
Abstract
Study Design:
Technical note, retrospective case series.
Objective:
The optimal surgical strategy for multilevel cervical ossification of the posterior longitudinal ligament (OPLL) with a negative kyphosis line (K-line (−)) remains controversial. We present a novel single-stage posterior approach that converts the K-line from negative to positive in patients with multilevel cervical OPLL, using a posterior thick cervical pedicle screw (CPS) system and report the procedure’s outcomes and feasibility.
Methods:
Twelve consecutive patients with multilevel cervical OPLL and K-line (−) underwent single-stage posterior thick CPS fixation, with laminectomy and foraminal decompression. A pre-bent rod was installed to convert the K-line from negative to positive. Radiographic parameters, including the extent and occupying ratio of OPLL and the C2-C7 angle, were examined. CPS accuracy was assessed using computed tomography. The Japanese Orthopaedic Association (JOA) and visual analog scale (VAS) scores were analyzed. Quality of life was assessed using the Neck Disability Index (NDI). The mean OPLL extent was 5 vertebral body levels, and posterior decompression was performed on 4.2 segments.
Results:
The average C2-C7 angle and the occupying ratio of OPLL improved from −9.0° to 14.3° and from 63% to 33%, respectively. The preoperative JOA, VAS, and NDI scores significantly improved from 8.4 to 13.3, from 7.1 to 2.2, and from 21.9 to 9.3, respectively. The K-line was converted from negative to positive in all cases. No severe complications were identified.
Conclusion:
Single-stage posterior surgery with a thick CPS system may be a reliable and effective treatment for multilevel cervical OPLL and K-line (−).
Keywords
Introduction
The incidence of the ossification of the posterior longitudinal ligament (OPLL) is high in the East Asian population. It can lead to cervical myelopathy and radiculopathy and requires surgical decompression. 1 Presently, several surgical strategies, such as anterior corpectomy with fusion, posterior laminectomy and fusion, and/or combined surgery, are used for OPLL treatment.1,2 Anterior surgery can directly resect the OPLL mass and result in superior recovery rates, especially for cases with OPLL over 1 or 2 levels, kyphotic alignment, and severe spinal cord compression. However, various complications are associated with anterior decompressive surgery, including neurological deterioration and cerebrospinal fluid (CSF) leakage.2,3 Meanwhile, posterior surgery is preferred in cases of lordotic alignment with multilevel involvement, as it has fewer complications and is technically less demanding. However, poor clinical efficacy in kyphotic and straight alignment originating from persistent compression of the anterior OPLL mass limits the clinical application of posterior surgery. 4
The kyphosis line (K-line), described first by Fujiyoshi et al. 5 in 2008, was defined as the line from the center of the canal of C2 to the center of the canal of C7. It was considered an important parameter for selecting the appropriate surgical approach for patients with cervical OPLL. Many studies have reported poor clinical outcomes in patients with a K-line (−) cervical spine who underwent single posterior decompression surgery due to the insufficient posterior shifting of the spinal cord.5,6 Hence, combined anterior and posterior surgery appears to be a prudent treatment for patients with multilevel OPLL with K-line (−). However, several studies have reported that combined surgery leads to longer operative and hospitalization durations, technical difficulties, extensive surgical trauma, and high cost.7-9 To avail the benefits of posterior surgery and avoid the shortcomings of anterior and/or combined surgery, we have designed a novel technique that is safe and effective for recovering K-line (+) via a single-stage posterior surgery for patients with multilevel OPLL with K-line (−) using a cervical pedicle screw (CPS) system. This study aimed to present a novel technique that converts the K-line from negative to positive in patients with multilevel OPLL using a posterior thick cervical pedicle screw system and to present the procedure’s outcomes and feasibility.
Materials and Methods
Patient Population
We retrospectively analyzed all patients with multilevel cervical OPLL (>3 vertebrae) and cervical kyphotic deformity (K-line (−)) who underwent posterior CPS system fixation with laminectomy with/without foraminal decompression from July 2011 to June 2019. The inclusion criteria were 1) preoperative cervical alignment with C2-C7 angle kyphosis and K-line (−); 2) cervical OPLL (>3 vertebrae) with cervical myelopathy, with or without radiculopathy; 3) maximal canal occupying ratio of more than 50%. Patients with continuous OPLL involving more than 5 vertebrae, dish syndrome in the cervical spine, and history of anterior cervical surgery were excluded. The type and segments of OPLL and cervical myelopathy were assessed using computed tomography (CT) and magnetic resonance imaging (MRI). Cervical mobility was evaluated by cervical dynamic lateral flexion and extension radiography. The postoperative CT and MRI scans were recorded before discharge. The pedicle screws were inserted under C-arm fluoroscopic guidance (in the first 4 patients) or navigation system (in the last 8 patients). Neuromonitoring was used in all patients.
During the study period, 14 patients underwent posterior CPS system fixation with laminectomy with or without foraminal decompression. Two patients with less than 1-year of follow-up were excluded. The remaining 12 patients included 8 men and 4 women (mean age, 61 years; range, 50-72 years). The patients’ demographic and clinical characteristics are summarized in Table 1. All patients were followed-up for a mean duration of 44 ± 26 months (range, 14-96 months).
Demographic and Clinical Data of the Patients.
