
Abstract
Study Design:
Retrospective cohort study.
Objective:
To evaluate the outcomes of conventionally-fractionated external beam radiation therapy (cEBRT) in the treatment of prostate cancer spinal metastases (PCSM).
Methods:
Patients who received palliative cEBRT for PCSM in our institution between 2008 and 2018 were included. Our outcomes were local progression-free survival (LPFS), overall survival (OS), pain response and toxicities graded using CTCAE version 4.03. Univariable and multivariable Cox proportional hazard regressions were performed to identify predictors for LPFS and OS.
Results:
A total of 100 patients with 132 sites of PCSM were identified, with a median follow-up of 54 months. Fourteen-percent of patients underwent surgical intervention before receiving cEBRT. Eighteen spinal segments (13.6%) had local progression, with a median time to local progression of 8 months. The median LPFS and OS were 7.8 and 9.0 months, respectively. The complete and partial pain response rates were 57% and 39% respectively. The incidence of grade ≥3 acute toxicities was 11%. Better ECOG performance status (0 to 1), castration-sensitive disease, spinal surgery and use of novel antiandrogen agent were identified as significant predictors for improved OS on multivariable analysis.
Conclusions:
In our prostate cancer cohort, cEBRT is an effective treatment modality for local palliation of spinal metastases. More aggressive treatment approach should be considered for patients with excellent performance status and castration-sensitive disease in light of their expected longer survival. Further studies are warranted to identify the predictors for radiotherapy response in this population.
Keywords
Introduction
Prostate cancer is the second most frequently diagnosed cancer and the fifth leading cause of death in males globally. 1 Osseous metastases occur in 90% of metastatic prostate cancer cases, 2 with the spine being the most common site. 3 The predilection of prostate cancer for metastasizing to the spine is well-known, purportedly owing to the spread via Batson plexus of valveless veins located in the epidural space between vertebral column and dura matter.4-6
Many prostate cancer patients become castrate-resistant along the disease course. 7 Up to 80% of patients with castrate-resistant disease develop spinal metastases. 8 About a third of prostate cancer spinal metastases (PCSM) are symptomatic 9 and manifest with intractable pain, neurological deficits from nerve root or metastatic spinal cord compression (MSCC) and mechanical instability, which occasionally necessitate surgical intervention.10-13 Conventionally-fractionated external beam radiation therapy (cEBRT) is widely utilized in the palliative treatment of PCSM. 14 Several retrospective studies showed that stereotactic body radiation therapy (SBRT) has gradually emerged as a promising and well-tolerated treatment strategy for spinal metastases in bone-only oligometastatic prostate cancer.15-17 In addition, 2 randomized phase II trials (STOMP and ORIOLE) demonstrated that metastasis-directed therapy using SBRT conferred the benefits of forestalling initiation of androgen deprivation therapy (ADT) and prolonging progression-free survival in patients with oligometastatic prostate cancer, compared to observation.18,19 However, this aggressive approach should be reserved for a highly-selected group of patients, such as those with limited metastases and longer life expectancy.
cEBRT remains the cornerstone of the management of PCSM, especially in the context of poly-metastatic disease. To date, there is a dearth of literature regarding the outcomes of cEBRT in the treatment of spinal metastases of this specific histology. Hence, we performed a retrospective cohort study to evaluate the outcomes of patients with PCSM treated with cEBRT in our institution over a 10-year period.
Methods and Materials
Study Design
This was a retrospective cohort study. This study was approved by Institutional Review Board, National Healthcare Group (NHG) Domain Specific Review Board (reference number: 2018/00 559). The requirement for patient informed consent was waived.
Study Population
We screened the radiotherapy databases of our institution for eligible patients. Eligibility criteria included: (1) diagnosis of prostate cancer established based on histologic confirmation or clinical suspicion with reference to biochemical and imaging evidence, (2) stage IV disease as per American Joint Committee on Cancer (AJCC) seventh edition definition, 20 (3) the presence of spinal metastasis detected on imaging and treated with palliative-intent cEBRT in our institution between January 2008 and December 2018. Magnetic resonance imaging (MRI) of spine was recommended to assess the local extent of spinal lesions, but not mandated. Technetium-99 m bone scintigraphy and computed tomography (CT) of thorax, abdomen and pelvis were performed to evaluate the number of osseous metastases and the presence of any visceral metastases. Prostate-specific membrane antigen-positron emission tomography (PSMA-PET) scan was an alternative staging option. Prior definitive local therapy to prostate primary was allowed. Those who were treated using SBRT were excluded. STROBE flow diagram is illustrated in Figure 1.
