
Abstract
Study Design
Retrospective study
Objective
The primary aim of this study was to investigate the predictors of severe complications in patients following surgery for pyogenic spondylodiscitis (PS) using a surgeon-maintained database. The secondary aim was to investigate the predictors of early recovery.
Methods
We introduced a surgeon-maintained database of prospectively collected multicenter data that mainly focused on perioperative complications in 2012. Our surgeon-maintained database allows the retrospective collection of detailed data. We analyzed 143 patients who underwent surgery for PS from the 19,056 patients in the prospective surgeon-maintained database at 27 affiliated institutions between 2013 and 2017. Data relating to preoperative patient factors, infection factors, surgical factors, and pre- and postoperative blood tests was retrospectively collected. We performed multivariate regression analysis to evaluate the predictors of postoperative severe complications and early recovery in patients with PS.
Results
High updated Charlson comorbidity index (uCCI), chronic pulmonary disease, diabetes, Gram-negative bacteria, pyogenic osteoarthritis, high preoperative white blood cell count, and low preoperative platelet count were significantly associated with severe complications in patients undergoing surgery for PS. A high uCCI was the sole independent negative predictor on early recovery.
Conclusion
Careful perioperative management is necessary if surgery is performed on patients who are at a high risk of life-threatening events.
Introduction
Pyogenic spondylodiscitis (PS) is a potentially fatal infectious disease. The in-hospital mortality rate of patients with spinal infection is approximately 4%–6%.1,2 With an aging society, the number of elderly patients with PS is increasing. 3 Thus, PS often occurs in immunosuppressed and chronically debilitated patients who are at a high risk of severe complications and prolonged infection. Surgical intervention is required even for high-risk patients when neurological deficits or deformities progress if antimicrobial therapy is not effective; however, it is still unclear which patient groups are at a high risk of severe complications and prolonged infection.
Recently, studies have suggested that national databases, which were established for simple medical data collection, tend to underestimate the incidence of perioperative complications compared with surgeon-maintained databases.4,5 We introduced a surgeon-maintained database of prospectively collected multicenter data that mainly focused on perioperative complications in 2012. Additionally, our surgeon-maintained database allows retrospective collection of detailed data that cannot be reviewed by national databases.
In the present study, we primarily aimed to investigate the predictors of severe complications in patients with PS using a surgeon-maintained database with sufficient sample size. The secondary aim was to investigate the predictors of early recovery.
Material and Methods
All protocols for this retrospective study were approved by the review board and ethics committee of our institution (No. 11360-3) and all subjects consented with their inclusion in this study.
Patient Demographics