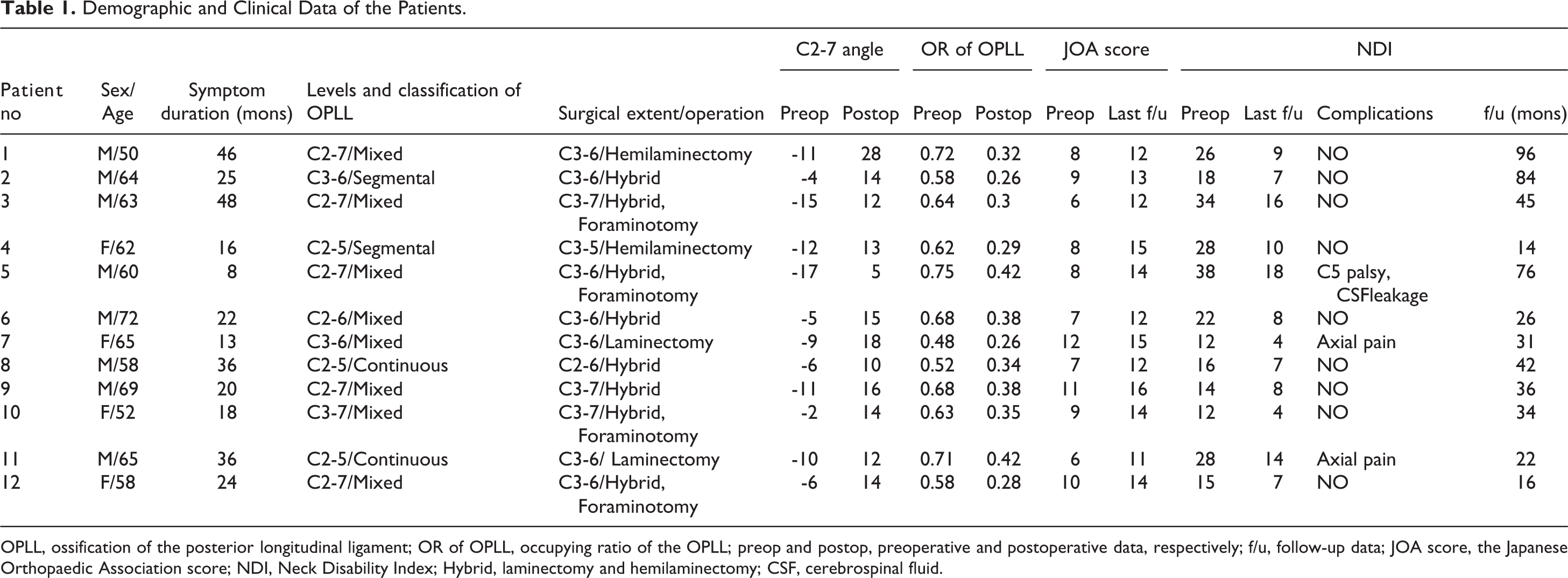
OPLL, ossification of the posterior longitudinal ligament; OR of OPLL, occupying ratio of the OPLL; preop and postop, preoperative and postoperative data, respectively; f/u, follow-up data; JOA score, the Japanese Orthopaedic Association score; NDI, Neck Disability Index; Hybrid, laminectomy and hemilaminectomy; CSF, cerebrospinal fluid.
Surgical Technique
After administering general anesthesia, the patient was positioned in a prone position. The cervical alignment was fixed with a Mayfield clamp with cervical neutral or slight flexion position to avoid worsening myelopathy. A posterior midline incision was created, and the paravertebral muscles were dissected laterally to expose lateral margins of the posterior elements of C2 to C7.
The entry point of the CPS was defined as the notch level in the sagittal plane and medial to the lateral border of the superior articular process by an amount of one-quarter of its width in the axial plane, which were slightly modified according to the sagittal and axial CT scan images of each patient. 10 Briefly, the entry points were exposed, and a pilot hole was bored using a 2-mm diameter high-speed burr. A small curved pedicle probe (2.5-mm diameter) was slowly inserted to find the path through the pilot hole. A ball tip feeler was used to confirm the integrity of the walls of the holes and the direction and insertion depth of the path. CPS insertions were guided by an O-Arm navigation system (Medtronic, Memphis, TN) in 2014 and after, whereas CPSs were inserted using the C-arm fluoroscopic guidance before 2014. For CPS insertion techniques using the O-Arm navigation system, a reference arc was placed onto the spinous process of C7. Then, a 3-dimensional intraoperative scan was performed, all the entry points of the CPS were marked with a high-speed bur, and a small pedicle probe was inserted into the pedicle under the single-level registration. For the freehand techniques, a small probe was inserted into the pedicle to confirm the direction and insertion depth, guided by the C-arm, under a lateral view. After tapping with a 3.5-mm diameter tap, the 4.0-, 4.35-, or 5.0-mm-diameter CPS (length, 18-26 mm; Expedium 4.5 system; Johnson & Johnson, New Brunswick, NJ, USA), which was selected based on preoperative measurements of axial CT image, was subsequently inserted.
Vertebral artery (VA) injury is a catastrophic complication related to CPS insertion. To avoid the VA injury, the inclination of the bony trajectory is one of the most critical parameters during the placement of CPS with the freehand technique. Two critical skills were required to achieve the proper inclination during the CPS insertion. First, the curved probe was used while creating a bone trajectory. As the medial wall of the cervical pedicle is the thickest and challenging to be penetrated by a pedicle probe, establishing the bony trajectory along the medial wall of the pedicle can minimize the VA injury. Second, for patients with strong paravertebral muscles, it may be necessary to create a muscle tunnel on the incision side to obtain a greater inclination angle. In addition, skipping a screw was also considered if a screw was certified to be outside the pedicle, and an adequate new track could not be created, or the pedicle diameter is < 3.5 mm on preoperative measurements of axial CT image.
