
Abstract
Purpose:
To assess the natural history of ossification of yellow ligament (OYL) in the thoracic spine and determine risk factors for progression based on a longitudinal population-based cohort.
Methods:
A prospective, longitudinal cohort study was performed on a population-based cohort of Southern Chinese volunteers. T2-weighted magnetic resonance imaging (MRI) was used at baseline to identify any OYL and was verified with computed tomography. Follow-up MRI was performed 5 years later. Parameters under study included the size of OYL, levels of involvement, morphology (round, triangular, beak), whether it crossed the midline and any disc degeneration.
Results:
A total of 114 (6.1%) individuals were identified to have OYL at baseline out of the 1864 individuals. Size progression occurred predominantly at the lower thoracic region. Majority of the new OYL were also in the lower thoracic spine and was associated with higher body mass index (BMI). Smokers were associated with OYL size progression while patients with higher BMI tended to develop new OYL at follow-up. Progression commonly occurred at the lower thoracic levels and regression occurred mostly at the upper thoracic levels.
Conclusions:
This is the first population-based series addressing the natural history of OYL. Better understanding of the natural history of OYL may provide incentive to introduce preventive measures such as weight reduction and close monitoring for myelopathy development in those at-risk groups for progression. This is especially important for patients with lower thoracic OYL and who are smokers with higher BMI.
Level of Evidence:
1 (prognostic study).
Introduction
Ligamentum flavum, also known as the yellow ligament, is in close proximity to the spinal cord. If it undergoes ossification, these ossified yellow ligaments (OYL) may cause spinal cord compression. 1 A previous population study showed that the overall prevalence of OYL within the Southern Chinese population was 3.8%. 2 It also showed that T2-weighted sagittal magnetic resonance imaging (MRI) was able to identify OYL as a hypointense signal intensity at the posterior margin of the spinal canal (Figure 1). 3,4 The majority of OYL occurs in the thoracic spine 2 and up to 75% of all cases of thoracic myelopathy are caused by OYL. 5 Thoracic myelopathy usually presents with gait disturbance, lower limb numbness and weakness. 6 Delay in treatment may cause individuals to develop spastic gait, urinary and bowel sphincter incontinence, paraplegia, and bedsores. 6,7 Hence, this condition imposes significant detriment to patients’ function.

Ossified yellow ligament (OYL; orange arrow) indicated by a hypodense lesion on sagittal T2-weighted magnetic resonance imaging.
Thoracic stenosis has been shown to be associated with advanced age and obesity. 8 Decompression surgery is important for neurological improvement in thoracic stenosis. However, decompression surgery in the presence of OYL is not without risk. OYL surgery is inherently high risk for intraoperative dural tear due to dural adhesions. 9 The chance of this complication may further increase with the presence of dural ossification. 10,11 In a series of 110 patients undergoing multilevel lumbar laminectomies, 9 dural tears occurred in all 10 patients with OYL. Moreover, three of these patients (30%) had dural ossification.
The development of OYL is likely a result of endochondral ossification. 12 There are 2 layers of ligamentum flavum: the interlaminar portion over the central (or medial) part and the lateral capsular portion. 12 Ossification is usually initiated in the capsular portion but may progress to the interlaminar area. 13 The ossification then proceeds to enlarge ventrally with compression of the spinal cord. If the ossification occurs bilaterally, the bony mass will then fuse in the middle and thicken to form a central tuberous mass. 13 In the sagittal plane, ossification begins at the site of attachment caudally along the superficial layer of the ligamentum flavum and then progresses cephalo-anteriorly. 12 Articular processes and laminae may also thicken with compact lamellar bone but usually do not directly cause cord compression.
Despite understanding of the pathological process of OYL, its natural history and risk factors for OYL progression are unknown. Similar to its anterior counterpart, the ossified posterior longitudinal ligament (OPLL), natural history is important as it indicates whether the disease process may continue to deteriorate and it determines when surgeons should intervene. 14 The authors believe that, if OYL progresses with time, treatment should not be delayed even in presence of mild symptoms. Without timely intervention, patients may deteriorate, lose the opportunity to regain complete function, and undergo decompression for more severe OYL, which carries higher risk of complications. Knowing the risk factors for progression can help to identify the high-risk subjects for closer monitoring. As such, this current study aims to identify the natural history of thoracic OYL on MRI and to determine risk factors for OYL progression based on a large-scale, population cohort assessed longitudinally.
Methods
Study Design
This was a prospective, longitudinal cohort study of 1864 subjects (n = 1158 women, n = 706 men) as part of the Hong Kong Disc Degeneration Population-Based Cohort. 15 -21 This study was ethically approved by a local institutional review board and informed consent was obtained by all subjects. Volunteers were between 18 and 55 years old and were recruited from the population by open invitation. All subjects were of Southern Chinese origin and had baseline T2-weighted sagittal MRI of the whole spine. Exclusion criteria included pregnancy, severe osteoporosis, previous spinal surgery, treated or untreated central nervous system impairment, fracture, illiteracy, subjects unable to undergo MRI scanning because of ferromagnetic implants, severe claustrophobia or inability to tolerate positioning for MRI.
Imaging
T2-weighted, 5-mm spin-echo sagittal MRI sequences using 1.5-T clinical MRI (General Electric Medical System, Milwaukee, WI, USA) were obtained. The field of view was 18 × 18 cm, slice thickness was 4 mm, and slice spacing was 0 mm. The imaging matrix was 288 × 192. The repetition time (TR) was 3325 ms and the echo time (TE) was 85 ms. Follow-up MRI used were 3 T.
All included patients had hypointense signal intensities identified on the baseline MRI with subsequent computed tomography (CT) scans to confirm that the lesions were ossifications and not calcifications. Ossification showed bony trabeculae in CT scan whereas calcification did not have trabeculae. Confirmed patients underwent another set of MRI at 5 years of follow-up to assess the natural history of the lesions on imaging.
Parameters Under Study
Clinical parameters included age, sex, height (meters), weight (kilograms), body mass index (BMI; kg/m2), and smoking status (smoker or nonsmoker). BMI greater than 25 kg/m2 was considered obese, BMI of 23 to 25 kg/m2 was considered overweight, BMI of 18.5 to 23 kg/m2 was considered normal, and BMI less than 18.5 kg/m2 was considered underweight. Imaging parameters included the size, level of involvement, and morphology of the OYL. As the clinical significance of OYL progression is represented by an increasing severity of cord compression, the size of the OYL should be expressed as a fill of the spinal canal. Thus, size was expressed as a percentage dividing the anteroposterior diameter of OYL in the sagittal cuts in which the diameter of OYL was largest, by the distance from posterior longitudinal ligament to the spinolaminar line at the corresponding level in the mid-sagittal cut (Figure 2). This provided the narrowest ratio between the 2 distances, which was most clinically relevant. Growth rates were also calculated and defined as the percentage change in OYL size divided by the initial OYL size. The types of OYL morphology had been described 2 as round (Figure 3), triangular (Figure 4), or beak types (Figure 5). The triangular type had a height smaller than or equal to its base while the beak type had a height greater than its base. Other imaging parameters included whether the OYL crossed the midline (bilateral involvement and visible in the mid-sagittal cuts) and the presence of disc degeneration defined as Pfirmann grade 4 (hypointense disc signal) or 5 (hypointense disc signal with disc space narrowing) 22 and disc protrusion (bulging of the disc beyond the posterior longitudinal ligament).
