
Abstract
Study Design:
Meta-analysis.
Objective:
To systematically compare the effectiveness and safety of vertebral augmentation procedure (VAP) with non-surgical management (NSM) for the treatment of osteoporotic vertebrate compression fractures (OVCFs).
Methods:
Systematic reviews and meta-analyses with the comparison between VAP and NSM were identified to extract randomized controlled trials from electronic database. Additionally, recently published RCTs were identified. Two researchers independently extracted the data. The primary outcome of this meta-analysis was pain relief evaluated by visual analogue scale (VAS).
Results:
Twenty RCTs involving 2566 patients with painful OVCFs were included. Significant differences were found between percutaneous vertebroplasty (PVP) and conservative treatment (CT) in VAS at each time point during follow-up period. The differences of VAS were not significant between PVP and sham procedure at most time points during follow-up period. In subgroup analysis based on fracture type and fracture location, significant differences of VAS were found between PVP and CT and were not found between PVP and sham procedure. In subgroup analysis of duration of back pain, significant differences were found between PVP and CT in VAS at 1 week, 3 month and 1 year. And the differences of VAS were not significant between PVP and CT at 1 month and 6 month.
Conclusion:
BKP is considered sufficient to achieve good clinical outcomes. PVP is associated with on beneficial effect on treatment of painful OVCFs compared with sham procedure. The indication and timing of VAP need further research. More independently high-quality RCTs with sufficiently large sample sizes reporting cost-effectiveness are needed.
Keywords
Introduction
With an estimated 1.4 million new patients occurring annually worldwide, 1 osteoporotic vertebrate compression fractures (OVCFs) are associated with high prevalence, multiple complications, difficult nursing and expensive treatment.2,3 As the world enters the aging society, OVCFs are considered as a huge drain on the public medical and health resources. Patients with symptomatic OVCFs suffer from substantial pain and disability caused by vertebral height loss and kyphosis. Without timely and effective treatment, some severe consequences may occur, such as Kummell disease, 4 which will bring more financial burdens to patients and their families.
In addition to open surgery and non-surgical management (NSM), vertebral augmentation procedure (VAP) is widely advocated as a minimally invasive treatment for painful OVCFs. Since its invention, VAP has been highly reported for significant pain relief in both short and long term worldwide. Additionally, it became very popular especially in recent 10 years. Both percutaneous vertebroplasty (PVP) and balloon kyphoplasty (BKP) inject bone cement into injured vertebrae to achieve pain relief and restore the height and stability of vertebrae. The difference between PVP and BKP is the latter uses a balloon to expand the vertebrae first. 5 Plenty of reviews and meta-analyses have been published to conduct the safety and efficacy of the VAP.6-9 However, the conclusion is disputed. Some suggested VAP was the most appropriate strategy in reducing pain, improving functional status and quality of life. 10 But others hold different opinions. Buchbinder et al concluded that the clinically important benefits of PVP are no demonstrable compared with a sham procedure. 11 So far, the inclusion criteria of patients and appropriate timing to perform VAP are still not adequately identified. 5 This meta-analysis was performed to systematically compare the effectiveness and safety of VAP with NSM for the treatment of OVCFs.
Materials and Methods
Search Methods and Selection Criteria
We systematically searched PubMed, EMBASE, the Cochrane Library, China National Knowledge Infrastructure (CNKI) from inception until Marth 4, 2020. Systematic reviews and meta-analyses which conducted the comparison between VAP and NSM published since 2006 to 2019 were identified, from which we extracted randomized controlled trials (RCT). Additionally, we used percutaneous vertebroplasty, balloon kyphoplasty and OVCFs as key words to identify recent RCTs published from 2016 to 2020. There were no language restrictions. All included RCTs met the inclusion criteria described below.
Trials were included according to the follow criteria: (1) conducting the comparison between VAP (PVP and/ or BKP) and NSM (conservative treatment or sham procedure); (2) patients aged 50 or older with painful OVCFs; (3) describing at least one outcome of interest. Trials were excluded if: Interventions were different from the previous description; Or original data was lost after confirmation with corresponding author.
Data Extraction and Statistical Analyses
Two researchers independently extracted the data, including the information of trials, inclusion criteria, participant characteristics, outcomes of interest and duration of treatment. The primary outcomes are visual analogue scale (VAS) and the Roland–Morris Disability Questionnaire (RMDQ). Secondary outcomes are the Oswestry Disability Index (ODI), the European Quality of Life–5Dimensions (EQ–5D) scale, and the Physical Component Summary (PCS) subscales of the Medical Outcomes Study 36-Item Short-Form General Health Survey (SF-36), kyphotic wedge angle, vertebral height and new vertebral fracture. To evaluate the effect of each approaches of VAP, (PVP and BKP), accurate analyses were performed based on the interventions of experimental group (PVP or BKP) and control group (conservative treatment or sham procedure). To further identify the optimal subsets of patients for VAP (PVP or BKP), subgroup analyses based on types of osteoporotic fractures (from pure edema to complete destruction), location of fracture (vertebral level with fracture) and duration of back pain (pain duration of patients
Assessment of Risk of Bias
The risk of bias in the included RCTs was evaluated by the Cochrane Collaboration’s risk-of-bias criteria. The classifications of bias were based on 7 items: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other bias. 12 Each item is graded into 3 degrees: low risk, unclear risk, or high risk. The quality of included trials was graded basing on the follow criteria:(1) a trial was evaluated as high quality when both randomization and allocation concealment were assessed as a low risk of bias and all other items of bias were graded as low or unclear; (2) quality of trial was low when either allocation concealment or randomization was assessed as a high risk of bias, regardless of other risk items; (3) quality of trial was moderate when a trial met neither the criteria of high nor low quality. 13
Results
Study Selection and Characteristics
Thirty-four trials were retrieved from published systematic reviews and meta-analyses.8,10,14-18 After removing duplications and full-text screening, 16 trials were eliminated. Additionally, two researchers independently retrieved recently eligible trials from electronic database. At final, 20 trials which met the eligibility criteria were included in this study.19-38 In total, 2566 patients with painful OVCFs were included in this meta-analysis. Among the 20 trials, BKP was performed in 4 trials22,23,25,36 and PVP in 16 trials19-21,24,26-35,37,38; sham procedure in 6 trials26,28,29,31,32,35 and conservative treatment (CT) in 14 trials19-25,27,28,30,33,34,36-38; preoperative medication situation was provided in 13 trials.23,27-38 Six trials were conducted in China.19-22,27,38 The characteristics of the included trials were shown in Table 1. More detailed information on the selection and quality of the included trials is provided in the Supplemental Materials.