After CPS insertion, posterior decompression procedures, including laminectomy, hemilaminectomy, or the hybrid method, were performed in the segments showing spinal canal stenosis with cervical cord compression on preoperative MRI. According to the type of OPLL protrusion, laminectomy was carried out if the OPLL mass is central, and hemilaminectomy was carried out if the OPLL mass is lateral. In the case of concomitant radiculopathy in the upper extremity and corresponding foraminal stenosis detected on preoperative MRI, posterior foraminotomy was performed by partially removing the inferior and superior articular processes to decompress the nerve root. After completing the decompression procedure, the Mayfield clamp was relaxed, and the cervical position gradually and softly transformed from neutral to extension; and, simultaneously, 2 pre-bent rods (Titanium alloy, 4.5 mm in diameter) were first installed and locked through the screw heads at the distal end. Then, the rods were pushed into the screw heads and gradually tightened using multiple tower reducers from the distal to the proximal. After cervical kyphosis was corrected by the excellent bony purchase of the CPS system (Figure 1), the Mayfield clamp was fixed again. Lateral view intraoperative fluoroscopy confirmed the cervical K-line conversion from negative to positive. The facet joints were bilaterally decorticated, and morselized cancellous autografts were placed over the decorticated area for arthrodesis.
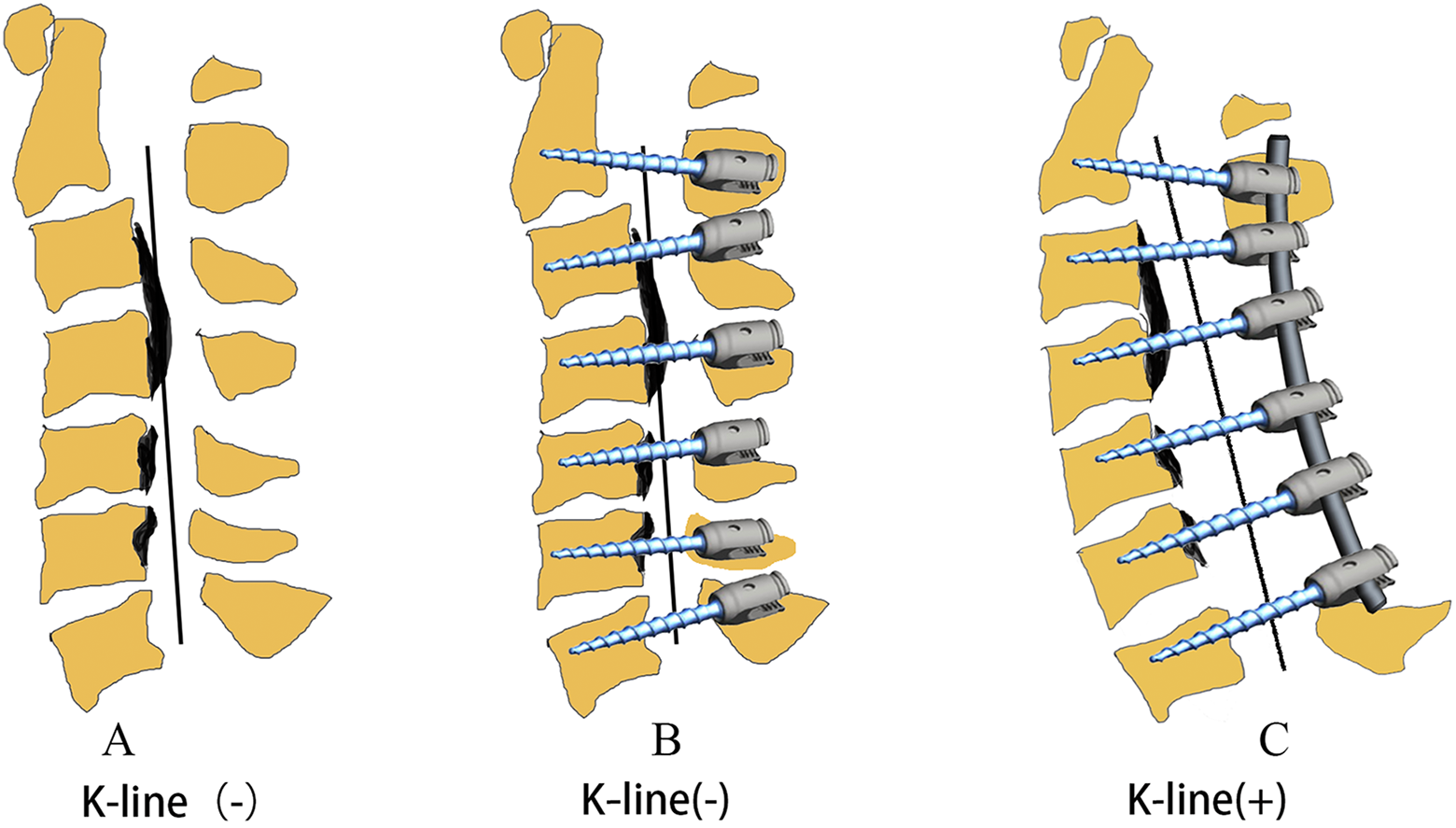
Three-dimensional images showing intraoperative manipulation for changing the K-line from negative to positive using the pedicle screw-rod construct. (A) K-line (−) with ossification of the posterior longitudinal ligament mass (black area). (B) Insertion of the cervical pedicle screws. (C) After decompression surgery, the K-line changed from negative to positive.
