
Abstract
Study Design:
A retrospective study.
Objectives:
This study aimed to evaluate the safety and effectiveness of the bridge crane technique versus laminectomy for the treatment of thoracic myelopathy caused by ossification of the ligamentum flavum (OLF).
Methods:
Totally 41 patients who underwent surgical decompression due to thoracic OLF from May 2017 to June 2018 in our institution were enrolled in this study and were divided into group BG (bridge crane technique, n = 19) and group L (laminoectomy, n = 22). Demographic data was collected from medical records and the modified Japanese Orthopaedic Association (JOA) scoring system was used to evaluate the neurological outcomes during the follow-up. Surgery-related complications were analyzed.
Results:
The mean duration of follow-up was comparable between group BG (19.4 ± 1.5 months) and group L (19.6 ± 1.4 months). No statistical differences were observed between two groups in terms of gender, age, duration of symptoms, preoperative occupying rate, involved levels, operation time, intraoperative blood loss, and complications. The JOA score significantly increased at the final follow-up in both groups. However, patients in group BG had higher JOA score and recovery rate (P < 0.05). Four patients in group L experienced complications, including 3 cerebrospinal fluid (CSF) leakage and one postoperative hematoma. Only one patient in group BG had CSF leakage.
Conclusion:
The results of this study suggested that bridge crane technique may be relatively safe and effective for patients with symptomatic thoracic OLF with more satisfactory clinical improvement. However, high-quality studies are still required to validate the results of this study.
Keywords
Introduction
Ossification of the ligamentum flavum (OLF) is a clinically rare disease, resulting in compression of the spinal cord and ensuing neurological dysfunction, and this disorder has been characterized by the replacement of ligamentum flavum tissue by the heterotopic ossification. 1 OLF has been almost exclusively occurred in East Asian population, with overall prevalence of 36% in Japanese patients and 63.9% in Southern Chinese population.1,2 Notably, OLF at thoracic spine is one of the major causes for thoracic myelopathy and the lower thoracic spine is the highest affected region. 3 Patients with thoracic OLF frequently exhibit symptoms such as muscle weakness or numbness and various degrees of difficulty walking after onset (within 2 years), sensory dysfunction in the lower limbs, neurogenic bladder and bowel, and even complete paraplegia.1,2 However, the diagnosis of thoracic OLF is usually delayed due to its insidious onset and slow progression at early stage. In addition, patients with symptomatic thoracic OLF frequently show no response to conservative management. 4 Therefore, surgical intervention has been advocated.
The objective of surgical treatment is to release the compression of the spinal cord and to maintain its stability and posterior decompression is mostly recommended.1,2,5 Laminectomy including piecemeal laminectomy and en bloc laminectomy can achieve direct spinal cord decompression via resection of the lamina and ossified ligamentum flavum. 5 However, due to the limited operator’s field of vision, iterative entry of the Kerrison rongeur into the spinal canal could increase the risk of spinal cord and nerve root injury during piecemeal laminectomy. 6 In clinical practice, en bloc laminectomy frequently uses high-speed drill rather than only Kerrison rongeur, which can in part reduce the risk of damaging the cord compared to piecemeal laminectomy.6,7 However, the usage of high-speed drill and the performance of the en bloc resection of the lamina and the ossified lesion are technically demanding. 7 In addition, the long operation time and high intraoperative blood loss are also attention-required issues in treating multilevel thoracic OLF.8,9 In addition, multilevel laminectomy may cause thoracic kyphotic deformity, which could result in late-period neurological deterioration.8,10
The concept of avoiding manipulation of the surgical instruments inside the spinal canal to reduce the potential compromise to the patients is not new. 7 Based on clinical practice, a novel technique, the bridge crane technique, was proposed for the treatment of patients with thoracic OLF via isolating and elevating the lamina-OLF complex (LOC) en bloc posteriorly without inserting any instrument into the spine canal and acquired satisfactory outcomes. 11 However, there is no study published to investigate whether the bridge crane technique is superior to laminectomy.
In this study, we aimed to assess the safety and effectiveness of the bridge crane for patients with thoracic myelopathy caused by OLF compared to laminectomy.
Methods and Materials
Patients Population
This study was approved by the institutional review board of our hospital (IRB: 2017SL040), and all the authors of this study complied with the related requirement of the institutional review board of our hospital. From May 2017 to June 2018, all patients with a diagnosis of thoracic OLF who underwent the bridge crane technique or laminectomy in our institution were reviewed respectively. The diagnosis of thoracic OLF was confirmed by the patients’ manifestations and preoperative imaging including X-rays, MRI, and CT scanning. The sample size in each group was determined by the number of eligible cases during the study period. The inclusion criteria and exclusion criteria are as follows. In fact, these criteria have been also the routine consideration for surgery in our clinical practice during we evaluate the patients.
The inclusion criteria were 1) those presented with typical symptoms of thoracic myelopathy caused by OLF (mainly including limb numbness, impaired motor function, and unsteady gait); 2) those without neurological symptoms resulting from spina cord compression of cervical or lumbar spine; 3) those with neurological symptoms consistent with radiological examination; 4) those with a general condition allowing staged surgical interventions; 5) those treated with bridge crane or laminectomy only.
The exclusion criteria were: 1) those with concurrent thoracic ventral compressive lesions, such as thoracic lumbar disc herniation; 2) those presented with other tandem spinal diseases such as spinal deformity that needed operative treatment;
with thoracic tumor, infection, trauma; 2) with previous thoracic surgery; 3) with clinical symptoms resulting from cervical or lumbar degenerative disease without complete follow-up data; 4) those having neurologic diseases such as Parkinson, Alzheimer, dementia, and so forth;5) those with diabetes or other metabolic diseases without regular treatment and well control; and 6) those with a history of psychosis or alcoholism or drug addiction.