Characteristics of the Included Trials.
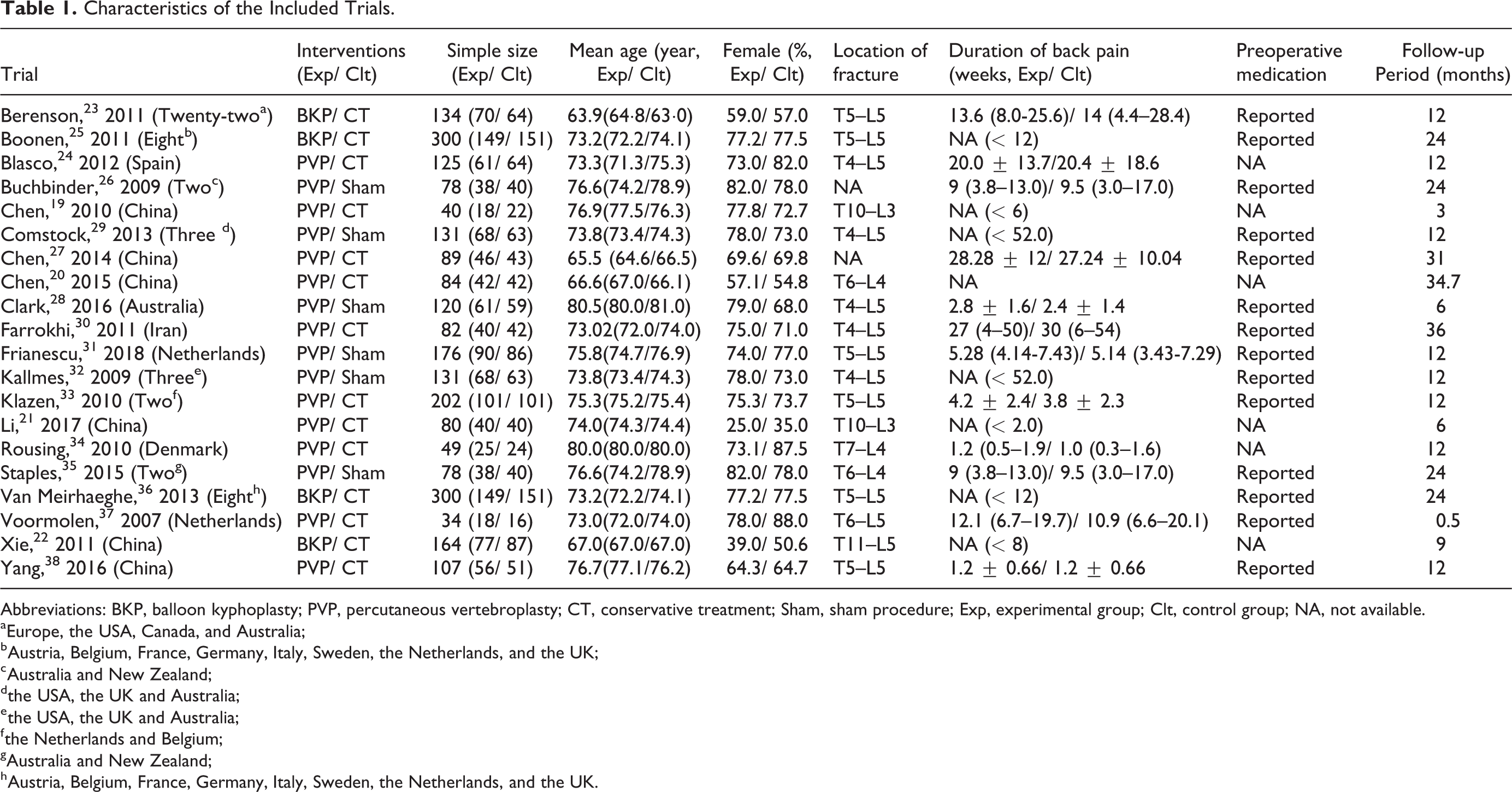
Abbreviations: BKP, balloon kyphoplasty; PVP, percutaneous vertebroplasty; CT, conservative treatment; Sham, sham procedure; Exp, experimental group; Clt, control group; NA, not available.
a Europe, the USA, Canada, and Australia;
b Austria, Belgium, France, Germany, Italy, Sweden, the Netherlands, and the UK;
c Australia and New Zealand;
d the USA, the UK and Australia;
e the USA, the UK and Australia;
f the Netherlands and Belgium;
g Australia and New Zealand;
h Austria, Belgium, France, Germany, Italy, Sweden, the Netherlands, and the UK.