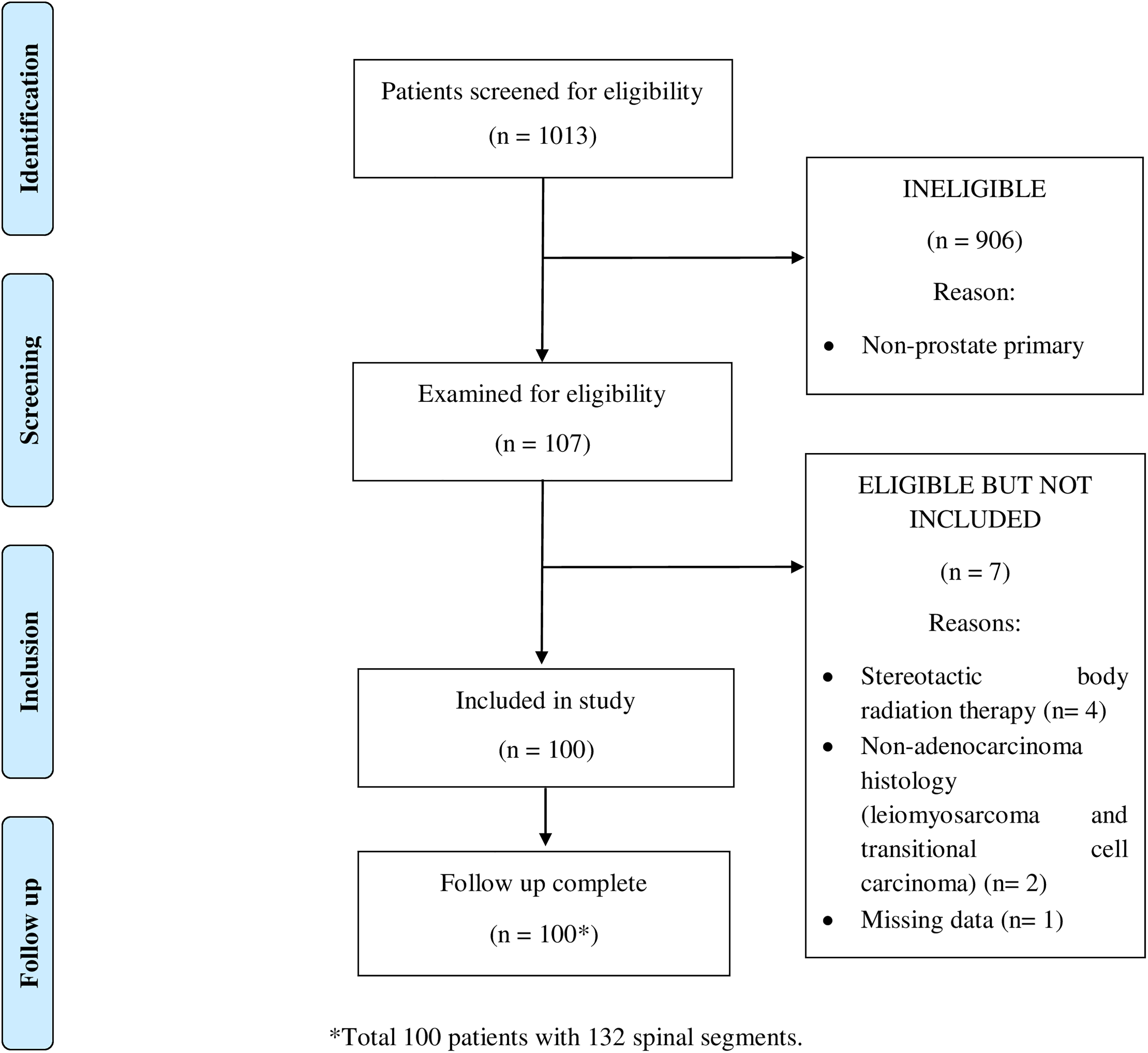
Strobe flow diagram.
Radiation Therapy Details
The indications of radiation therapy (RT) for PCSM in our institution included palliation of uncontrolled pain, local crisis or impending local crisis (such as MSCC) and post-operative consolidation. If indicated, patients were referred to a spine surgeon to discuss the option of surgery before RT was started. After spinal surgery, patients were usually given a duration of at least 2 weeks to allow optimal wound healing before commencement of RT. 21
All patients underwent CT-based treatment planning. The target vertebral segments were identified using CT, MRI or PSMA-PET diagnostic imaging where available. The RT portal encompassed any soft tissue component with an adequate margin and at least 1 vertebral level above and below the involved vertebral segments. Three-dimensional conformal radiation therapy (3DCRT) planning was done via XiO planning system, with at least 85% of the prescribed dose covering the entire body. Radiation was administered using 6 to 10 megavoltage photons via a posterior field. If the maximum dose exceeded 125% of the prescribed dose, anteroposterior-posteroanterior technique was deployed by adding a lightly-weighted anterior field. Opposed lateral field technique was typically used for cervical spine. The Quantitative Analyses of Normal Tissue Effects in the Clinic (QUANTEC) dose constraints were adopted during treatment planning from March 2010 onward. 22 The most common dose fractionation regimens for spinal metastases used in our institution were 30 Gy in 10 fractions and 20 Gy in 5 fractions administered once daily over consecutive weekdays. The dose fractionation regimen was determined upon the discretion of treating physician based on clinical factors, performance status and life expectancy. Quality assurance of the radiation volumes and plans was conducted within the first week of RT start.