First, a prospective multicenter database for spinal surgery at our 27 affiliated institutions between January 2013 and December 2017 was reviewed. During the research period, a total of 19,056 patients who underwent spinal surgery were registered in our database. Among them, 147 consecutive patients were surgically treated for PS across the 23 institutions (Figure 1). All patients were treated by orthopedic spine surgeons. The spine surgeons responsible for the database at each institution registered data immediately after the patients were discharged. The prospective data from each institution was collected by the university hospital for processing each year. The data manager at the University Hospital checked the integrity of the data and deidentified the collected patient data before analysis. Flow Chart of Patient Selection.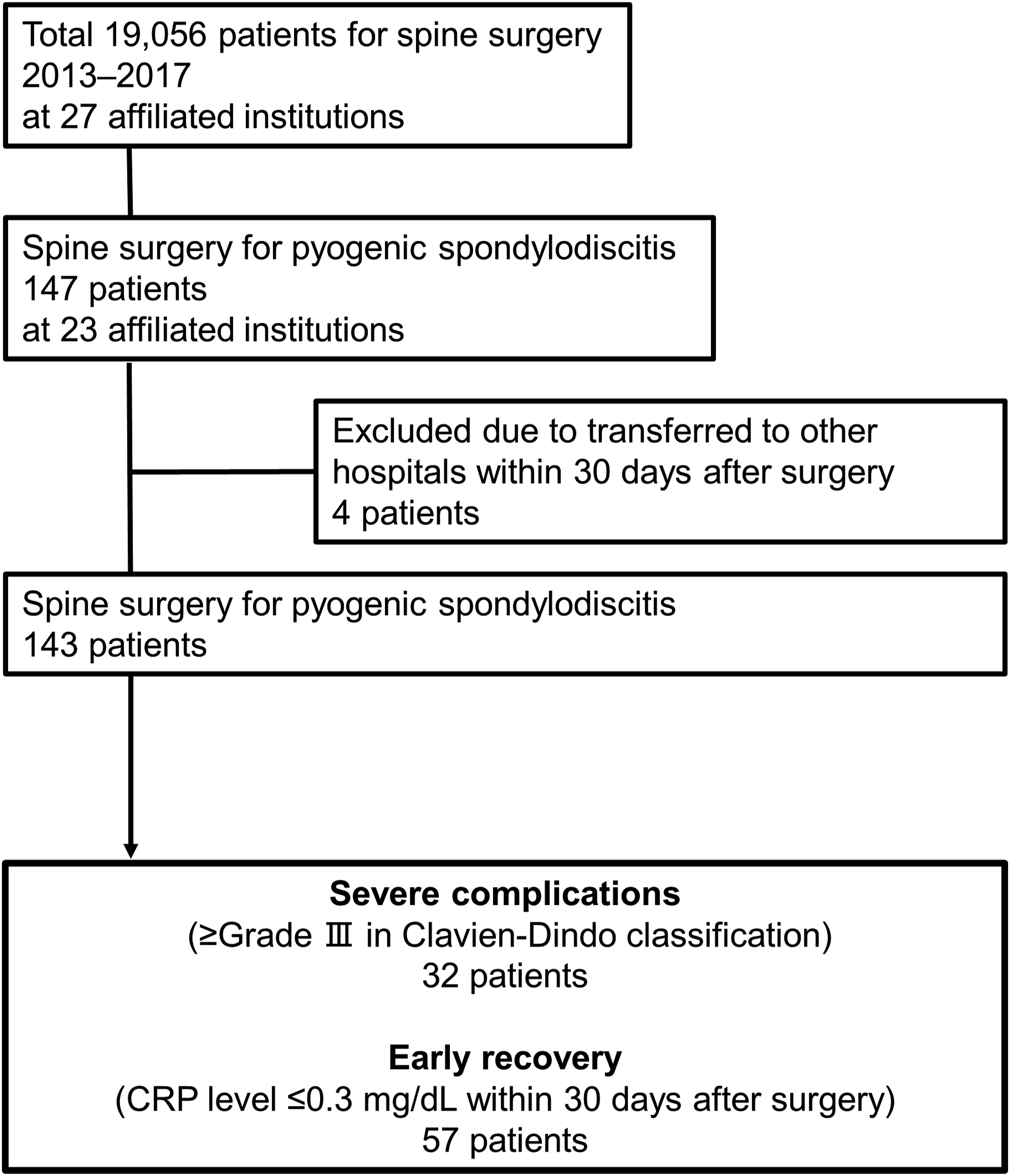
The database included the demographic data of each patient, including primary disease; surgical procedures; and perioperative, surgery-related, and systemic complications of spinal surgery. On the basis of these basic data, we retrospectively collected detailed data on PS surgery, including the potential predictors of severe complications and early recovery in all participating institutions with the same questionnaires using the same Excel file. PS diagnosis was comprehensively established using data on patients’ clinical histories, physical examinations, blood tests, radiological examinations, magnetic resonance imaging (MRI) results, and intraoperative findings (i.e., discharge of pus or formation of granulation tissues). The surgical strategy was at the discretion of the spine surgeon. The antibiotics used to treat PS were selected according to the treatment protocol for infection at each hospital. Therefore, the treatment protocol and surgical procedures may have differed among institutions. However, the spine surgeons at our affiliated institutions underwent unified residency and fellowship programs and they employ comparable treatment protocols and surgical procedures for the treatment of PS. In terms of data collection, operative reports and chart records do not differ substantially among institutions.
To classify surgical complications, we used the Clavien–Dindo (CD) classification. 6 Grade III, IV, and V complications in the CD classification were defined as severe complications. The definitions of grade III, IV, and V in the CD classification are as follows: grade III, requiring surgical, endoscopic, or radiological intervention; grade IV, a life-threatening complication requiring intensive care unit management; and grade V, death. The patient complications in this study were retrospectively graded using the CD classification based on the medical records at each hospital according to the previous reports.6,7 Of the 147 patients, 4 patients who were transferred to other hospitals within 30 days after surgery with ≤grade II in the CD classification were excluded because we were not able to acquire adequate information about complications at the hospitals. The follow-up term (30 days) was set according to a previous study, which investigated mortality within 30 days after surgery for spinal abscess. 8 Finally, we evaluated a total of 143 patients in this study. To evaluate infection control, we reviewed the period of normalization of C-reactive protein level (CRP; ≤.3 mg/dL) after surgery. Then, patients whose CRP level was normalized within 30 days after surgery were defined as those with early recovery. The flowchart of patients included in this study is showing in Figure 1.
