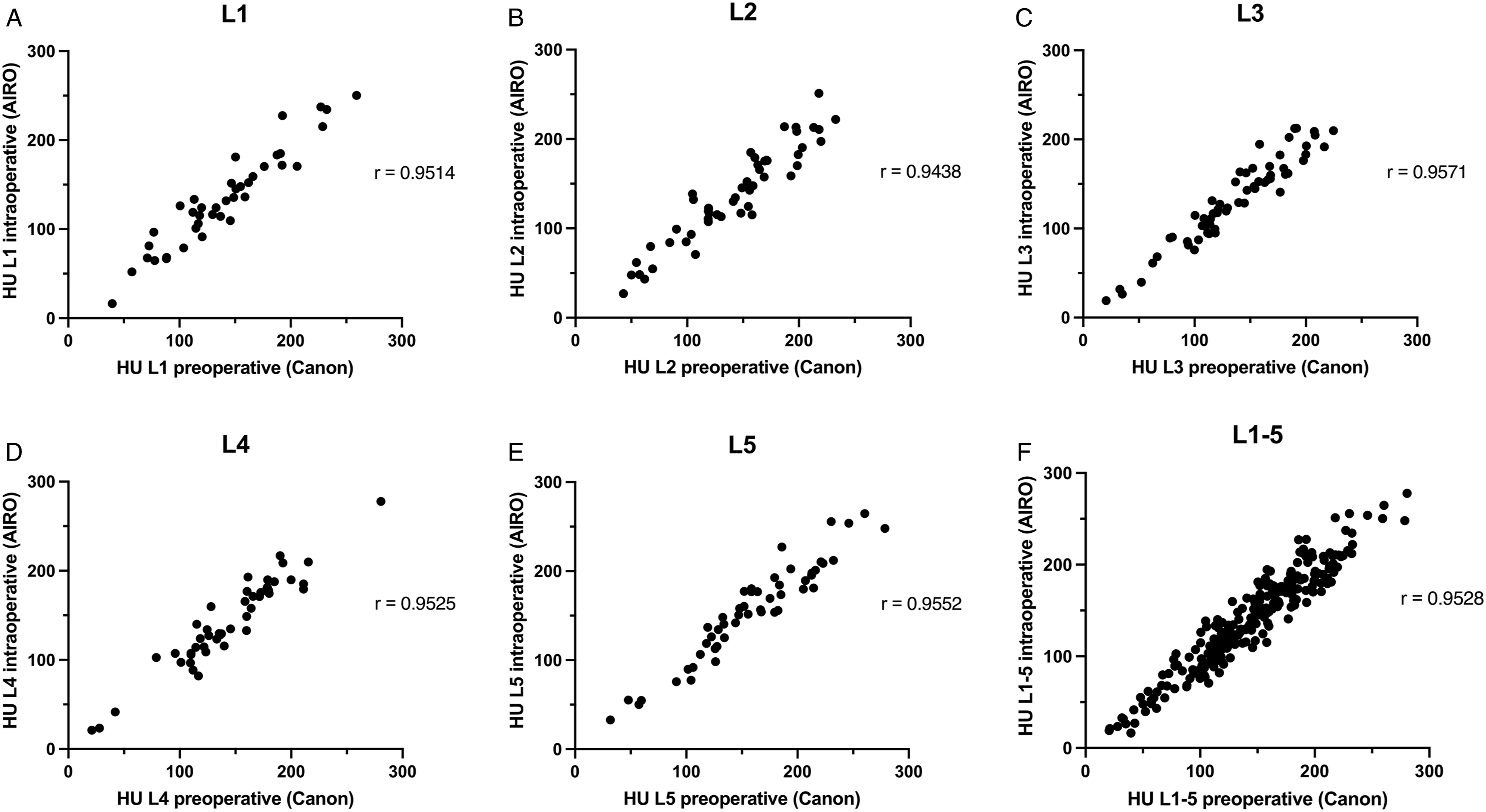
Intraoperative (AIRO) and preoperative (Canon) CT HU values showed statistically significant positive Pearson correlation with a correlation coefficient r of .9514 in L1 (A; n = 40), .9438 in L2 (B; n = 52), .9571 in L3 (C; n = 60), .9525 in L4 (D; n = 47) and .9552 in L5 (E; n = 51) when values were analysed for each vertebra separately and .9528 (F; n = 250) when all values (L1–L5) were compared together. P was <.0001 for all vertebrae.