The use of ADT and novel antiandrogen agents such as and enzalutamide was allowed during RT period. Cytotoxic chemotherapy and systemic radioisotope therapy were withheld during RT period.
Co-Variates
We collected the clinical data on patient demographic, tumor and treatment characteristics from institutional electronic medical records (CPSS2) and radiotherapy database system (MOSAIQ) using standardized data collection form. Patient-related data included age at the start of RT, ethnicity, Eastern Cooperative Oncology Group (ECOG) performance status, Charlson comorbidity index,23,24 and pre-treatment ambulatory status. Tumor-related data included histologic subtype, Gleason grade group, 25 serum prostate-specific antigen (PSA) within 3 months before RT start, D’Amico risk category,26,27 presence of visceral metastases, metastatic burden, castration status, timing of spinal metastasis relative to the diagnosis of prostate cancer, pre-treatment MRI use, revised Tokuhashi score, 28 Tomita score, 29 Crnalic score, 8 Rades score, 30 spinal instability neoplastic score (SINS), 31 Bilsky grade 32 and presence of soft tissue mass (defined as any cortical breach of vertebral body on CT or MRI). Treatment-related data included delivered radiation dose, fraction size, equivalent dose in 2Gy-fraction (EQD2) calculated using linear-quadratic equation assuming alpha/ beta (α/β) ratio of 1.5, 33 number of spinal levels irradiated, spinal surgery prior to receiving cEBRT, prior definitive local treatment to prostate primary, use of ADT, novel antiandrogen agents (such as abiraterone, enzalutamide and apalutamide), chemotherapy, ketoconazole, Radium-223 therapy, PSMA-Lutetium therapy and bone-modifying agents.
Metastatic burden was defined as per CHAARTED and STAMPEDE trials.34,35 Patients with 4 or more bone metastases with 1 or more outside the vertebral bodies or pelvis, or visceral metastases, or both, were considered to have high metastatic burden; all other assessable patients were considered to have low metastatic burden. Castration-resistant disease was defined as prostate cancer that progresses clinically, radiographically, or biochemically despite castrate levels of serum testosterone (less than 50 ng/dL) after being on ADT. 36 Spinal metastasis was considered as a synchronous lesion if it was diagnosed within 3 months from the date of prostate cancer diagnosis. The SINS, Bilsky grade, and presence of soft tissue mass was determined after reviewing imaging and reports and, in consultation with the reporting radiologist if clarification was needed. The detailed description of Tomita score, 29 Crnalic score 8 and Rades score 30 systems is illustrated in Supplementary Tables 1 to 3.
Outcomes
The outcomes of interest were local progression-free survival (LPFS), overall survival (OS), pain response and toxicity.
Local progression was defined as any clinical or radiological evidence of disease progression at the index site of spinal metastasis which received cEBRT. Clinical progression refers to symptomatic progression such as pain and neurological deficits, or any event that warrants interventions such as salvage surgery, re-irradiation or interventional radiology procedures (like vertebroplasty). Radiological progression was assessed using CT or MRI imaging and determined based on the revised Response Evaluation Criteria In Solid Tumors (RECIST) version 1.1. 37 LPFS was calculated from RT initiation to local progression, death from any cause or last censor. OS was calculated from RT initiation to death from any cause or last censor. Pain response was assessed at the first post-RT follow-up at 1 month and categorized as complete response, partial response or no response. A complete response was defined as resolution of pain; a partial response was defined as a decrease in pain score or a reduction in the use of analgesics. Acute and late toxicities were graded using Common Terminology Criteria for Adverse Events (CTCAE) version 4.03. Acute toxicity was defined as toxicity that occurs within 3 months of RT treatment. Patients were reviewed clinically 1 month after RT treatment, followed by 3- to 6-monthly follow-up subsequently.
Statistical Analysis
The follow-up interval was calculated from RT initiation to the date of last censor or death. Frequencies with percentages and medians with ranges were used to describe the baseline characteristics of the study population. The age at the start of RT treatment, pre-RT serum PSA, duration between diagnosis of prostate cancer and spinal metastases, SINS, Bilsky grade, number of spinal levels irradiated were analyzed as continuous variables. ECOG performance status (0 to 1 versus (vs) 2 to 4), Charlson comorbidity index (<9 vs ≥9), pre-treatment ambulatory status (ambulant vs non-ambulant), Gleason grade group (1 to 3 vs 4 to 5), presence of visceral metastases, metastatic burden (low vs high), castration status (castration-sensitive vs castration-resistant), timing of spinal metastases (synchronous vs metachronous), pre-treatment MRI use, revised Tokuhashi score (0 to 8 vs 9 to 15), Tomita score (2 to 5 vs 6 to10), Crnalic score (0 to 1 vs 2 to 4 vs 5 to 6), Rades score (20 to 34 vs 35 to 39), presence of soft tissue mass, EQD2 (≥38.57Gy1.5 vs <38.57Gy1.5), spinal surgery, prior definitive local treatment to prostate primary, ADT, novel antiandrogen agent and chemotherapy were analyzed as dichotomous variables. Univariable and multivariable Cox proportional hazard regressions were performed to evaluate for variables associated with LPFS and OS. LPFS was analyzed with death from any cause as the competing event. The variables with P-value of less than 0.05 on univariable analyses were entered into multivariable models to identify predictors for LPFS and OS. A P-value of less than 0.05 was considered as statistically significant. The analyses were performed using STATA version 14.0.