Potential Predictive Factors
Preoperative patient factors, infection, surgical factors, and pre- and postoperative blood tests were assessed as potential predictive factors of severe complications and early recovery. Preoperative patient factors included sex, age, comorbidity, updated Charlson comorbidity index (uCCI),7,9 congestive heart failure, dementia, chronic pulmonary disease, rheumatologic disease, liver disease (mild [without portal hypertension] or moderate-to-severe [with portal hypertension]), diabetes with chronic complications, hemiplegia or paraplegia, renal disease, malignancy including leukemia and lymphoma, metastatic solid tumor, acquired immune deficiency syndrome/human immunodeficiency virus, antiplatelet coagulant medication, and use of immunosuppressive medications. Comorbidity was defined in case the patient went to the hospital regularly for treatment of the disease. Infection factors included causative bacteria, positive blood culture, pyogenic osteoarthritis (PS presenting with skip lesions or pyogenic arthritis), time to diagnosis from the first symptom (occurrence of pain or fever), presence of epidural abscess, bone destruction observed on MRI at the time of PS diagnosis, and region of bone infection (cervical, thoracic, or lumbar). Causative bacteria were defined according to blood culture or biopsy results. Multidrug resistant bacteria were defined as bacteria resistant to more than one antimicrobial agent. 10 The diagnosis of pyogenic osteoarthritis was comprehensively established using data on clinical history, physical examination, radiological examination, MRI, and arthrocentesis. Surgical factors included surgical procedure, surgical time, estimated blood loss, presence of instrumentation, and bone graft. The surgical time and estimated blood loss were totaled in all surgeries in case surgery was performed on two or more occasions. Preoperative blood tests were the latest blood tests, which were performed within a week before surgery. The results of preoperative blood tests included information on the following: white blood cell (WBC) count; hemoglobin (Hb) concentration; platelet (Plt) count, and aspartate aminotransferase, alkaline phosphate, creatinine (Cre), and CRP levels. Data on postoperative CRP levels was collected 7–10 days after the index surgery because peak CRP levels are observed within 6 postoperative days without surgical site infection. 11
Statistical Analysis
The SPSS statistical software version 21.0 (IBM Corp, Armonk, New York, USA) was used for all statistical analyses. An overall summary, including the mean and standard deviation of continuous variables, the median and quartile deviation for discrete variables, and frequencies and percentages for categorical variables, were calculated. We analyzed the association between potential predictive factors and severe complications or early recovery using univariate analysis. We used the Student’s t-test, Welch’s t-test, Mann–Whitney U test, and Fisher’s exact test as appropriate to compare the measured variables between the two groups. Multivariate logistic regression analysis was performed and included variables in the univariate analysis with P-values of <.2. We sought the best model based on the Akaike information criterion. Statistical significance for all analyses was set at P < .05.
Results
Univariate Analysis for Severe Complications
Detailed Information About CD Classification.
