
Abstract
Study Design:
Retrospective comparative study.
Objectives:
To compare radiological and functional outcomes of patients with fixation constructs utilizing pedicle screw stabilization at the fracture level (FL group) versus patients with non-fracture level (NFL group) fixation in single level fractures of the thoracolumbar junction (T11-L1).
Methods:
53 patients of whom fracture level screw was used in 34 (FL group) were compared to 19 patients in NFL group. Radiological parameters analyzed were sagittal index, bi-segmental kyphosis (Cobb) angle and degree of vertebral height restoration. Prospectively collected patient reported functional outcomes and post-operative complications were also studied. Stepwise regression analysis adjusted by age, gender and functional scores was performed to account for the small numbers and unequal sizes of the groups.
Results:
Back pain score was significantly lower in the FL group (P < 0.025). Core Outcome Measures Index scores and leg pain scores, though low in the FL group, were not statistically significant. The regression analysis showed that the inclusion of the fracture-level screw was independently associated with a greater change in sagittal index and vertebral height restoration post-operatively. Sagittal index was maintained through to final follow up as well. The bi-segmental Cobb’s angle correction was not associated with fracture-level screw construct. There was no significant difference between the groups for revision surgery, deep infection, implant failure or length of hospital stay.
Conclusion:
The inclusion of the fracture-level pedicle screws in the fixation construct significantly improves the immediate and final measured radiological parameters, with improved functional scores in single level unstable vertebral fractures of the thoracolumbar junction.
Introduction
The thoracolumbar junction represents the transition zone between the rigid thoracic and the mobile lumbar spine. Also, the facet joint orientation changes at this region. Vertebral fractures in this area are therefore common and are subjected to greater loading stresses. 1,2 Injuries at the junctional region often lead to instability, and post-traumatic deformity is common in this area. 3 Associated neurological damage is noted in 20% of the cases. 4
Operative stabilization is usually indicated in unstable fracture pattern, resultant pain and/or deformity, associated neurological injury and in some polytrauma cases. Posterior pedicle screw stabilization is considered the gold standard means of fixation in thoracolumbar fractures and reported to be reliable, safe and efficient method with good return to function.5,6 The fixation allows for immediate stability, correction & prevention of kyphotic deformity, achieves indirect decompression of the spinal canal and permits early mobilization when compared to the non-surgical treatment. 7
Despite several constructs including short segment fixation, long segment fixation and mono-segment instrumentation (with or without bone grafting), the lack of high-quality evidence precludes the superiority of one method over the others. 8 Though short segment instrumentation has the advantages of preservation of motion segments, lesser tissue morbidity and shorter operative times, long term results show loss of correction and implant failures.9-11 To counter this failure, various methods proposed include anterior stabilization, strut grafting, transpedicular bone grafting, placement of body augmenter and cement augmentation of vertebrae. 12
Over the last decade, application of the pedicle screw in the injured vertebra has become an attractive surgical option. Biomechanical cadaveric studies and subsequent clinical studies have purported the advantages of inclusion of fracture level screws in keeping the construct short without compromising the rigidity.13-16 The studies reporting this technique and the various metanalysis have mainly focused on complications and radiological parameters as outcome measures, with none looking at patient reported functional outcomes.17-19 Moreover, the studies looked at treated fracture levels not entirely confined to the thoraco-lumbar junction. The aim of our study is to assess functional clinical outcomes, radiological results and complications of pedicle screw stabilization of single level fractures of the thoracolumbar junction. We analyzed the outcomes between constructs using fracture-level screw (FL group) versus non fracture-level screw (NFL group).
Material and Methods
From our tertiary referral spinal unit prospective database, we identified 53 patients who had posterior pedicle screw stabilization of single level traumatic fractures of the thoracolumbar junction (T11-L1) between the years 2010-2018. Electronic patient records (EPR) and radiological imaging were used to collect all the data including patient demographics, injury patterns and associated injuries (Table 1). Institutional Review Board approval was not sought, nor needed for this study due to the retrospective observational nature of the study. Fractures were graded according to AO classification and Thoraco-Lumbar Injury Classification and Severity (TLICS) scores were calculated. Neurological status was documented using the ASIA scale. Indications for surgical intervention were unstable fracture patterns (TLICS score ≥4), associated neurological deficit, failed conservative treatment or fractures associated with other system injuries to aid rehabilitation. All patients who had multiple level fractures, fractures not involving T11-L1 vertebrae, pathological fractures, incomplete radiographic data and revision fixation were excluded from the study.