Results
Baseline Characteristics
The baseline characteristics of study population are summarized in Table 1.
Baseline Characteristics of Study Population.

Abbreviations: EBRT, external beam radiation therapy; ECOG, Eastern Cooperative Oncology group; MRI, magnetic resonance imaging; PSA, prostate-specific antigen; PSMA, prostate-specific membrane antigen; RT, radiation therapy.
We identified 100 eligible patients with 132 sites of spinal metastases. Most patients (75%) received cEBRT at single site of spinal metastases; whereas 19%, 5% and 1% of patients received cEBRT at 2, 3 and 4 sites of spinal metastases. The median follow-up duration was 54 months (range, 0 to 86). The median age was 71 years (range, 50 to 91). Our population was mainly Chinese in ethnicity (75%). Most of the patients had ECOG performance status of 0 to 1 (58%) and Charlson comorbidity index of at least 9 (70%), and were ambulant before treatment (87%).
Majority of patients were diagnosed histologically (90%), with predominantly acinar adenocarcinoma (88%) and high Gleason grade group (Gleason grade group 4 to 5, 55%). The median PSA within 1 month before RT was 170.75 ng/mL (range, 2.41 to > 10 000). MRI of spine was performed in 82% of the patients before the start of treatment.
Ninety-one percent of patients were categorized as having D’Amico high-risk disease. The medians of the revised Tokuhashi score, Tomita score, Crnalic score and Rades score were 8 (range, 5 to 12), 4 (3 to 8), 4 (0 to 6) and 35 (20 to 39), respectively. About two-third of the spinal metastases were judged to be stable (SINS 0 to 6, 68%) and had high Bilsky grade (grade 2 to 3, 66%), associated with soft tissue mass component (67%). Visceral metastases were present in one-third of the patients (31%). Eighty-two percent of patients had high metastatic burden and 62% had castration-resistant disease. The most common site of spinal metastasis was thoracic region (58%), followed by lumbar (46%), sacral (23%) and cervical regions (19%). Majority of the spinal metastases were metachronous lesions (85%). The median duration between diagnosis of prostate cancer and spinal metastases was 17 months (range, 0 to 131).
The most commonly used radiation dose fractionation was 30 Gy in 10 fractions (47%), followed by 20Gy in 5 fractions (33%). The other radiation dose fractionations included 8Gy in 1 fraction (3%), 30Gy in 12 fractions (3%), 27Gy in 9 fractions (3%), 25Gy in 10 fractions (1%) and others (10%). Some of the patients (9%) did not complete the planned radiation dose due to various reasons, such as treatment toxicity, death from prostate cancer, early commencement of systemic chemotherapy and logistic issue. About half of the population received EQD2 of less than 38.57Gy1.5 (53%). The median number of spinal levels irradiated was 5 (range, 1 to 18). Prior to receiving cEBRT, 14% of patients underwent spinal surgery, in the form of decompression laminectomy and/ or corpectomy (12%) or stabilization only (2%). Minority of patients in our cohort (14%) underwent definitive local treatment to prostate before developing spinal metastases, including cEBRT alone (8%), cEBRT plus high-dose-rate brachytherapy (2%), as well as radical prostatectomy with (2%) and without (2%) post-operative cEBRT. There was a large proportion of patients (87%) who had received ADT, including surgical castration (29%). Various systemic therapeutic agents were used, namely the novel antiandrogen agents (49%), chemotherapy (39%), ketoconazole (18%), Radium-223 (13%) and PSMA-Lutetium therapy (2%). The use of bone-modifying agent was recorded in 44% of patients.
Outcomes
Eighteen spinal sites (13.6%) developed local progression, with a median time to local progression of 8 months. The median LPFS was 8 months (range, 0 to 84). The 6- and 12-month LPFS were 60% and 42%, respectively. Local progression was detected radiologically (3/18, 17%), clinically (4/18, 22%) or both (11/18, 61%). Twelve progressing spinal sites received re-irradiation; while one underwent salvage surgery in the form of posterior decompression, laminectomy and instrumentation.
Eighty-four patients died at the time of censor. The median OS was 9 months (range, 0 to 86). The 6- and 12-month OS were 57% and 39%, respectively. Among the known causes of death, prostate cancer was the leading cause of death (12 patients), followed by infection (11), myocardial infarct (2), massive cerebral infarct (1), intracranial hemorrhage (1) and gastric adenocarcinoma (1).
The pain response outcome was insufficiently captured in approximately half of our cohort (52%). Among the patients with available data on pain outcome, 57% (39/69) spinal sites achieved complete and 39% (27/69) achieved partial response, resulting in an overall pain response rate of 96%.