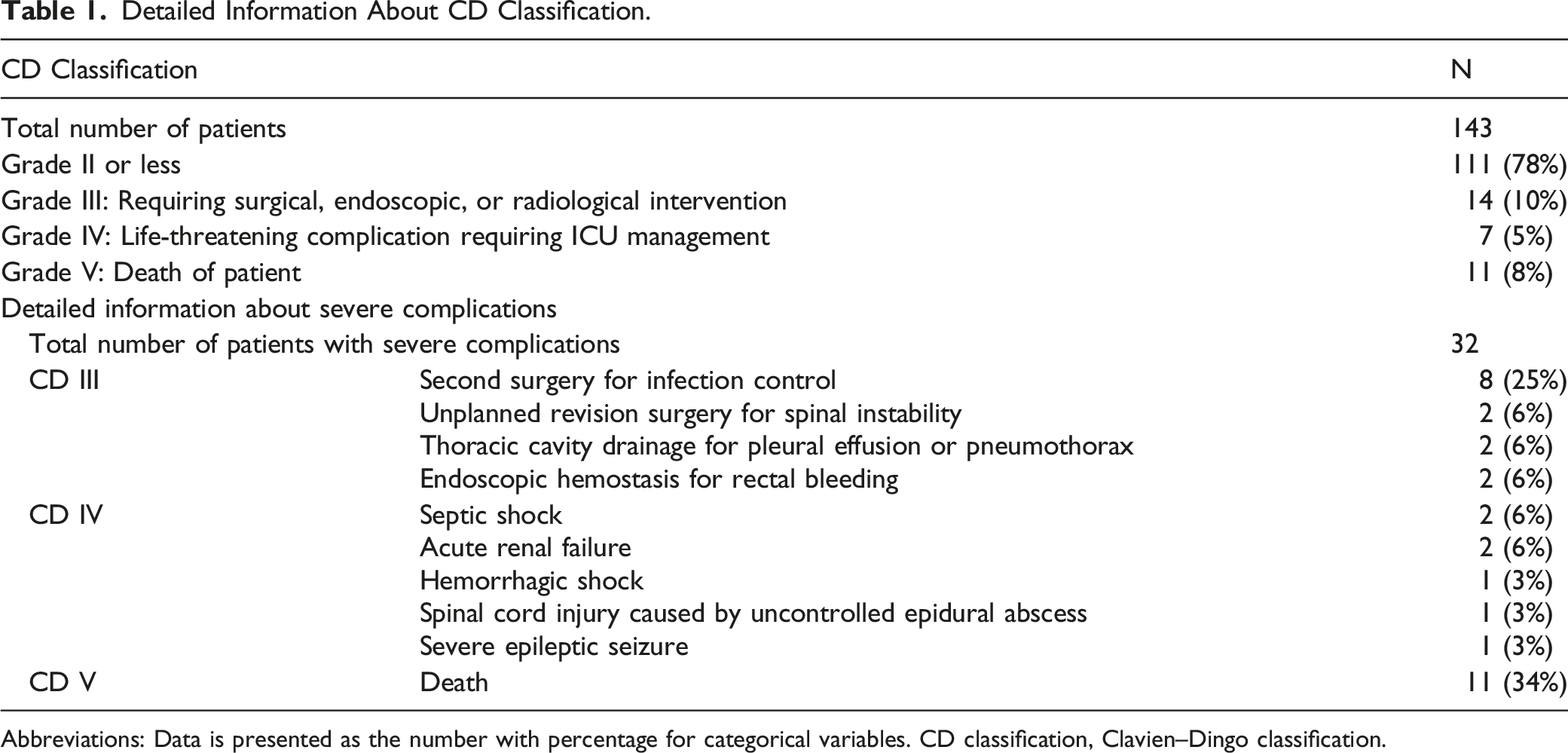
Abbreviations: Data is presented as the number with percentage for categorical variables. CD classification, Clavien–Dingo classification.
Characteristics of Patients with (Cases) or Without (Control) Severe Complications and with (Cases) or Without (Control) Early Recovery After Surgery for Pyogenic Spondylodiscitis.
