
Abstract
Study Design:
Retrospective radiological analysis.
Objective:
To explore whether proximal fusion level above first coronal reverse vertebrae (FCRV) could decrease risk of adjacent segment degeneration (ASD) in degenerative lumbar scoliosis (DLS).
Methods:
One hundred and 16 DLS patients were divided into 2 groups according to occurrence of ASD: study group (ASD positive group) and control group (ASD negative group). FCRV was defined as the first vertebrae that presents opposite orientation of asymmetric Hounsfield unit (HU) ratio from the other vertebrae within major curve. Incidence of ASD was evaluated in subgroups according to location between FCRV and upper instrumented vertebrae (UIV).
Results:
The fusion level was shorter in study group than that in control group. There were 12 patients presented FCRV 2-level proximal than SV, 32 patients presented FCRV 1-level proximal than SV, 35 patients presented the same vertebra of FCRV with SV, 23 patients presented FCRV 1-level distal than SV, 14 patients presented FCRV 2-level distal than SV. When UIV located above FCRV, no patient presented ASD, while 15.4% patients presented ASD when UIV located on FCRV. In study group, proximal scoliosis progression was detected in 1 patient (3.9%) when UIV located on FCRV, and 17 patients (29.8%) when UIV located below FCRV.
Conclusions:
Proximal fusion level above FCRV could decrease the risk of ASD in DLS, especially for the proximal scoliosis progression. FCRV represent the transitional point of the mechanical load on coronal plane, and may be within a more stable condition than stable vertebrae measured from radiographs.
Introduction
Postoperative adjacent segment degeneration (ASD) is not uncommon followed posterior decompression and instrumented fusion for degenerative lumbar scoliosis (DLS), it may progressed to adjacent segment disease or even coronal/sagittal spine imbalance.1-3 Selection of upper instrumented vertebrae (UIV) has been proved to be related to the postoperative proximal ASD. 4 Bridwell 5 stated that choosing the proximal level requires identification of the stable vertebra (SV), neutral vertebra (NV), upper end vertebrae (UEV) and horizontal vertebra (HV) on the coronal plane, curve progression developed more commonly when the proximal fusion stopped at the UEV or below in DLS. Ha et al. 6 found that radiographic adjacent segment pathology was statistically higher in patients who received fusions below the proximal neutral vertebrae. However, identification of these vertebrae are performed on standing full-spine radiograph, there may be great variability in the identification of the vertebrae mentioned above, especially for patients with severe degenerated para-spinal muscles, they may present different SV or HV from start of standing to long-time standing due to the para-spinal muscle fatigue. 7
Measuring Hounsfield unit (HU) from computed tomography (CT) scans has been proposed to be a useful technique for assessing vertebral bone quality, it can provide direct measurement data of bone density inside vertebral body, the reliability and accuracy of HU measurement are not affected by posture.8,9 Based on HU measurement of convex and concave side of the vertebrae separately, our previous work demonstrate that progression of degenerative scoliosis increase the asymmetrical vertebral degeneration that manifested as high HU value within concavity and low HU value within convexity of the same vertebrae. 10 When measuring the concave-convex HU of vertebrae from distal to cranial, there must be a vertebrae that present opposite orientation of asymmetric HU ratio from the other vertebrae within the major curve, we defined it as first coronal reverse vertebrae (FCRV). It is reasonable to believe that the disc below the FCRV may bear large shear force, if the UIV is located below the FCRV, the stress concentration between UIV and FCRV that may lead to proximal curve progression should not be underestimated, but it has never been proved.
The purpose of this study was to explore whether proximal fusion level above FCRV could decrease the incidence of postoperative proximal ASD in DLS patients.
Methods
Patients
This study was approved by the Institutional Review Board of our hospital before data collection and analysis, the IRB approval number is IRB00006761-M2020291. The need for individual consent was waived. Inclusion criteria: 1. DLS patients with age more than 45 years at the time of surgery. 2. Minimum follow-up of 2 years. 3. Posterior instrumentation from thoraco-lumbar (T10-L2) to L5 or sacrum. Exclusion criteria: 1. previous surgery for degenerative lumbar disease. 2. Spinal infections or metabolic disease that may potentially affect the surgical outcome. 3. The anatomical identification was difficult to recognize for radiological measurement.
By retrieving the medical records from January 2015 to April 2018 in our hospital, 116 patients who met both the inclusion and exclusion criteria were retrospectively reviewed. There were 28 men and 88 women. They were divided into 2 groups according to the occurrence of ASD at 2-year follow up: study group (ASD positive group) and control group (ASD negative group).
Clinical and Radiological Data
The patient demographics including age, gender, body mass index (BMI) were recorded. Perioperative parameters included operation time, estimated blood loss (EBL), UIV location, LIV location, fusion level were reviewed.
All radiographic parameters were measured by 2 independent observers (first and second author), and were averaged to give a mean value for statistical analysis. Postoperative proximal ASD was evaluated at 2 years follow up, diagnosis of ASD include proximal scoliosis progression on the coronal plane and proximal junctional kyphosis (PJK) on the sagittal plane. The proximal scoliosis progression (PSP) was defined as the disc wedging increased 10 degrees from postoperative to 2-year follow up on the AP radiograph. PJK was defined by 2 criteria: proximal junction sagittal Cobb angle >10° and proximal junction sagittal Cobb angle at least 10° greater than the preoperative measurement, the presence of both criteria was necessary to be considered abnormal.