The incidence of post-RT fracture was 1.5%. The incidence of grade ≥3 acute toxicities was 11%. Hematological toxicities were most commonly observed (10%), predominantly thrombocytopenia (6%) and anemia (4%). Only 1 patient had grade ≥3 non-hematological toxicity (diarrhea, 1%). There was one patient (1%) who developed grade 2 wound dehiscence, for which he was treated with antibiotics with no operative intervention required. RT was ceased due to the wound complication (completed 21 Gy out of the planned 30 Gy). There was no late toxicity recorded in our cohort.
Univariable and Multivariable Analyses for Local Progression-Free Survival and Overall Survival
For LPFS, multivariable analysis was not performed as there were only 2 covariables significantly associated with LPFS on univariable analysis (Table 2).
Univariable Cox Proportional Hazard Analyses for Freedom from Local Progression With Death as Competing Risk.
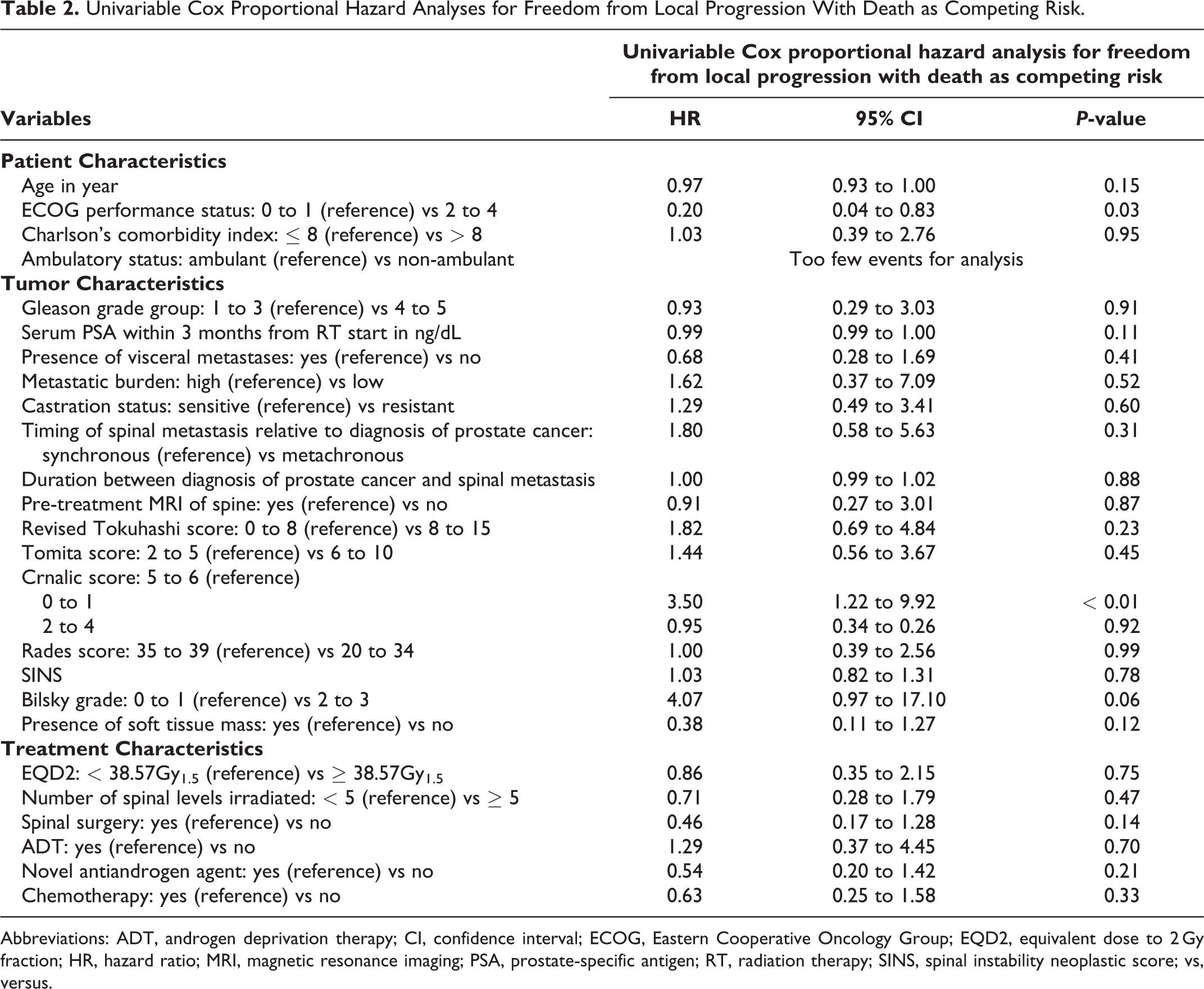
Abbreviations: ADT, androgen deprivation therapy; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; EQD2, equivalent dose to 2 Gy fraction; HR, hazard ratio; MRI, magnetic resonance imaging; PSA, prostate-specific antigen; RT, radiation therapy; SINS, spinal instability neoplastic score; vs, versus.