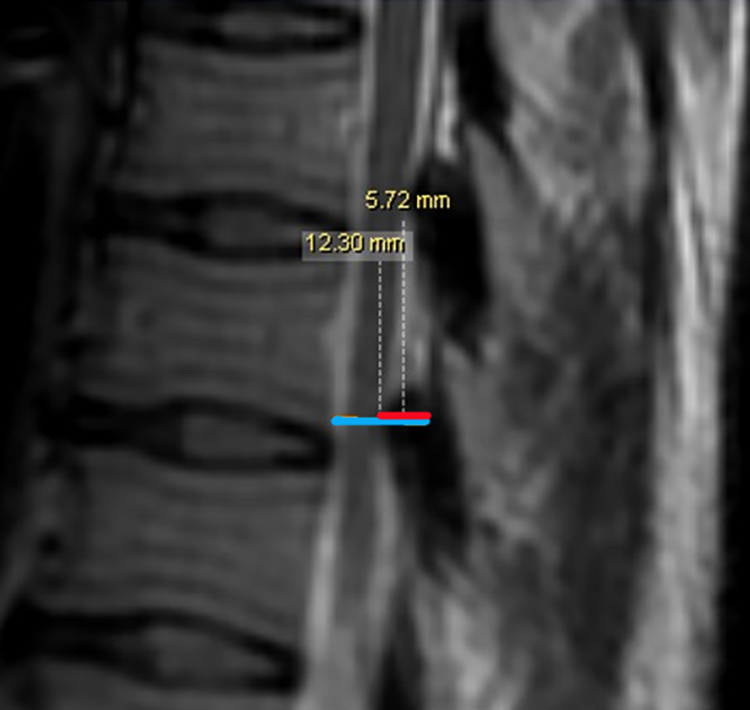
Ossified yellow ligament (OYL) size is measured on sagittal T2-weighted magnetic resonance imaging scans. The OYL size is expressed as a percentage of the spinal canal size. The anteroposterior diameter of OYL is first measured (blue line). Then, the spinal canal diameter is measured by the distance from, the posterior longitudinal ligament to the spinolaminar line at the corresponding level (red line). Finally, the first measurement is divided by the second measurement and expressed in terms of a percentage.
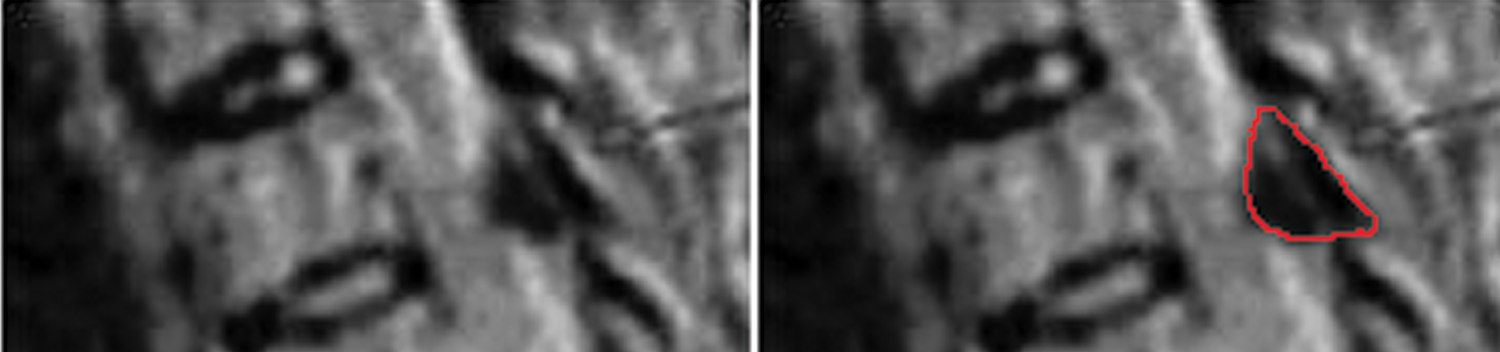
Round-type ossified yellow ligament (OYL; red line marked its margin).
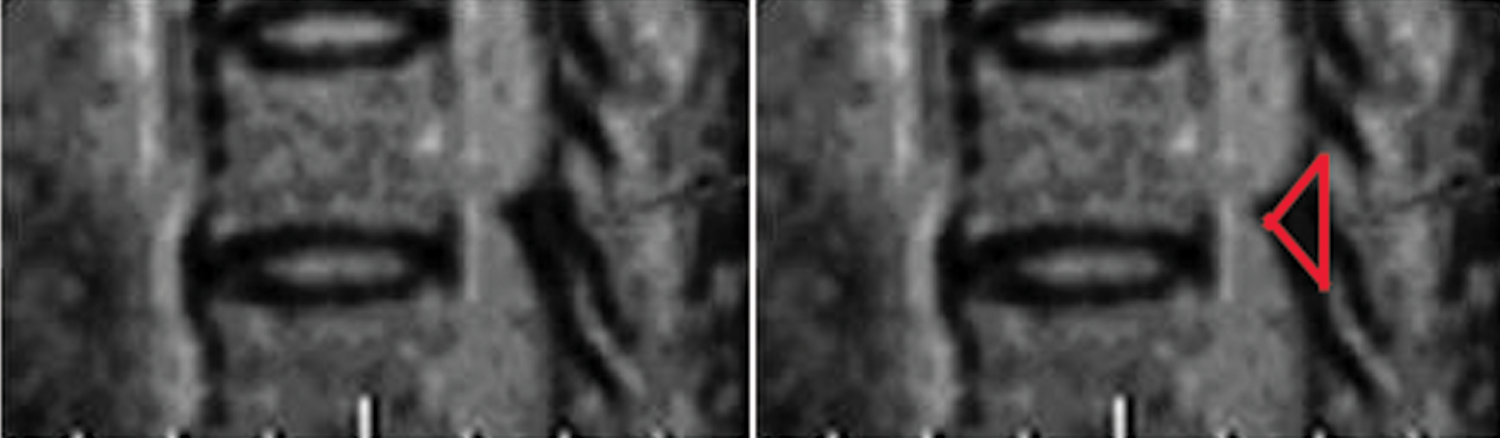
Triangular-type ossified yellow ligament (OYL) is indicated when the height of the ossification is smaller than or equal to the base (red line marked its margin).
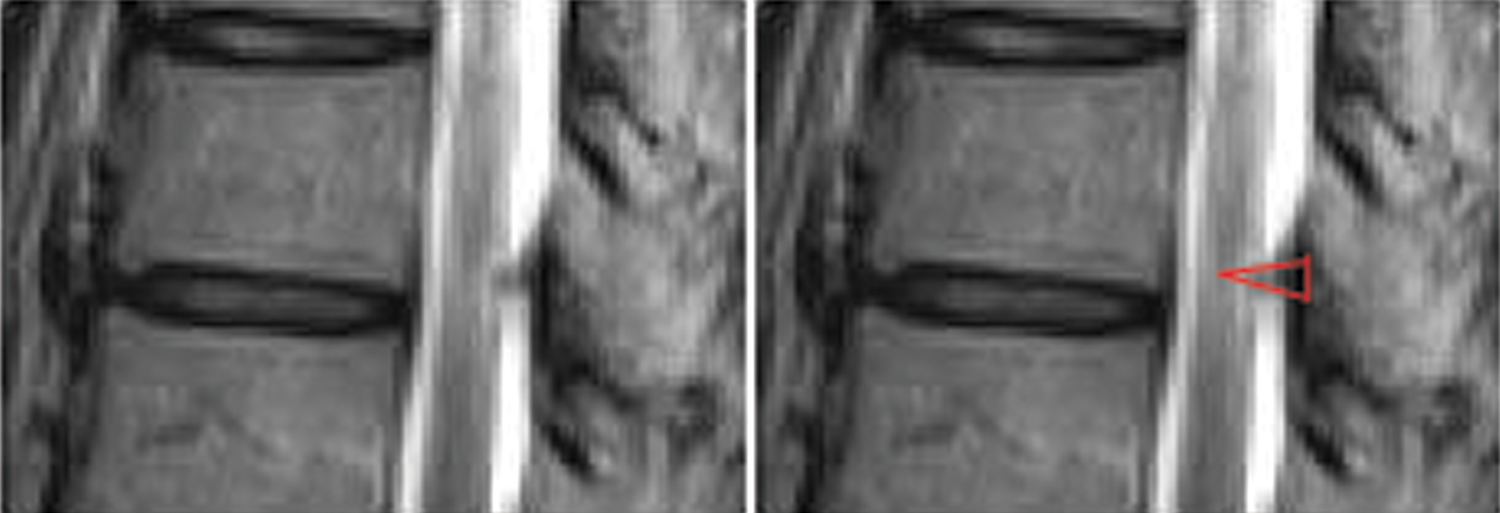
Beak-type ossified yellow ligament (OYL) is indicated when the height of the ossification is greater than the base (red line marked its margin).