The Cobb angle of the major lumbar curve, disc wedging above UIV, coronal balance distance (CBD) were measured on the coronal plane. Sagittal vertical axis (SVA), proximal junctional angle (PJA), lumbar lordosis (LL), sacrum slope (SS) and pelvic incidence (PI) were measured on the sagittal plane. (Figure 1)
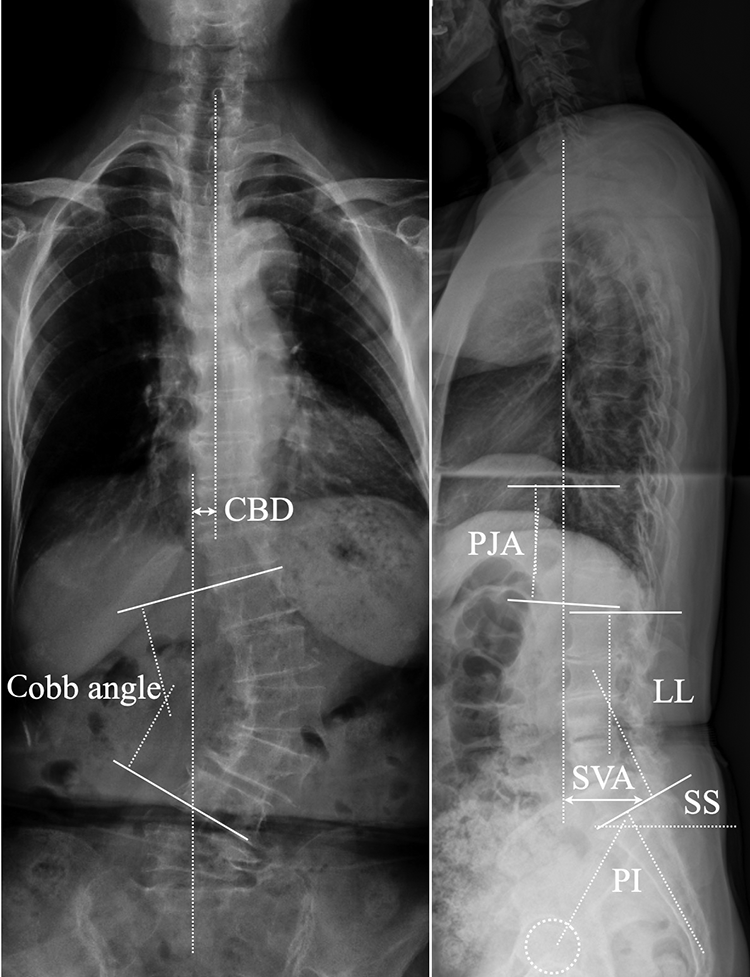
Schematic diagram of coronal and sagittal spinal parameters measurement. Cobb’s angle was measured between the most tilted vertebrae. Coronal balance distance (CBD) was the distance between C7 plumb line and central sacral vertical line (CSVL). Sagittal vertical axis was measured as the distance from C7 plumb line to the perpendicular line drawn from superior posterior endplate of S1. Proximal junctional angle was measured as the Cobb angle between the 2 level cephalad endplates to the UIV and the caudal endplate of the UIV. Lumbar lordosis was measured as the lines projected from upper endplate of L1 and upper endplate of S1. Pelvic incidence (PI) was defined as the angle between the line perpendicular to the sacral plate and the line connecting the midpoint of the sacral plate to the bicoxofemoral axis. Sacrum slope (SS) was the angle between the S1 superior end plate and a horizontal line.