Radiographic and Clinical Measurement
The data on the number of posterior fusion levels, surgical time, intraoperative estimated blood loss (EBL), hospitalization period, and clinical complications (i.e., specific complications related to pedicle screw insertion) was obtained from the medical records. The radiographic parameters, including the extent of OPLL, occupying ratio of OPLL, and C2-C7 angle, were determined from the preoperative and postoperative radiographic data. The occupying ratio of OPLL (a/b×100) was calculated using the midsagittal OPLL thickness (mm) and canal diameter (mm) at the level of the maximal canal compromise. The posterior margin of the dura (mm) at the same level was used to calculate the postoperative occupying ratio (a′/b′×100) (Figure 2). 7 For functional assessment, the visual analog scale (VAS) score, the Japanese Orthopaedic Association (JOA) score, and Neck Disability Index (NDI) were recorded preoperatively and at the last follow-up. On the postoperative CT scans, screw placement accuracy was evaluated, as previously described:11,12 type I, ideal placement without cortical violation; type II, acceptable placement with less than half the diameter of the screw violating the surrounding cortex and less than 1 mm protruding from the anterior cortex; type III, unacceptable placement with a clear violation of the transverse foramen or spinal canal (Figure 3). The distribution and diameter of the pedicle screws were also reviewed and recorded.
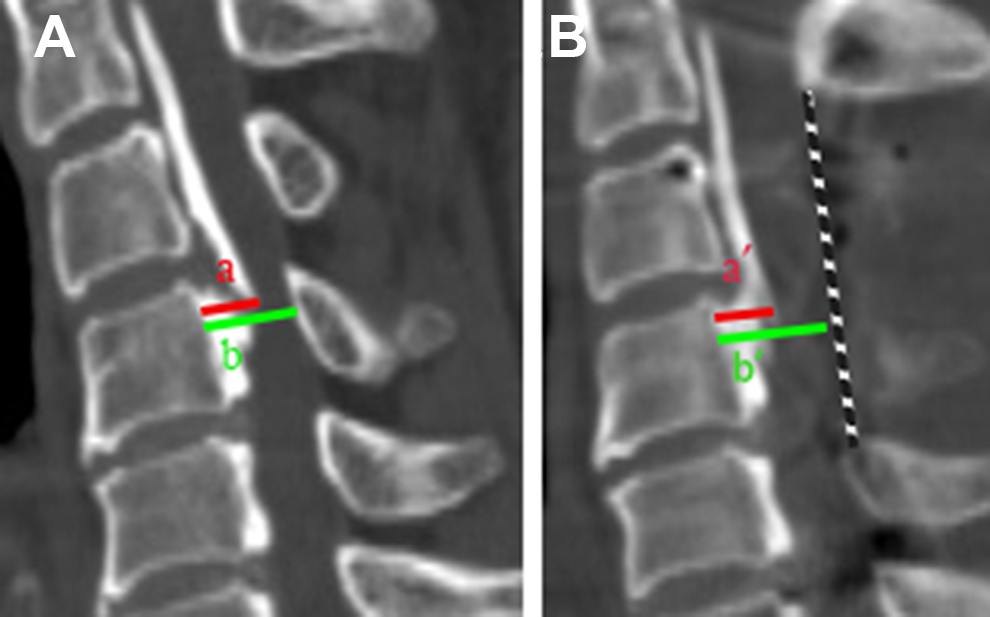
Occupying ratio of the ossification of the posterior longitudinal ligament (OPLL). (A) Preoperative occupying ratio (a = midsagittal OPLL thickness; b = canal diameter at the level of maximal canal compromise). (B) Postoperative occupying ratio (a′ = postoperative midsagittal OPLL thickness; b′ = distance between the posterior wall of the vertebral body and posterior margin of the dura).