Patient Demographics and Injury Details.
FL group, Fracture-level group; NFL group, Non fracture-level group; AO, Arbeitsgemeinschaft für Osteosynthesefragen; TLICS, Thoraco-Lumbar Injury Classification and Severity score.
Fracture level screw construct was used in 34 patients (FL group) compared to 19 patients who did not have pedicle screws at the fractured vertebra (NFL group) (Figure 1A-H, 2A-E). The decision to use the fracture level screw was entirely the surgeon choice. In most cases 30- or 35-mm screws were used at fracture level, unless the fracture configuration allowed a longer pedicle screw. A 5 mm rod and 6.5 mm pedicle screw construct were used in most cases. All patients, irrespective of the method of fixation, were mobilized as pain tolerated soon after the procedure. Fracture healing, implant failure, revision surgery and surgical complications were studied till final discharge. Implant failure was deemed on direct or indirect radiological signs such as screw breakage or pull-out, rod breakage or displacement, screw or rod deformation, screw head dislodgement, implant loosening; and progressive deformity.
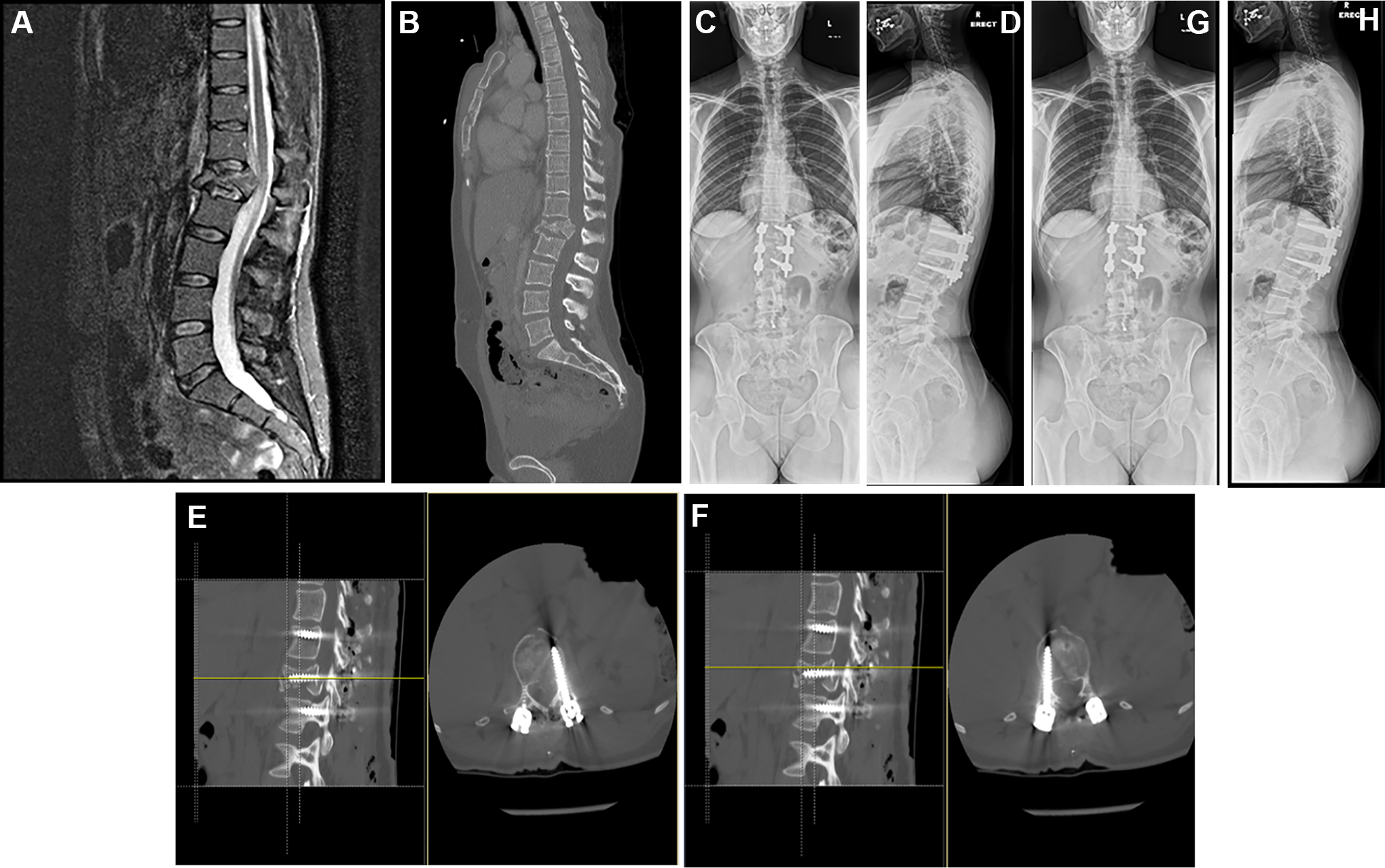
A-H, 40-year lady, with AO type A4 fracture of L1 and sternal fracture, with fracture-level pedicle screw stabilization: pre-operative imaging, post-operative CT scans and 5 month follow-up erect radiographs.