Clinical and Radiological Assessment
All patients were followed-up at least 12 months after surgery. The Modified Japanese Orthopaedic Association (JOA) score for thoracic myelopathy by excluding the upper extremity scores were used to evaluate neurologic function.4,7 The maximum score of 11 indicates normal function, and the recovery ratio of the JOA score was calculated as follows: (final JOA score—preoperative JOA score)/(11-preoperative JOA score) x 100%. 12 Similar to the RR of JOA score for cervical myelopathy, surgical outcome was defined by RR as follows: excellent (RR ≥ 75%), good (75% > RR ≥ 50%), fair (50% > RR≥ 25%), and poor (RR < 25%). 12 Demographic data, intraoperative blood loss, operation time, and surgery-related complications during the follow-up were also evaluated. All patients underwent X-rays, MRI, and CT scanning before and after surgery. Occupying ratio of the spinal canal was defined as the thickness OLF to anteroposterior diameter of bony spinal canal at the most compressed level on the axial CT. Also, number of levels involved and the distribution of OLF were analyzed.
In this study, to minimize the measurement error, the occupying ratio was measured independently by 3 surgeons. In fact, each surgeon was required to measure and calculate the occupying ratio for 3 times, and each time had a 1 week interval. If there was statistically significant difference among the 3 measurements for the same surgeon, the parameter would be measured again. The average value of all 3 times was defined as the exact value of occupying ratio by the same surgeon. Finally, the mean value of all the average values by the 3 surgeons was defined as the exact value of occupying ratio for analysis. We have added this description in our new manuscript.
Surgical Technique
All patients were treated by the spine surgeons from the same surgery team who had at least 5-year experience of spine surgery in our spine center. In fact, all patients, including those treated by these 2 techniques, would be informed of the surgical details and potential benefits and risk before surgery. However, although the acceptance of patients would be considered, the final decision of the surgical technique was mainly determined by surgeons’ experience after comprehensive evaluation of patients’ physical conditions. The purpose of this paragraph was to present the routine preoperative item in our institution for patients who would require operation.
The procedure of laminectomy has been reported previously.3,9,13 Briefly, after the resection of the spinous processes at affected segments, the laminectomies were performed using high speed drill, with the range of 1 or 2 laminae superior and inferior to the diseased segment in addition to the medial one-third to one-half of the facet joint. In cases with dura ossification, the ossified portion was floated without being totally resected to avoid tearing the dura mater. If the dura defect was confirmed intraoperatively, the repairment would be performed.
The bridge crane technique has been described previously. 11 The procedure was illustrated in Figure 1, as well as the intraoperative photos in Figure 2. Briefly, 2 longitudinal bony incisions were firstly made bilaterally at the medial margin of the pedicles on the laminae. The longitudinal osteotomy incisions were made to the lateral of the ossification lesion and to the medial of the bilateral pedicles with the width of about 2 mm. Due to the similarity of bilateral slotting in the bridge crane technique to traditional en bloc laminectomy, the isolation procedure of the lamina-ossified mass complex (LOC) is safe. In addition, when the dura underneath the OLF is ossified, wider exposure of the lesion is recommended. Subsequently, the spinous processes of the involved laminae were then excised gently to facilitate further posterior suspension of the LOC. Holes at 5 mm to the midline of the base of the spinous processes bilaterally were made at the every level of OLF with a stay prolene suture (0#, Ethicon Inc., USA). A transverse incision was then made at the lowest affected lamine to connect the bilateral longitudinal incisions. Next, bilateral pedicle screws were placed with the installation of 2 longitudinal rods and 2 transverse connectors to serve as the “bridge” for further evaluation of LOC, and slipknot was made to tighten the stay prolene sutures onto the corresponding transverse connectors. Subsequently, the second transverse incision was made at the upmost affected lamina. After complete isolation of LOC, tightening of the stay prolene sutures was conducted in a gradual process to facilitate the posterior suspension of the LOC, and improved pulsation of the LOC along with the dura pulsation frequently indicated a good decompression and can be observed. Finally, The LOC was then fixed onto the 2 transverse connectors with the stay prolene sutures by tying surgical knots above the original slipknot, and posterior fusion was then carried out between bilateral longitudinal incision. The fascia and skin were then sutured layer-by-layer with a wound drain remained. Standard antibiotics were used to prevent infection. Patients in both groups received an atmospheric drainage tube for 3 days. Neurophysiologic monitoring involving somatosensory-evoked potentials (SSEPs) and motor-evoked potentials (MEPs) was utilized to predict the postoperative neurologic deficit.