Pain Relief
Twenty RCTs19-38 involving 2566 patients with painful OVCFs were included in this meta-analysis. Fifteen trials19-22,26-34,36,37 reported pain relief evaluated by VAS. Significant differences were found between PVP and CT in VAS at 1 day (MD, −2.84 [95% CI, −3.38 to −2.29]), 1 week (MD, −2.87 [95% CI, −3.00 to −2.74]), 1 month (MD, −0.76 [95% CI, −0.89 to −0.64]), 3 months (MD, −0.89 [95% CI, −1.02 to −0.75]), 6 months (MD, −0.64 [95% CI, −0.73 to −0.55]) and 1 year (MD, −1.60 [95% CI, −1.85 to −1.35]) shown in Figure 1. The differences of VAS were not significant between PVP and sham procedure at 1 week (MD, 0.24 [95% CI, −0.38 to 0.86]), 2 week (MD, −0.53 [95% CI, −1.29 to 0.22]), 1 month (MD, −0.53 [95% CI, −1.07 to 0.02]), 3 month (MD, −0.40 [95% CI, −0.99 to 0.19]) and 1 year (MD, −0.60 [95% CI, −1.13 to −0.07]) after intervention and significant difference was found between PVP and sham procedure in VAS at 6 months (MD, −0.58 [95% CI, −1.26 to 0.09]) shown in Figure 2.
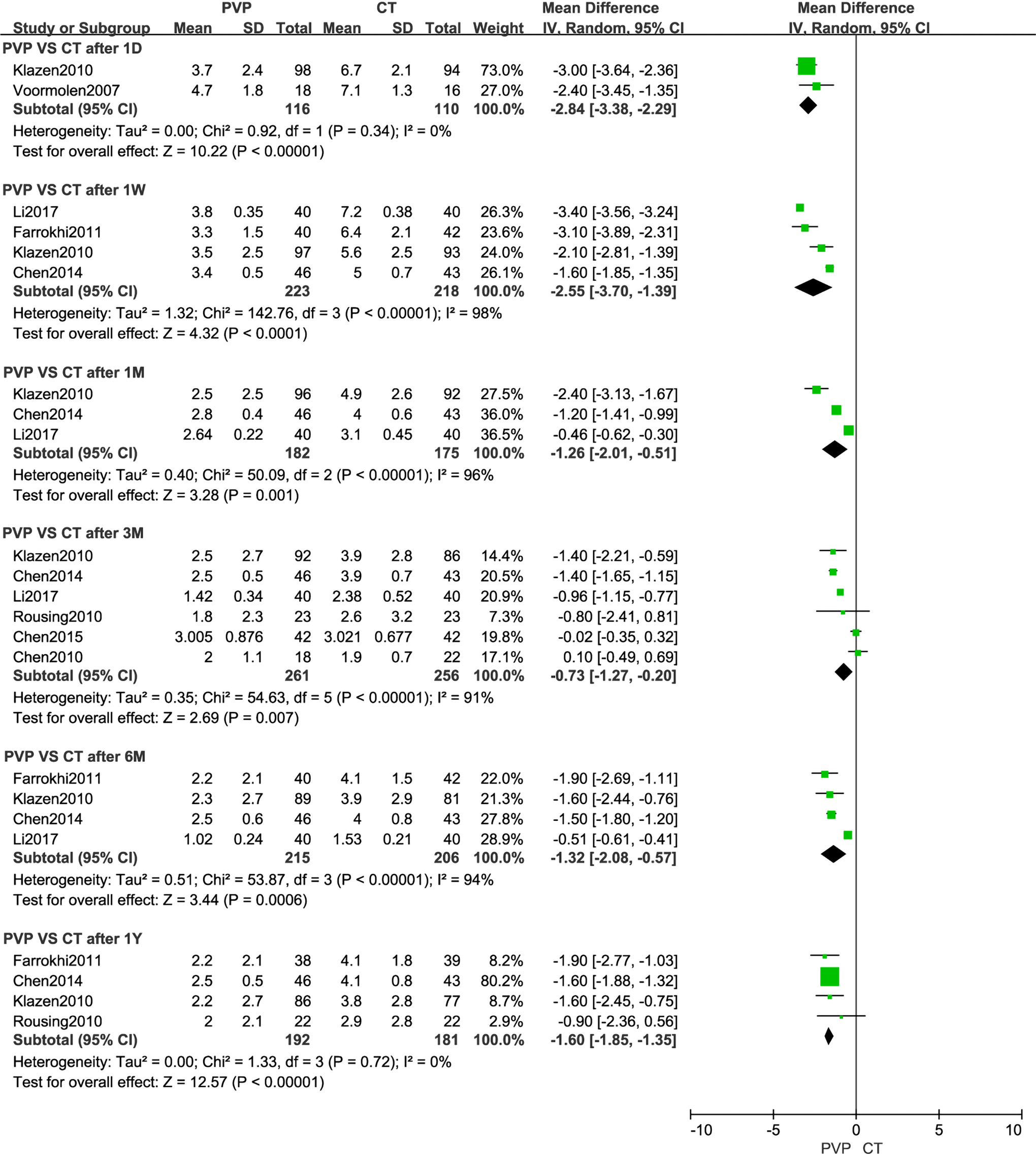
Meta-analysis results of pain relief evaluated by visual analogue scale between PVP and CT.