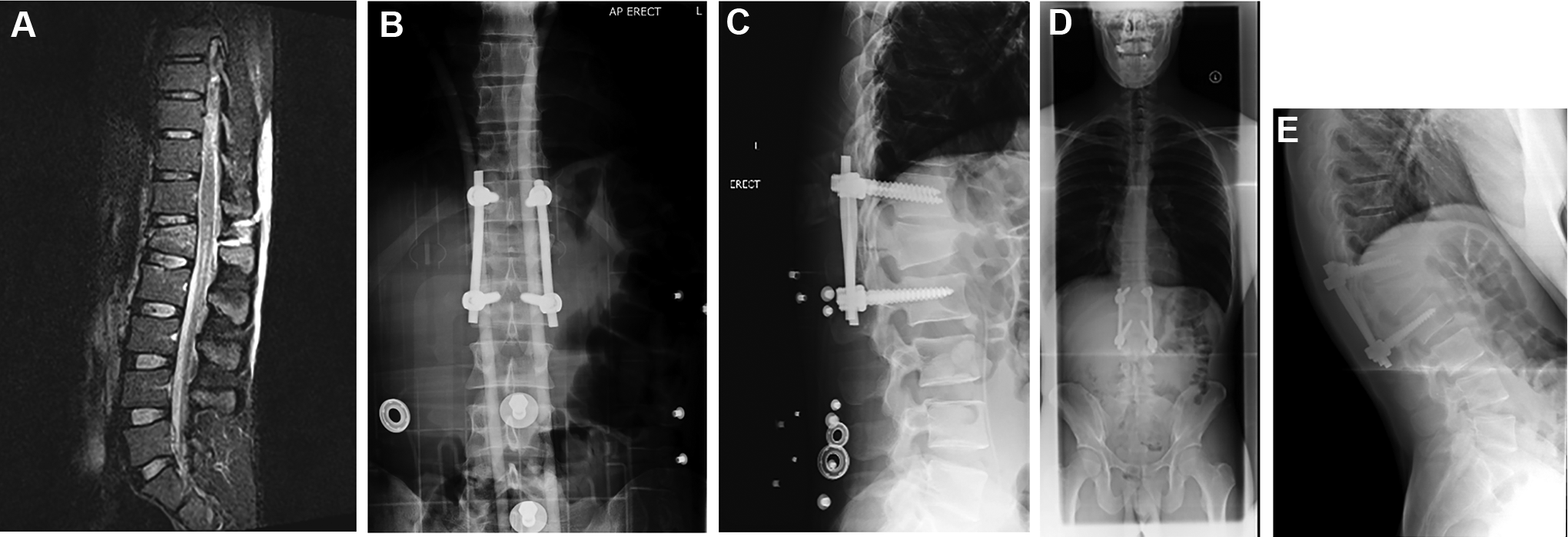
28-year male, with AO type B2 chance fracture of L1, with short segment fixation without fracture-level screws: initial (B,C) and 9 month (D,E) follow-up radiographs.