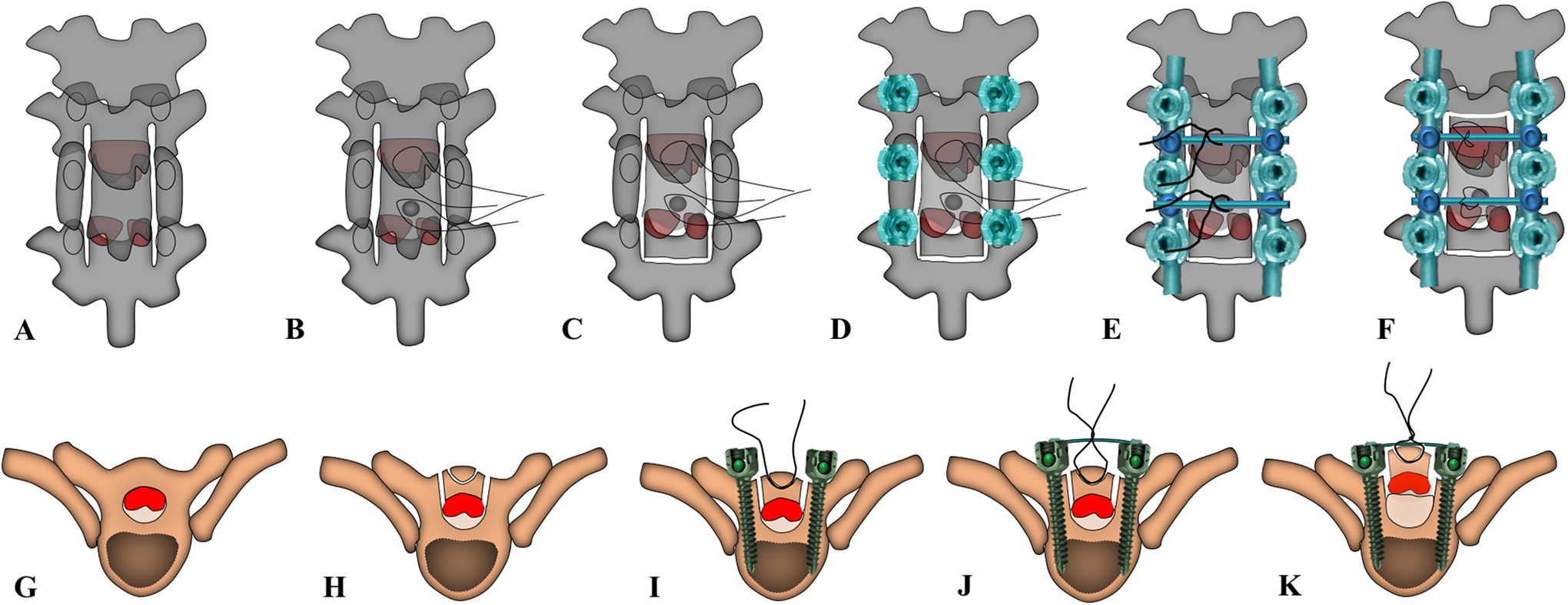
Illustration of the procedure of the bridge crane technique. A, Two lateral longitudinal bonyincisions were made at affected segments. B, A tunnel was made with a stay prolene suture at each affected levels. C, The first transverse bony incision was made at the pedicle level of lowest lamina. D and E, Pedicle screws were then placed bilaterally, affixed with 2 longitudinal rods and 2 transverse connectors. F, Two slipknots were made, followed by the second transverse incision made at the pedicle level of uppermost lamina to complete the isolation of the LOC en bloc. G, Excision of the spinal proce. H, Two lateral longitudinal bony incisions were made with a stay prolene suture. I, Placement of pedicle screws. J, Establishment of slipknot. K, The evaluation of the LOC and establishment of surgical knots. LOC, lamina-ossified ligamentum flavum complex.
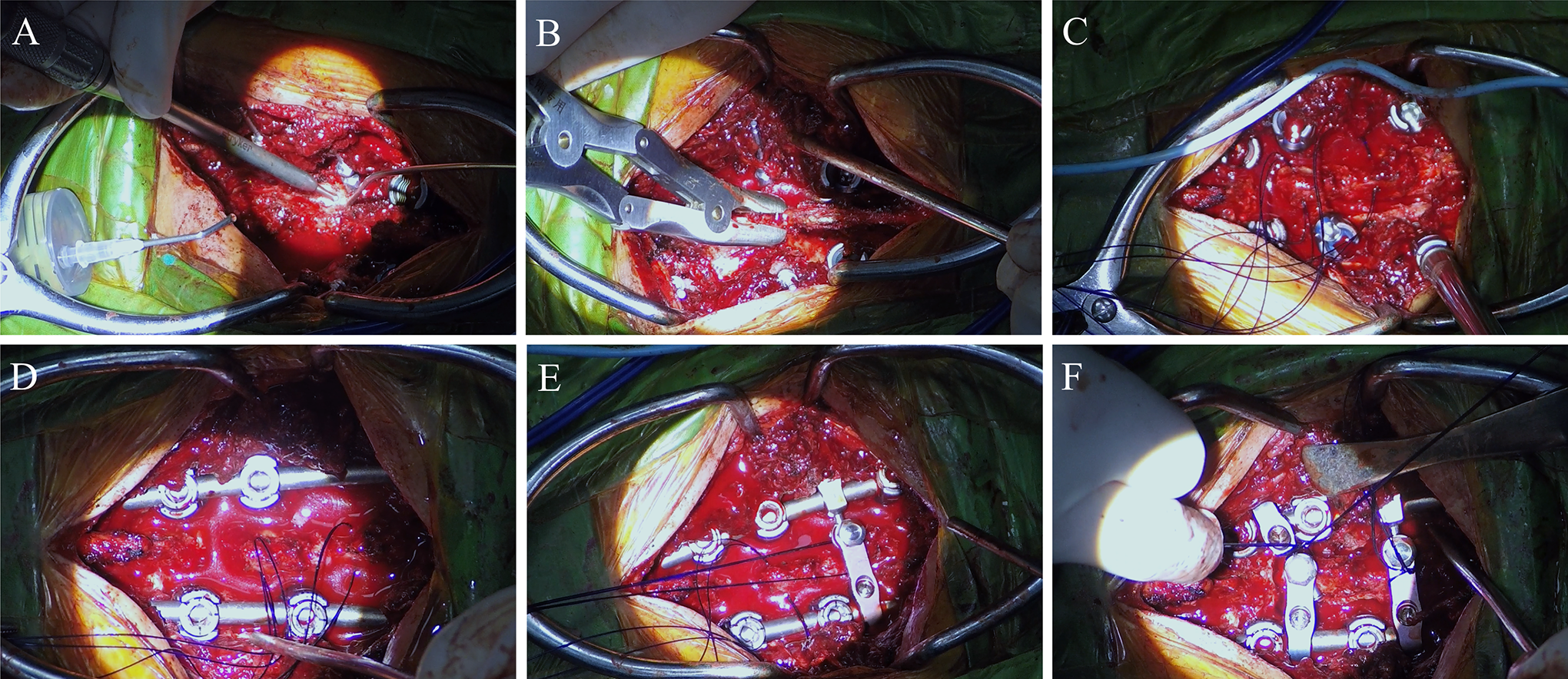
Intraoperative photos of the bridge crane technique. A, Establishment of 2 longitudinal bony incisions bilaterally at the medial margin of the pedicles on the laminae. B, Partial resection of the spinous process at affected segments. C, Installment of pedicle screws, with a stay prolene suture going through the base of remaining spinous process. D, Installment of bilateral longitudinal rods. E, Fixation of transverse connector. F, Posterior elevation of the lamina-ossified mass complex (LOC).