The HU measurement for each vertebra was obtained by using a protocol described by Schreiber. 11 Regions of interest were measured on coronal images of the vertebrae at 3 separate locations: immediately posterior to the anterior vertebrae margin, in the middle of the vertebral body, and anterior to the posterior vertebrae margin. HU measurement within the concave and convex side of the vertebrae were obtained separately from T10 to sacrum. The HU values from the 3 coronal slices were averaged to give a mean HU value for each vertebral body. FCRV was defined as the first vertebrae that presents opposite orientation of asymmetric HU ratio from the other vertebrae within the major curve on the coronal plane. (Figures 2–4)
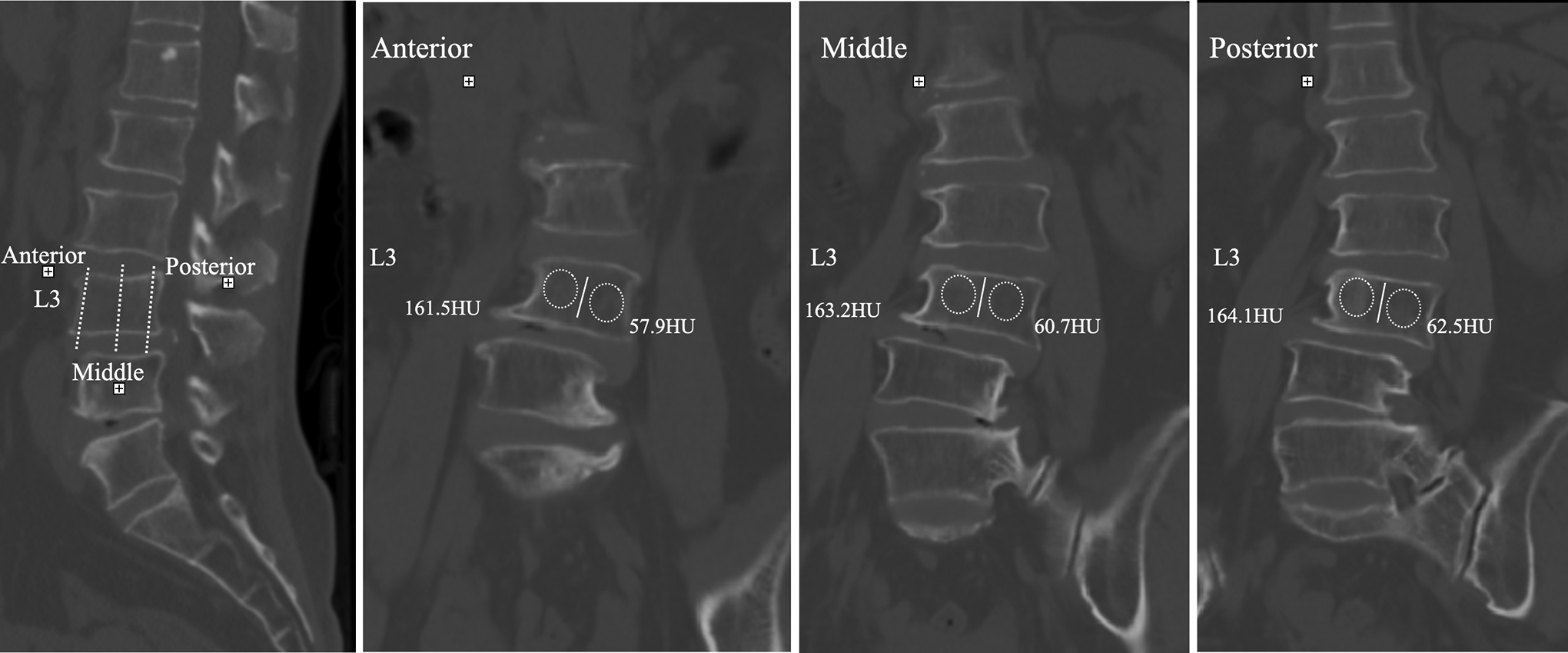
Schematic diagram of HU measurement within the concave and convex sides separately at 3 locations of the vertebrae on coronal plane: immediately posterior to the anterior vertebrae margin, in the middle of the vertebral body, and anterior to the posterior vertebrae margin. For each measurement, the largest possible elliptical region of interest was drawn, excluding the cortical margins to prevent volume averaging.
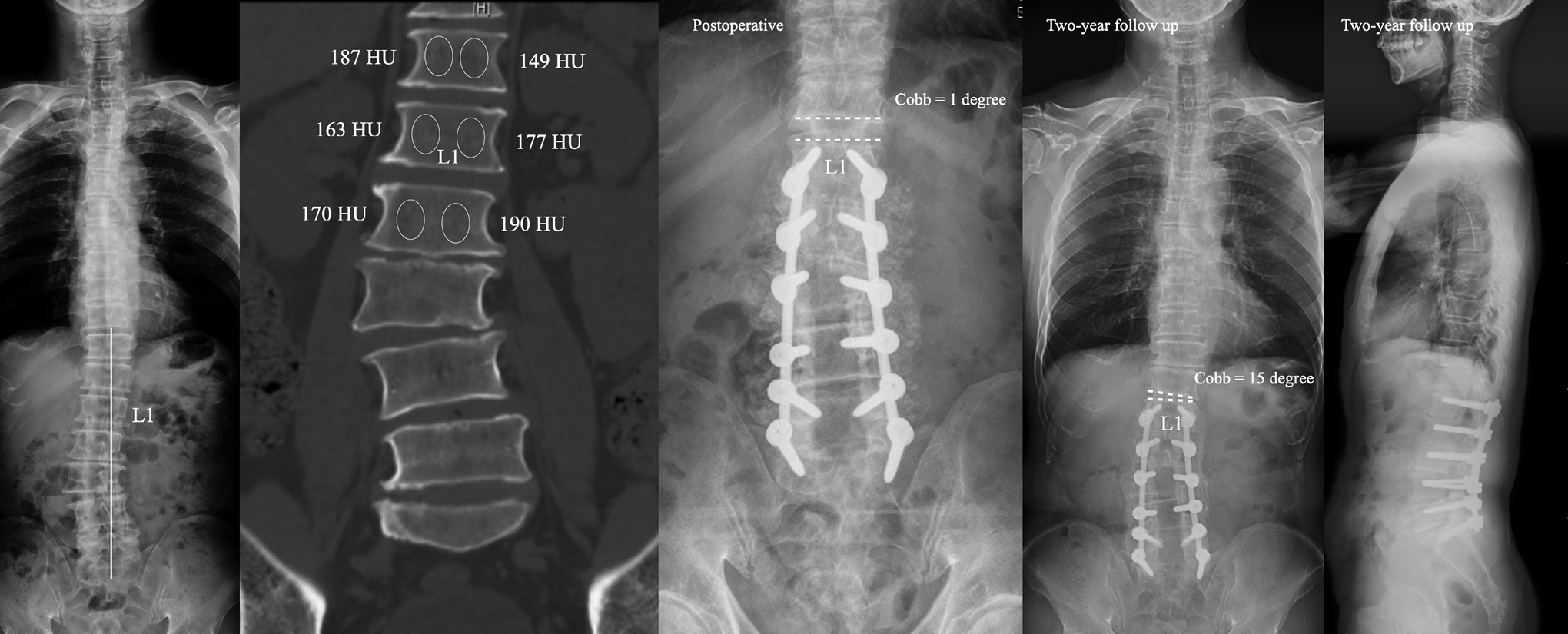
The case in the study group. Male, 57 years. Preoperative X-ray showed L1 was the stable vertebrae and CT showed T12 was the FCRV. Surgical strategy was fusion from L1 to S1. Disc wedging angle above the UIV was 1 degree at immediate postoperative. Disc wedging angle above the UIV was 15 degrees at 2-year follow up without PJK.