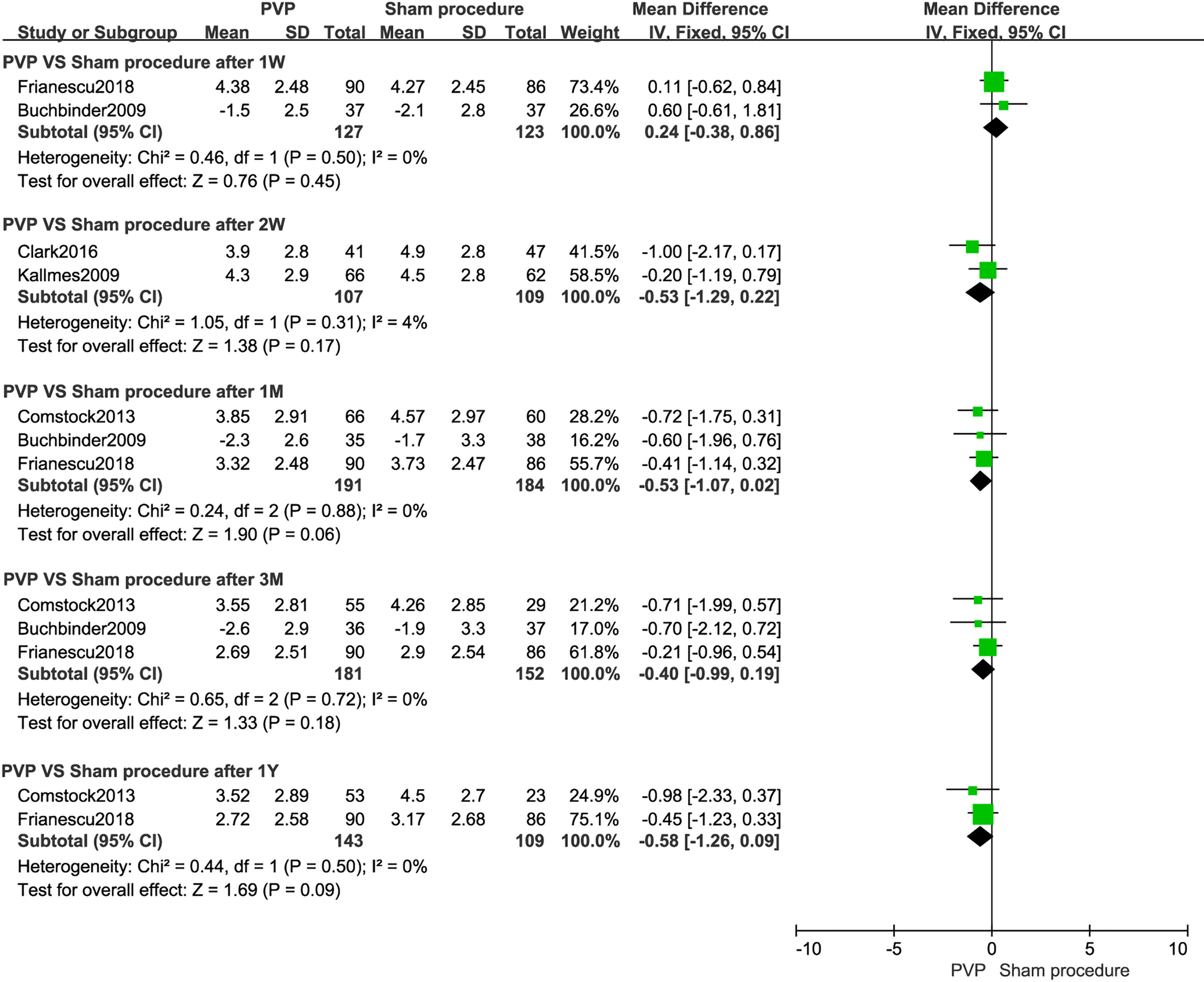
Meta-analysis results of pain relief evaluated by visual analogue scale between PVP and Sham procedure.
In subgroup analysis of patients with vertebra deformity and marrow edema, significant differences were found between PVP and CT in VAS at 1 day (MD, −2.84 [95% CI, −3.38 to −2.29]), 1 week (MD, −2.59 [95% CI, −3.56 to −1.61]), 6 month (MD, −1.76 [95% CI, −2.34 to −1.18]) and 1 year (MD, −1.75 [95% CI, −2.35 to −1.14]). The difference of VAS was not significant between PVP and Sham procedure at 1 week (MD, 0.24 [95% CI, −0.38 to 0.86]), 1 month (MD, −0.45 [95% CI, −1.10 to 0.19]), 3 month (MD, −0.32 [95% CI, −0.98 to 0.35]) and 6 month (MD, −0.37 [95% CI, −1.05 to 0.31]). In subgroup analysis of location of fracture (T4/5 to L5), significant differences were found between PVP and CT in VAS at 1 week (MD, −2.59 [95% CI, −3.56 to −1.61]), 6 month (MD, −1.76 [95% CI, −2.34 to −1.18]) and 1 year (MD, −1.75 [95% CI, −2.35 to −1.14]). The difference of VAS was not significant between PVP and Sham procedure at 2 week (MD, −0.53 [95% CI, −1.29 to 0.22]), 1 month (MD, −0.51 [95% CI, −1.11 to 0.08]), 3 month (MD, −0.34 [95% CI, −0.98 to 0.31]) and 1 year (MD, −0.58 [95% CI, −1.26 to 0.09]). Significant differences of VAS were found between PVP and Sham procedure at 6 month (MD, −0.64 [95% CI, −1.21 to −0.08]). In subgroup analysis of duration of back pain
Subgroup-Analysis Results of Pain Relief Evaluated by Visual Analogue Scale (Based on Fracture Type, Fracture Location and Duration of Back Pain).