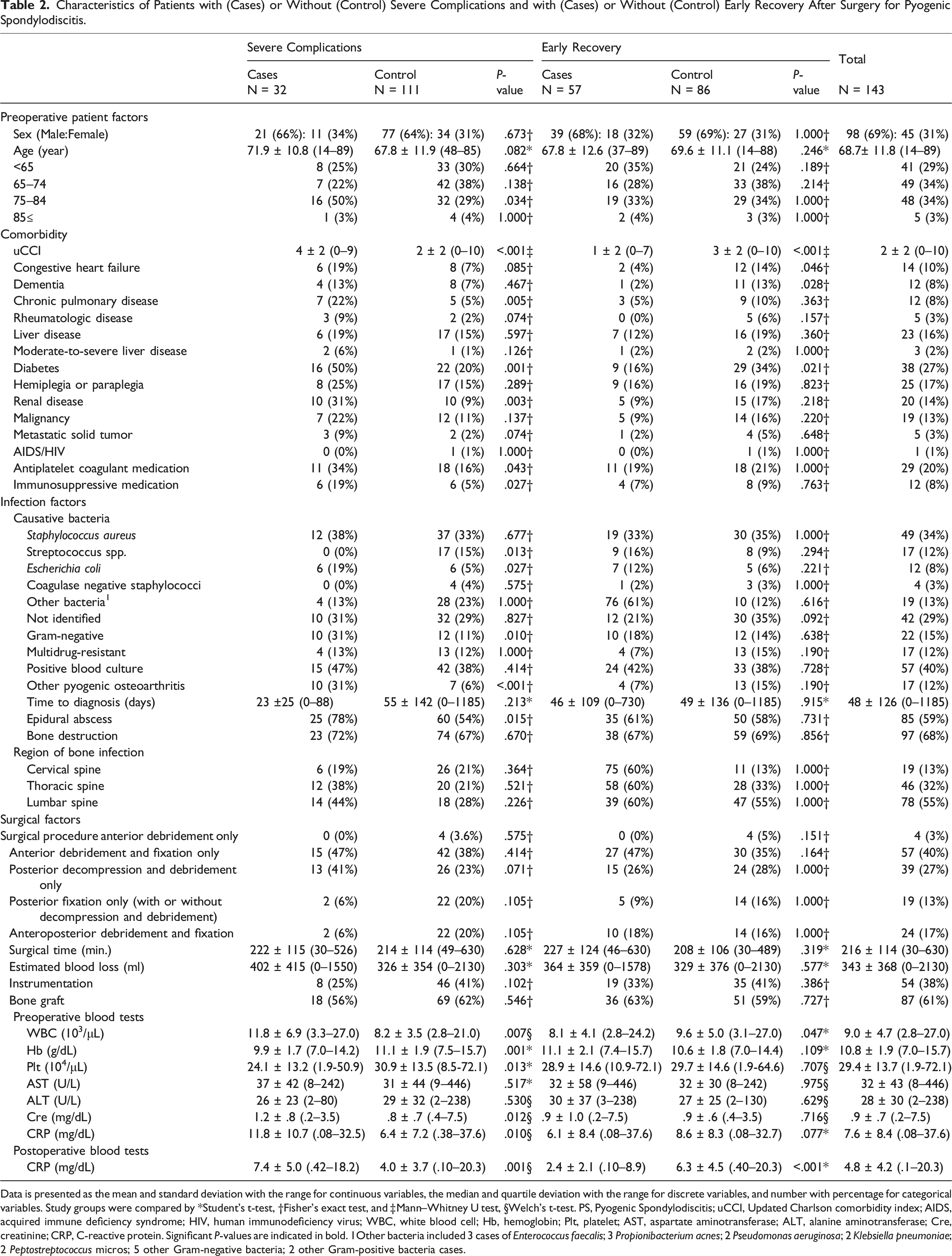
Data is presented as the mean and standard deviation with the range for continuous variables, the median and quartile deviation with the range for discrete variables, and number with percentage for categorical variables. Study groups were compared by *Student’s t-test, †Fisher’s exact test, and ‡Mann–Whitney U test, §Welch’s t-test. PS, Pyogenic Spondylodiscitis; uCCI, Updated Charlson comorbidity index; AIDS, acquired immune deficiency syndrome; HIV, human immunodeficiency virus; WBC, white blood cell; Hb, hemoglobin; Plt, platelet; AST, aspartate aminotransferase; ALT, alanine aminotransferase; Cre, creatinine; CRP, C-reactive protein. Significant P-values are indicated in bold. 1Other bacteria included 3 cases of Enterococcus faecalis; 3 Propionibacterium acnes; 2 Pseudomonas aeruginosa; 2 Klebsiella pneumoniae; 2 Peptostreptococcus micros; 5 other Gram-negative bacteria; 2 other Gram-positive bacteria cases.
Multivariate Analysis for Severe Complications
Results of the multivariate logistic regression analysis for severe complications.