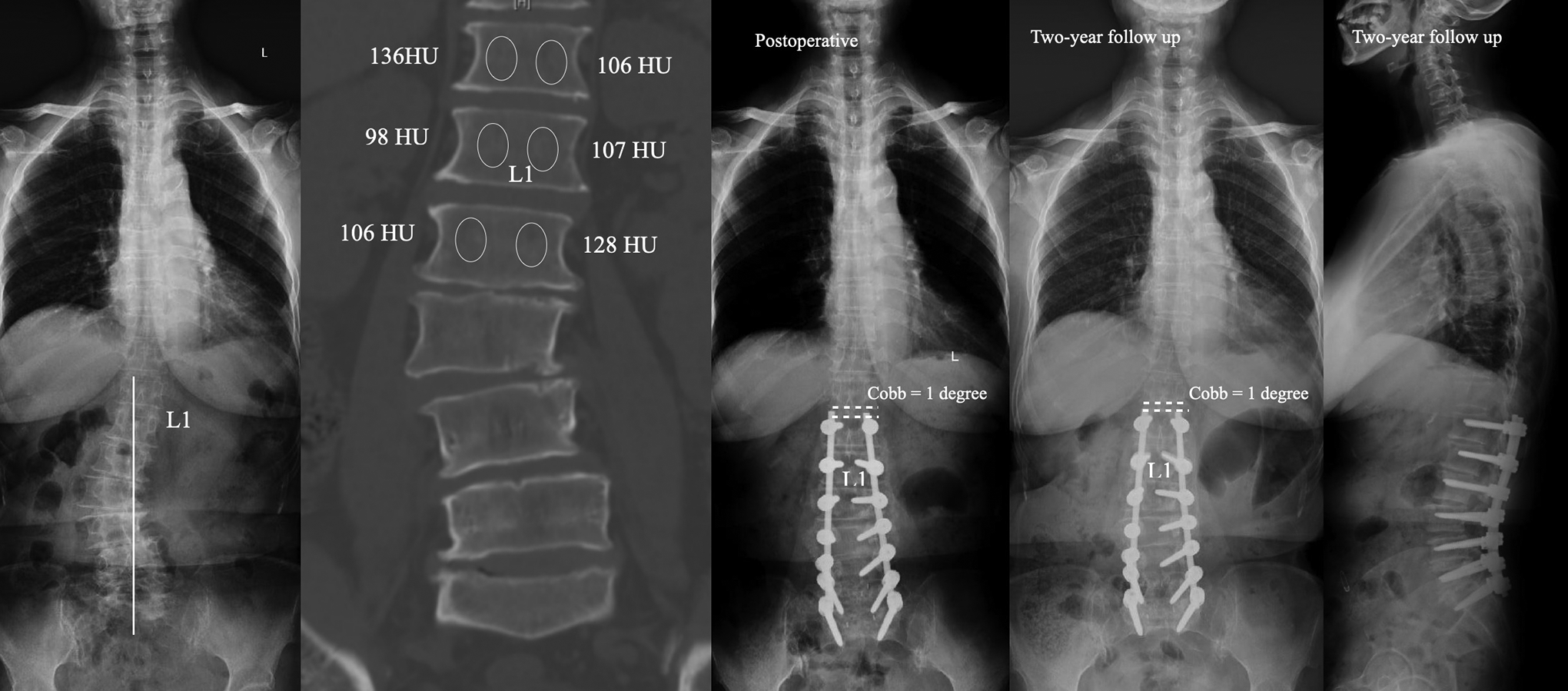
The case in the control group. Female, 62 years. Preoperative X-ray showed L1 was the stable vertebrae and CT showed T12 was the FCRV. Surgical strategy was fusion from T12 to S1. Disc wedging angle above the UIV was 1 degree at immediate postoperative. Disc wedging angle above the UIV was 1 degree at 2-year follow up without PJK.