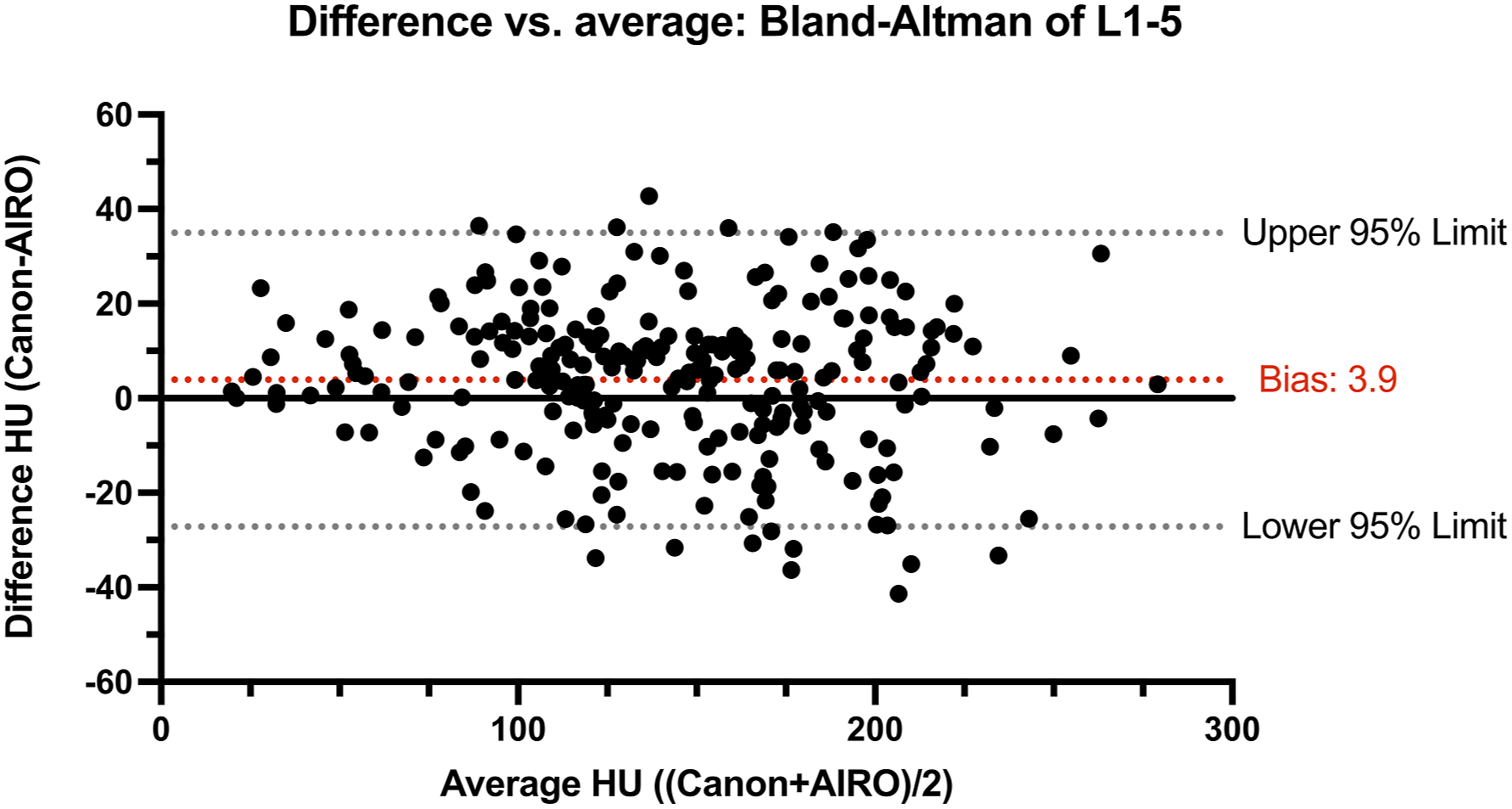
Difference (HU values of Canon-AIRO) vs average (HU values of ((Canon+AIRO)/2)): Bland-Altman plot of Canon and AIRO indicated consistency between the two measurements with a bias of 3.9 and a 95% limit of agreement from –27.17 to 34.97 when comparing all CT HU values of L1–L5.