Both original baseline images and 5-year follow-up images were read by 2 experienced orthopedic surgeons independently. Measurement differences of >10% for numerical measurements and differences in categorical measurements, if any, were settled by consensus. The average scores were used for analysis. All patient details were blinded to the readers during measurements. They were also blinded to the results of the initial MRI when interpreting the 5-year images. Four major features were studied over the 5-year period including the change in size and morphology, and any disappearance or de novo appearance. Size progression was defined as a larger sized OYL (in terms of the size of OYL in relation to the size of spinal canal) in the follow-up MRI than that of baseline. Growth rates were expressed as a percentage calculated by dividing the follow-up size by the initial size. Spinal levels were compared from baseline to follow-up to determine any disappearance (absence of OYL at the follow-up but present at baseline) and de novo appearance (presence of OYL at follow-up but not present at baseline).
Statistical Analysis
Descriptive statistics were expressed in mean ± standard deviation (SD). This was used for age, gender, BMI, smoking status, levels of involvement, OYL size, morphology, whether it crossed the midline and disc degeneration. Interobserver reliability was assessed by intraclass correlation (ICC). Cronbach alpha values of .90 to 1.00 were considered to indicate excellent reliability; .70 to .89, good reliability; and ≤.69, poor reliability. 23,24 Paired t tests were used to compare the changes between baseline and follow-up for changes in size and growth rate. Correlations (r) between growth rates and levels of involvement were also determined. Chi-square test was used to assess for correlation between smoking status, BMI, and disappearance of de novo appearance of OYL at follow-up.
Results
At baseline, 114 subjects (n = 40 males and n = 74 females) or 6.1% of the cohort were found to have OYL (Figure 6). There were no dropouts during follow-up. The mean age of subjects was 47.5 ± 6.5 years (range 19.7-60.5 years) (Figure 7) and the mean BMI was 24.0 ± 5.6 kg/m2 (range 14.2-71.6 kg/m2). Up to 7.0% of the study population were smokers. A total of 298 spinal segments were found to have OYL on the baseline MRI and 518 spinal segments had OYL at follow-up indicating an overall progression in OYL observed. The majority (61.7%) of OYL at the baseline MRI were in the lower thoracic region (T8-12: 184 spinal segments). In the follow-up MRI, the majority (54.2%) of OYL were also found in the lower thoracic region (T8-12: 281 spinal segments). A total of 31 spinal segments (10.4%; n = 14 subjects) at baseline had OYL that crossed the midline. In addition, 8 (2.7%) spinal segments with OYL had corresponding levels of disc degeneration, all of whom were nonsmokers. Three of these patients had OYL progression. A total of 50 (9.7%) spinal segments in the follow-up MRI had OYL that crossed the midline (20 new spinal segments) and 16 of these (3.1%) had corresponding levels of disc degeneration (9 of these 16 were newly developed).
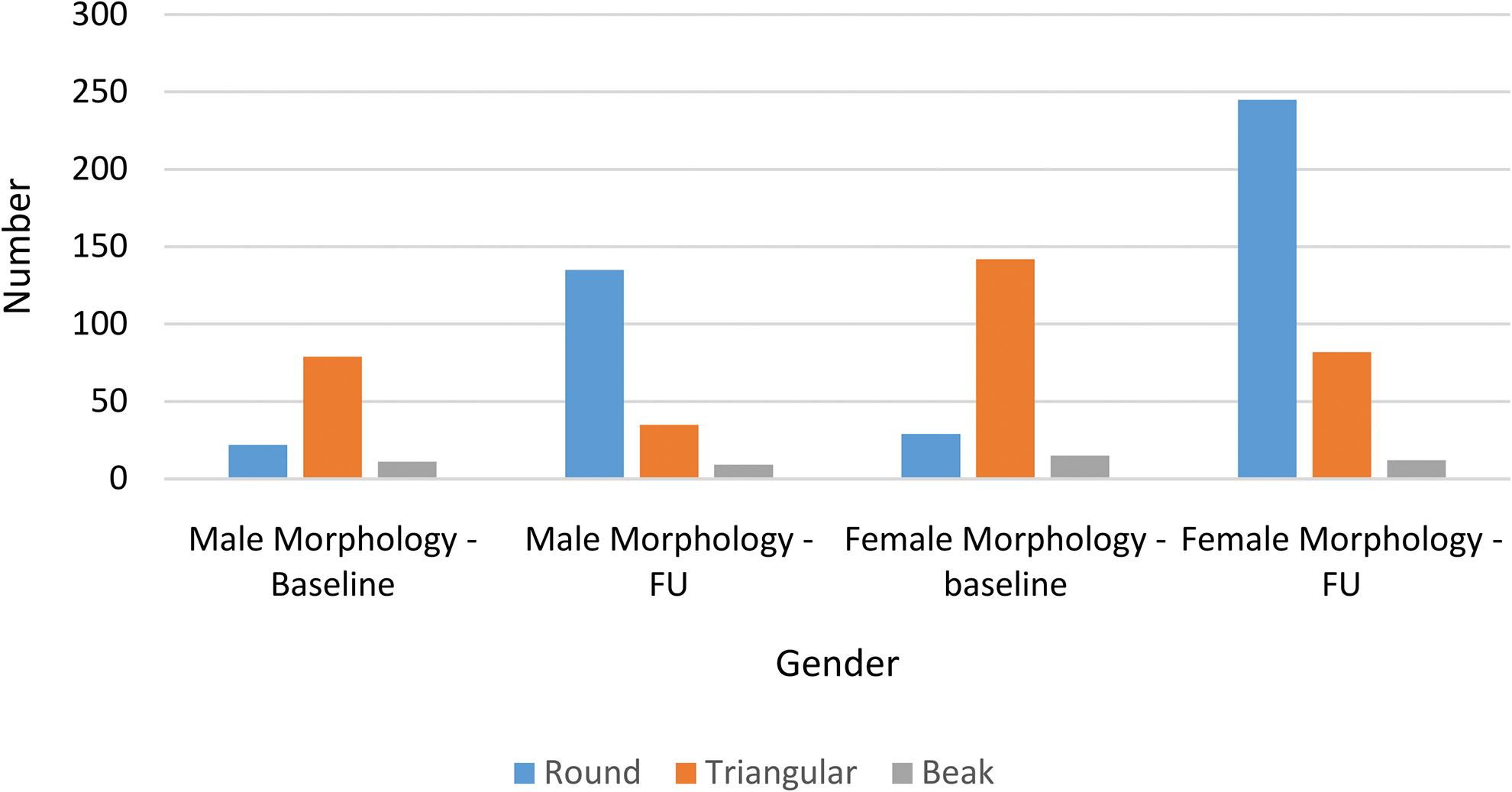
Ossified yellow ligament (OYL) type according to gender at baseline and follow-up (FU).