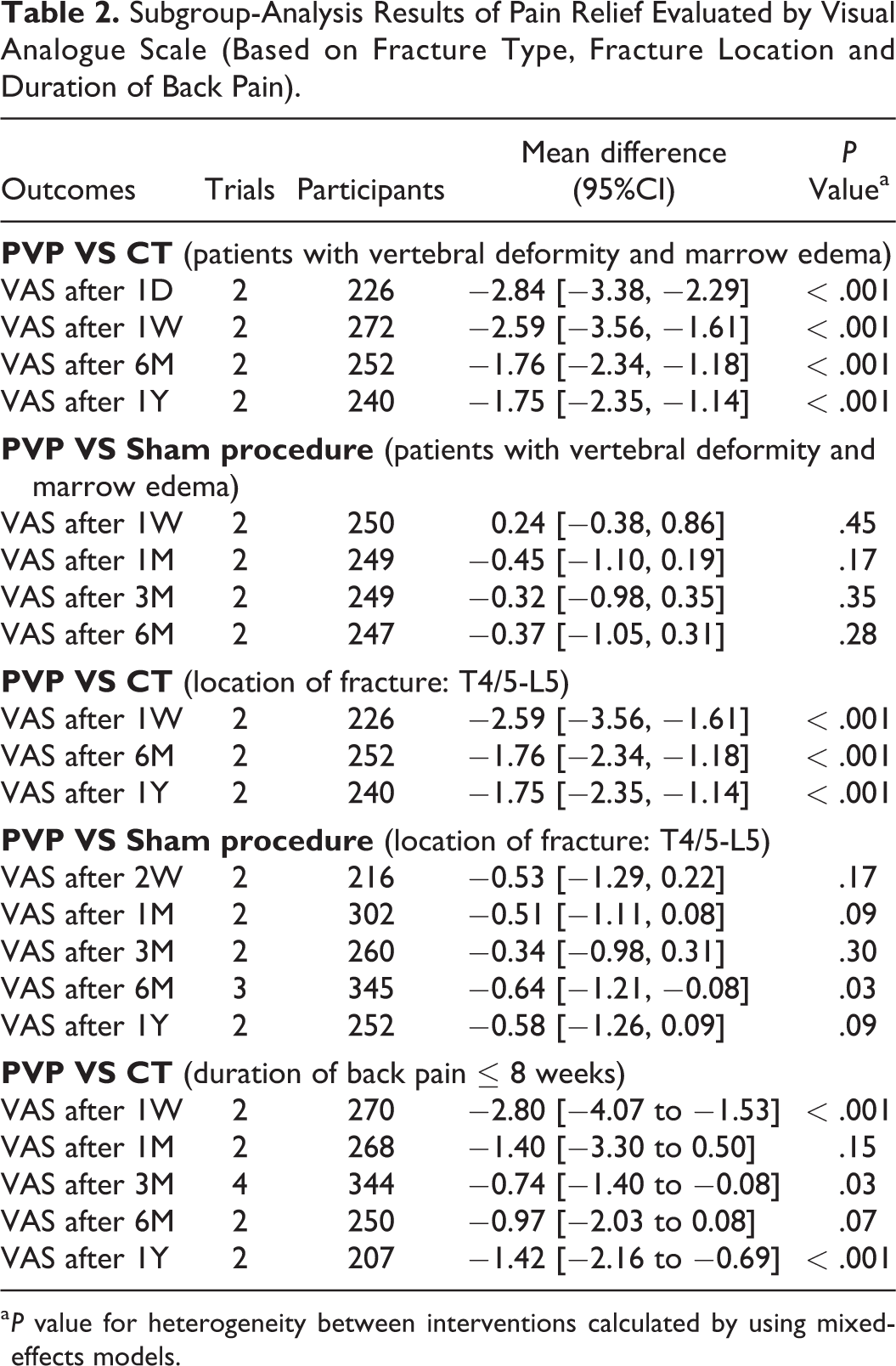
a P value for heterogeneity between interventions calculated by using mixed-effects models.
Functional Status
The differences of ODI in PVP group were not significant at 1 week (MD, −7.71 [95% CI, −20.45 to 5.03]), 1 month (MD, −9.33 [95% CI, −20.50 to 1.84]) and 3 months (MD, −6.00 [95% CI, −14.83 to 2.84]) compared with CT group. The differences of RMDQ between PVP and sham procedure were not significant at 3 day (MD, 1.01 [95% CI, −0.34 to 2.36]), 3 month (MD, −0.98 [95% CI, −3.60 to 1.64]) 6 month (MD, −2.30 [95% CI, −4.56 to −0.04]) and 1 year (MD, −0.85 [95% CI, −2.84 to 1.14]). Significant differences were found between BKP and CT in RMDQ at 1 month (MD, −6.23 [95% CI, −10.34 to −2.11]) and 6 months (MD, −3.12 [95% CI, −4.55 to −1.69]) (Table 3).
Meta-Analysis Results of Functional Status (Evaluated by ODI and RMDQ) and Quality of Life (Evaluated by EQ–5D).
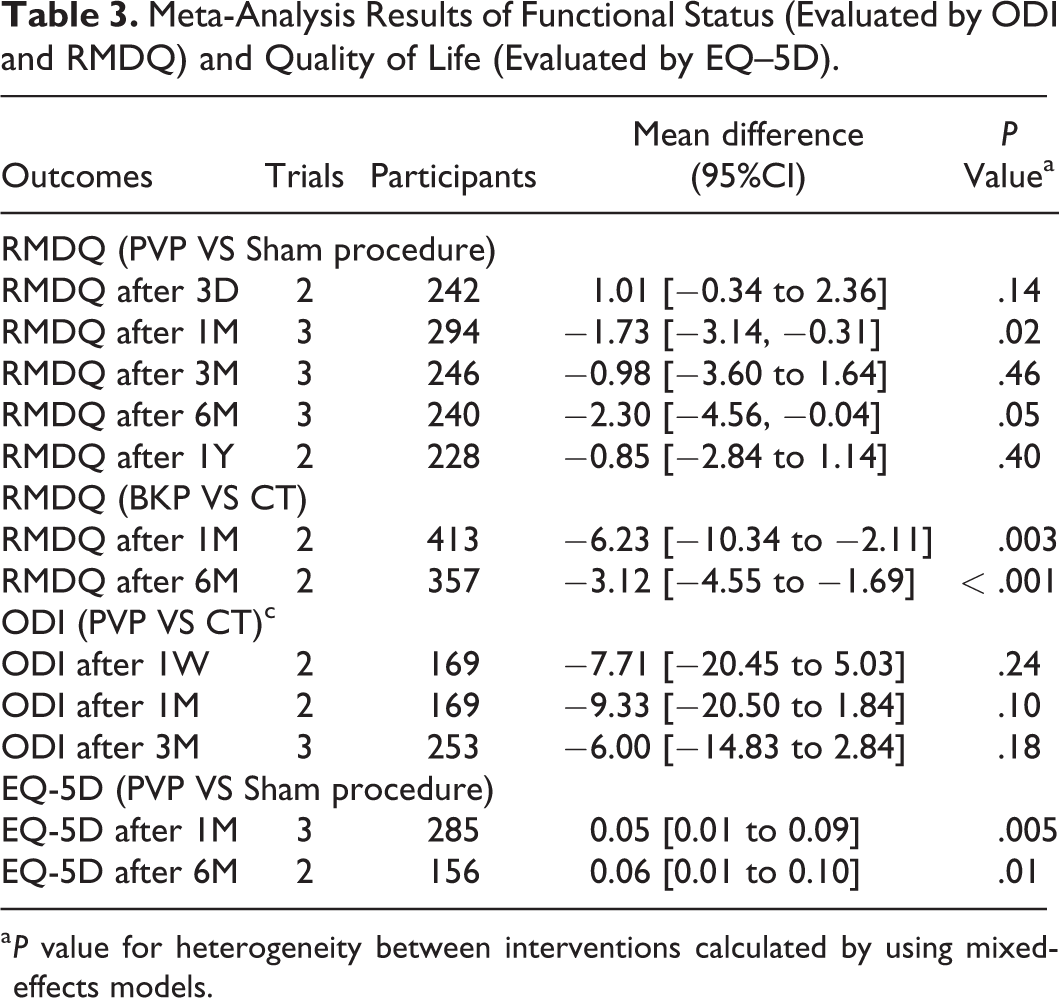
a P value for heterogeneity between interventions calculated by using mixed-effects models.