Radiological parameters analyzed were sagittal index, bi-segmental kyphosis (Cobb) angle and degree of vertebral height restoration (Figure 3) according to the description by the Spine Trauma Study Group. 20 The parameters were measured at pre-operative, immediate post-operative and final follow up periods by 2 authors (RM and ME) at different times and the average value was taken into consideration for data analysis. Any measurement that differed by >5° or 5% calculation between the researchers was re-measured and the final average was utilized for analysis. Sagittal index, first proposed by Farcy et al, 21 is a useful criterion to assess deformity and predict progression of segmental kyphosis. Sagittal index is calculated by measuring the segmental kyphosis of the fractured vertebra (angle between both endplates of the fractured vertebra) and substracting the baseline sagittal contour at that level. Baseline estimates for the intact sagittal curve are 5° in the thoracic spine, 0° in the thoracolumbar junction, and −10° in the lumbar spine. The local kyphosis was measured using Cobb angle method. Bi-segmental Cobb angle is the angle formed between a line drawn parallel to the superior endplate of the cranial vertebra above the fracture and a line drawn parallel to the inferior endplate of the caudal vertebra below the fracture. The degree of vertebral body height restoration is computed by measuring the ratio of the anterior vertebral height (AVH) to posterior vertebral height (PVH).
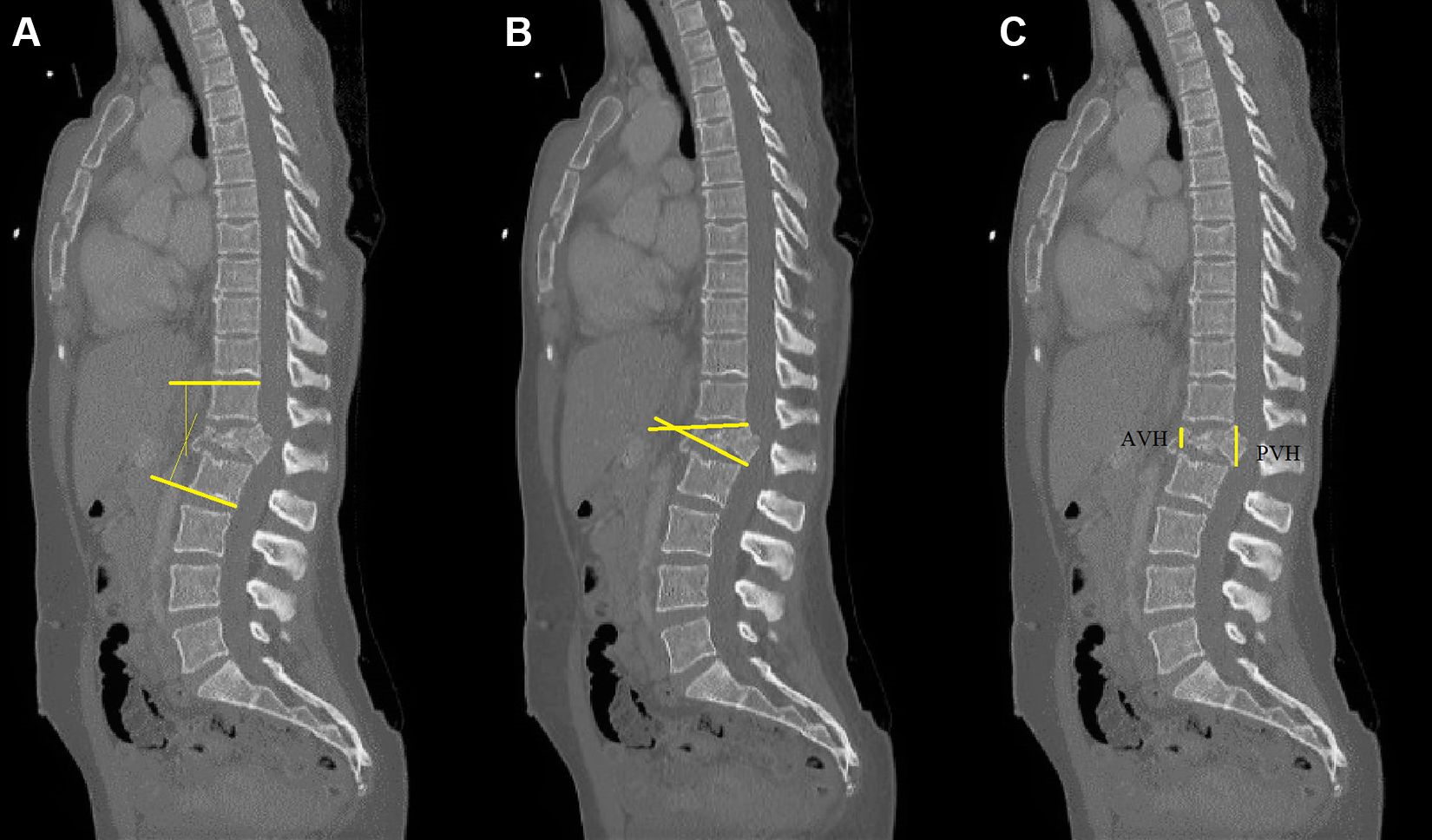
Radiological measurements: (A) Bi-segmental Cobb angle, (B) Sagittal index, (C) ratio of the anterior vertebral height (AVH) to posterior vertebral height (PVH).
