
Abstract
Study Design:
Retrospective study.
Objectives:
Although the role of surgery in the management of metastatic spinal cord compression (MSCC) has been well established, elderly patients may still be denied surgery because of higher risk of complications and shorter life expectancy. The purpose of this study was to determine whether elderly patients with MSCC could benefit from surgery and discuss the criteria for surgical decision-making in such patients.
Methods:
Enrolled in this study were 55 consecutive patients aged 75 years or older who were surgically treated for MSCC in our center. Prognostic factors predicting overall survival (OS) were explored by the Kaplan-Meier method and Cox regression model. The quality of life (QoL) of the patients was evaluated by the SOSGOQ and compared using Student’s t test. Risk factors for postoperative complications were identified by Chi-square test and multiple logistic regression analysis.
Results:
Surgical treatment for MSCC substantially improved the neurological function in 55.8% patients and QoL in 88.5% patients with acceptable rates of postoperative complications (16.4%), reoperation (9.1%), and 30-day mortality (1.8%). Postoperative ECOG-PS of 1-2, total en-bloc spondylectomy (TES), and postoperative chemotherapy were favorable prognostic factors for OS, while a high Charlson Comorbidity Index (CCI) and a long operation time were risk factors for postoperative complications.
Conclusions:
Surgery should be encouraged for elderly patients with MSCC 1) who are compromised by the current or potential neurological dysfunction; 2) with radioresistant tumors; 3) with spinal instability; and 4) with no comorbidity, ECOG-PS of 0-2, and systemic treatment adherence. In addition, surgery should be performed by a skilled and experienced surgical team.
Keywords
Introduction
Metastatic spinal cord compression (MSCC) is a disastrous complication of cancer that affects 5-14% of patients during the course of their malignant disease. 1 Owing to the continuous improvement in cancer treatment, patients with advanced stage cancer live longer and the proportion of elderly cancer patients with MSCC is also increased. 2 As an oncologic emergency, MSCC may cause paraplegia of the affected patients, leading to an inevitably striking change in patients’ quality of life (QoL) if untreated. 3 It is well established that surgery represents the most direct and effective method that leads to immediate relief of spinal compression.1,4,5 However, many elderly patients may be denied surgical treatment due to their poor cardio-pulmonary function, frequent comorbidities and a relatively short life expectancy. 6
Whether elderly cancer patients can benefit from surgical treatment for MSCC remains controversial. In a matched-pair analysis, Rades et al. compared 42 elderly cancer patients older than 65 years who received surgery plus postoperative radiotherapy for MSCC and 84 matched elderly patients who received radiotherapy alone. The results showed that elderly patients with MSCC did not significantly benefit from surgery plus radiotherapy. 7 Liang et al. reviewed 92 patients older than 60 years who underwent surgery for spinal metastases, and found that surgery could relieve pain and improve the neurologic symptoms and general conditions of the patients but also ran a high risk of complications. They did not give a definite conclusion about the risk and effect of surgery in such patients. 8 In the multicenter study reported by Amelot et al., patients were compared between 3 different age groups: <70, 70-80, and >80 years, and the authors concluded that surgeons should not be biased against operating elderly patients. 9
In view of the existing dispute regarding surgical management of MSCC in patients with advanced age, we conducted this study in an isolated cohort of patients aged 75 years or older in an attempt to answer the following questions: Can elderly patients benefit from surgery for MSCC? If so, are these patients fit for a radical surgery such as total en-bloc spondylectomy (TES)? Is there any way to reduce the risk of postoperative complications? More importantly, what are the criteria for surgical decision-making in such elderly patients?
Materials and Methods
Clinical data of eligible 55 patients in our center between January 2013 and January 2019 were reviewed retrospectively. Patient selection was restricted to fulfill the following inclusive criteria: (1) patients with MSCC; (2) patients receiving surgical treatment; (3) patients ≧75 years; and (4) patients with complete and accessible medical and surgical records. Patients ≧75 years were regarded as elderly patients in this study according to the division standard of the World Health Organization (WHO). This study was approved by the hospital ethics committee, and informed consent was obtained from all the patients or their families.
The clinical and operative records, radiographic images, and pathological reports of all patients were reviewed by 2 researchers independently. Primary tumors were divided into 2 categories: rapid growth (lung, liver, stomach, colorectum, and primary unknown) and slow or moderate growth (prostate, thyroid, breast, kidney, and uterus). Frankel Grade, and Eastern Cooperative Oncology Group performance score (ECOG-PS) were used to evaluate the neurological and performance status, respectively. Comorbidity was weighed by Charlson Comorbidity Index (CCI). Positron emission tomography-computed tomography (PET-CT) was performed to identify possible metastatic sites.