Notably, comprehensive preoperative design is extremely critical. Careful measurement and assessment of the thickness of OLF on axial CT are required, which determines the degree of posterior isolation of LOC. To confirm the efficiency of preoperative design for isolation, in our initial practice of the bridge crane technique, intraoperative CT is required to validate that the decompression is sufficient. After a period of clinical practice, we found that decompression based on the design of preoperative CT is effective to decompress the spinal cord. Therefore, currently, we do not include intraoperative CT as a routine item to confirm that the decompression effect. Rather, a intraoperative C-arm fluoroscopy is still used to confirmed the good position of the rods and screws.
Statistical Analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (Version 20.0; IBM Corp., Armonk, New York, USA). Variables were measured as mean ± standard deviation (SD). The Chi-square test was used in the comparisons of the categorical variables, such as age, sex, involved levels, and complications between the 2 groups. Mann-Whitney U test was used for the other data, such as operation time, blood loss, and JOA score between the two groups. Differences were considered statistically significant at P < 0.05.
Results
Demographic Data of Patients
Demographic data of the patients in this study was shown in Table 1. No significant differences were observed between the two groups in terms of age, gender, duration of the symptoms, surgical levels, duration of the follow-up, and intraoperative blood loss. Based on the selection of surgical decompression, patients in this study were divided into group BG (the Bridge Crane Technique) and group L (laminectomy). There were totally 19 patients in group BG (12 male and 7 female) and 22 patients (12 male and 10 female) in group L. The average age of patients was 55.3 ± 2.5 years (rage 37-77 years) in group BG and 57.8 ± 2.2 years (rage 43-77 years) in group L (P > 0.05). The mean preoperative duration of symptoms from onset of initial symptoms to surgery in group BG was 28.2 ± 1.5 months, and in group L the duration was 26.9 ± 1.4 months (P > 0.05). The mean duration of follow-up was 19.4 ± 1.5 months and 19.6 ± 1.4 months in group BG and group L, respectively (P > 0.05). The mean duration of follow-up was 19.4 ± 1.5 months and 19.6 ± 1.4 months in group BG and group L, respectively (P > 0.05). No significant difference was observed in terms of preoperative occupying rate, duration of follow-up, operation time, complications, and surgical levels between 2 groups (Table 2). In addition, of these patients, the most affected segments were the lower thoracic spine in both groups (Figure 2).
Demographic Data of Patients in This Study.
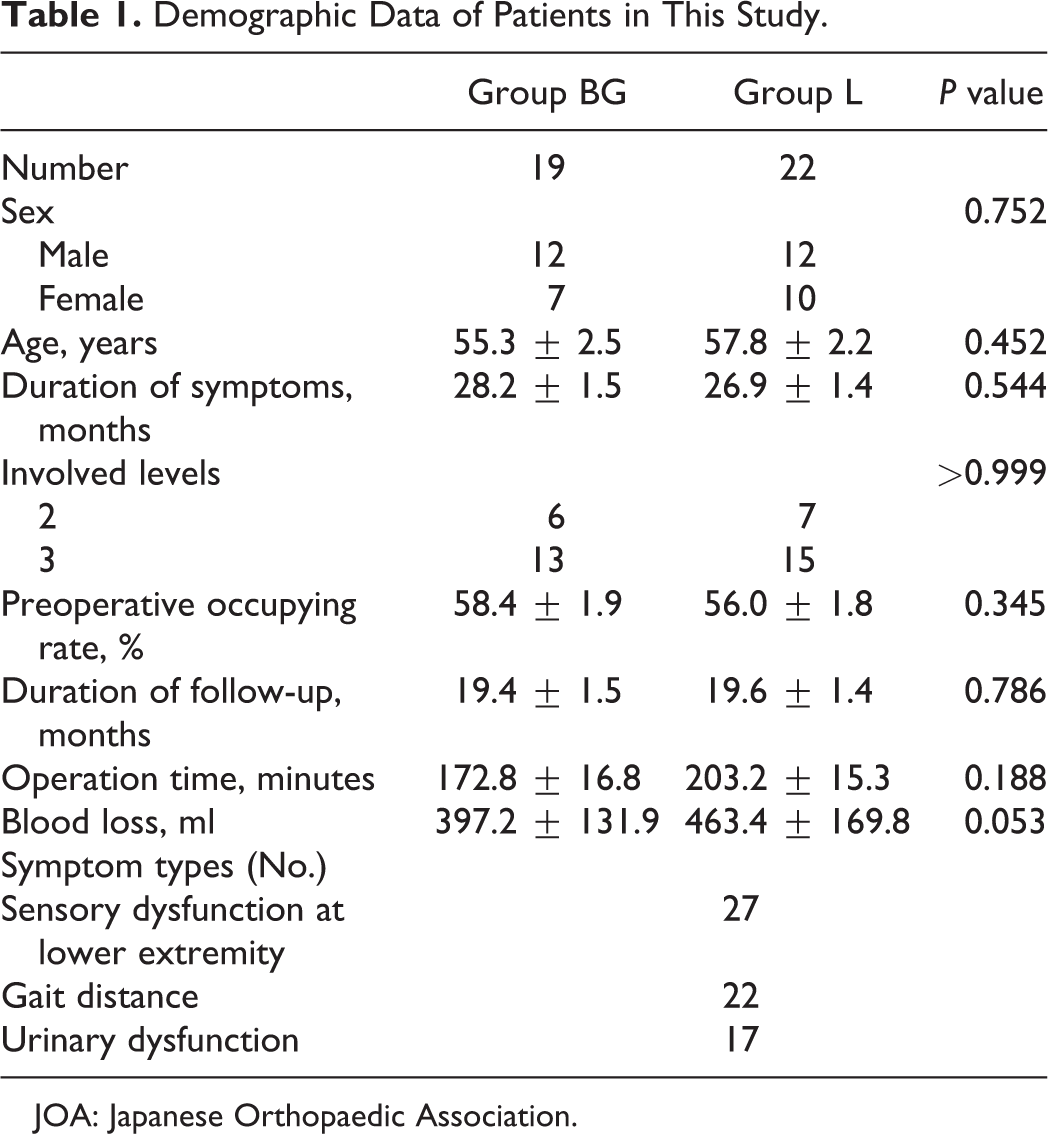
JOA: Japanese Orthopaedic Association.