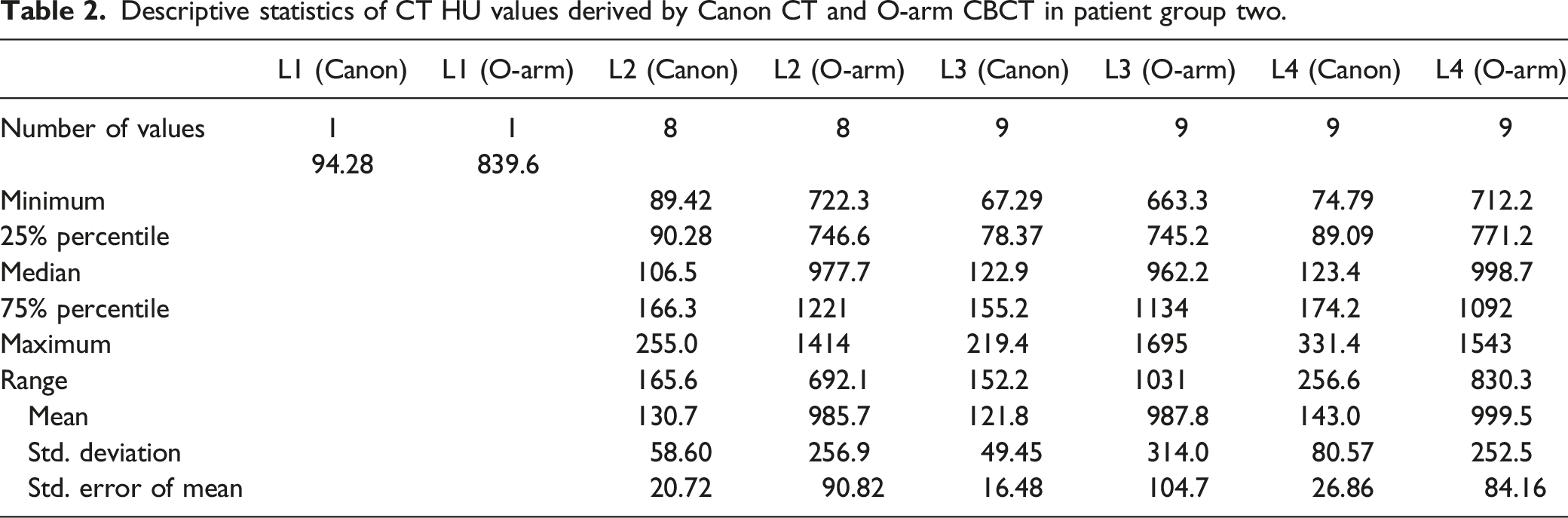
Descriptive statistics of CT HU values derived by Canon CT and O-arm CBCT in patient group two.