The surgical decision-making was on the guidance of NOMS framework.10,11 Generally, surgical indications were progressive neurologic deficits, spinal instability, or both. In addition, patients with solitary spinal metastasis without other bone or visceral metastases were potential candidates for TES (Figure 1). All surgical patients were evaluated to have the ability to tolerate the proposed general anesthesia and surgical intervention and a life expectancy of more than 3 months based on the extent of systemic comorbidities and tumor burden. Postoperative adjuvant treatment included chemotherapy and radiotherapy were tailored individually by the multidisciplinary team.
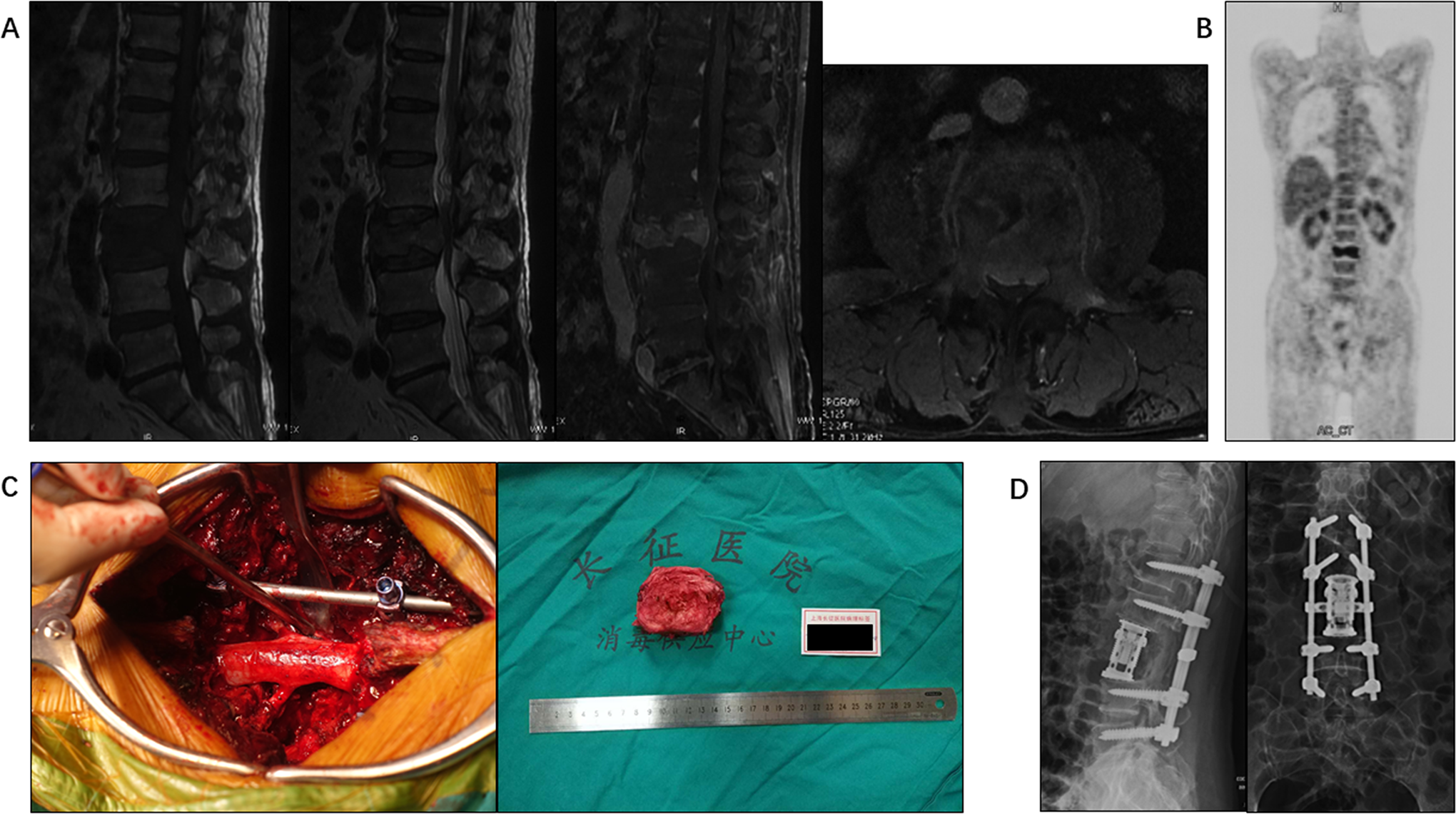
Images of a 76-year-old man with L3 metastasis from prostate cancer who received TES. A, T1-, T2- and contrast-enhanced T1 weighted MR images show the vertebral tumor extending into the spinal canal with severe dural sac compression. B, PET-CT confirms a solitary L3 metastasis. C, Intraoperative photographs show the TES performed. D, Postoperative X-ray.