Quality of Life and Imageology Results
The EQ–5D in PVP group was superior to that in sham procedure group at 1 month (MD, 0.08 [95% CI, 0.02 to 0.14]) and 6 months (MD, 0.08 [95% CI, 0.04 to 0.11]) (Table 3). There was no significant difference in new vertebral fracture between PVP and CT (OR, 1.25 [95% CI, 0.50 to 3.11]), BKP and CT (OR, 1.82 [95% CI, 0.32 to 10.54]) and PVP and sham procedure (OR, 1.33 [95% CI, 0.74 to 2.39]) shown in Figure 3.
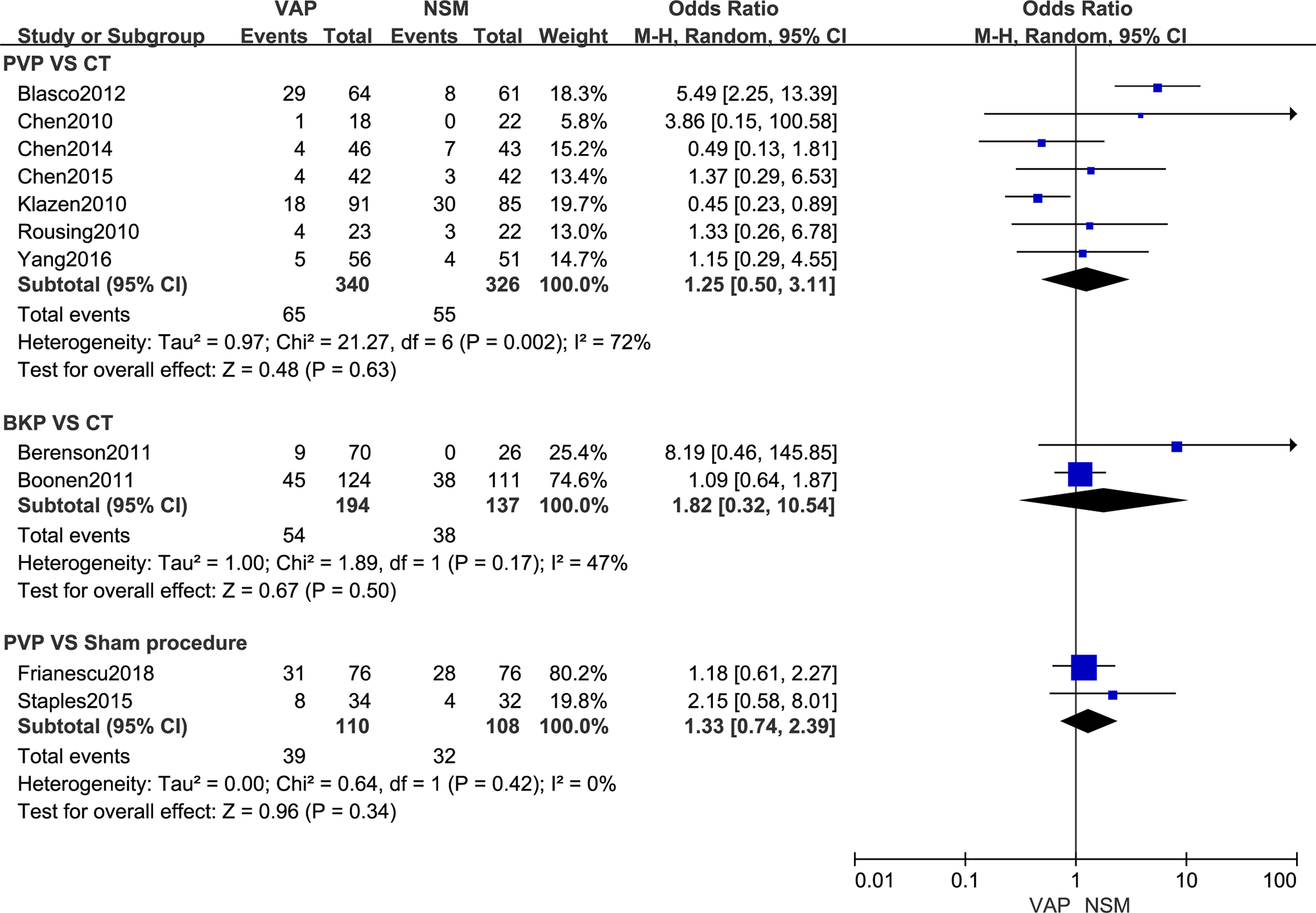
Meta-analysis results of new vertebral fracture.