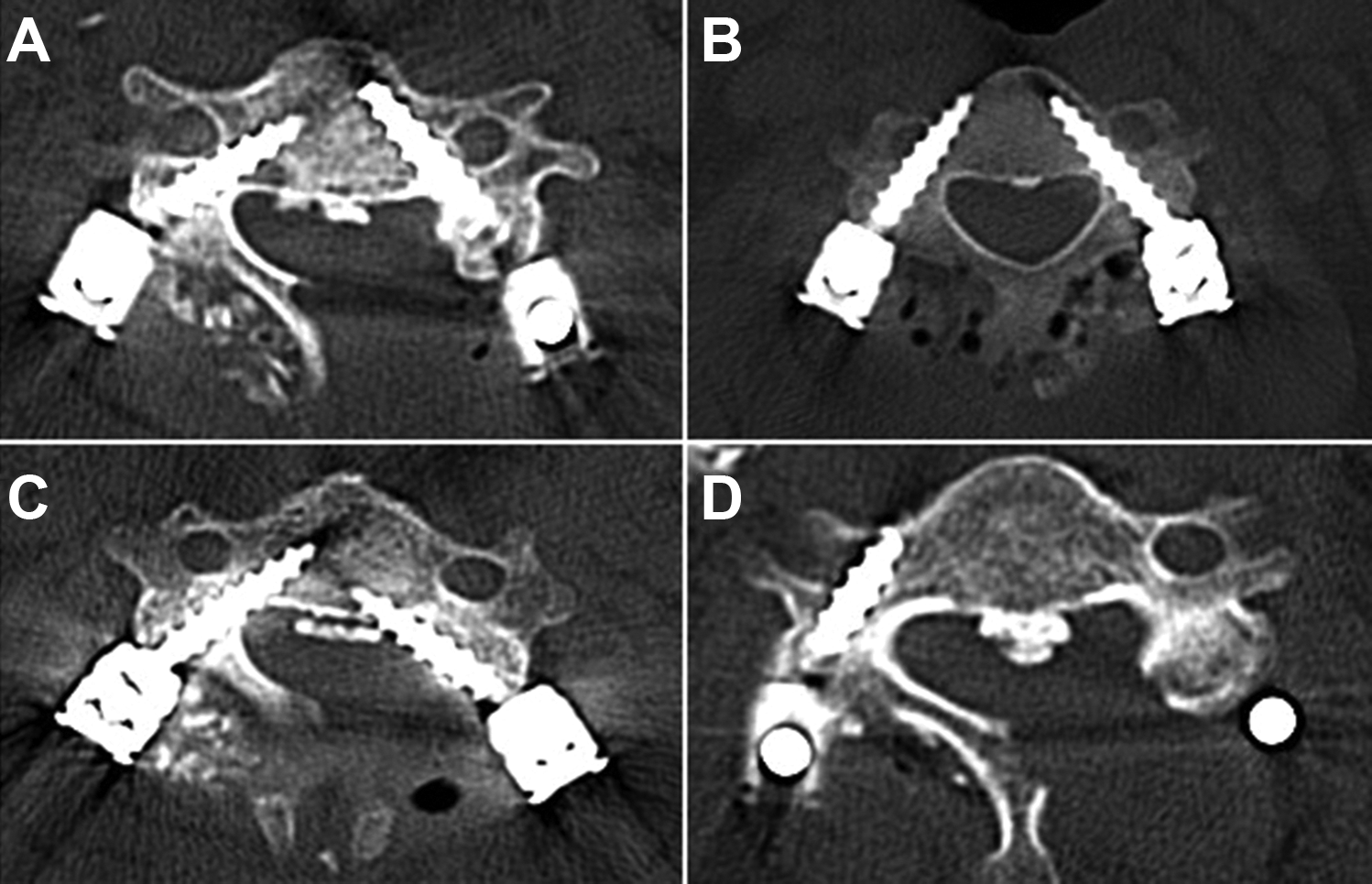
Axial computed tomography image: (A) Type I screws inserted bilaterally. (B) Type II screw on the right and type I screw on the left. (C) Type I screw on the right and type III screw on the left. (D) Type III screw on the right.
Statistical Analysis
SPSS Statistics for Windows, version 18.0 (SPSS Inc., Chicago, Ill., USA) was used for the statistical analyses. The Student’s t-test was used to determine the difference between the 2 groups. P values <0.05 were considered statistically significant.
Results
The hospitalization duration ranged from 8 to 15 days. The mean EBL and operative time were 240 mL (range, 160-450 mL) and 130 min (range, 110-210 min), respaectively. None of the patients received a blood transfusion. The mean extent of OPLL was 5 vertebral body levels, and the posterior decompression procedure was performed on a mean of 4.2 segments. All patients underwent CPS fixation of C2-C7 (excluding one patient who underwent CPS fixation of C2-C6) followed by laminectomy in 2 patients, hemilaminectomy in 2 patients, and the hybrid procedure in 8 patients. Four patients underwent foraminal decompression.
The average C2-C7 angle improved from −9.0° ± 4.3° preoperatively to 14.3° ± 5.2° at the last follow-up (P < 0.01). The occupying ratio of OPLL decreased from 63% ± 8% preoperatively to 33 ± 6% at the postoperative follow-up (P < 0.01). Compared with the preoperative scores, the JOA scores significantly improved from 8.4 ± 1.8 to 13.3 ± 1.5, VAS scores significantly decreased from 7.1 ± 2.6 to 2.2 ± 1.5, and NDI scores significantly improved from 21.9 ± 8.4 to 9.3 ± 4.3 at the last follow-up (P < 0.01). In all cases, the preoperative K-line (−) was converted to K-line (+) by the CPS system (Figures 4 and 5).