Patients were followed up at 3, 6, and 12 months after surgery, every 6 months for the next 2 years, and once a year thereafter. There were 3 main outcomes measured in our study: (1) overall survival (OS) was defined as the interval between the date of the spinal surgery for MSCC in our center and the date of death or until January 2020 for surviving patients. The last status of patients was obtained from office visits or telephone interviews. (2) Patient-reported QoL was assessed by the Spine Oncology Study Group Outcomes Questionnaire (SOSGOQ), an instrument developed specifically for patients with spinal metastases. 12 The Chinese-language version of the SOSGOQ was administered before surgery and at 3-months follow-up. (3) Postoperative complications were defined as complications required pharmacologic or surgical treatment within 30 days after surgery.
All statistical calculations were performed by SPSS Statistics, version 22.0 (IBM corp., New York, USA). The Kaplan-Meier method was adopted to estimate the OS time, with log-rank test to identify the difference. Factors with P value less than 0.05 were subjected to multivariate analysis using the Cox proportional hazards model to further determine factors that independently predicted survival. Comparison of the SOSGOQ scores was conducted by Student’s t test. Chi-square test and multiple logistic regression analysis were used to clarify the risk factors for postoperative complications. All tests of significance were 2-sided. P <0.05 and P <0.1 was considered statistically significant in univariate and multivariate analyses, respectively.
Results
Patient Descriptions
The characteristics of the 55 included patients are summarized in Table 1. The series comprised 39 men and 16 women, with a mean age of 78.5 (median 78, range 75-88) years. The most frequent site of the primary cancer in our series was the lung (14), followed by the prostate (10), thyroid (8), breast (7), kidney (5), colorectum (4), primary unknown (3), stomach (2), uterus (1), and liver (1). For the treatment of the primary lesions of the 55 patients, 24 patients received surgical excision, 17 patients received radiotherapy and/or