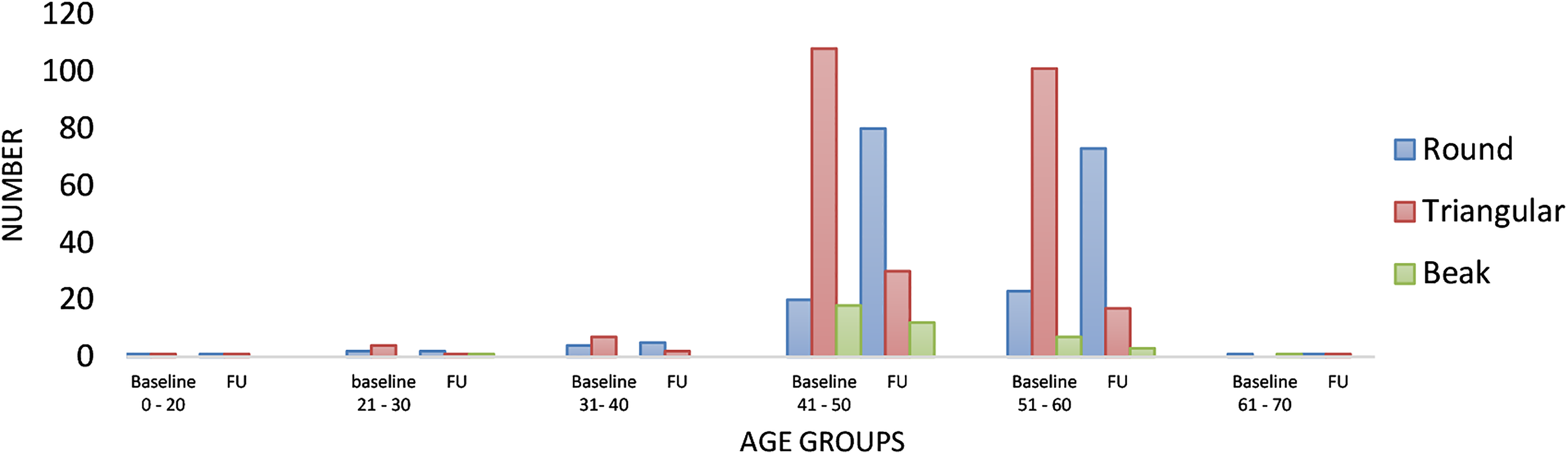
Ossified yellow ligament (OYL) type according to each age group at baseline and follow-up (FU).
Of the outcomes described below, no statistically significant associations were found with age, gender, whether the OYL crossed the midline initially and disc degeneration (Table 1).
Risk Factors for Changes in Ossified Yellow Ligament (OYL) Size, Morphology, and Disappearance.a
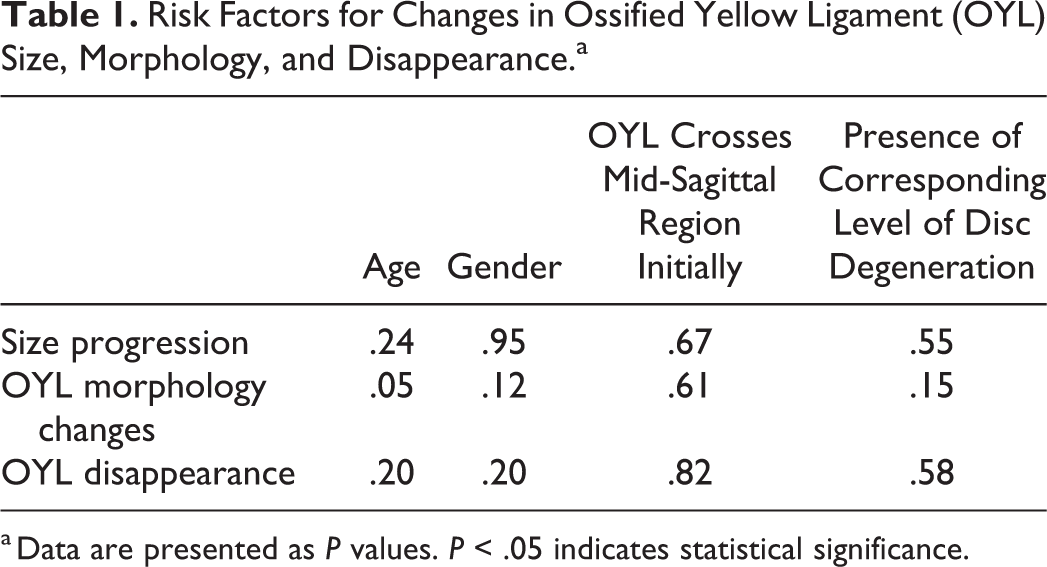
a Data are presented as P values. P < .05 indicates statistical significance.
Size Progression
The mean initial size of OYL was 40.8% ± 10.9% and the mean size at follow-up was 41.7% ± 11.0%. Majority of OYL in the lower thoracic region, especially T9-T10 level, showed size progression (Figure 8). In the subgroup analysis, 70% of OYL at T9-T10 and 62% of OYL at T10-T11 became larger (P < .05). T9-T10 OYL had statistically significant size progression (from 41.8% to 46.3%) while C7-T1 OYL had statistically significant size regression (from 49.4% to 32.9%) (P < .05). The chance of size progression was not related to BMI (P = .38) or initial morphology (P = .13). Growth rates at T9-T10 and T10-T11 were +13.4% and +3.8%, respectively (Figure 9). Within the level of T9-T10, the growth rate was negatively correlated (r = −0.32) with the size of OYL (P = .02). This suggested that a smaller sized OYL would grow more, while a larger sized OYL would grow less. A total of 75% of smokers had size progression while only 46% of nonsmokers had size progression (P = .04). A total of 53.4% of those with low back pain and 46.7% of those without low back pain had size progression. Presence of low back pain did not predict the size progression of OYL at 5 years (P = .39). An example of OYL size progression in 5 years is shown in Figure 10.