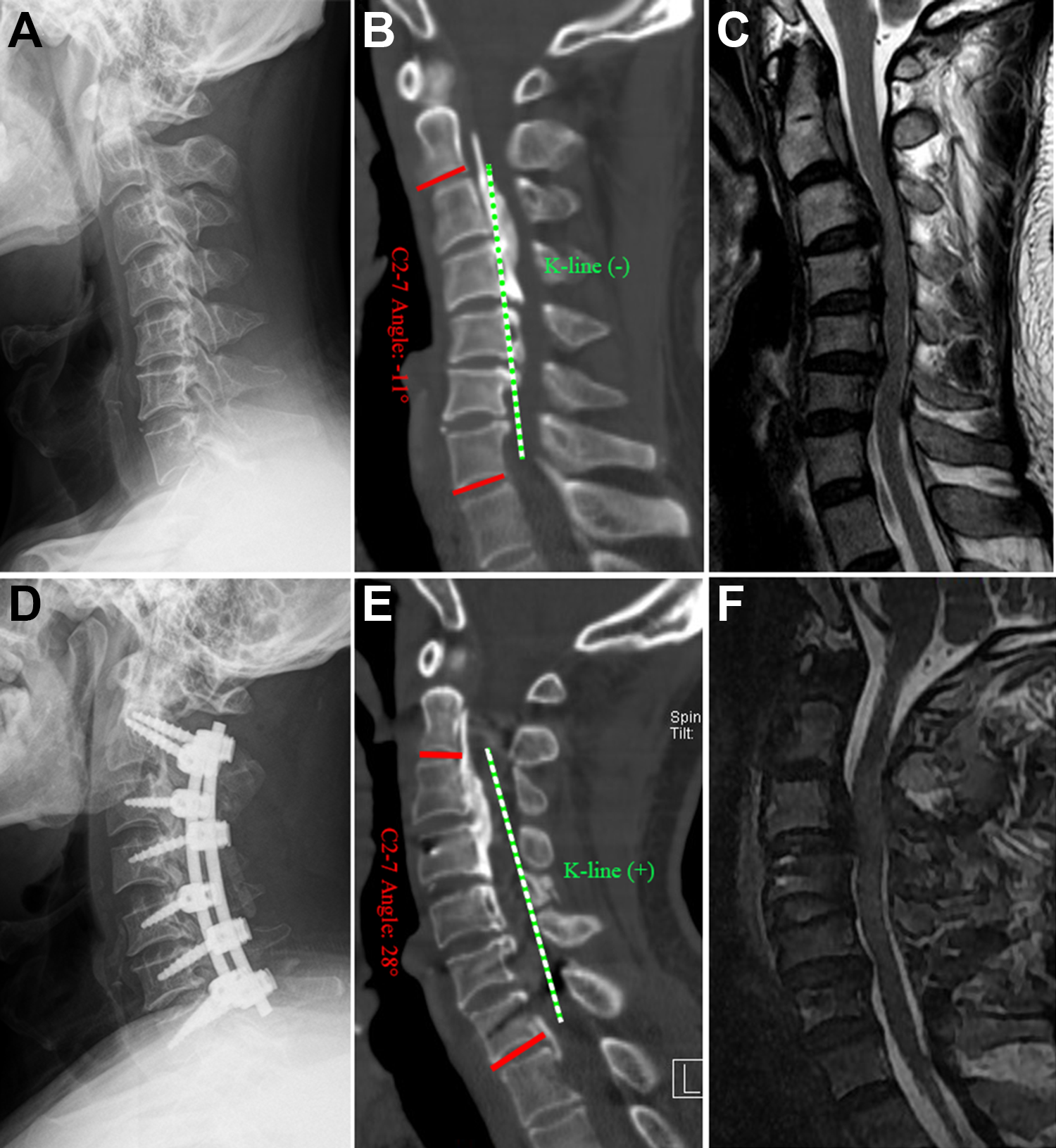
A 55-year-old patient with a multilevel posterior longitudinal ligament (OPLL) with K-line (−) underwent posterior decompression and fixation. (A-C) Preoperative images revealing cervical kyphosis with K-line (−), huge OPLL mass, and severe spinal cord compression. (D-F) Postoperative images revealing cervical lordosis curve with K-line (+) and sufficient spinal cord decompression.
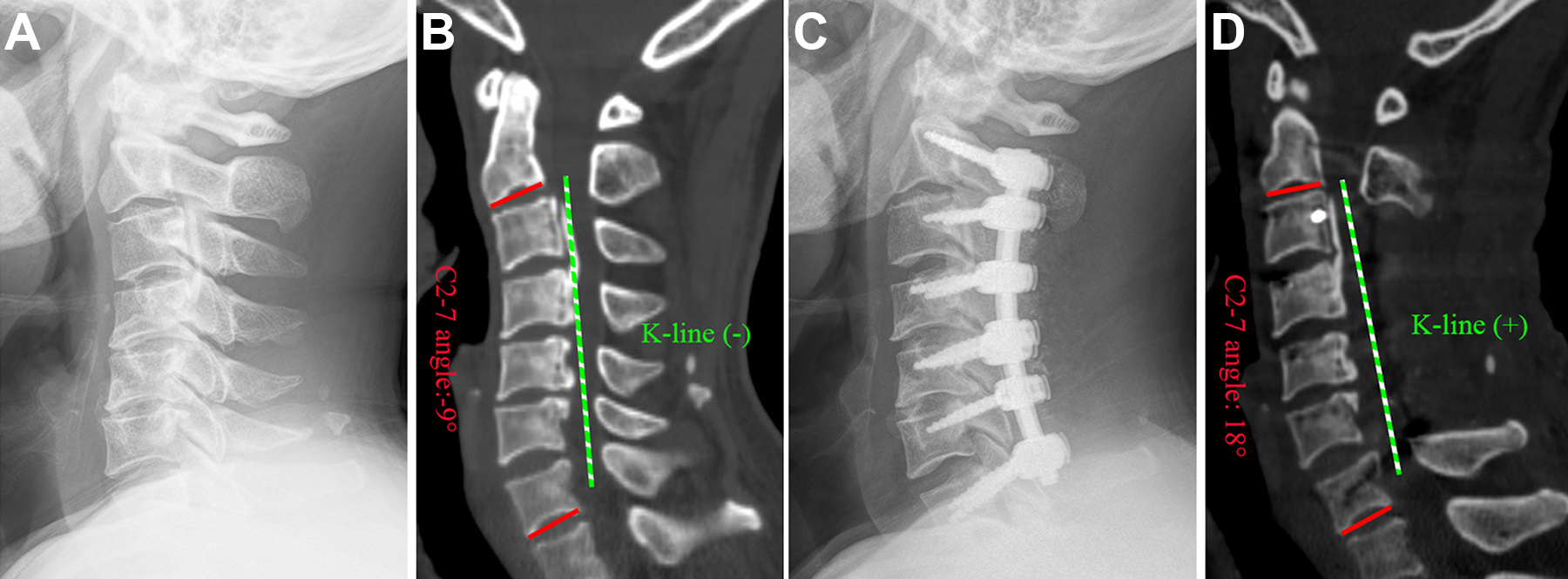
A 65-year-old patient with a multilevel posterior longitudinal ligament (OPLL) with K-line (−) underwent posterior fixation with laminectomy. (A and B) Preoperative images revealing cervical kyphosis and K-line (−) with multilevel OPLL. (C and D) Postoperative images revealing the cervical lordotic curve and K-line (+).