systemic medical treatment, and the remaining 14 patients were initially identified as having spinal metastasis. The most common symptom was neck or back pain (51 cases), which was exacerbated by physical activity. Motor weakness was another common symptom (43 cases), and notably 27 patients of them had lost their ambulation ability before surgery. With respect to comorbidities, diabetes was found in 14 patients, cardiovascular diseases in 4, chronic obstructive pulmonary disease in 2, and peripheral vascular disease, hepatitis, peptic ulcer disease, and connective tissue disease in one each.
Patient Characteristics, Univariate and Multivariate Analyses of the Prognostic Factors Affecting OS.
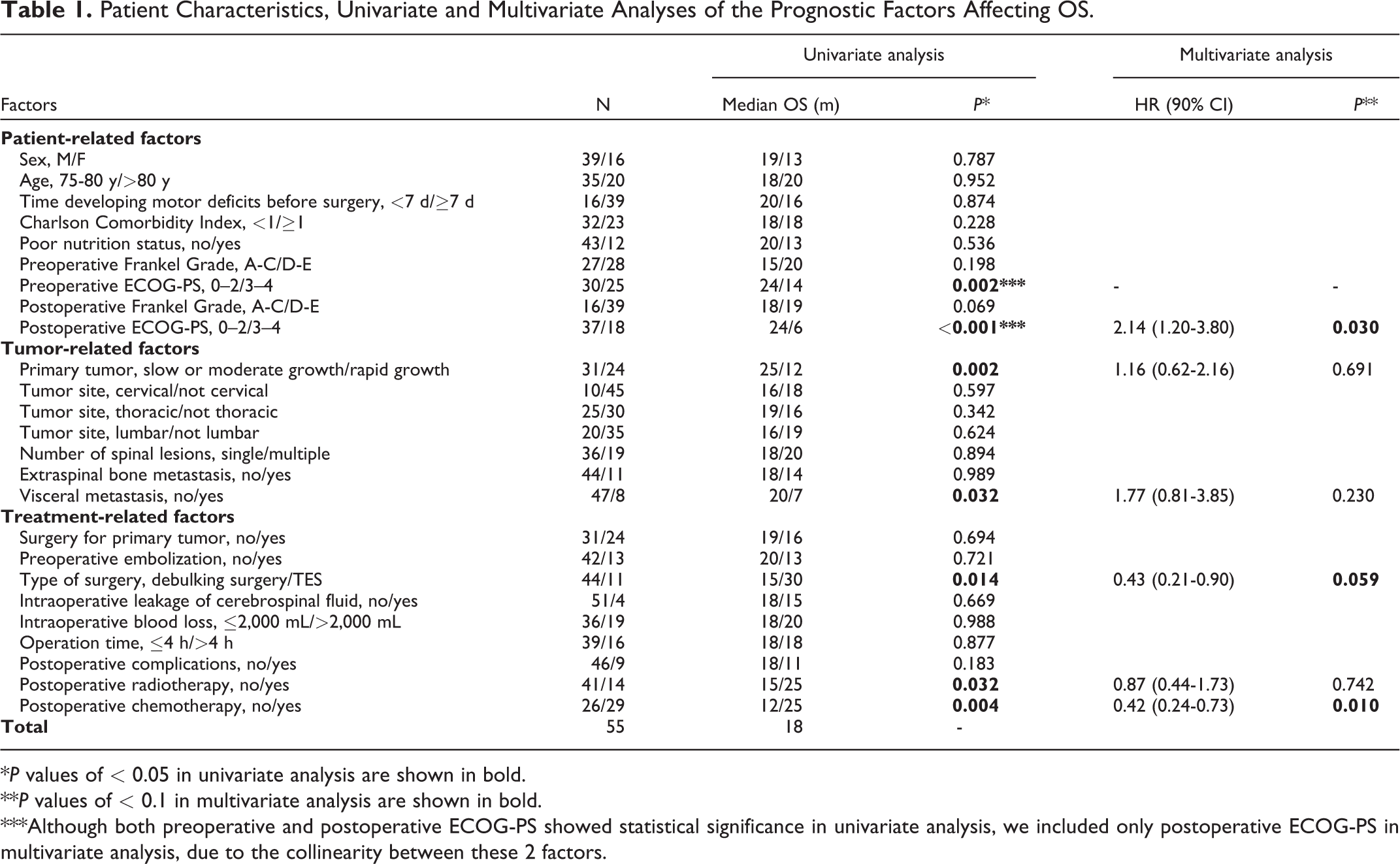
*P values of < 0.05 in univariate analysis are shown in bold.
**P values of < 0.1 in multivariate analysis are shown in bold.
***Although both preoperative and postoperative ECOG-PS showed statistical significance in univariate analysis, we included only postoperative ECOG-PS in multivariate analysis, due to the collinearity between these 2 factors.
Treatment for MSCC
All patients in our series received surgical treatment after carefully preoperative assessment and preparation. Palliative debulking surgery and TES were performed in 44 and 11 patients, respectively. The mean operation time was 209 minutes (median 195, range 80-400), and the operation time was longer than 4 hours in 16 patients. The mean intraoperative blood loss was 1387 mL (median 1200, range 200-3400), and more than 2000 mL in 19 cases. Postoperative radiotherapy and systematic chemotherapy were performed by multidisciplinary team in 14 and 29 patients, respectively.
Follow-Up and Survival
The mean follow-up duration was 21.8 (range 1-77) months for all patients. Fifty (91%) patients died with a mean period of 18.5 months (range 1-62) between the diagnosis of MSCC and death, and 5 (9%) patients are still alive with a mean survival time of 54.2 months (range 33-77). According to Kaplan-Meier curve (Figure 2A), the 1-, 2- and 3-year survival rate in all patients was 67.3%, 36.4%, and 11.7%, respectively, with the median OS time of 18 (95% CI 13.5-22.5) months.