Statistical Analysis
Data was analyzed using Statistical Product and Service Solutions software (version 17; SPSS, Chicago, IL). Continuous variables were recorded as mean ± standard deviation, and categorical variables were expressed as frequency or percentages. An independent t test or 1-way analysis of variance (ANOVA) was used to analyze the difference of continuous variables. An χ2 analysis and Fisher’s exact test were used to examine the differences among categorical variables. Statistical significance was set at P < 0.05.
Results
At 2 years follow up, 30 patients presented ASD and were enrolled into study group, among them, 9 patients presented PJK, 18 patients presented PSP, 3 patients presented both PJK and PSP. While 86 patients presented no ASD and were enrolled into control group.
There was no significant difference in age, gender, BMI, preoperative disc degeneration above UIV between study and control groups. There was no significant difference in both coronal and sagittal preoperative spinal parameters, including Cobb angle, CBD, SVA, LL, SS, PI, PI-LL mismatch between study and control groups. (Table 1)
Comparison of General and Radiological Data Between Study and Control Groups.
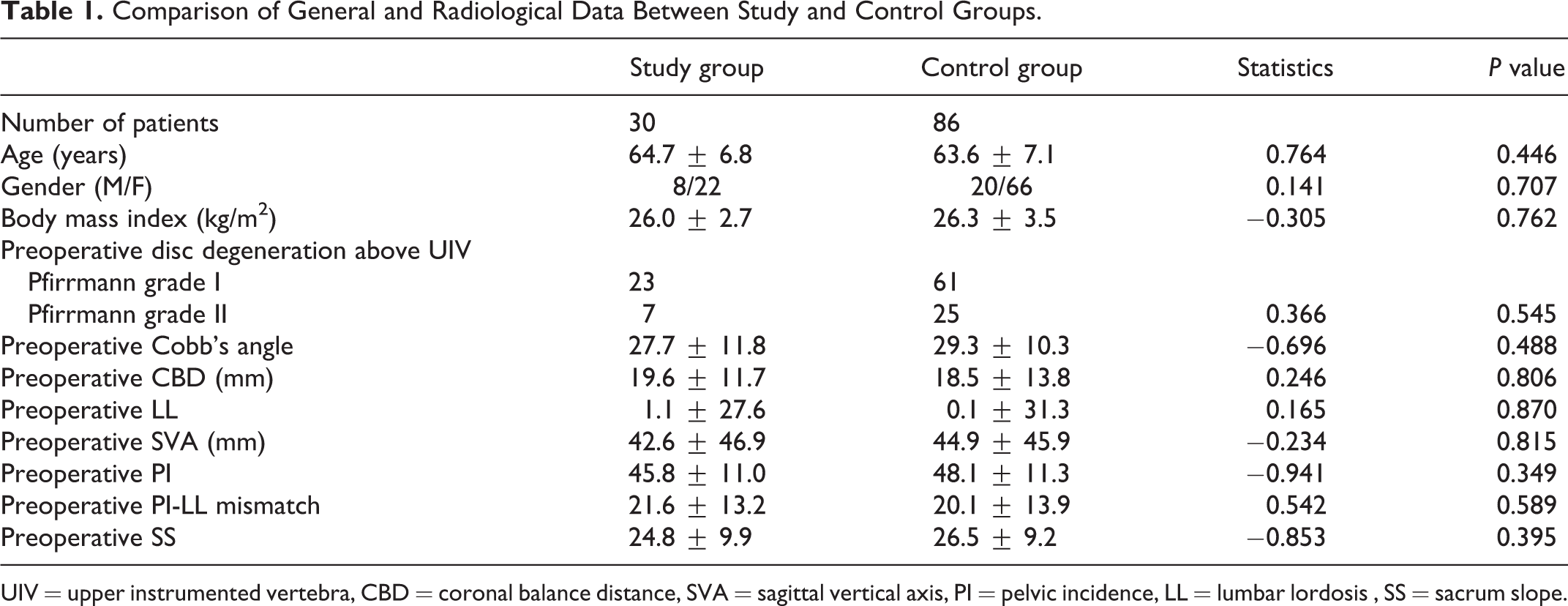
UIV = upper instrumented vertebra, CBD = coronal balance distance, SVA = sagittal vertical axis, PI = pelvic incidence, LL = lumbar lordosis , SS = sacrum slope.
The fusion level was shorter in study group than that in control group (t = −4.376, P = 0.001). There was no significant difference in LIV location, surgical time, blood loss between study and control groups. There was no significant difference in change of both coronal and sagittal spinal parameters, including Cobb angle, CBD, SVA, LL, SS between study and control groups. (Table 2)
Comparison of Surgical Data Between Study and Control Groups.