Risk of Bias
All included trials were randomized. Nineteen trials described the appropriate random sequence generation19-36,38 and 12 trials reported the allocation concealment.23,25,26,28-36 Five trials were double-blind26,28,29,31,32 (shown in Figure 4). There were 6 trials evaluated as high quality23,26,28,29,31,32 while others as moderate quality.19-22,24,25,27,30,33-38 Trials of Yang et al 38 and Boonen et al 25 failed to report that the number of new vertebral fractures was according to whether people or cases after we tried to connect the corresponding authors. Sensitivity analysis showed that the inclusion of these data had no effect on the results. When 10 or more trials were pooled in one outcome, inspection of funnel plot was performed to assess publication bias.
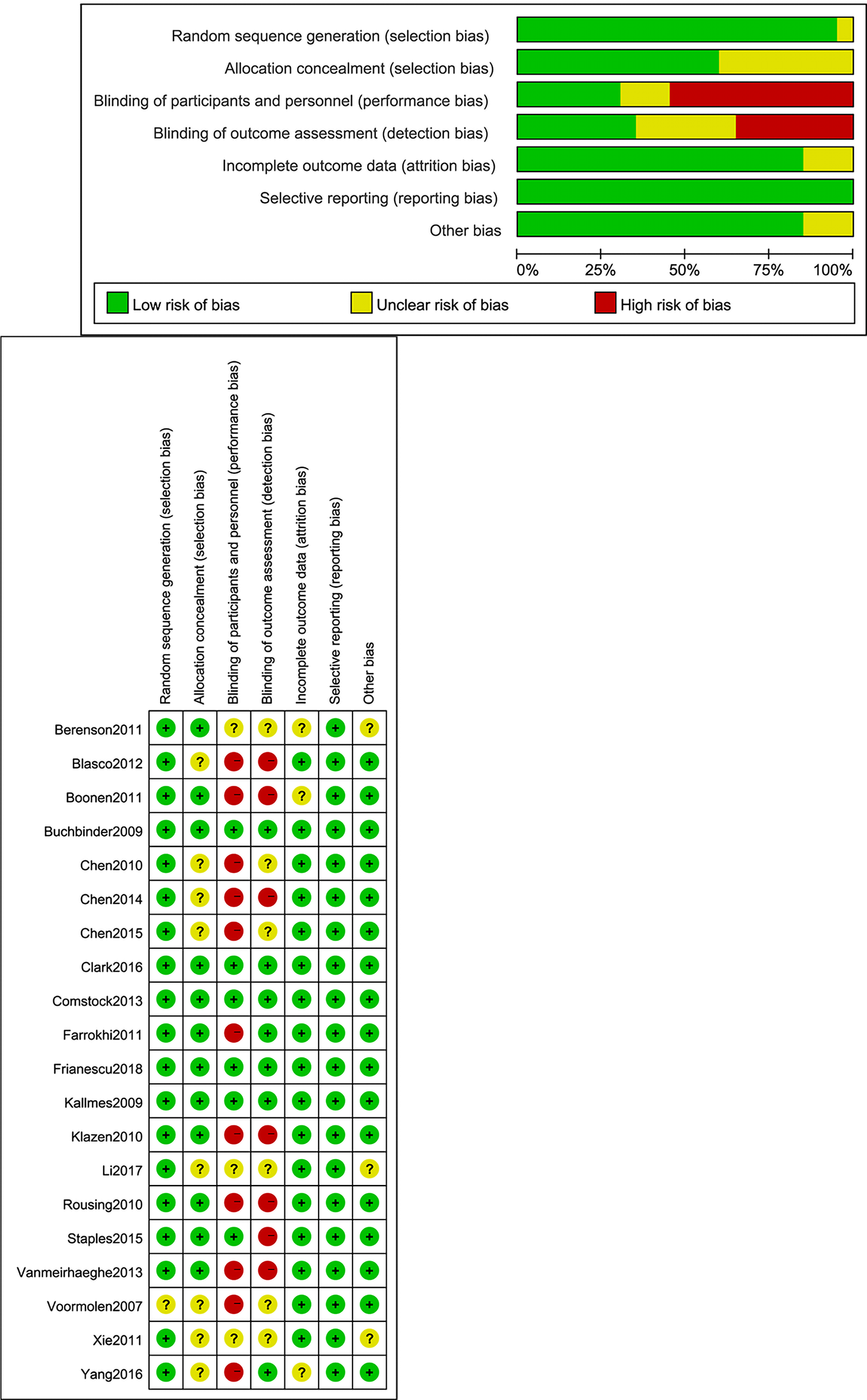
Risk of bias summary.
Discussion
In this meta-analysis, PVP was associated with significant pain relief compared with CT at each time point during follow-up period. And the differences of VAS were not significant between PVP and sham procedure at most time points during follow-up period. In subgroup analysis of patients with vertebra deformity and marrow edema, significant differences were found between PVP and CT in VAS at each time point during follow-up period. The difference of VAS was not significant between PVP and Sham procedure at each time point during follow-up period. In subgroup analysis of location of fracture (T4/5 to L5), significant differences were found between PVP and CT in VAS at each time point during follow-up period. The difference of VAS was not significant between PVP and Sham procedure at most time points during follow-up period, except at 6 month. Pain is a complex physiological and psychological activity, having a great relationship with anxiety. All trials included in sham procedure subgroup analysis stimulated patients in sham procedure group by such as pressure on the back and the odor associated with mixing of PMMA. Bahar et al suggested that psychological intervention could be useful for pain treatment. 39 In other words, sham procedure could be regarded as a psychological intervention. Sham procedure provided a solid psychological hint for patients that they did receive VAP and their psychological states and anxiety may have changed dramatically. All included trials in the comparison of pain relief between PVP and sham procedure were double-blind and reported the preoperative medication, which had good results for heterogeneity control. Hence, these reported findings suggested that the effects of PVP may come from psychological hints to a great extent and psychological counseling could also be used as a method to relieve pain for patients with OVCF.