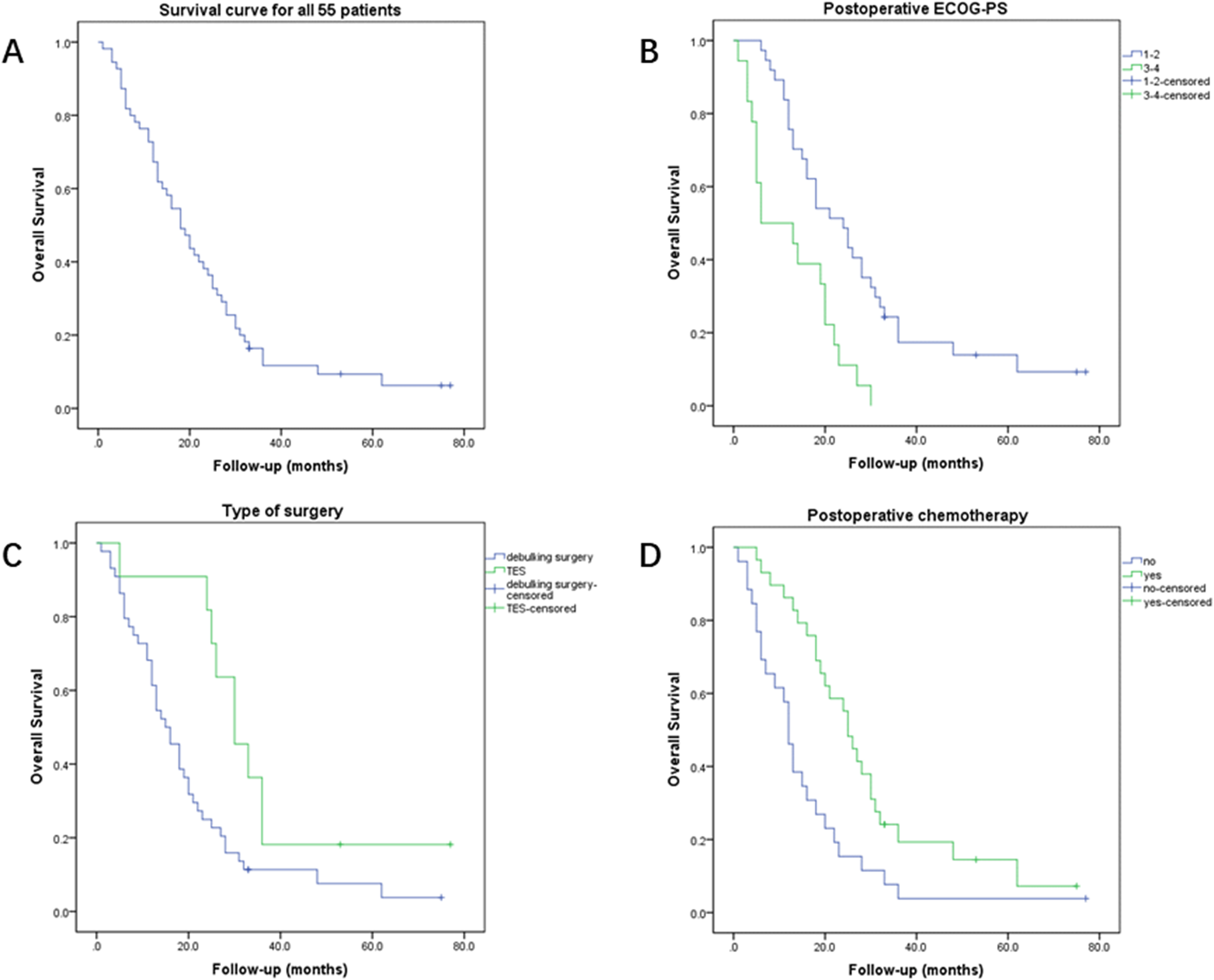
(A) Kaplan-Meier curve of overall survival (OS) for all patients. Kaplan-Meier curves of OS based on 3 independent factors for prognosis: (B) postoperative ECOG-PS, (C) type of surgery, and (D) postoperative chemotherapy.
The results of univariate and multivariate analyses of the prognostic factors affecting OS are shown in Table 1. Postoperative ECOG-PS of 3-4 was significantly associated with a higher risk of death, while the risk of death was significantly decreased in patients who received TES or postoperative chemotherapy (Figure 2B-D).
QoL Assessment
The total SOSCOQ score was increased significantly in 46 (88.5%) of the 52 patients who survived more than 3 months. The total SOSCOQ score and sub-scores in the 4 specific life domains are shown in Table 2. Postoperative improvement was observed not only in the mean total SOSCOQ score (51.4 vs. 41.6, P < 0.001) but also in the mean sub-score of the physical function domain (56.8 vs. 46.0, P = 0.023), pain domain (57.5 vs. 33.0, P < 0.001), and mental health domain (60.1 vs. 48.2, P = 0.026), but the difference in social function domain was not significant.
Quality of Life Scores Measured With SOSGOQ.