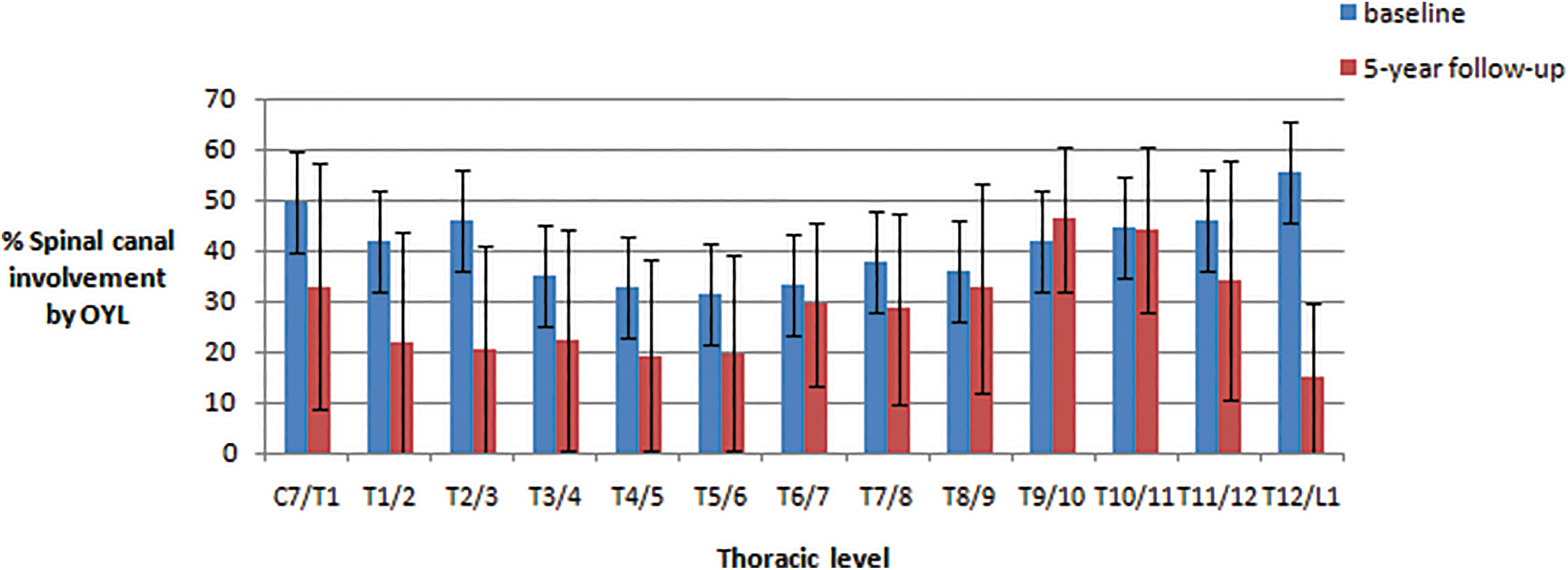
This chart highlights ossified yellow ligament (OYL) size progression in this study comparing percentages of spinal canal involvement according to specific spinal levels between baseline and 5-year follow-up with standard error bars. There is statistically significant OYL size progression at T9/10 and significant OYL size regression at C7/T1.
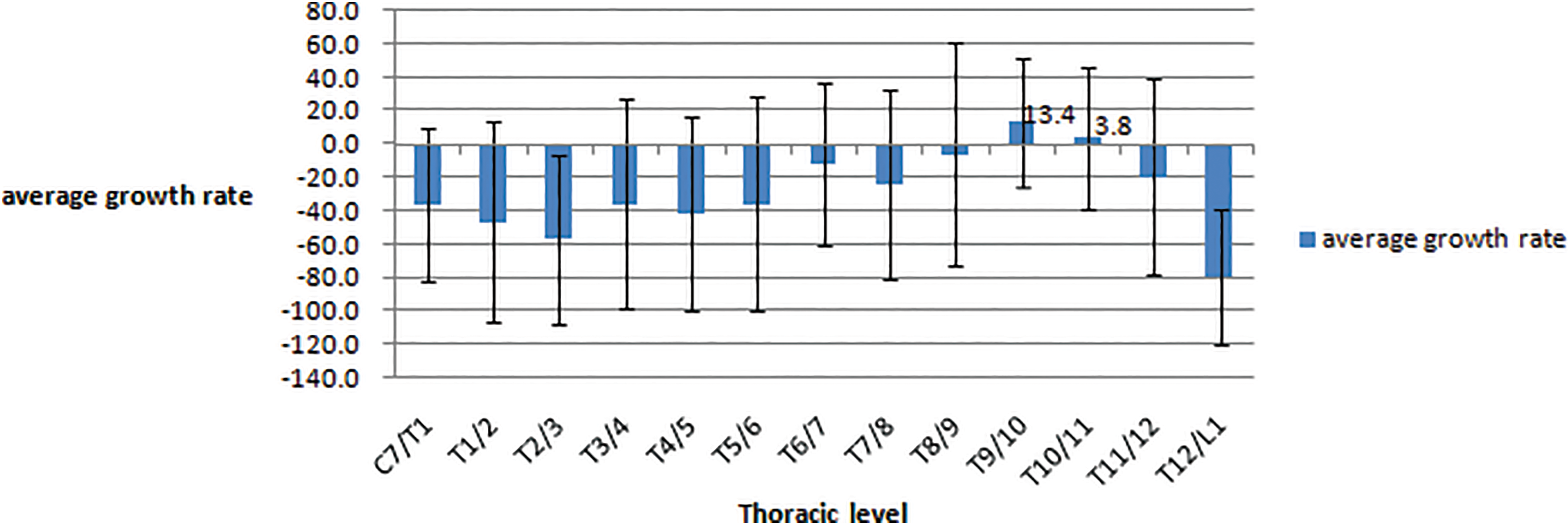
This chart highlights the average growth rate of ossified yellow ligament (OYL) over 5-year follow-up. There were positive growth rates at T9/10 and T10/11. Growth rate was calculated as the percentage change in OYL size divided by the initial OYL size.
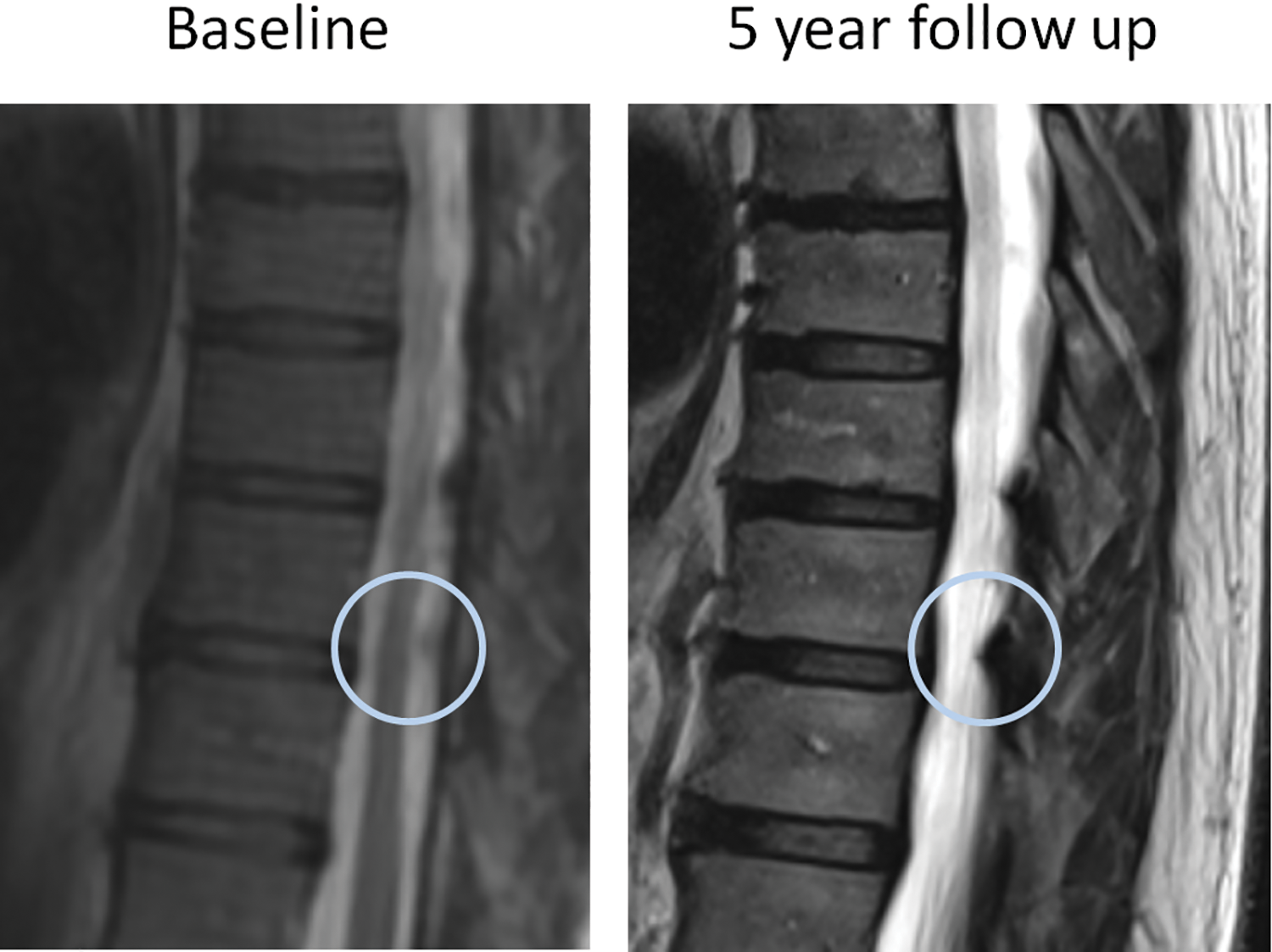
Serial magnetic resonance imaging scans in 5 years showed T9/10 ossified yellow ligament (OYL) size progression.