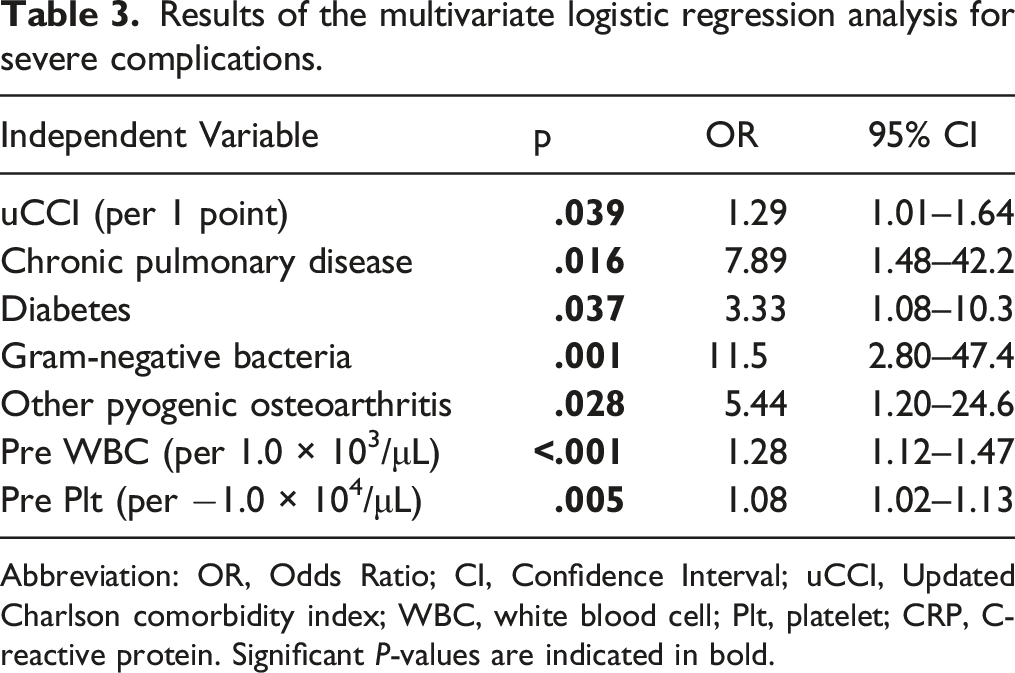
Abbreviation: OR, Odds Ratio; CI, Confidence Interval; uCCI, Updated Charlson comorbidity index; WBC, white blood cell; Plt, platelet; CRP, C-reactive protein. Significant P-values are indicated in bold.
Early Recovery Results
The overall rate of early recovery was 40% (57 of 143 patients). Univariate analysis was performed to evaluate the characteristics of patients with PS with (cases) or without (controls) early recovery. A high uCCI, congestive heart failure, dementia, and diabetes had a significant negative impact on early recovery. A high WBC count in preoperative blood tests and high CRP level in postoperative blood tests also had a significant negative impact on early recovery (Table 2). After seeking the best model using the Akaike information criterion, the analysis revealed that a high uCCI was the sole independent negative predictor of early recovery (OR = .72 per 1 point; 95% CI 0.59–.87; P = .001).
Discussion
This study showed that a high uCCI, chronic pulmonary disease, diabetes, Gram-negative bacteria, pyogenic osteoarthritis, a high preoperative WBC count, and a low preoperative Plt count were significantly associated with severe complications in PS surgery. A high uCCI score was the sole significant independent negative predictor of early recovery.
Although national databases have large sample sizes, they tend to underestimate the incidence of perioperative complications compared with surgeon-maintained databases.4,5 As a strong advantage of our surgeon-maintained database, we can retrospectively collect accurate data related to life-threatening perioperative complications after PS surgery. The mortality rate can be counted accurately even by national databases. Therefore, a recent study using a national database revealed the risk factors for mortality within 30 days after surgery for spinal epidural abscess. 8 However, in PS surgery, perioperative life-threatening severe complications, which are a prelude to death, need to be evaluated. This study identified the risk factors for severe complications by taking advantage of a surgeon-maintained database.
Among preoperative patient comorbidity factors, a high uCCI score, diabetes, and chronic pulmonary disease were identified as independent risk factors of severe complications after PS surgery. These factors are often observed in immunosuppressed and chronically debilitated elderly patients. A high uCCI score was also identified as the sole independent negative predictor of early recovery. uCCI was originally established as a risk factor of mortality.7,9 The results of the present study match the concept of uCCI. Diabetes and chronic pulmonary disease are associated with mortality after surgery for spinal epidural abscess. 8 Furthermore, diabetes is reported to be a risk factor of mortality and unfavorable clinical outcome in conservative treatment for PS.1,12 Together with the results of our study, diabetes increases the incidence of life-threatening events in both surgical and conservative treatment for PS, whereas chronic pulmonary disease is associated with life-threatening events only after surgical treatment for PS. If surgery is necessary for PS patients with chronic pulmonary disease with neurological decline, careful perioperative diabetes and/or respiratory management is of great importance, and patients and physicians should understand the negative predictive impact on the prognosis before making decisions related to surgery.