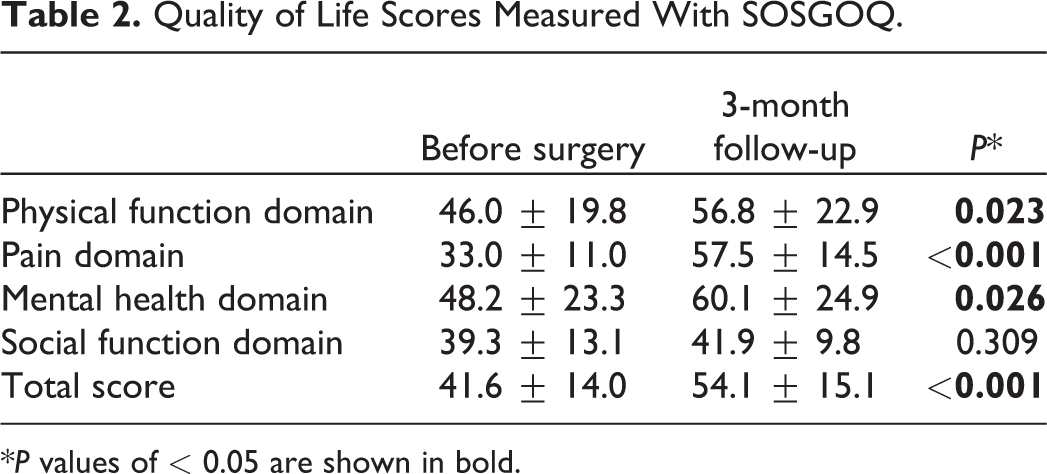
*P values of < 0.05 are shown in bold.
Postoperative Complications
Postoperative complications were observed in 9 patients (16.4%) within 30 days after surgery, including surgical site infection (4), pneumonia (2), sepsis (1), spinal epidural hematoma (1), and delirium (1). Five patients (9.1%) received a second operation, and perioperative death was observed in 1 patient (1.8%) who died of sepsis.
The results of univariate and multivariate analyses to identify risk factors for postoperative complications are shown in Table 3. The patients who developed postoperative complications had a higher CCI and a longer operation time than those without postoperative complications, and both factors (CCI ≥1 and operation time >4 h) were demonstrated to be independent risk factors for postoperative complications.
Univariate and Multivariate Analyses of the Risk Factors for Postoperative Complications.
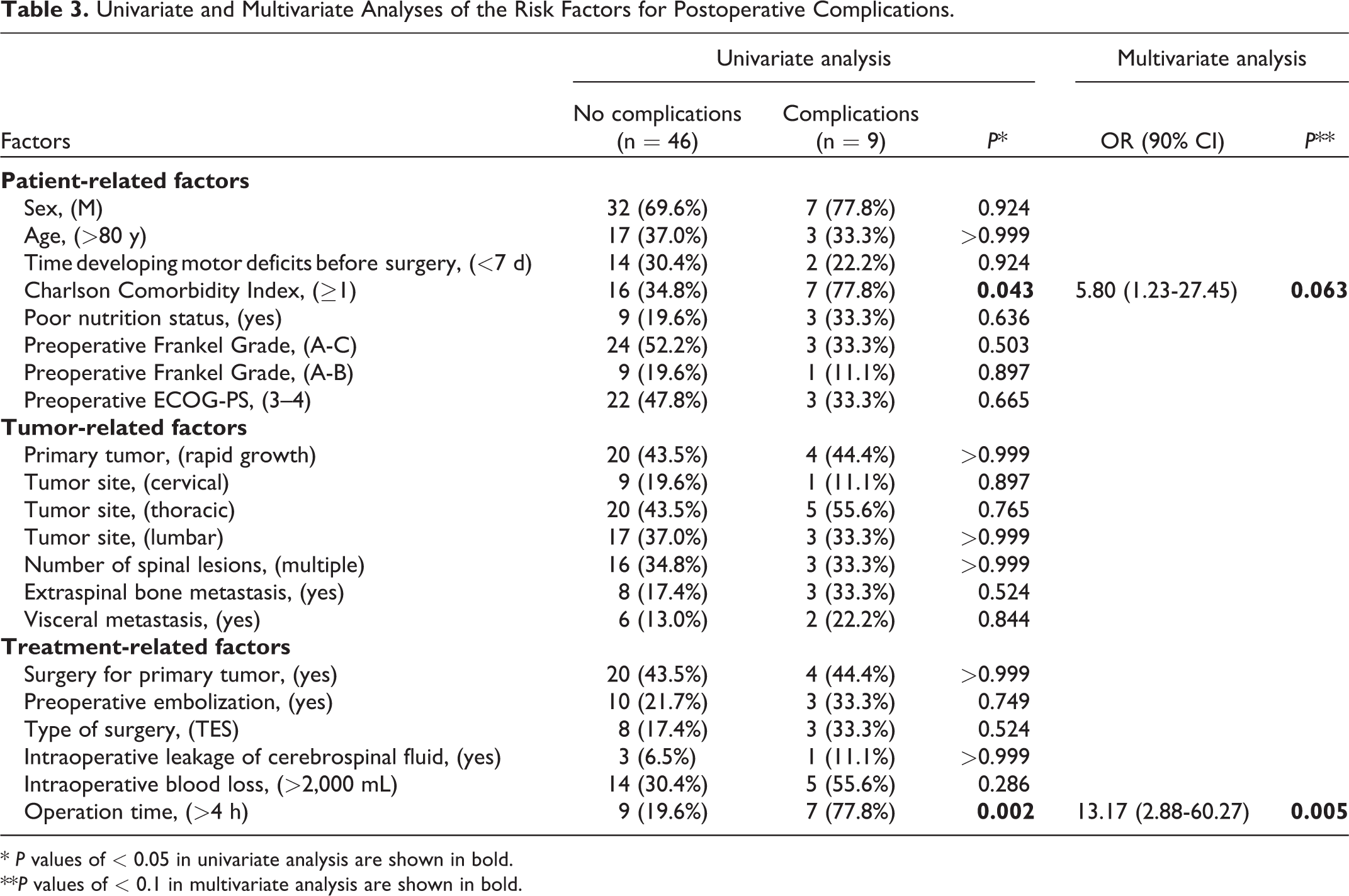
* P values of < 0.05 in univariate analysis are shown in bold.
**P values of < 0.1 in multivariate analysis are shown in bold.
Discussion
The significant benefits of decompressive surgery in the management of MSCC have been well acknowledged since a landmark trial published in 2005, 1 but due to the higher risk of surgery- and anesthesia-related complications, and shorter life expectancy, some scholars would prefer to avoid spinal surgery in elderly patients.2,7,13 In this study, we reviewed an isolated cohort of elderly patients with MSCC who received surgical treatment to discuss the 4 key questions proposed in the Introduction part.
Can Elderly Patients Benefit From Surgery for MSCC?