Change in Morphology
Regarding the morphology at baseline, 74.2% were triangular type, 17.1% were round type, and 8.7% were beak type. For the subsequent morphology changes at follow-up, 22.6% remained triangular type, 70.4% were round type, and 7.0% were beak type. Regarding the 74.2% triangular OYL at baseline, 55.7% of them became round type. Up to 123 segments changed from triangular to round type with follow-up (Figure 11).
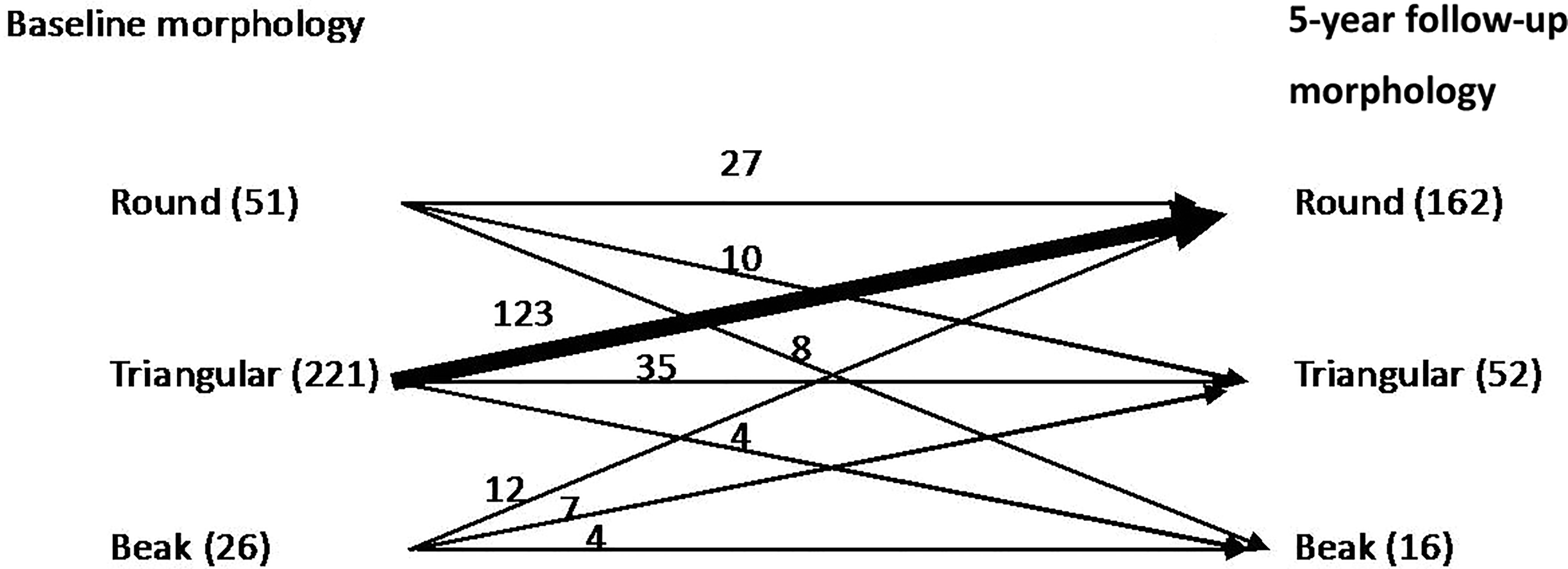
This diagram highlights the ossified yellow ligament (OYL) morphology changes over 5-year follow-up. Majority of OYL were triangular at the baseline, while majority of OYL were round at follow-up. Of note, 123 triangular-type OYL changed to round type at follow-up.
OYL Disappearance
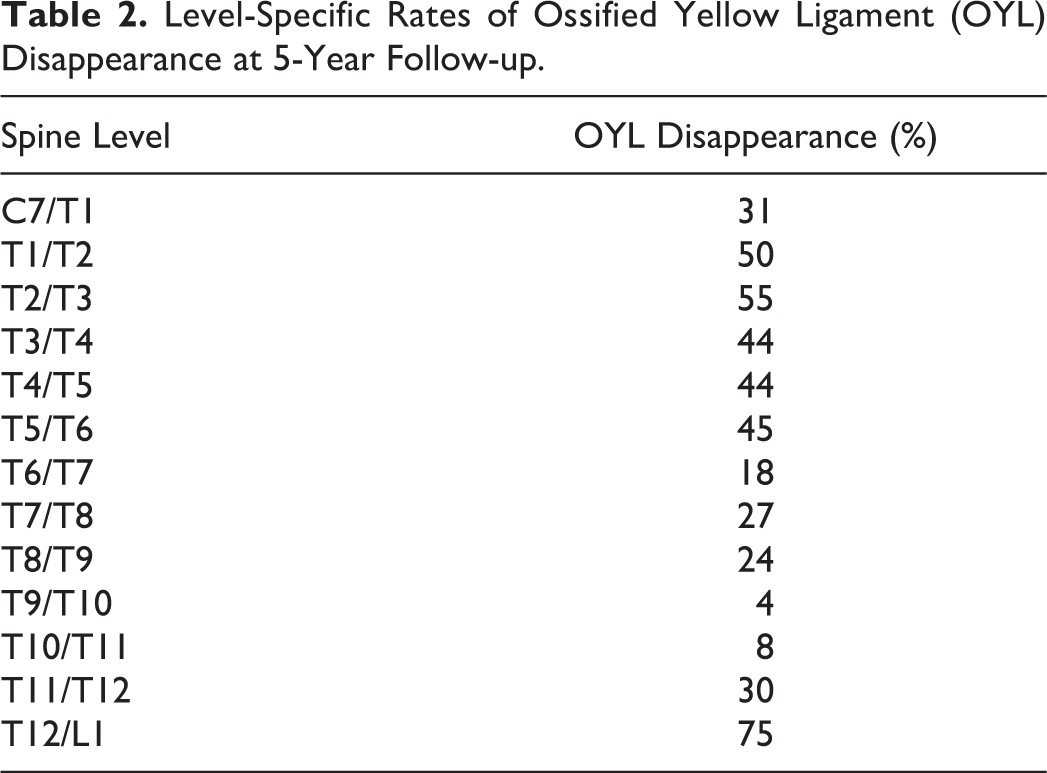
OYL disappearance was observed in 22.8% (68 out of 298 segments) of segments. In the subgroup analysis of different levels, T9-T10 and T10-T11 OYL were least likely to disappear (P < .05) (Table 2). Only 3.7% of T9-T10 and 7.6% of T10-T11 OYL disappeared. In patients aged 30 to 40 years, 41.7% of OYL resolved (P = .03). Four subjects who had OYL disappearance in 5 years were smokers and they continued to smoke within the study period. Reduced BMI was observed in subjects with OYL disappearance within the 5-year follow-up (initial BMI of 23.7 vs 5-year follow-up BMI of 23.4, P < .01). An example of OYL disappearance in 5 years is shown in Figure 12.