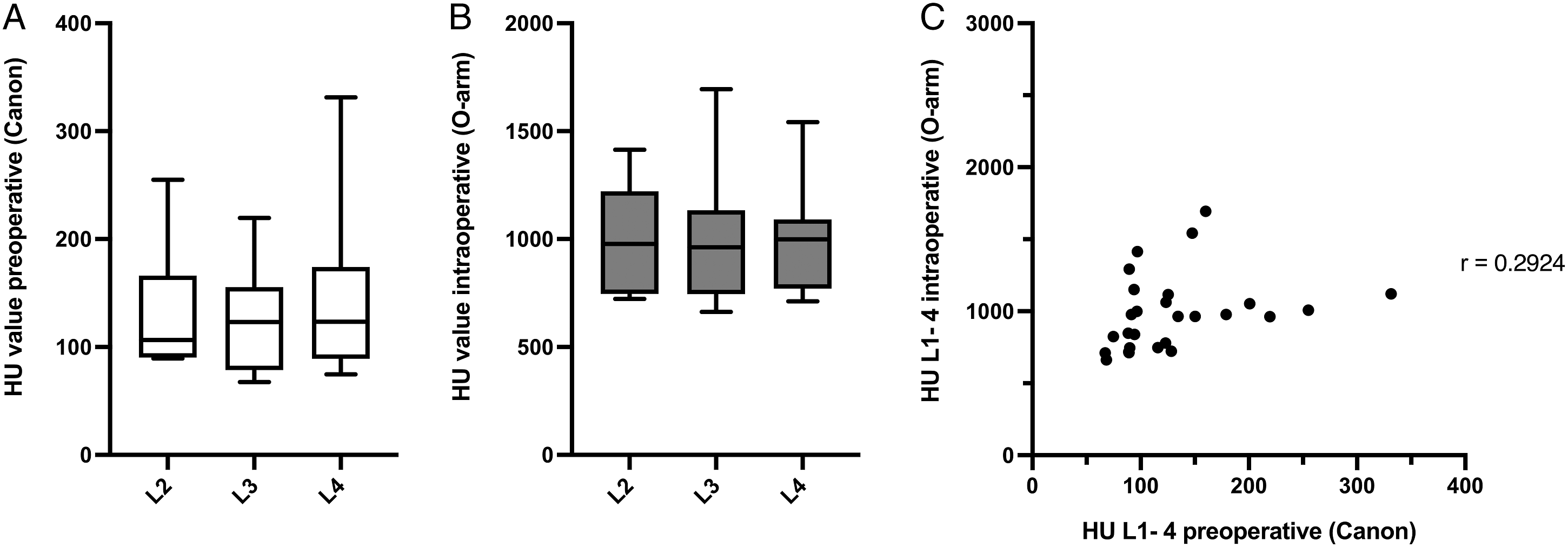
Preoperative (Canon, A) and intraoperative (O-arm, B) CT HU values of L2–4 in patient group two, shown as box and whiskers (box extends from the 25th to 75th percentiles, the line in the middle of the box is plotted at the median. Whiskers represent minimum and maximum). L2: n = 8; L3: n = 9; L4: n = 9. C: Intraoperative (O-arm) and preoperative (Canon) CT HU values showed a Pearson correlation coefficient r of .2924 when all values (L1–L4) were compared together (n = 27).
Radiation Exposure
CTDI values were analysed and compared in 35 patients of patient group one. Mean CTDI ± SD in Canon CT vs AIRO CT were 10.11 ± 6.957 mGy (range 2.3–38.29) vs 12.70 ± 8.58 mGy (range 3.05–35.93). Statistical analysis showed no significant difference of CTDI between Canon CT vs AIRO CT (P = .1148).
Discussion
In this study, we investigated the accuracy and use of intraoperative CT HU values in patients undergoing lumbar interbody fusion. HU values measured intraoperatively with the AIRO CT showed strong correlation to preoperatively measured HU values and approximately matched with those. HU values measured intraoperatively with the O-arm CBCT showed weak correlation to preoperatively measured HU values and did not match with those. The radiation dose in terms of CTDI did not differ significantly between preoperative Canon and intraoperative AIRO CT imaging.