Among infection factors, Gram-negative bacteria and pyogenic osteoarthritis were identified as risk factors of severe complications. To the best of our knowledge, in PS surgery, Gram-negative bacteria are not reported as a risk factor of poor outcomes. On the contrary, several reports have revealed that Staphylococcus aureus (Gram-positive bacteria) is an independent risk factor of treatment failure, including neurological complications.13,14 Patients with Gram-negative bacteria-induced PS more frequently present with severe sepsis, 15 but are significantly less likely to present with epidural and paravertebral abscess compared with those with Gram-positive bacteria-induced PS. 16 Combined with the previous results, our findings indicate that Gram-negative bacteria-induced PS is less likely to result in neurological complications; however, it has a high risk of severe complications due to sepsis. Pyogenic osteoarthritis (PS presenting with skip lesions or pyogenic arthritis) mainly occurs as a result of hematogenous spread, which is also related to severe sepsis16-18 and may involve multiple joints. 17 Multiple spine involvement in PS has been reported to be a risk factor of mortality and recurrence.18,19 This study revealed infiltration of infection into not only the spine but also other joints are the risk factor for poor postoperative outcomes. Multiple pyogenic lesions are challenging to treat surgically compared with simple PS.
Among the preoperative blood test factors, a high preoperative WBC count and low preoperative Plt count were identified as independent risk factors of severe complications. A previous study reported that high CRP level (>15 mg/dL) was one of the risk factors of severe neurological complications in patients with PS. 14 Their result is consistent with our result of WBC count considering the strong correlation between the WBC count and CRP level in the current study (r2 = .743, P < .001). And similar to our result of Plt, low Plt count (≤1.5 × 105/μL) has been reported to be a risk factor of mortality after surgery for epidural abscess. 8 A high WBC count and a low Plt count are included in the definition of sepsis.20-22 Our result suggests that perioperative sepsis can result in severe complications after PS surgery.
This study has several limitations. First, the data was retrospectively collected. Four patients were transferred to another hospital soon after surgery and the medical records for the CD classification at a different hospital were unclear and incomplete. However, we could completely evaluate almost all patients (143 of 147 [97%]). Second, the follow-up period in this study was limited to 30 days. A minimum follow-up of 1 year is required to investigate the comprehensive prognosis of surgically treated pyogenic spondylodiscitis. However, in this study, we focused on severe complications and death in the early postoperative period. A previous national database study showed that the postoperative 30-day mortality rate for spinal epidural abscess was 3.7%. 8 Of the mortalities that occurred within 30 days of surgery, the majority (70%) occurred within 2 weeks. 8 Combining the previous results with the primary aim of this study, we believe that the 30-day follow-up period is acceptable.
In conclusion, the present study demonstrates that a high uCCI score, chronic pulmonary disease, diabetes, Gram-negative bacteria, pyogenic osteoarthritis, a high preoperative WBC count, and a low preoperative Plt count are significant independent predictive factors of severe complications. A high uCCI score is the sole significant independent negative predictor of early recovery in this study. These findings may guide clinicians’ decisions about surgical intervention for patients with PS, and careful perioperative management is necessary to treat high-risk patients with PS.
Footnotes
Acknowledgments
Yuichiro Ukon received a funding for this study from the Grant of Japan Orthopaedics and Traumatology Research Foundation No. 443. We thank Sadaaki Kanayama MD (Ikeda Municipal Hospital), Kazutaka Izawa MD (Toneyama National Hospital), Toshihiko Tanimoto MD (Amagasaki Chuo Hospital), Hideaki Enami MD (Japanese Red Cross Society Himeji Hospital), Daisuke Yamakawa MD (Sakai City Hospital Organization, Sakai City Medical Center), Atsunori Ohnishi MD (Kansai Rosai Hospital), Kunihiko Hashimoto MD (Osaka Police Hospital), Hiroki Hagizawa MD (Minoh City Hospital), Takahiro Maenaka MD (Osaka General Medical Center), and Junzo Hayashi MD (Itami City Hospital) for their dedication in collecting patient data. No funding was received for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.