Level-Specific Rates of Ossified Yellow Ligament (OYL) Disappearance at 5-Year Follow-up.
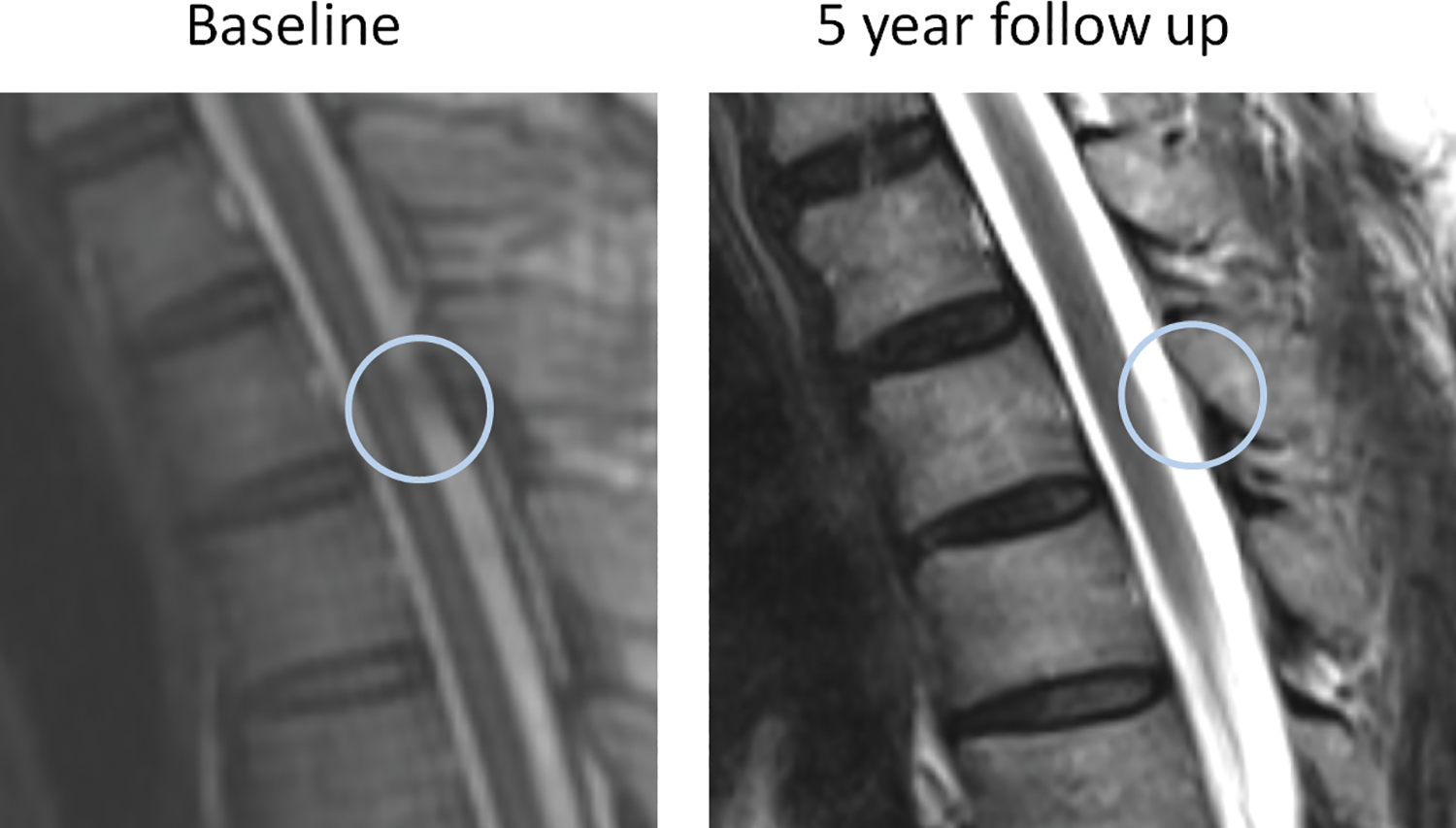
Serial magnetic resonance imaging scans in 5 years showed disappearance of T2/3 ossified yellow ligament (OYL).
De Novo Appearance
There was de novo OYL formation in 55.6% of spinal segments. The majority occurred in the lower thoracic levels: T8-T9 (11.5%), T9-T10 (11.1%), T10-T11 (10.4%), and T11-T12 (10.1%) (Table 3). De novo formation was associated with higher BMI as 55.8% of the spinal segments with newly formed OYL occurred in obese subjects. By comparison, 52.8% of segments occurred in overweight subjects, 42.7% in subjects with normal BMI and 30.8% in underweight subjects (P = .02). A total of 48.1% of those with low back pain and 52.8% of those without low back pain had de novo OYL appearance. Presence of low back pain did not predict the de novo OYL appearance at 5 years (P = .37).
Level-Specific Rates of De Novo Ossified Yellow Ligament (OYL) Formation.a
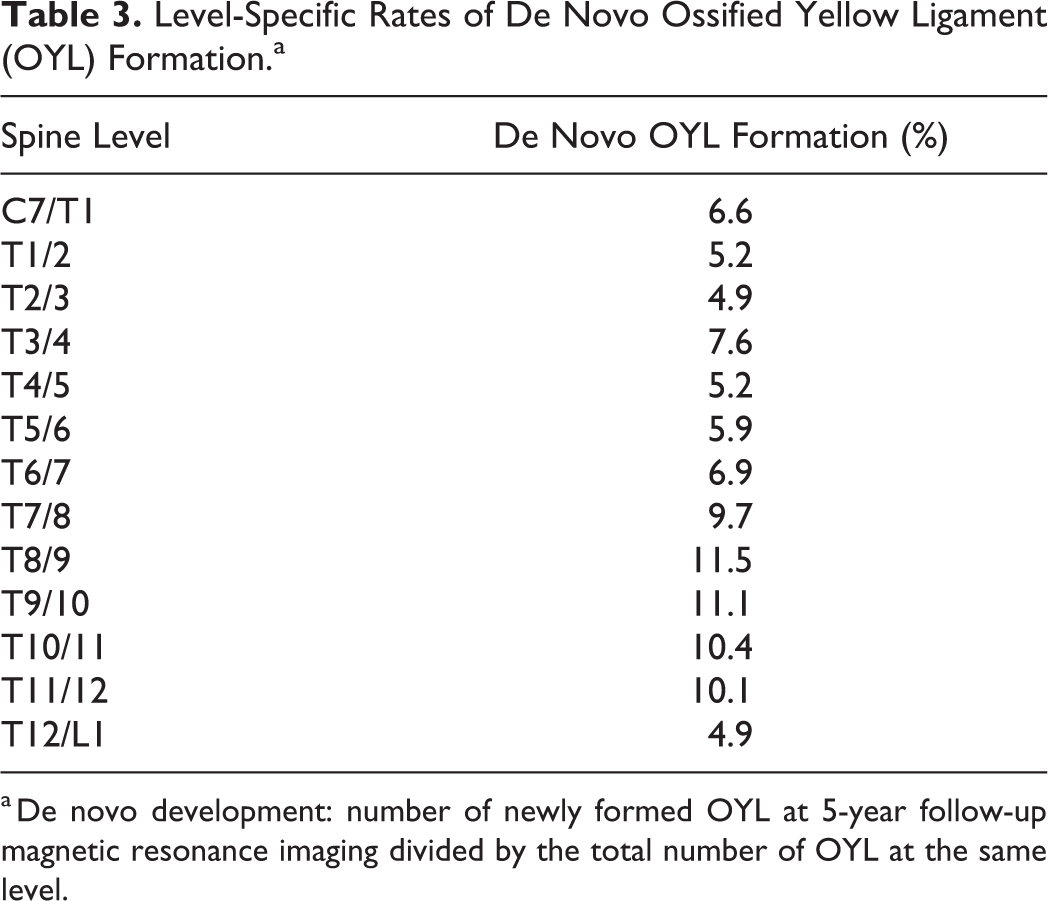
a De novo development: number of newly formed OYL at 5-year follow-up magnetic resonance imaging divided by the total number of OYL at the same level.