Relevance of Correct Intraoperative CT HU Measurement
Our present study shows for the first time that correct and reliable CT HU measurement as mandatory key factor for the intraoperative assessment of bone quality and robotic (-assisted) surgical procedures is feasible with intraoperative AIRO CT imaging without higher radiation exposure. This is an important finding in the process of economizing and reducing CT scans as thereby the preoperative diagnostic scan for the assessment of bone quality and the intraoperative scan for robotic (-assisted) surgery could be conducted intraoperatively in the same setting, potentially reducing the need for preoperative CT scans. Certainly, preoperative CT imaging cannot be dispensed with in complex spinal diseases since the indication and planning of the surgery often depends on CT imaging. However, for several spinal diseases such as low-grade spondylolistheses or neuroforaminal stenoses that can be treated surgically with lumbar interbody fusion, preoperative CT imaging is not absolutely necessary to plan and determine the indication for surgery. In these cases, as correct HU measurement is possible with AIRO CT scanning, diagnostic information about bone quality could be assessed intraoperatively at no extra cost when scanning for robotic (-assisted) surgery. If our data may decrease the usage of preoperative CT appears questionable as current practice suggests otherwise. Most surgeons rely on preoperative analysis of osteoporosis and its effects on morbidity. However, knowing HU accuracy of intraoperative scanners may be beneficial in emergency cases or situations where preoperative CT is not readily available.
Characteristics of Measured HU Values
HU values showed an increase from the cranial to the caudal lumbar vertebrae in both intraoperative and preoperative CT imaging (Figure 2). This was not congruent with the results of previous studies as e.g. Zou et al. described an increase in HU values from the caudal to the cranial lumbar vertebrae in their ‘degenerative group’ which was epidemiologically similar to our group one (120.2 ± 39.4 in L1, 112.1 ± 38.0 in L2, 106.1 ± 37.1 in L3 and 107.0 ± 41.6 in L4).12,27 Other studies in turn provided similar results to our study, e.g. Meredith et al. reported increasing HU values towards the caudal lumbar vertebrae. 18 These differences may be due to small, inhomogeneous and non-representative patient groups as well as differences in the measurement of HU values. When calculating the mean intraoperative CT HU values of all vertebrae per person of patient group one, a decrease of CT HU values associated with age in males and females was seen (Figure 3), confirming previous findings. 9 In our study, women of younger age (<60) tended to have higher HU values than men of the same age, which could be caused by the small number of patients. Nevertheless, previous studies have also described higher HU values in women than in men of younger age groups, whereas men tend to have higher HU values when >60, which corresponds to our results. 9
HU Values Determined by CBCT
CBCT has the disadvantage of providing non-quantitative results for BMD evaluation. Pearson correlation between intraoperatively derived O-arm CBCT HU values and preoperative Canon CT HU values only showed a weak correlation of r = .2924 when all values were compared together (Figure 6C) and Bland-Altman analysis showed that the HU measures were not equivalent. First of all, the significance of these results is clearly limited due to the small number of patients studied. Only 10 patients were included in this group, in which 27 vertebrae were compared, considerably limiting the correlation analysis and making the comparison between preoperative and intraoperative HU values as well as the comparison between patient group 1 and 2 difficult. Despite this, CBCT HU values were much higher compared to normal CT HU values, which has also been reported in previous studies. 30 To compare HU values measured by different devices, HU calibration is mandatory. The CBCT O-arm is a digital volume tomography (DVT) scanner and not a true CT. The goal of high-contrast DVT imaging is to guide and support surgical procedures by using anatomic landmarks and the absolute intensity of these landmarks does not need to be accurate rather than the intensity differences between these landmarks. Thus, no HU calibration is performed on the O-arm and the HU values of the same tissue are not comparable when placed in a different relative position, 31 which explains why O-arm HU values without calibration cannot be compared to the HU values derived by a conventional, calibrated CT. Nevertheless, our findings suggest that the assessment of bone quality using an O-arm remains hampered regardless of the calibration effect, because the O-arm HU values were not only much higher as a result of lacking HU calibration, but also did not correlate well with the Canon CT HU values.