All patients were registered in our hospital Spine data registry and prospective functional outcomes were collected. Core Outcome Measures Index (COMI) scores were collected prospectively to evaluate pain, function, generic health status or well-being, and disability after the intervention. 22
Statistical analysis was performed using IBM® SPSS® and Stata/IC 14.0 (StataCorp) statistics software. Student t-test, chi-squared test and Wilcoxon rank test were used to compare the data from the 2 groups as appropriate. In view of the small patient cohort and the uneven numbers in the 2 groups studied, we also performed a stepwise regression analysis adjusted by age at the time of intervention, gender, and the COMI scores. Only those variables with P value ≤0.200 were selected in the stepwise regression model. A P value ≤ 0.05 was considered statistically significant.
Results
Back pain score was found to be significantly lower in the IC group (P < 0.025) compared to NFL group. Core Outcome Measures Index (COMI) scores and leg pain scores, though low in the FL group, were not statistically significant (Table 2).
Patient Reported Outcome Scores at 3 Months.
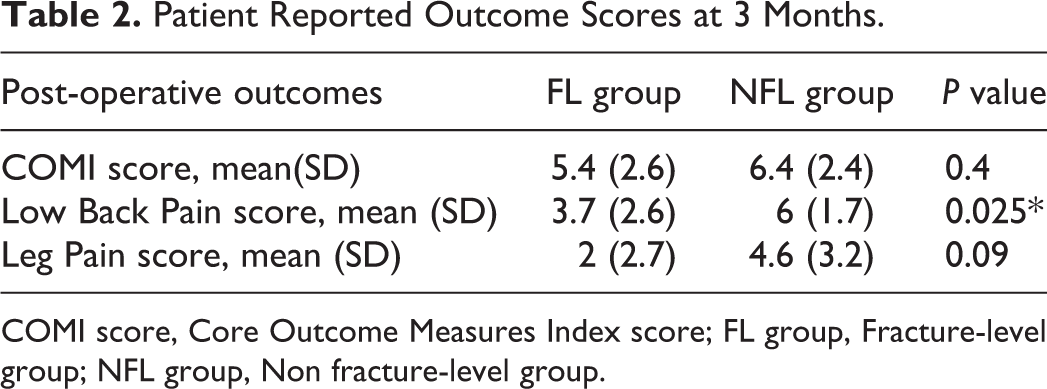
COMI score, Core Outcome Measures Index score; FL group, Fracture-level group; NFL group, Non fracture-level group.
In the regression analysis, we found that the fracture-level screw construct was independently associated with a greater change in sagittal index from the pre-operative to immediate post-operative and to the final follow-up measurement. Also noted was the significant association with a greater change in AVH/PVH ratio from pre-operative to immediate post-operative measurements (Table 3). Though the AVH/PVH ratio improved from the pre-op measurement to final follow up, this association was not statistically significant. The Cobb angle measurements did not however have an independent association with inclusion of fracture-level screw in the fixation construct.
Stepwise Regression Analysis Data Adjusted by Age, Sex and COMI Scores.