Among the 130 pedicle screws, 125 (96.2%) were deemed safe (type I or II); of these, 95 (73%) were rated as ideal (type I), and 5 screws (3.8%) were identified as unacceptable (type III; including violation of the transverse foramen in 3 cases and violation of the spinal canal in 2 cases; Figure 3). The accuracy, distribution, and diameter of the pedicle screws are shown in Table 2. Three patients (25%) experienced complications. Two patients experienced cervical axial pain after surgery that was effectively alleviated at 6 months postoperatively. One patient experienced C5 palsy, which resolved 9 months after surgery. A postoperative CSF leakage possibly caused from the damage by a burr during foraminal decompression was successfully managed by drain placement for 1 week. None of the patients required revision surgery due to screw malposition, implant failure and/or breakage, or deformity recurrence.
Accuracy, Distribution, and Diameter of the Pedicle Screws.
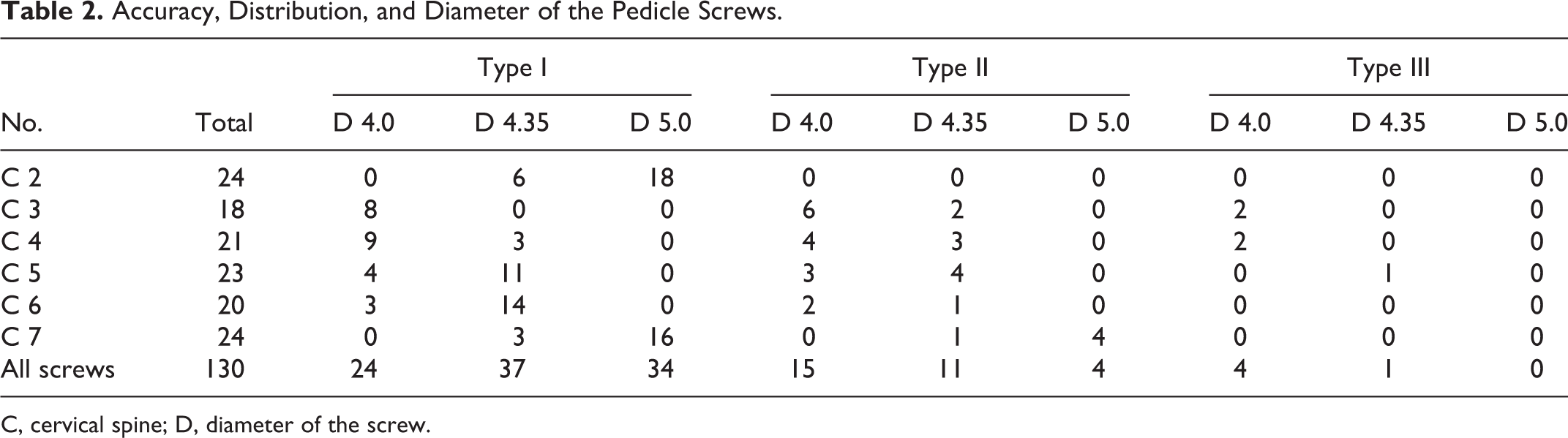
C, cervical spine; D, diameter of the screw.
Discussion
In the present study, we introduced a novel single-stage posterior approach that circumvents the disadvantages of a single anterior or posterior decompressive procedure to convert the K-line from negative to positive in patients with multilevel OPLL using a CPS system. K-line is an important preoperative parameter used for selecting the appropriate procedures and as a prognostic indicator of the surgical outcomes for patients with OPLL.2,5 If the K-line is negative in the OPLL patients, single posterior decompression surgery cannot obtain sufficient posterior shifting of the spinal cord and ideal surgical outcomes. Compared to the conventional Cobb angle, the K-line can theoretically reflect both cervical alignment and thickness of the OPLL mass, and thus, the surgical outcomes can be determined using one parameter.2,9 In addition, it should be noted that the K-line may be negative due to the protruding OPLL mass, even with lordotic and straight cervical alignment in the OPLL patients. Therefore, in the present study, we used the K-line, instead of the Cobb angle, to evaluate cervical alignment. The patients with multilevel OPLL with K-line (−) had poor functional outcome after posterior laminoplasty due to continued cord compression by the anterior OPLL mass.13,14 Accordingly, combined surgery was warranted. Thus, we introduced our technique of restoring cervical alignment by converting the K-line through a single-stage posterior procedure, thereby avoiding the shortcomings of anterior and/or combined surgery. In this technique, we applied the Expedium 4.5 system (Johnson & Johnson) as the CPS, which was originally used in thoracic and lumbar surgery in children and included 4.0-, 4.35- or 5.0-mm-diameter pedicle screws and 4.5-mm-diameter rods.