HU Values Determined by AIRO CT
The preoperative Canon CT imaging tends to deliver slightly higher HU values than the intraoperative AIRO CT imaging as the bias calculated in the Bland-Altman analysis (calculated as average of the differences between preoperative Canon CT HU values minus intraoperative AIRO CT HU values) yielded a value of 3.9. Regarding the range of the HU scale ranging from −1000 (air) to around 1000 (cortical bone) and more, this bias of 3.9 appears small. The bias could be explained by both intra-observer reliability and technical differences between the devices leading to deviation in HU measurements, which has been described before. 32 Nevertheless, the 95% limits of agreement ranged from −27.17 to 34.97. Accordingly, larger differences between the intraoperative and preoperative HU values occur in some patients. Such inaccuracy in the measurement of HU values in some patients is also recognized when e.g. analysing scatter plots of the correlation between vertebral T-score and CT HU values described in the study of Zou et al. 12 This indicates that when assessing the bone quality solely by intraoperative CT HU value analysis one has to evaluate as many vertebrae as possible to reduce the impact of false high/low values and cut off values of a very high sensitivity and specificity for diagnosing osteoporosis have to be established. Therefore, intraoperatively obtained HU values appear to be a valuable adjunct to help alert the physician to metabolic bone diseases such as osteoporosis, but reported differences between intraoperative and preoperative CT HU values underline that caution is advised when relying on these values alone for therapeutic decision-making.
Radiation Exposure
Statistical analysis showed no significant difference of CTDI between preoperative Canon CT and intraoperative AIRO CT (P = .1148). This is an important finding as CT-navigated screw implantation gains widespread application in spine surgery 33 and radiation exposure is commonly underestimated by surgeons and patients34,35 although multiple studies have demonstrated an association between iatrogenic radiation exposure and increased cancer risk. 36 To keep the radiation dose as low as reasonably achievable, CT scans must be appropriately justified for clinical necessity and redundant CT scans must be avoided whenever possible. Therefore, it is important to compare different methods and devices for determining a clinical issue such as CT HU values in terms of their radiation exposure for the patient. Since the radiation doses did not differ between the preoperative Canon CT scan and the intraoperative AIRO scan in our study, neither method is superior to the other in this regard, and in selected cases such as emergencies, CT HU values could be determined solely intraoperatively without higher radiation exposure for the patient compared to preoperative CT imaging.
Limitations
Besides the above-mentioned, there are several other limitations to our study. First, this was a retrospective study, using a relatively small data set of patients from a single academic institution, evaluated in large part by a single examinator. Second, we only compared data from three different imaging devices in two comparisons, implicating limited generalizability of our findings. Third, only the lumbar spine was assessed, making it impossible to transfer the conducted knowledge to other parts of the spine.
Conclusion
In this study, we demonstrated for the first time that HU values measured intraoperatively with the AIRO CT showed a strong correlation to preoperatively measured CT HU values and approximately matched with those. The radiation dose did not differ significantly between preoperative Canon CT and intraoperative AIRO CT imaging. Although the significance is limited due to the small number of patients studied, HU values measured intraoperatively with the O-arm CBCT only showed a weak correlation to preoperatively measured HU values and did not match with those. Thus, intraoperative CT HU values measured with an AIRO CT but not with an O-arm CBCT are reliable and sufficient for CT-assisted robotic surgery and the intraoperative assessment of bone quality, which may be beneficial in emergency cases or situations where preoperative CT is not readily available. Future studies need to confirm our results and HU values measured with other intraoperative CT devices have to be analysed as well.
Consent for publication
Included within the Ethics approval of the Charité – Universitätsmedizin Berlin, Germany (EA4/046/16) and granted by the authors of the study.
Footnotes
Acknowledgments
The authors would like to thank Jürgen Mews, Markus Schade and Christian Balaweider for technical support.
Authors’ Contribution
Conception and design: PV, RM. Data acquisition: RM and HCB. Data interpretation: all authors. Statistical analysis: RM. Drafting of the manuscript: RM, NH, PV. Critical revision of the manuscript for important intellectual content: all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NH is Berlin Institute of Health (BIH) Clinical Fellow, funded by Stiftung Charité. The other authors did not receive any financial support for the authorship, research and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (ethics committee of the Charité University Hospital in Berlin, Germany; EA4/046/16) and with the Declaration of Helsinki (1964) and its later amendments or comparable ethical standards.