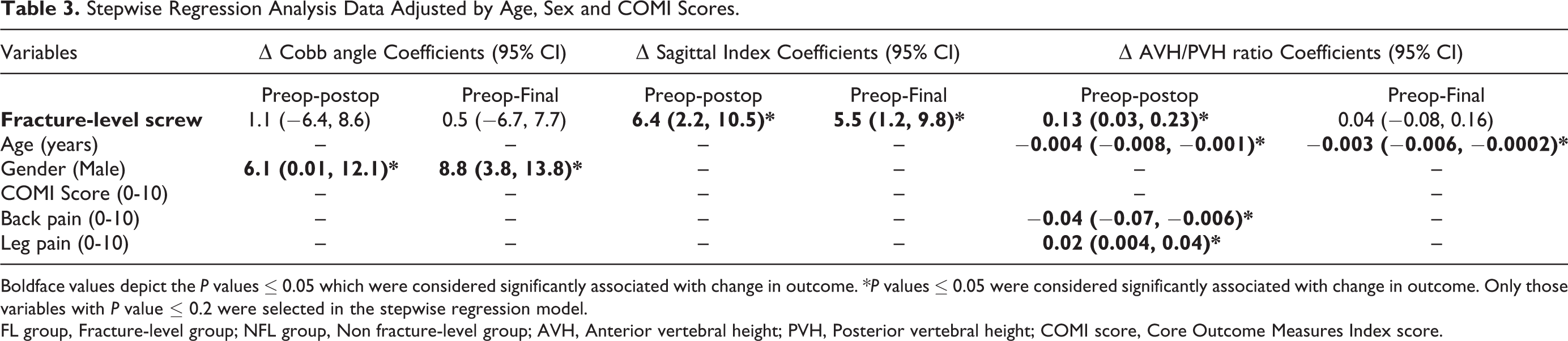
Boldface values depict the P values ≤ 0.05 which were considered significantly associated with change in outcome. *P values ≤ 0.05 were considered significantly associated with change in outcome. Only those variables with P value ≤ 0.2 were selected in the stepwise regression model.
FL group, Fracture-level group; NFL group, Non fracture-level group; AVH, Anterior vertebral height; PVH, Posterior vertebral height; COMI score, Core Outcome Measures Index score.
Loss of kyphosis correction was noted in both groups at final follow up compared to immediate post-operative values. The NFL group demonstrated a mean 5.9° and 2.4° loss of local kyphosis and sagittal index measurements compared to 3.5° and 0.3° in the FL group. Loss of vertebral height restoration showed more similar trends between the groups, at 3% and 4% in FL and NFL groups respectively.
Revision surgery was required in 6 patients, 5 for metalwork problems (FL: NFL 4:1) and one for deep infection. In the FL group, one immediate revision was to change longer sized pedicle screw to an appropriate size, and one late revision was due to loss of reduction as the locking blocker nut (innie) had come disengaged. In the NFL group 2 patients with failed fixation and one with progressive deformity did not end up being revised due to either being asymptomatic or for medical comorbidities. There was no significant difference between the groups for revision surgery, deep infection, implant failure or post-operative length of hospital stay (Figure 2).
Discussion
The thoraco-lumbar junction undergoes the greatest stress levels in the spine, which accounts for high incidence of fractures here when compared to other areas of the thoracic or lumbar spine.1,23 Injury pattern demonstrates compressive fractures usually, but distraction injuries and translation injuries can also occur. 24 Posterior stabilization concept has evolved over these past few decades from long constructs, to short segment fixations and in the last decade or so to include fracture level screws. The additional fixation points afforded by the index level screws allows for load sharing within the construct, thereby acting to achieve stability, maintain correction and at the same time keep the fixation segments short.
Meta-analysis of studies analyzing the efficacy of the intermediate screw in fixation constructs suggest better correction of deformity, lesser loss of correction and lower implant failure rate, with resultant longer operative times and higher blood loss.17-19
Mahar et al have suggested that by indirectly supporting the anterior column, the supplemental screw may have a protective effect on the fractured vertebral body. 13 They postulate that the fixation provided by the pedicle screw allows for 3-point reduction maneuver, analogous to the method employed in long bone fractures. Our study showed that the anterior vertebral height (AVH) and thereby the AVH/PVH ratio was better restored using the FL pedicle screw.