Clinical Outcomes of Patients in This Study.
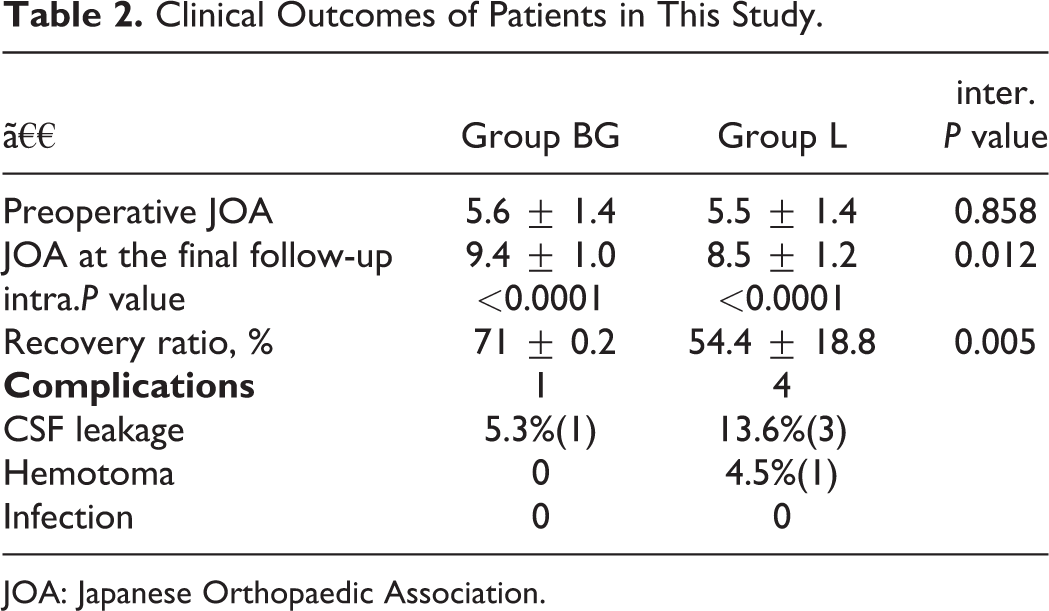
JOA: Japanese Orthopaedic Association.
Clinical Outcomes
The mean preoperative JOA score of patients in group BG was 5.6 ± 1.4 and in Group L the JOA score was 5.5 ± 1.4 (P > 0.05) (Table 2). However, at the final follow up, patients treated by the bridge crane had better JOA score (9.4 ± 1.0) than those who underwent laminectomy (8.5 ± 1.2) (P < 0.05). In addition, patients in group BG had higher recovery rate of JOA score (71% ± 20% vs 54.4% ± 18.8%) (P < 0.05). Figure 3 also showed the patients in group BG had better recovery of neurological function and less intraoperative blood loss (Figure 4).
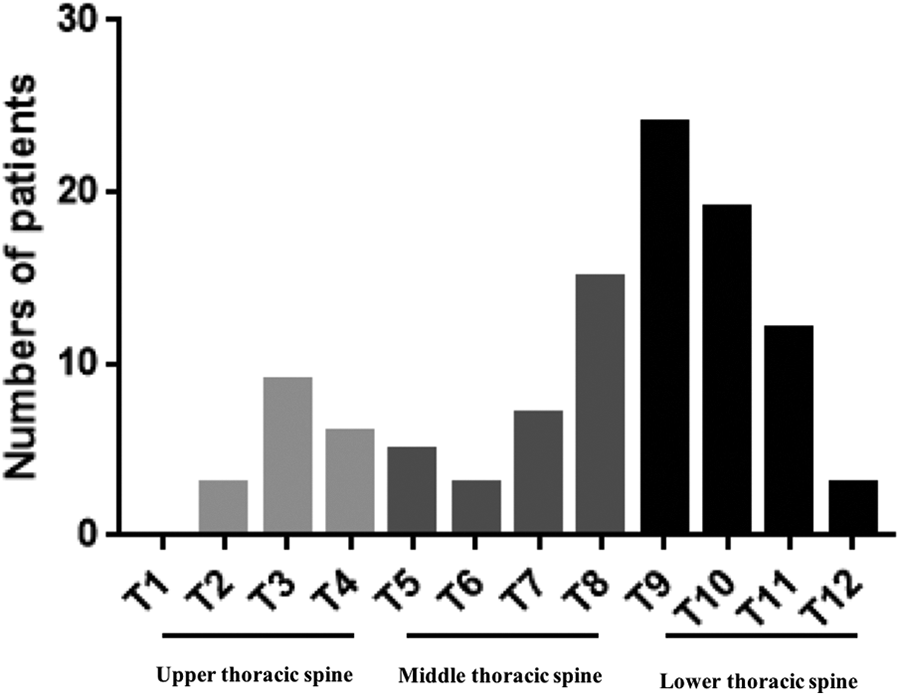
Distribution of OLF at thoracic spine in this study. OLF: ossification of the ligamentum flavum.