Many systematic reviews and meta-analysis advocated that VAP was suitable for either acute/subacute or chronic OVCFs, and patients who underwent VAP could benefit from it in both short and long term.15,17,40 It could be difficult to define when an osteoporotic vertebra compression fracture occurs in clinical practice. By the time the patient is aware of back pain, OVCF has already existed. The majority of these included trials24-33,35,37 set the time from onset of back pain to replace the estimated age of fracture as one of the inclusion criteria and reported the duration of back pain in the basic characteristics of their patients. But there is a certain amount of estimating and approximating by using duration of back pain to represent the duration of fracture, which is feasible in principle but not entirely accurate. In the subgroup analysis of the duration of back pain ≤ 8 weeks, significant differences were found between PVP and CT in VAS at 1 week, 3 month and 1 year. And the differences of VAS were not significant between PVP and CT at 1 month and 6 month. Although at the follow-up time point of 1 week after operation, PVP showed superior pain relief with statistical significance than conservative treatment. However, we believed that to evaluate the difference of pain relief between VAP and NSM can not only be judged from one time point in the follow-up. For the results of this subgroup analysis, there was no rule to explain the pain relief of PVP for patients with OVCFs from the time sequence of follow-up based on the existing data. the early detection and diagnosis of vertebral compression fractures. The indication and timing of VAP need further research. And researches on the early detection and diagnosis of OVCFs should be further performed.
Both RMDQ and ODI are questionnaires evaluating dysfunction and the sensitivity of ODI is superior to that of RMDQ.41,42 All trials reporting ODI were performed by Chinese research team and all trials including RMDQ were performed by non-Chinese. At present, the conclusion on whether PVP or BKP is more advantageous in functional recovery is still not unified.16,43-45 In this meta-analysis, the differences of ODI in PVP group were not significant throughout the follow-up period compared with CT group. The differences of RMDQ between PVP and sham procedure were not significant at most time points. Significant differences were found between BKP and CT in RMDQ at 1 month and 6 month. Many published reviews and meta-analyses reported that BKP could improve the functional status of patients with OVCFs by improving vertebral stability. 16 By the combination of balloon and bone cement, BKP could promote the restoration of vertebral height and improvement of kyphosis more effectively, thus improving the stability of vertebral body and the functional status of patients. The findings of this meta-analysis suggested that BKP may be able to achieve superior result of functional improvement. Due to the small number of included trials in these comparisons, researches on functional improvement should be further performed. More independent high-quality RCTs reporting functional status evaluated by RMDQ or ODI with large sample sizes are still needed. EQ–5D is a scale for evaluating the quality of life. Compared with other life quality evaluating scale questionnaire such as SF-36, it focuses more on clinical relevance.46,47 By restoring vertebral height and improving kyphosis, PVP could be associated with improving life quality. However, considering that the number of trials reporting EQ–5D is relatively small, researches on life quality should be further performed. The imageology results in this meta-analysis suggested that VAP could be associated with no risk of new vertebral fracture. But the number of trials reporting new adjacent vertebral fracture is relatively small. And trials should be more specifically described when it comes to this kind of results, such as new vertebral fracture. Two trials describe new fractures in terms of the number of patients,25,38 while others describe new fractures in terms of the number of new fractures.19,20,23,24,27,31,33-35
During the analyses, we found when it came to the results related with Chinese-performed trials, the statistical heterogeneity exists. The reason could be associated with broad inclusion criteria and different baseline patients’ characteristic. The application of MRI imaging plays an important role in the diagnosis of OVCFs, including diagnosis of marrow edema and estimating the age of fracture. Seventeen trials21,23-38 explicitly reported the application of MRI imaging for diagnosis of osteoporotic vertebra compression fracture as one of the inclusion criteria in total included trials. And trials of Chen et al, 19 Chen et al 20 and Xie et al 22 failed to obtain this information. Inexact description of inclusion criteria might be another reason that the statistical heterogeneity existed in the results related with Chinese-performed trials. Therefore, in order to obtain more accurate clinical data for research and analysis, it is necessary to strictly control carefully describe the inclusion criteria, which will also help to confirm the optimal subset of patients with OVCFs for treatment of VAP.
This meta-analysis was performed to systematically compare the effectiveness and safety of VAP with NSM for the treatment of OVCFs. Many published studies have performed the comparison of the same topic with or without pure RCTs included. The advantage of this study is greater number of high-quality RCTs are available that compared VAP (PVP or BKP) and NSM (CT or sham procedure) allowing more accurate classification of interventions. And for confirming the suitable subset of patients with OVCFs for treatment of VAP, sub-analyses were performed based on types of osteoporotic fractures (from pure edema to complete destruction), location of fracture (vertebral level with fracture) and duration of back pain (pain duration of patients
Conclusion
In this meta-analysis, BKP is considered sufficient to achieve good clinical outcomes. PVP is associated with on beneficial effect on treatment of painful OVCFs compared with sham procedure. The optimal timing for VAP remains unclear based on existing data. The indication and timing of VAP need further research. More independently high-quality RCTs with sufficiently large sample sizes reporting careful patient selection, strict inclusion criteria and cost-effectiveness are needed.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_2192568221999369 - The Effect of Vertebral Augmentation Procedure on Painful OVCFs: A Meta-Analysis of Randomized Controlled Trials
Supplemental Material, sj-docx-1-gsj-10.1177_2192568221999369 for The Effect of Vertebral Augmentation Procedure on Painful OVCFs: A Meta-Analysis of Randomized Controlled Trials by Wei-Shang Li, Yun-Fei Cai and Lin Cong in Global Spine Journal
Footnotes
Abbreviations
Authors’ Note
WSL did study concept and design, data acquisition and interpretation, and drafted the manuscript; YFC did data acquisition and interpretation; LC did study concept and design, study supervision, and critical review of the manuscript. All authors reviewed the study findings and read and approved the final version before submission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (NO: 81 871 803). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.