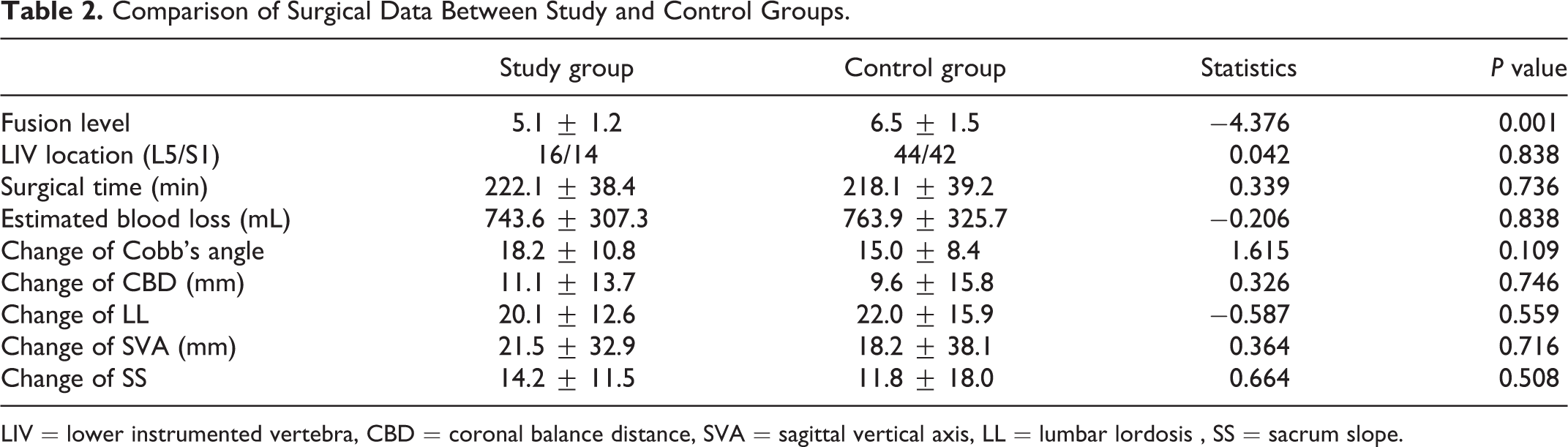
LIV = lower instrumented vertebra, CBD = coronal balance distance, SVA = sagittal vertical axis, LL = lumbar lordosis , SS = sacrum slope.
FCRV was primarily located on T12 (35.3%), L1 (23.3%), T11 (22.4%). SV was primarily located on T12 (34.5%), T11 (21.6%).(Table 3) There were 12 patients presented FCRV 2-level proximal than SV, 32 patients presented FCRV 1-level proximal than SV, 35 patients presented the same vertebra of FCRV with SV, 23 patients presented FCRV 1-level distal than SV, 14 patients presented FCRV 2-level distal than SV. (Figure 5)
Distribution of FCRV and SV in all the Patients.
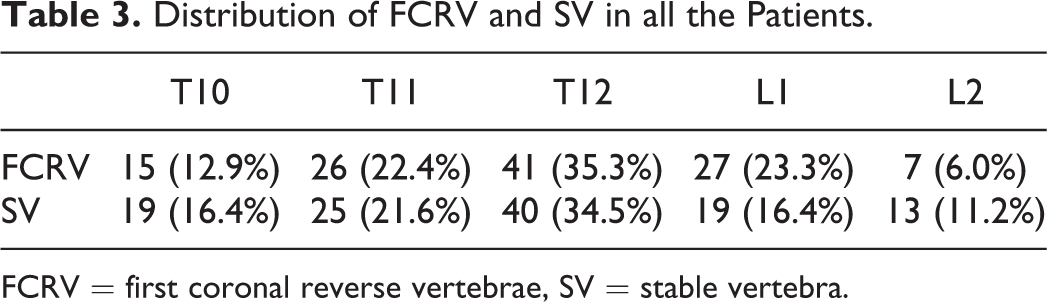
FCRV = first coronal reverse vertebrae, SV = stable vertebra.
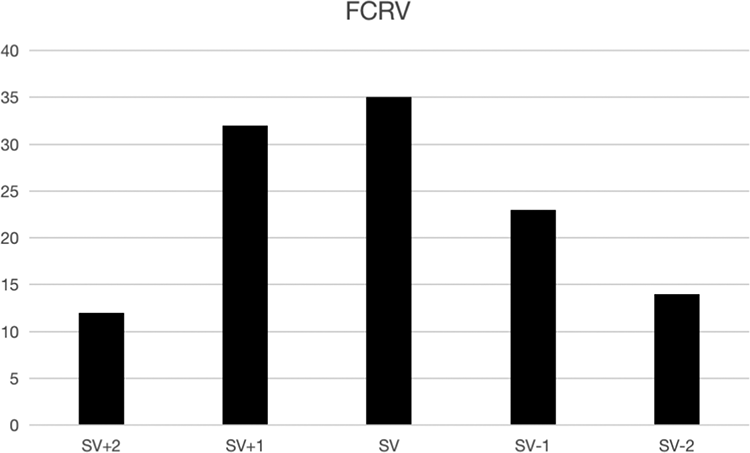
The relationship between stable vertebra (SV) and FCRV.
No patient presented ASD when UIV located above FCRV, while 15.4% of the patients presented ASD when UIV located on FCRV. 13.3% of the patients presented ASD when UIV located above SV, while 28.6% of the patients presented ASD when UIV located on SV. (Table 4)
Prevalence of ASD in Varied Groups According to Relation Between FCRV, SV and UIV.