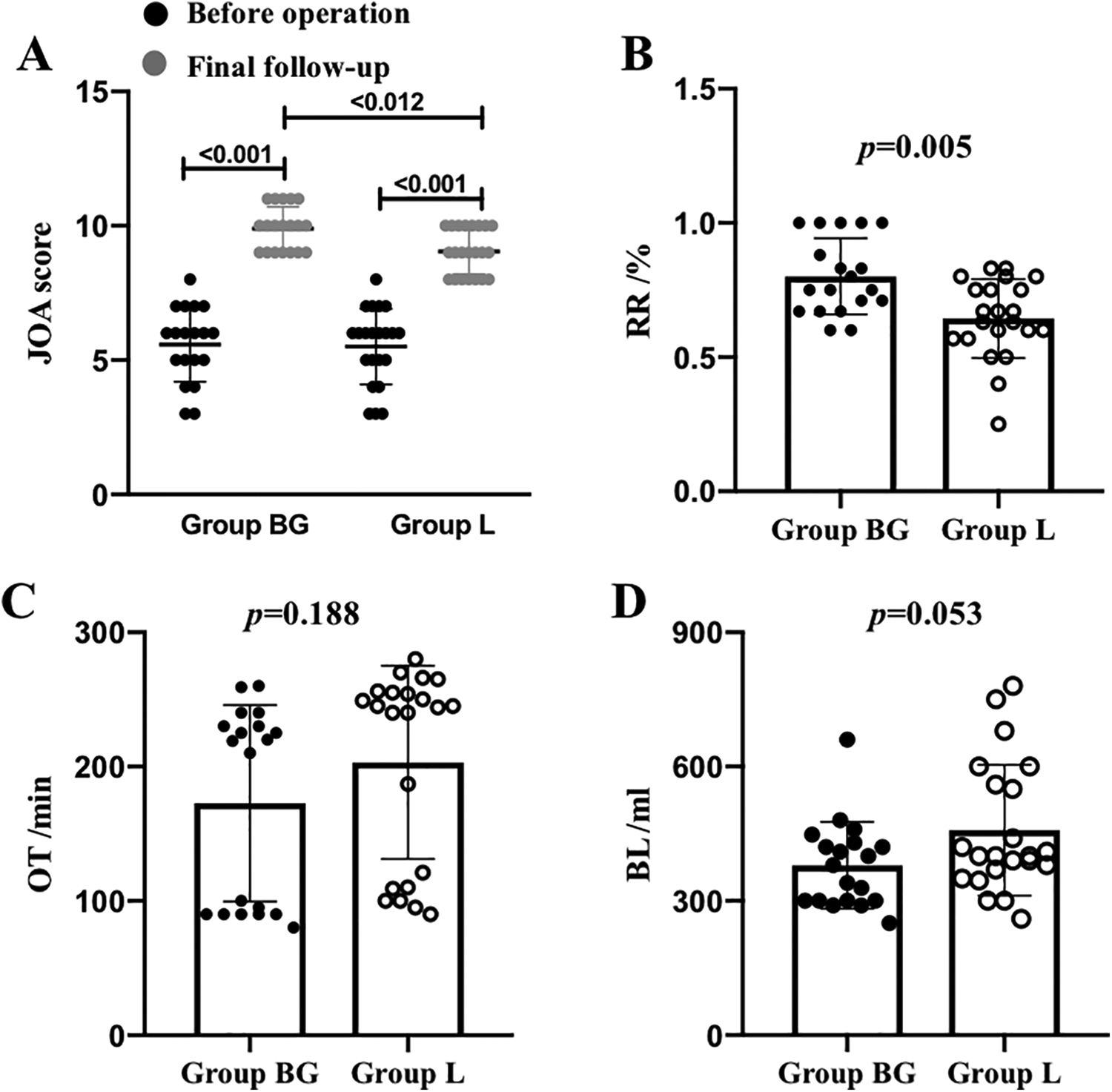
Surgery-related results between two groups. A, JOA score between two groups before surgery and at the final follow-up. B, Recovery rate of JOA between two groups at the final follow-up. C, Operation time between two groups. D, Blood loss between two groups. JOA, Japanese Orthopaedic Association. RR: recovery rate; OT: operation time; BL: blood loss.
Complications and Managements
All patients were required to bedrest after the operation for appropriate period according to their physical condition (generally ranging from 3 days to 1 weeks). In fact, not all patients were asked to stay in bad for more than 1 week, only for those whose physical conditions were not satisfactory, such as lower immunity. However, for the most patients in this study, nearly 3 days after operation, they would be encouraged to accept early ambulation for immediate rehabilitation exercise and lower postoperative complications.
Cerebrospinal fluid (CSF) leakage was the main perioperative complication in thoracic decompression surgery. Three cases in group L was found to have ossified dura mater and ensuing CSF leakage during removal of OLF adhered to the dura mater. However, only one patient in group BG had CSF leakage, although the difference was not significant. However, the higher rate of CSF leak in group L may be related to other potential factors rather than just the laminectomy. Therefore, studies with larger sample and higher statistical strength will be required.