With the advances in surgical instrumentation and technique, a broader spectrum of surgical interventions and improved outcomes are available to patients suffering from spinal metastatic tumors with the goals to preserve the neurologic function, relieve pain and improve QoL.14,15 But whether these goals can be achieved effectively among patients aged 75 years or older still need to be confirmed. In our series, the neurological function was greatly improved in more than 50% of the 55 patients included. Remarkably, more than 40% of the paralyzed patients regained their ambulatory ability 3 months after surgery. Moreover, nearly 90% patients showed a significant improvement in the total score of SOSGOQ, which was applied to systematically evaluate the QoL of the patients from different domains: physical function, pain, mental health, and social function. Besides the increase in Frankel Grade, significant improvement in physical function was also reflected by specific items in the questionnaire, such as “the level of activity,” “the ability of care for themselves,” and “the require assistance from others to travel outside the home.” Pain relief represents the most prominent improvement in all domains according to the SOSGOQ assessment. As the most common chief complaint, unbearable pain was observed in more than 90% patients, and substantial pain relief was achieved in all of them after surgery. Meanwhile, the relief of symptoms also contributed to reduced depression and anxiety. Largely because social activity was not the primary part of life among the elders, no significant improvement in social function was recorded. Stated thus, though not in every domain, elderly patients do benefit from surgery for MSCC owing to the improvement QoL.
Are Elderly Patients Fit for a Radical Surgery Such as TES?