To change the K-line from negative to positive, anterior, or combined surgery in patients with multilevel OPLL is a logical choice. Previous studies reported that anterior decompression with fusion could facilitate direct decompression, reduce OPLL progression, restore lordotic alignment, and improve the outcomes in patients with multilevel OPLL.2,3 However, anterior surgery for multilevel OPLL is technically more demanding and is associated with a higher incidence of operation-related complications, including CSF leakage, spinal cord damage, instrumentation-related complications, and dysphagia. 15 Our results showed that the CPS-rod construct has an excellent ability to correct deformities and can provide durable stability for posterior fusion surgery with acceptable complication rates. We observed postoperative CSF leakage in one patient with preoperative radiculopathy in the upper extremity in the present study. Posterior CSF leakage is easier to treat, as the abundant paravertebral muscles provide protection. 2 Axial pain is the most frequently reported complication after posterior cervical surgery, with its incidence ranging from 16% to 48%.2,16,17 In our study, 2 patients reported axial pain, which was effectively alleviated at 6 months postoperatively, similar to that noted in previous reports.2,17 C5 palsy, another common complication of cervical laminoplasty, with incidence rates between 0% and 13.6%, may develop due to posterior decompression, leading to spinal cord shifting with resultant traction on the spinal cord and/or nerve roots. 18 In the present study, one patient who underwent hybrid decompression procedures and foraminotomy, with improvement of C2-C7 angle from −17.0° to 5°, had C5 palsy that was resolved at 9 postoperative months through rehabilitation.
Despite the higher risks associated with the proximity of these screws to the cervical spinal cord, VA, and nerve root, the subaxial pedicle screw fixation has been widely used to treat degenerative disorders and correct the cervical spine deformities because of the biomechanical stability and greater pullout strength of these screws. 19 To correct cervical deformities, the strength of the CPSs and rods should be high. Therefore, we first introduced the use of the Expedium 4.5 system with pedicle screw and rod of thicker diameter into the adult cervical spine, which can provide stronger pullout strength and a greater ability to correct deformities compared to the Mountaineer system (for upper cervical spine in adult, including 3.0- and 3.5-mm diameter pedicle screw and 3.5 mm diameter rod). In our series, 130 pedicle screws were placed in 12 patients using the fluoroscopy-guided freehand or navigation technique. Our results showed that most of the C2 and C7 screws have a 5.0 mm diameter, considering that the upper and lower screws were subjected to more stress. Although 5 (3.8%) of the 130 pedicle screws were rated as unacceptable (type III), no neurologic or vascular complications were detected on follow-up. A review of surgical records revealed that 2 unacceptable screws inserted with the navigation could be caused by the image-drifting due to the greater mobility of the cervical spine. Overall, 96.2% of the screws were deemed safe (type I or II), of which 73% were ideal or perfectly placed screws. Most type II and III screws were distributed at the C3 (n = 11) and C4 (n = 10) levels, which may be due to the smaller pedicle of C3 and C4. Our results showed a lower malposition rate compared to that reported previously, which ranged from 6.8% to 16% for the subaxial pedicle screws inserted using the freehand technique20,21; however, this may be related to the small sample size. In our study, all patients with type III screw malpositioning were postoperatively asymptomatic, and none of the patients required revision surgery to place the screws correctly. The most catastrophic complications occur due to screw malpositioning; therefore, intraoperative navigation (if available) should be used, as it can increase the accuracy and safety of screw placement. 22 Our results suggest that the Expedium 4.5 system can be safely and effectively used for correcting cervical deformities.
Our clinical results were satisfactory, and no major complications directly related to the use of subaxial pedicle screws were observed. In the present study, following the improvement in the C2-C7 angle and occupying ratio, we also observed significant improvements in the JOA, VAS, and NDI scores. According to our results, the hospitalization duration, EBL, and operative times were significantly reduced, compared to those reported previously for combined surgery recipients.7-9 Generally, it is difficult to correct the kyphotic angle of a continuous bridge of OPLL without breaking it, whereas the OPLL mass is always rigid. The type and extension of OPLL are the key factors in determining the usefulness of this procedure. In our series, mixed-type OPLL was observed in most cases, with only 2 patients having a continuous (C2-C5) type. Although the integral C2-C7 angle was converted from kyphosis to lordosis in these 2 patients, the improvements of the C2-C7 angle were mainly achieved via the “free” segments (C5/6 and C6/7) but not the affected segments (C2-C5) according to postoperative imaging. Hence, we excluded the patients with continuous OPLL involving more than 5 vertebrae. Although the K-line was converted from negative to positive in these 2 patients, as well as JOA and NDI scores, they were not as good as those in the other patients. Since there is no clarity on the optimal degree of correction for K-line (−) OPLL, the aggressive correction of kyphosis for K-line (+) should be avoided to prevent excessive complications. Therefore, further research is needed to evaluate the effectiveness of our novel technique for the treatment of patients with continuous-type OPLL. The preliminary results suggest that our novel technique is beneficial in posterior surgery and avoids the shortcomings of anterior and/or combined surgery for patients with multilevel OPLL with K-line (−). Since the new technique was performed in only 12 patients, further studies with larger sample populations and longer follow-up duration are required to evaluate the generalizability of the findings.
Conclusion
The novel technique introduced in this report is safe and effective for recovering K-line (+) in patients with multilevel OPLL using a single-stage posterior surgery with a thick CPS system. However, the procedure is technically demanding, and further studies with more cases are necessary to evaluate the procedure’s safety and generalizability.
Footnotes
Author Contribution
Yue-Hui Zhang, MD, PhD and Hai-Tao Liu, BS contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by the Ethics Committee of Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine. (Approval No. XHEC-D-2020-172)
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Shanghai Municipal Health Commission (No. 201 840 061).
Informed Consent
All patients involved in this study gave their written informed consent.