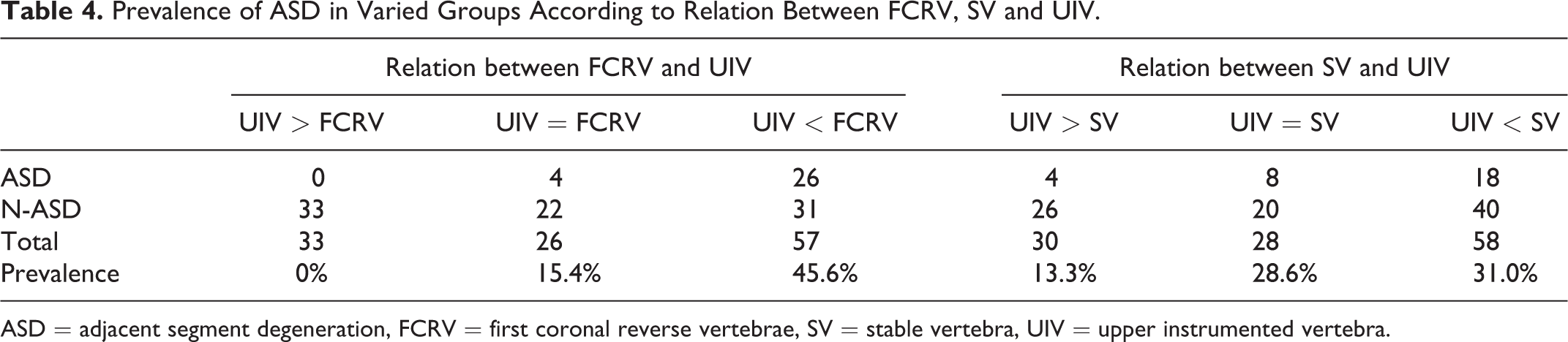
ASD = adjacent segment degeneration, FCRV = first coronal reverse vertebrae, SV = stable vertebra, UIV = upper instrumented vertebra.
In the study group, PJK was detected in no patient when UIV located above FCRV, and 9 patients (10.8%) when UIV located on and below FCRV. PSP was detected in no patient when UIV located above FCRV, and 18 patients (21.6%) when UIV located on and below FCRV. PJK+PSP was detected in no patient when UIV located above FCRV, and 3 patients (3.6%) when UIV located on and below FCRV. There was significant difference in the incidence of ASD between UIV > FCRV and UIV≦FCRV subgroups (χ2 = 16.089, P ≤ 0.001). (Table 5)
Prevalence of ASD Between UIV > FCRV and UIV≦FCRV Subgroups.
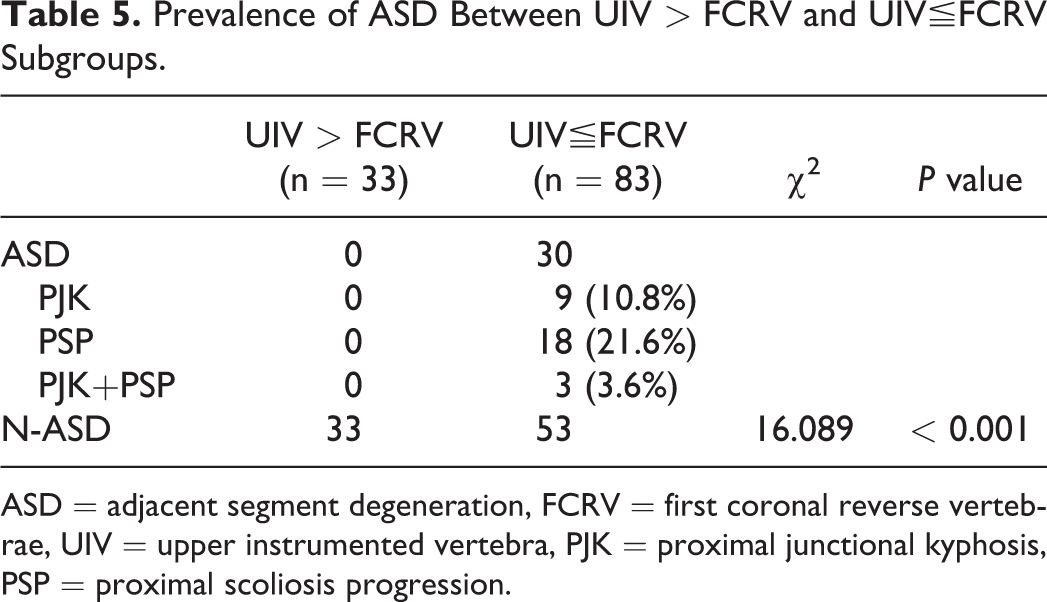
ASD = adjacent segment degeneration, FCRV = first coronal reverse vertebrae, UIV = upper instrumented vertebra, PJK = proximal junctional kyphosis, PSP = proximal scoliosis progression.