Although surgical treatment for metastatic spinal disease is mostly aimed at palliation, surgery may extend the survival time indirectly by improving the neurological and performance status, thus enabling patients to withstand the following systematic therapies and avoiding bedridden-related problems. 16 Notably, our study found that besides postoperative ECOG-PS and postoperative chemotherapy, the type of surgery could also influence the OS time. Classical theories of Tomita and Tokuhashi recommended a radical excision to obtain long-term local control for selected patients.17,18 But with the development of stereotactic radiotherapy, a paradigm shift in the extent of tumor resection was proposed, and the surgical goal became to simply create a margin between the tumor and spinal cord for safe delivery of postoperative radiotherapy, without resection of the vertebral body or paraspinal tumor.5,11 In addition, although Liu et al. supported performing total en bloc surgery for patients older than 65 years with solitary spinal metastasis, 19 it is more generally accepted that surgery should be simplified and minimized in elderly patients to prevent the adverse effects. 2 However, in our series, patients who received TES had a longer OS time than patients who underwent palliative debulking surgery. On the one hand, the difference in OS is mainly because of the strict criteria, in which only patients with solitary metastasis and a satisfactory general status are candidates for TES. More importantly, for elderly patients with limited life expectancy, the one-shot radical surgery, which aims at providing favorable maintenance of ambulation capacity and local control during the rest of lifetime, is more acceptable for patients and their families. The short-term recurrence and the repeated radiotherapy would increase anxiety and reduce QoL for the elders. Accordingly, we suggest that the old age should not discourage surgeons from performing TES when needed, provided that it is technically possible.
Is There Any Way to Reduce the Risk of Postoperative Complications?
Postoperative complications following surgery for spinal metastasis are considered to be more common in the elderly group.20,21 But in our series, acceptable rates of postoperative complications (16.4%), reoperation (9.1%), and 30-day mortality (1.8%) were observed, compared with the reported overall average rates for spinal metastases surgery (26.87%, 12.64%, and 6.7%, respectively). 22 Given previous studies that longer operation time was associated with perioperative complications of spine surgery in elderly patients, 23 and comorbidity was an important risk factor of complications after spinal metastasis surgery,24,25 it is not surprising that the operation time and CCI were found to be significant predictors in our series. Therefore, surgical technique and patient selection are 2 ways to reduce the risk of postoperative complications for elderly patients. For example, to control the operation time within 4 hours should be encouraged, especially for patients with comorbidity. In addition, although our results showed that TES was not found to be a significant risk factor, TES for elders should be performed by specifically dedicated teams with trained spine tumor surgeons and anesthesiologists.
What Are the Criteria for Surgical Decision-Making in the Elders?
The NOMS (neurological, oncological, mechanical and systemic) framework is one of the generally accepted criteria used for decision-making for patients with MSCC. Briefly, the presence of spinal cord compression (neurological consideration) and/or spinal instability (mechanical consideration) usually requires surgical treatment, except in the setting of a pure radiosensitive histology (oncological consideration).10,11 The above-mentioned NOM considerations are also applicable to elderly patients. Meanwhile, more attention should be paid to the systemic consideration for the elders. In order to reduce the risk of complications, spine oncology practitioners need to be cautious when facing elderly patients with comorbidity. Besides, it is vital that surgery should be performed by skilled and experienced surgeons and their teams who are capable to complete the operative process within 4 hours. Considering that ECOG-PS of 0-2 and chemotherapy are associated with a longer OS time, patients with a good performance status and systemic treatment adherence would benefit more from surgery.
In summary, based on the NOMS framework and our results, we propose that surgery should be encouraged for elderly patients with MSCC who meet the following criteria: 1. current neurological function or potential neurological compromise; 2. radioresistant tumors; 3. spinal instability; 4. no comorbidity, ECOG-PS of 0-2, and systemic treatment adherence; 5. a skilled and experienced surgical team. Moreover, in order to achieve a tumor-free margin, and thus decrease the risk of local recurrence, TES surgery in our center is mainly indicated for solitary spinal metastasis without spreading into or invading adjacent visceral organs or great vessels. 26
Limitation
Our study has several limitations. First, the retrospective nature is the main limitation. Second, our study lacked a control group. Moreover, due to the limited sample size, the reliability of our results needs to be confirmed by further researches.
Conclusions
The results of our study in an isolated cohort of patients ≧75 years of age demonstrated that surgical treatment for MSCC substantially improved QoL in a high percentage of patients with an acceptable complications rate. Therefore, surgery should not be avoided solely due to the advanced age. Meanwhile, old age should not discourage surgeons from performing TES when needed, provided that it is technically possible. We propose that surgery could and/or should be considered in elderly patients with MSCC as long as they meet the following criteria: 1) current neurological function or potential neurological compromise; 2) radioresistant tumors; 3) spinal instability; 4) no comorbidity, ECOG-PS of 0-2, and systemic treatment adherence; and 5) a skilled and experienced surgical team.
Footnotes
Authors’ Note
Xin Gao, Zheyu Wu, and Tao Wang contributed equally to this work, and all the 3 authors can be regarded as first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.