For OS, multivariable analysis demonstrated that better ECOG performance status (HR 2.49; 95% CI, 1.06 to 5.80; P = 0.04), castration-sensitive disease (HR, 2.86; 95% CI, 1.32 to 6.18; P < 0.01), spinal surgery (HR, 2.73; 95%, 1.13 to 6.57; P = 0.03) and the use of novel antiandrogen agent (HR, 2.57; 95% CI, 1.44 to 4.58; P < 0.01) were identified as independent predictors for improved OS (Tables 3 and 4).
Univariable Cox Proportional Hazard Analyses for Death From Any Cause.
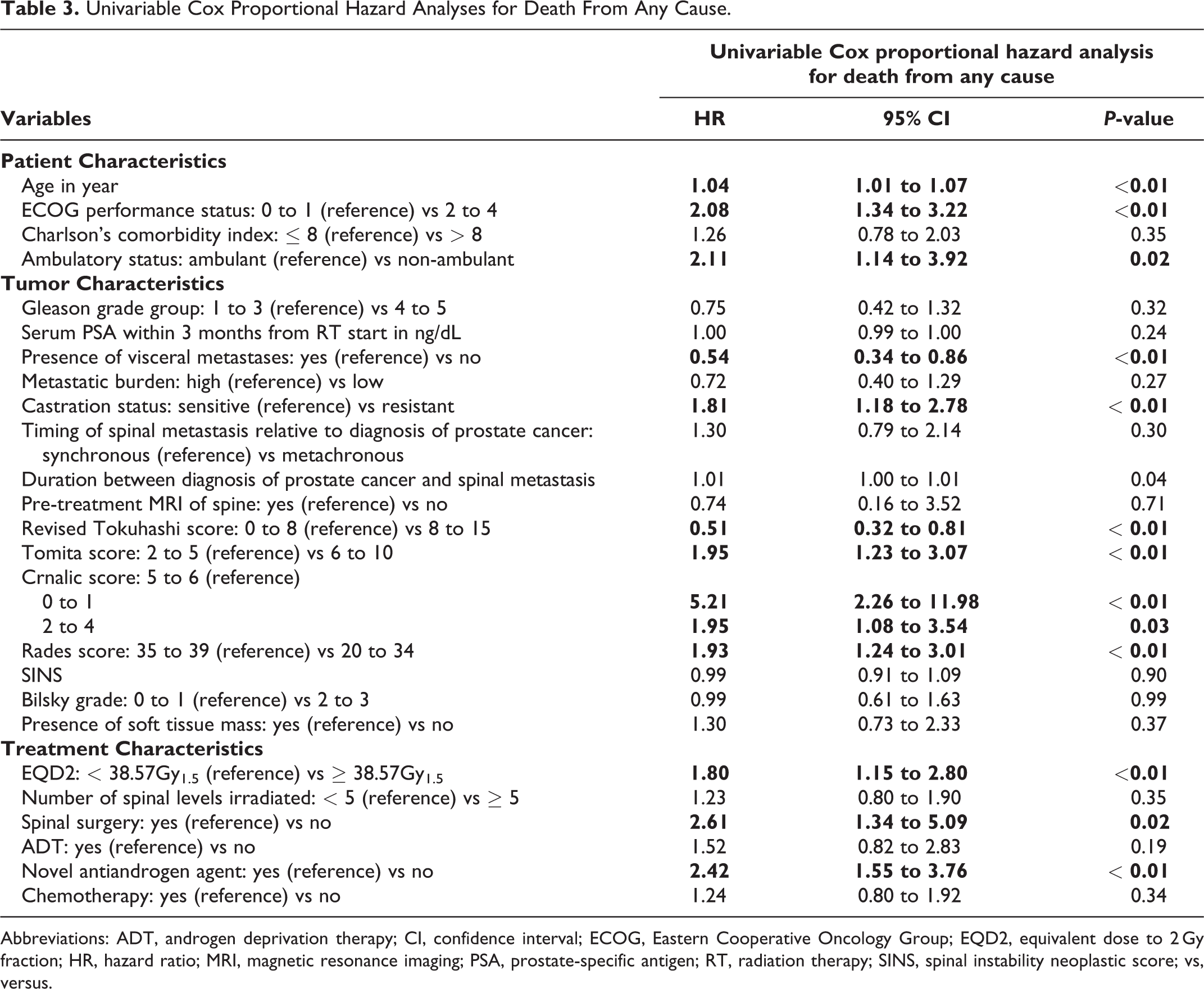
Abbreviations: ADT, androgen deprivation therapy; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; EQD2, equivalent dose to 2 Gy fraction; HR, hazard ratio; MRI, magnetic resonance imaging; PSA, prostate-specific antigen; RT, radiation therapy; SINS, spinal instability neoplastic score; vs, versus.
Multivariable Cox Proportional Hazard Analyses for Death From Any Cause.