Results from our series suggest that use of fracture level screw corrected the sagittal index post-operatively better than without the use of the screw. Guven et al 15 report that the pedicle screw at fracture construct achieves and maintains better correction of deformity through vertebral endplate augmentation with its buttress effect (bending force). In addition to anterior column support, the screw may also provide a mass effect at the fractured vertebra and prevent the vertebra from collapsing.
Most of the published evidence have looked at unstable compression fractures of thoracolumbar spine. Our series of thoracolumbar junction (T11-L1) fractures did not include any rotational or translational fracture patterns. In a biomechanical study of thoracolumbar burst fractures, Bolesta et al suggested that even with the addition of intermediate screw, the construct aided the stability of the segments beyond that of the intact state in flexion-extension and lateral bending loading, but not in axial rotation. 25 However in a clinical outcome study, Farrokhi et al have used this technique in T12-L2 level fractures and found that the higher degree of deformity correction most notably in Magerl type C (rotational/translational) fractures and propose that fracture level pedicle screw construct be particularly recommended for this unstable pattern.16
Loss of kyphosis correction has been shown in both groups in our study, with more losses noted in NFL group. This is in keeping with the trends reported in literature,17-19 depicting that show loss of correction in final follow-up is inevitable compared to the initial post-operative levels. The fracture configuration inevitably contributes to explaining the loss of correction, but other clinical features may also play a part. Formica el al have analyzed these factors and suggested that loss of kyphosis correction occurred significantly in obese patients (BMI > 30) with the other variables tested like gender, smoking habit, and preoperative neurological status not showing statistically significant correlation. 26
Implant failures have been reported in various studies with the intermediate screw fixation as well, though less than the bridging fixation method. Li et al in their metanalysis reported a failure rate in combined screw fixation vs conventional fixation of 1.5% vs 11.7% (P = 0.007). They propose that the intermediate screw application in the fixation construct can significantly improve the stress distribution of screws, reduce the screw load, and provide a fulcrum for the fracture reduction. In our series both groups had equal number of implant failures. The relatively small numbers in our study are not enough to draw any meaningful conclusion regarding this outcome.
Recent work has looked at the application of the intermediate screw technique even in severely unstable burst fractures. Kanna et al report on unstable thoracolumbar injuries with a load sharing classification score ≥7. 27 Their study suggests that with the use of short-segment pedicle screw fixation including the fractured vertebra, reduction of fracture can be achieved and maintained even at 2 years follow-up, avoiding the need for anterior reconstruction. In our long term follow up study, no cases needed anterior reconstruction nor revision due to loss of correction nor progressive deformity. Future large number prospective randomized trials might be able to shed more conclusive evidence for the benefits of intermediate screw fixation technique for all fracture patterns.
Our study has some limitations in being retrospective and small numbers but addresses a homogenous group of single level thoracolumbar junction fractures only. This report is the subset of data we are currently collecting for all our thoracic and lumbar spinal fractures treated surgically and pertains only to the thoraco-lumbar junction (TLJ) injuries (T11-L1 level). The focus on the TLJ was because of the exceeding biomechanical demands on the spine at this level and not to group these injuries with the rest of the thoracic/lumbar spine fractures. The cohort of TLJ spinal injuries is common due to significant biomechanical stresses, and we feel that addressing the question of a better fixation construct would help surgeons in the decision-making process. To our knowledge, this is the first study in the literature to report on the patient reported functional and clinical outcome in single level vertebral fractures of the thoracolumbar junction with short construct instrumenting the fractured vertebra. Our study shows that addition of the fracture-level screw improved radiological and functional outcomes in this group of patients, and it is our current practice to use the intermediate screws in all situations possible.
Conclusion
The inclusion of the intercalary pedicle screw in the fixation construct seems to significantly improve immediate and final measured radiological parameters, with improved functional scores in single level unstable vertebral fractures of the thoracolumbar junction. Our current practice has evolved to aim for intercalary screw placement in all possible situations to improve the construct stability, while limiting the fixation segments.
Footnotes
Authors’ Note
Institution work was carried out at Department of Complex Spinal Surgery, Salford Royal Hospital, Manchester, M6 8HD, United Kingdom. RM: data curation, literature search, formal analysis, writing—original draft. RC: statistics, manuscript review. RV, IS, ME, SM: supervision, writing—review & editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.