Discussion
In the current study, we demonstrate that patients in study group present shorter fusion level and no difference of LIV location when compared to the patients in control group, suggesting that selection of UIV may be closely related to the occurrence of proximal ASD. Choosing the UIV should be based on factors thought to be important to the overall survival of spinal segments adjacent to a spinal fusion, these factors include starting with healthy adjacent segments with no degeneration or instability in any plane, stopping adjacent to spinal segments with normal sagittal, coronal, and axial alignment, the proximal spine should be sited in the stable region, with the coronal vertical wheel base of less than 2 cm, the UIV should not be rotated.12-14 Using these criteria, chosen UIV will vary depending on the patient’s degenerative pathoanatomy, curve characteristics, and sagittal profile. Although the above consensus provides some guideline for the selection of UIV in degenerative scoliosis patients, it may be cumbersome and non-quantitative to implement in clinical practice. It is generally considered that the more distal proximal fusion level at a neutral and stable vertebra may be satisfactory in selection of proximal fusion level for adult lumbar scoliosis, but identification of SV and NV based on standing full-spine radiograph may be not so accurate as expected, and may lead to unpredictable adjacent segment degeneration, because patients with severe degenerated para-spinal muscles may present different SV and NV from start of standing to long-time standing due to the para-spinal muscle fatigue. 15 SV measured from X-ray may be not within a stable state as expected previously.
The primary strength of the current study is that we firstly define the FCRV based on HU measurement from CT examination, which is the first vertebrae that presents opposite orientation of asymmetric HU ratio from the other vertebrae within the major curve on the coronal plane. Radiological presentation of asymmetrical vertebral degeneration could indirectly reflect the biomechanical properties of the vertebral body, FCRV represent the transitional point of the mechanical load on coronal plane, and may be within a more stable condition than stable vertebrae measured from radiographs. An examination of changes in the internal response of the spine structure due to asymmetric vertebral degeneration will provide a better understanding of the radiological presentations. Périé et al. 16 explored the correlations between displacement of the nucleus zone within intervertebral discs and the migration of mechanical center within vertebral bodies in scoliotic patients, the nucleus zone migration occurred in the convexity of the curvature whereas the mechanical migration occurred in the concavity of the curvature, indicating that the gravity load transmitted through the convex side of the vertebrae decreased, and the load through the concave side of the vertebrae increased. Wolff’s law theorizes that repetitive loading of bone will cause adaptive responses enabling the bone to better cope with these loads, which may explain the asymmetric HU value within concave and convex side of the same vertebrae in DLS patients. If load to a bone increases, remodeling will occur so that the bone is strengthened to resist such loads. If load to a bone decreases, homeostatic mechanisms will shift toward a catabolic state, and bone will be equipped to withstand only the loads to which it is subjected.17-19 FCRV presents opposite asymmetrical vertebral degeneration from FCRV-1, it is reasonable to believe that the disc between FCRV and FCRV-1 may bear large shear force at preoperative, the shear force may drastically increase when UIV is located below the FCRV due to the stress concentration between UIV and FCRV at postoperative.
From the perspective of vertebral body distribution, FCRV and SV were located within the thoracolumbar junction (T10-L2), which has unique anatomic characteristics. It serves as the transition from the immobile thoracic spine to the mobile lumbar spine. The sagittal alignment changes from thoracic kyphosis to lumbar lordosis, there is a change in the orientation of the facet joints from the coronal plane proximally to the sagittal plane distally. In most patients with primary degenerative lumbar curves and acceptable thoracic and thoracolumbar sagittal alignment, the surgeon can stop the fusion in the thoracolumbar junction, but UIV at T10 to T12 differs from UIV at L1 or L2. 13 Swank et al. 20 demonstrate that instrumented lumbosacral fusions with UIV at L1 or L2 have an unacceptably high mechanical failure rate in adult patients and cannot be recommended. Simmons et al. 21 reported adjacent segment problems in 60% of elderly patients who had lumbar fusion extending to L1 or L2. Fusion to T11 or T12 was acceptable when UIV was above UEV, since there was no significant difference in the rate of proximal adjacent segment degeneration between fusion to T10 and fusion to T11 or T12.7,22 It is reasonable to believe that UIV above FCRV may potentially decrease the incidence of postoperative proximal ASD, due to the fact that FCRV was primarily located on T12 (35.3%).
The second strength of the current study is that we prove the FCRV can provide a meaningful reference in the selection of UIV for DLS patients, UIV on or above FCRV is superior to SV in reducing the incidence of proximal ASD for DLS patients that received posterior fusion surgery. The most possible explanation is that FCRV measured from CT examination may be within a more stable state than SV measured from X-ray. The identification of SV on standing full-spine radiographs may be not so accurate as expected due to the paraspinal muscle fatigue. Contrarily, the reliability and accuracy of vertebral HU measurement are not affected by the posture, it is reasonable to believe that FCRV is more reliable and objective than SV in the preoperative evaluation of UIV for DLS patients that underwent long posterior fusion. When CT scans are available, HU assessments can easily be obtained by the practitioner to provide additional information on global and regional bone density with no additional cost. 11
There are several limitations in this study. First, it was a retrospective review of pre-existing data and suffers from the inherent limitations of such studies. Second, the subjects selected are all Chinese Han individuals, whether the conclusion is applicable to other ethnic groups needs to be further investigated in the future.
Conclusion
Proximal fusion level above FCRV could decrease the risk of ASD in DLS, especially for the proximal scoliosis progression. FCRV represent the transitional point of the mechanical load on coronal plane, and may be within a more stable condition than stable vertebrae measured from radiographs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by AOSPINE China Research Grant (2017-06).