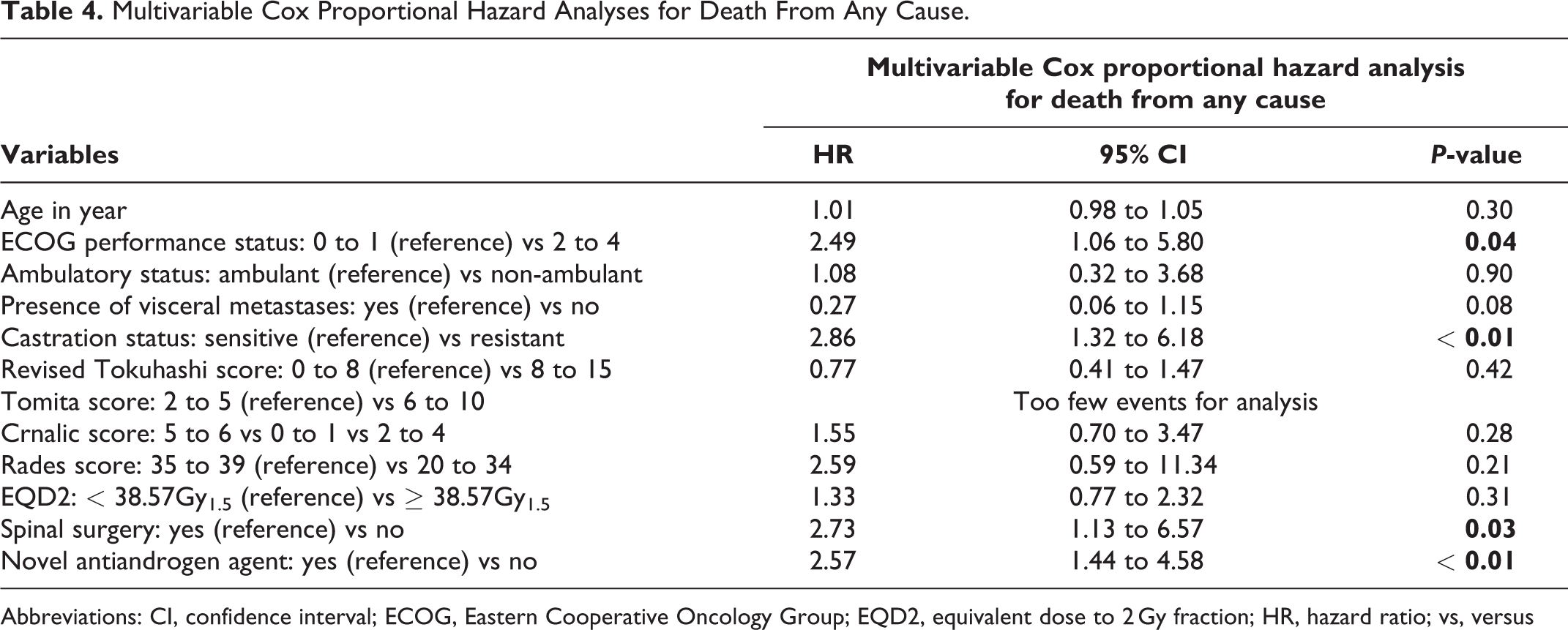
Abbreviations: CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; EQD2, equivalent dose to 2 Gy fraction; HR, hazard ratio; vs, versus
Discussion
We report the outcomes of patients diagnosed with spinal metastases from prostate cancer who were treated with palliative cEBRT. The median OS was short at 9 months. The rate of local progression was low at 13.6%, with a median interval of 8 months. The overall pain response rate was 96%. The overall incidence of grade ≥3 acute toxicities was as low as 11% and they were mostly hematological.
Our study results are comparable with other studies.38,39 Rades et al. retrospectively evaluated 281 prostate cancer patients who received cEBRT for MSCC. 38 The local progression occurred at a rate of 11%, after a median interval of 6 months. Local progression in this study was defined as MSCC associated with motor deficits in the pre-irradiated spinal region and confirmed by CT or MRI. A prospective observational cohort study by Maranzano et al. included 44 patients with MSCC from prostate cancer who were treated with either a split-course (61%) or a short-course RT regimen. 39 They observed an overall pain response rate of 82%. 39 Cereceda et al. conducted a retrospective analysis of 119 patients with vertebral metastases from prostate cancer treated with various treatment modalities. 14 Among 103 patients who were treated with cEBRT, the overall response rate in term of pain and neurologic improvement was 85%.