No significant difference was observed between the two groups regarding complications. In this study, for those with CSF leakage, the dura mater repair was performed, with a drainage tube in 12 hours after operation, and continuous pressure was required. These 4 patients had resolution of all CSF leakage-related signs and symptoms within 2 weeks. There was also one patient in group L had neurological deterioration in his lower extremities muscle strength due to postoperative hematoma 5 hour after operation. However, he acquired good recovery after immediate evacuation of the hematoma, diuresis treatment, and dexamethasone therapy.
There was no patient with wound infection, kyphotic deformity, or recurrence of ossification at the operated segments in both groups during the follow-up.
Discussion
Thoracic OLF has been a disease developing slowly and insidiously, and patients with myelopathic symptoms frequently exhibit severe spinal cord compression. 14 In this present study, OLF occurred mostly at lower thoracic segments, which was consistent with previous studies.15,16 Anatomically, the predominance of OLF at the lower thoracic spine is thought to correlate with the transitional segment between the end of the rib cage and the thoracolumbar junction resulting in less anatomical protection from the rib cage, increased motion, and microtrauma to the ligamentum flavum. 17 The major symptoms for patients with thoracic OLF include sensory dysfunction in the lower extremities or trunk, lower limb dyskinesia, and sphincter disturbance. 2 In this present study, 27 patients complained of sensory numb or pain at lower extremity, 22 patients had gait distance of varying degrees, and 17 patients suffered urinary dysfunction. These neurological deficits fitted indications for surgery (Table 1).
Thoracic OLF frequently results in chronic compression to the spinal cord and subsequent neurologic deterioration.18,19 Therefore, immediate surgical decompression is generally suggested. Posterior laminectomy has been widely performed previously. 6 However, the manipulation inside the spinal canal using Kerrison rongeur may increase the risk of spinal cord injury. In addition, for cases with multilevel OLF, the potential instability after surgery especially at cervicothoracic or thoracolumbar junction may cause late-onset thoracic kyphotic deformity and even reoccurrence of OLF. 20 Therefore, the spinal fusion with instrumentation was advocated to reduce the focal mechanical stress.9,18 A retrospective study by Jia et al recommended en bloc laminectomy for thoracic OLF in which the lamina and the ossified mass was excised as a whole and acquired good recovery of the neurological outcomes using JOA score (averaged 60.5%). 7 Although no patient experienced postoperative kyphosis during their follow-up, the high incidence of dura mater tearing (11.1%) cannot be ignored. During the en bloc resection of the lamina and OLF, handing of the drill must be particularly meticulous without any violence to minimize the risk of cord injury due to the difference of the size of the ossified mass and the depths of OLF between the laminae and the ossified lesion in front of the facet joint. 7 What’s more, the elevation of the one-side lamina and OLF may result the falling of the other side into the spinal canal can injury the cord. Compared to laminectomy, laminoplasty can reduce risk of mechanical disturbance into spinal canal and is relatively safe and less technically demanding. However, for severe OLF, the decompression may be insufficient. Other treatments include percutaneous endoscopic surgery, 21 transforaminal en bloc laminectomy, 22 and segmental en bloc laminectomy. 23 However, the long-term outcomes remain to be assessed. In this present study, 19 patients underwent the bridge crane technique, and 22 patients were treated by posterior laminectomy. All patients acquired improved neurological function at the final follow-up. However, patients in group BG had better neurological recovery at the final follow-up. In addition, the recovery rate of patients who underwent our novel technique was comparable to previous studies (Table 3).3,5,7,8,13 Therefore, we believe that the bridge crane technique could provide satisfactory clinical outcomes and neurological improvement. However, higher-quality study with larger samples and longer-term duration of follow-up will be required to confirm the results of this study.
Outcomes and Complications for the Surgical Treatment of OLF From Literature Review.
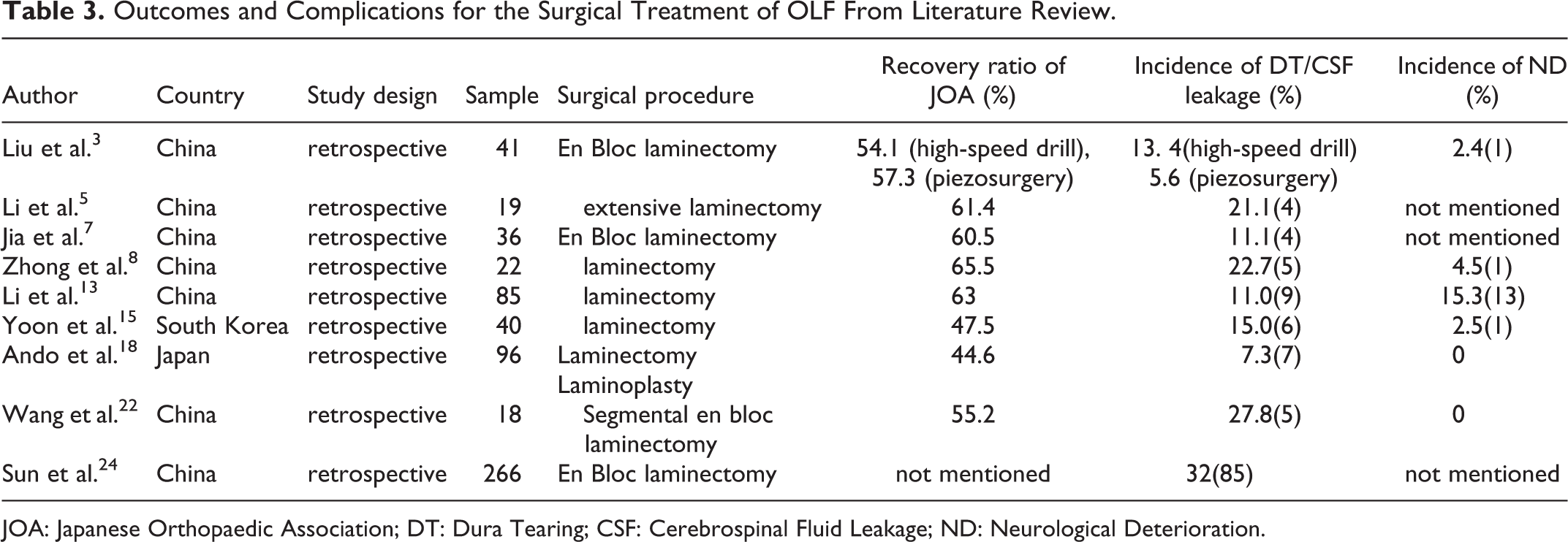
JOA: Japanese Orthopaedic Association; DT: Dura Tearing; CSF: Cerebrospinal Fluid Leakage; ND: Neurological Deterioration.