Discussion
This is the first population-based series addressing the natural history of OYL and risk factors for its progression. The strength of the study is in the large number of subjects screened at baseline and with all of them followed up longitudinally for 5 years with repeated scans. Not only does this study identify the prevalence of OYL (6.1%) in a cohort that essentially represents the general southern Chinese population, it also suggests that OYL has variable natural history that may be related to a subject’s BMI, smoking status, location, and morphology of OYL. OYL tend to progress in smokers and in the lower thoracic region. Furthermore, morphology changes and new formation occur with time and especially in higher BMI groups. Presence of low back pain has no association with size progression or de novo appearance of OYL.
One of the key messages highlighted by this study is size progression with time. Within 5 years of follow-up, a significant increase in size has been identified, which occurs particularly in the lower thoracic region. This is of concern since it is in the experience of the authors that thoracic myelopathy caused by OYL usually occurs in the same region. This may indicate that clinically relevant OYL disease deteriorates with time with more significant compression. 25 However, this is a theory that is difficult to prove as patients with myelopathy are rarely studied prospectively without intervention. Biomechanics is the likely rationale for predominantly the lower thoracic region to observe size progression. The lower thoracic region is more mobile due to the transition of thoracic to lumbar spine and the less rigid portion of the rib cage with false ribs. Higher tensile forces exist and as a result, the spine is more prone to degeneration. Conversely, the upper thoracic region is relatively stiffer and thus regression is more commonly found at this region. OYL forms by this process with deposition of calcium pyrophosphate dehydrate and calcium hydroxyapatite in the ligamentum flavum, which has undergone collagen hyperplasia and hypertrophy. 26 Another risk factor that links OYL with the spine degeneration pathway is smoking. 27 Despite the small number of smokers in our study with OYL, undoubtedly the analysis suggests that smoking may be related to size progression.
Alternatively, most of the OYL with size reduction occurred at the upper thoracic segments. It is interesting to find that some OYL reduces in size at follow-up. This phenomenon may be explained by a similar occurrence reported with OPLL. 28 Non-ossified segments of OPLL may decrease in size after stabilization of the segment. Hence, the size reductions may have occurred due to the comparably stiffer upper thoracic region. This suggests that remodeling occurs with time and may be region specific.
Remodeling may also pertain to morphological changes. A large portion of triangular-type OYL converted into round-type at follow-up. This may have significant clinical implications since it is logical to think that round type may cause a more diffuse compression while triangular or beak type may cause a more focal compression. The “rounding-off” of triangular OYL with time may also have implications on postoperative neurological outcomes. A previous study 29 showed that a beak-type OYL experienced a higher recovery rate and a better satisfaction grade than did those with a round-type OYL after operation. This may be related to the chronicity of compression as a longer period of time has elapsed before beak types become round types. Hence, if subjects present with a round-type OYL, they may have had the compression longer. It is also important to note that beak-types were quite uncommon in our cohort. We postulate that beak types may be more likely to be symptomatic and thus these subjects are less likely to undergo a 5-year follow-up without requiring intervention.
Another interesting observation was the new formation of OYL with longitudinal follow-up. Ossification of spinal ligaments is a condition characterized by ectopic bone formation in the spinal ligaments such as posterior longitudinal ligament, yellow ligament, and anterolateral spinal ligament. They are caused by complex interaction between genetic and environmental factors as evidenced by the previous studies. 30 -33 Results suggest that 55.6% of spinal segments with OYL at baseline developed new OYL at other levels suggesting that OYL may be more likely to appear once it has developed in a spinal segment. Growth factors including bone morphogenetic proteins (BMPs) and transforming growth factor–β (TGFβ) may also have important roles in OYL development. 34 BMPs initiate cartilage and bone differentiation and induce new cartilage and bone formation in vivo, while TGFβ stimulates cartilage and bone formation via determined chondroprogenitor and osteoprogenitor cells in vivo. 35 Diet that involves pickles (salted products) have also been implicated in the development of spinal ligament ossification. 30,36 Thus, OYL may be more prevalent in Chinese and Japanese populations. Patients with OYL also have a higher prevalence of obesity, diabetes mellitus, hyperinsulinism, and impaired glucose tolerance. 32,33 De novo appearance of OYL was found in this study to be more common in patients with higher BMI. This relationship may be related to the higher biomechanical stress brought on by obesity in addition to the endocrine factors described above. Mechanical stress may increase the tension of ligamentum flavum, such as disc degeneration and vertebral wedging, which contributes to the ossification. 12 Similarly, patients with OYL disappearance appeared to have lost weight with longitudinal follow-up. Nevertheless, this causal relationship, and the effect of diabetes, require further pathomechanistic studies.
One important limitation of this study is the lack of CT scan verification at follow-up. Although these lesions on MRI were verified with CT scan at baseline, we avoided overexposure of radiation with repeated scans at follow-up. However, because of this, we cannot verify whether the new appearances of OYL at follow-up are calcifications or ossifications. Hence, the incidence of new OYL formation may be overestimated. 37 There is also a limitation with the clinical assessment. This longitudinal cohort was based on the Hong Kong Disc Degeneration Population-Based Cohort, which was originally built for lumbar disc degenerative disease. Hence, we only had assessments for presence of back pain rather than focused assessments for myelopathy such as limb spasticity and proprioceptive loss. Some patients may have developed subtle myelopathy but were not systematically identified. Another limitation is the lack of information regarding smoking exposures (pack-years), which made it impossible for dose-response relationship analysis. Nevertheless, it is important to note that this was a prospective longitudinal follow-up study and any findings at follow-up is representative of changes that occurred with time. Another limitation is the lack of size measurements on axial scans which may better represent the severity of canal compromise. Thus, these findings of OYL progression should be validated with other cohorts with axial images available. It is also important to correlate our findings with changes in clinical symptomatology. Finally, the longitudinal follow-up only included subjects with OYL at baseline and thus our prevalence may be underestimated. It is possible for previous unaffected individuals develop OYL only at the follow-up.
Conclusion
This is the first prospective, longitudinal follow-up study of OYL based on a population-based cohort. Study results show that OYL may progress, may regress, and may remodel with variable morphology and appearance. This has significant implications on our understanding of OYL natural history. With predominant progression in the lower thoracic spine, we can deduce that patients with thoracic myelopathy caused by OYL in the lower thoracic levels will likely progress and thus may require more timely surgery. Further study concerning symptomatology and other clinical data is necessary to link these radiological findings with the clinical presentation. In addition, further understanding behind why OYL progresses is necessary, including genetic predisposition and spine biomechanics.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Hong Kong Theme-Based Research Scheme (T12-708/12N).