Our study found that higher radiation dose (EQD2 of ≥ 38.57Gy1.5) was not correlated with better local control. There have been several prospective randomized trials comparing different radiation fractionation regimens (single vs multiple fractionations) for the treatment of painful osseous metastases from any primary malignancy suggesting similar effectiveness of the various radiation fractionation regimens. Radiation Therapy Oncology Group (RTOG) 9714 included 898 patients with painful osseous metastases (nearly 50% from prostate cancer and 50% at spinal sites) and found no statistical difference in pain response at 3 months between 8 Gy in 1 fraction and 30 Gy in 10 fractions, with overall response rates of 65% and 66% respectively. 40 A few other trials (approximately one third from prostate cancer) also reported no difference in overall response rates between 8 Gy in 1 fraction and 20 Gy in 5 fractions.41-43 Maranzano et al.’s study focusing on MSCC from prostate cancer showed that there was no significant difference in term of response rate between split-course (15 Gy in 3 fractions, 4-day rest, and then 15 Gy in 5 fractions) and short-course (8 Gy in 1 fraction, 7-day rest, and then 8 Gy in 1 fraction) RT regimens, 39 although the finding should be interpreted with caution as the treatment allocation in this prospective study was not randomized where a short-course regimen was adopted mainly for patients with poorer prognosis. On the contrary to these studies, Rades et al.’s study on MSCC from prostate cancer reported that long-course RT schedule (30 Gy in 10 fractions, 37.5 Gy in 15 fractions and 40 Gy in 20 fractions) was significantly associated with better local control compared with short-course RT schedule (8 Gy in 1 fraction and 20 Gy in 5 fractions), with 2-year local control rates of 94% and 73% respectively. The inconsistency of the findings could be related to the variations in the outcome measures and the dose fractionation regimens used in the comparison arms. Besides, these studies included patients with MSCC only,38,39 compared to our cohort who had a mixture of MSCC and symptomatic vertebral metastases. MSCC is often associated with soft tissue mass component and hence thought to have increased tumor burden whereby the pain response is expected to be lower compared to those with uncomplicated vertebral metastases. While there is no robust evidence suggesting definite dose-response relationship, low radiation dose with shorter schedule should be sufficient to achieve local palliation of spinal metastases with optimized convenience for both patients and caregivers, particularly in a cohort with short median survival of less than 1 year.
The median OS was 9 months in our present study. This is comparable with other studies which reported median OS ranging from 4 to 17 months.14,39,44,45 We demonstrated that better ECOG performance status, castration-sensitive disease, spinal surgery and the use of novel antiandrogen agent were significant predictors for better OS. There could be effect of collinearity between performance status and spinal surgery as patients with better performance status were more likely to have undergone spinal surgery. There are a number of validated scoring systems used to prognosticate the survival of patients with vertebral metastases, namely the revised Tokuhashi, Tomita score, Crnalic score and Rades score.8,28-30,44 Meng et al. validated the use of Tomita score in a cohort of prostate cancer patients who underwent surgical intervention to the spine, suggesting that a Tomita score of no more than 6 is a favorable prognostic factor. 12 Crnalic score 8 and Rades score were developed to predict the survival for patients with MSCC from prostate cancer.30,44 In our present study, we could not validate the use of these scoring tools in survival prognostication on our multivariable analysis. Various other prognostic factors have also been reportedly described to be linked with survival in patients with PCSM, including the use of ADT, 46 number of extra-spinal organs involved, 47 number of spinal levels involved, 48 visceral metastases, 12 PSA level at the diagnosis of spinal metastasis, 49 duration between diagnosis of prostate cancer and spinal metastases, 49 and presence of additional metastasis at the diagnosis of spinal metastasis. 49 However, we could not demonstrate the associations between survival and most of these factors.
There are several strengths in our study. First, we evaluated the outcomes of spinal metastases with and without MSCC. This differs from the previous studies which focused on MSCC exclusively;38,39,46 it is recognized that patients with MSCC represent a subset of patients with more ominous prognosis owing to the higher chance of permanent neurologic deficits. 50 Second, this study was performed in an era with contemporary treatment modalities, including 3DCRT technique and more effective systemic therapy such as novel antiandrogen agents. Approximately half of our population received novel antiandrogen agents. Third, we investigated several published scoring tools used for survival prognostication and assessed whether they could be validated in our local population. Fourth, our institution follows a standardized RT protocol and strict quality assurance. Our study was limited by its retrospective study design and the lack of patient-reported outcomes. Some important data was not adequately captured, for instance, a proportion of patients had missing data on pain response. The patients in our cohort did not routinely have imaging on follow up. The short median survival has probably restricted the evaluation of longer-term local control and late toxicity.
The implication of this study is that the excellent palliation in term of local control and pain relief justifies the use of cEBRT in patients with spinal metastases from prostate cancer in this modern era. As there is no dose-response relationship established, a lower dose fractionation is equally effective to achieve symptom palliation. A survival prognostication tool should act as an adjunct when tailoring personalized treatment approach. Future studies should explore the impact of palliative cEBRT in patient-reported outcomes and quality of life.
Conclusion
In our prostate cancer cohort, cEBRT is an effective treatment modality for local palliation of spinal metastases. More aggressive treatment approach, such as SBRT and surgical resection, should be considered for patients with excellent performance status and castration-sensitive disease in light of their expected longer survival in the era where novel antiandrogen therapy is commonly used. Further studies are warranted to identify the predictors for radiotherapy response in this population.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_2192568221994798 - Outcomes of Patients With Spinal Metastases From Prostate Cancer Treated With Conventionally-Fractionated External Beam Radiation Therapy
Supplemental Material, sj-docx-1-gsj-10.1177_2192568221994798 for Outcomes of Patients With Spinal Metastases From Prostate Cancer Treated With Conventionally-Fractionated External Beam Radiation Therapy by Chia Ching Lee, Jeremy Tey, Timothy Cheo, Chau Hung Lee, Alvin Wong, Naresh Kumar and Balamurugan Vellayappan in Global Spine Journal
Footnotes
Abbreviations
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.