CSF leakage is one of the common complications due to dura adhesion or ossification (Table 3).3,5,7,8,13,15,18,22,27 Complications related to CSF leakage including CSF pseudocyst, wound dehiscence, respiratory obstruction, and even meningitis. In traditional surgery, both the iterative entry of the instruments into the spinal canal and the attempt to dissect and resect the adhesion form dura would increase the risk of dura mater rupture and CSF leakage. In a study by Zhong et al., the incidence of dura defect was 22.7% after laminectomy. 8 Jia et al. also reported 11.1% of the 36 patients had dura mater tearing after en bloc laminectomy, of whom one patient had CSF cyst after the operation. 7 Of the additional procedures to dura defect repair, various methods have been used, including suture, muscle/fascia, fat grafts, fibrin glue, and artificial dura.26-29 However, the long-term effects of any of these methods remain unknown. Furthermore, the process of recovery is a painful experience. 25 In fact, the idea of our procedure was based on the en bloc laminectomy and we isolated the LOC by the similar procedures of en bloc laminectomy. Different from laminectomy, the bridge crane technique hoisted posteriorly the LOC rather than resection, which is similar to the manipulation of anterior controllable antedisplacement and fusion (ACAF) for cervical ossification of the posterior longitudinal ligament. 30 The whole procedure was performed outside the spinal canal, and the adhesive or ossified dura mater was not dealt with, which could minimize the risk of dura mater rupture or CSF leakage. In addition, if the size of OLF is larger, we may also extend outside the 2 bilateral incision with partial resection of the facet joint throughout the involved segments. However, the elevation extent of OLF should be controllable. Too much posterior hoisting the OLF may also increase the risk of dura tearing. In this present study, one patient in group BG experienced CSF leakage during operation. Although the elevation was stopped immediately, postoperative MRI indicated his spinal cord was decompressed well. However, 3 patients in group L suffered from CSF leakage, which correlated with the manipulation of dissection or resection between ossified dura mater and the OLF.
Another important complication for thoracic OLF patients treated by traditional decompression operation is acute neurological deterioration. Young et al. reported the incidence of acute neurological deterioration in thoracic segment (14.5%) was higher than that in cervical spine (5.5%). 31 Anatomically, the blood supply is scantier and the spinal canal space at thoracic segment is relatively narrower, which may renders it vulnerable to ischemic damage. 8 Additionally, intraoperative manipulation inside the spinal canal or hematoma can also damage the cord.29,31 Other factors include intraoperative instability, increased thoracic kyphotic deformity, combined ossification of the posterior longitudinal ligament (OPLL), and ischemic reperfusion. 32 In this present study, one patient treated by laminectomy with instrumented fusion experienced acute neurological deterioration in his lower extremities muscle strength due to postoperative hematoma, and appropriate and prompt surgery is performed to prevent further catastrophic consequences. We attributed the lower incidence of acute neurological deterioration for patients in group BG to the out-sided manipulation and the slow and gradual decompression of the cord.
This study has several limitations. Firstly, this was a retrospective single-center study and the results need to be prospectively verified by multicenter and randomized-control studies in the future. Secondly, as mentioned in our previous study, because the decompression of our novel technique mainly depended on the distance between the LOC and the 2 transverse connectors, this technique is only limited to the thoracic spine with neutral to lordotic segments and may have a limited effect in kyphotic spines due to the risk of insufficient float of the cord. 11 Thirdly, the sample of patients in this single-center study was relatively small and the duration of follow-up was relatively short. Even that it seems that a result could exist, there is lack of statistical power. Therefore, to minimized the source of bias, all the surgeons in this study were from the same spine surgery team, with relatively similar surgical experience and habits. The primary results in this study demonstrated significant advantages of the bridge crane technique over laminectomy in treating cases with thoracic OLF regarding recovery rate of JOA score at the final follow-up, which would provide some clinical references when the surgeons make their decision of selection of surgical techniques. However, multi-center prospective studies with larger samples and long-term of follow-up will be required to verify the results in this study.
Conclusion
In conclusion, the bridge crane technique is relatively safe and sufficient for patients with symptomatic thoracic OLF with more satisfactory clinical improvement. However, high-quality study with larger sample and longer duration of follow-up is still necessary to validate the results of this study.
Footnotes
Authors’ Note
Kaiqiang Sun, Xiaofei Sun, and Jian Zhu contributed equally to this study and should be considered as the co-first authors. Jingchuan Sun and Jiangang Shi contributed equally to this study regarding the design and revision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported by the National Natural Science Foundation of China, Grant/Award Numbers: 81871828.