
Abstract
Study Design:
A sex- and age-matched case-control study and a cross-sectional study.
Objective:
In our previous study, patients with early-onset (<50 years of age) ossification of the posterior longitudinal ligament (OPLL) had distinct features such as morbid obesity, a high prevalence of lifestyle-related diseases, and diffuse ossified lesions mainly affecting the thoracic spine. Our goals were to determine whether early-onset OPLL patients have unbalanced dietary habits and to identify nutritional factors associated with OPLL exacerbation.
Methods:
In Study 1, the simple brief-type self-administered diet history questionnaire (BDHQ) was used to compare nutrient intake levels of early-onset OPLL patients (n = 13) with those of sex- and age-matched non-OPLL controls (n = 39) or with those of common OPLL (onset age ≥ 50 years, n = 62). In Study 2, serological validation was conducted for thoracic OPLL patients (n = 77) and non-OPLL controls (n = 101) in a nationwide multicenter study in Japan.
Results:
The BDHQ showed that the early-onset OPLL patients had significantly lower intakes of vitamins A and B6 than non-OPLL controls. These results were validated by lower serum vitamins A and B6 levels in the early-onset thoracic OPLL patients. The severity of OPLL negatively correlated with serum vitamin A levels in male early-onset OPLL patients. The multiple regression analysis revealed that the severity of thoracic OPLL had an association with onset age and serum vitamin A level.
Conclusions:
Vitamin A deficiency resulting from unbalanced dietary habits is associated with exacerbation of male early-onset OPLL.
Introduction
Heterotopic ossification of the posterior longitudinal ligament of the spine (OPLL) is a common skeletal disorder in East Asian countries. OPLL patients develop various degrees of myelopathy as well as ankylosis of the spine, but effective drug therapy has not been established. Epidemiological and familial studies have suggested that OPLL is a multifactorial disease in which complex genetic (polygenic) and non-genetic (environmental) factors interact1-3; however, its etiology remains unclear.
OPLL commonly develops in the cervical spine when patients are in their 50 s and 60s,2,3 but it occurs rarely at 50 years of age or younger. Our previous study found that patients with early-onset OPLL (<50 years of age) had distinct features such as more severe obesity (body mass index [BMI] > 35 kg/m2) as well as diffuse heterotopic ossification of the spinal ligaments mainly affecting the thoracic spine, compared to patients with common OPLL (onset at ≥ 50 years of age). 4 Given that a higher prevalence of micronutrient deficiencies in obese individuals is associated with an increased risk of chronic diseases, 5 it could be assumed that unbalanced dietary habits or nutritional conditions are associated with the development or exacerbation of OPLL especially in obese patients with early-onset OPLL.
Dietary habits have been thought to be a causative or aggravating factor for OPLL. Racial differences in the incidence of OPLL and higher prevalence of life-related diseases such as diabetes and obesity in OPLL patients support this idea. Some studies reported that OPLL patients prefer plant protein to animal protein in comparison with non-OPLL controls, 6 but there is no conclusive proof of this observation. Dietary factors associated with the development or progression of OPLL should be investigated by well-designed studies. The aims of this study were to determine whether early-onset OPLL patients had unbalanced dietary habits and to identify nutritional factors associated with the exacerbation of OPLL. This study addresses the need for dietary care in patients with OPLL and helps identify a therapeutic target to prevent progression of OPLL.
Materials and Methods
Study Design
The present study was composed of a sex- and age-matched case-control study and a cross-sectional study. All patients were enrolled between June 2017 and September 2019. The investigation consisted of 2 nutritional surveillance studies: a self-administered diet history questionnaire
Study 1: Self-Administered Diet History Questionnaire
Patients and controls
A total of 131 Japanese patients with OPLL who regularly visited the Hokkaido University Hospital and affiliated hospitals were recruited. All patients were diagnosed with OPLL by either neurosurgeons or orthopedic spine surgeons, according to radiologic examinations and clinical symptoms. Patients with congenital skeletal disorders, pregnancy, and autoimmune diseases were excluded. Patients with gastrointestinal disorders, including inflammatory bowel diseases and those with cancer and severe paralysis who had difficulty eating food were also excluded. The analysis excluded data from patients older than 80 years, those who were taking any dietary supplement, and those who had declared significant changes in their dietary habits during their lives or after OPLL diagnosis or surgery. The final decision concerning the inclusion or exclusion of cases and controls was made by 2 board-certified spine surgeons (TE, MT).
After 56 patients had been excluded, the data of 75 eligible OPLL patients were analyzed. Eligible patients were divided into 2 groups, according to the age at symptom onset: the early-onset OPLL group (age < 50 years) (n = 13) and the common OPLL group (age ≥ 50 years) (n = 62). In total, 39 non-OPLL controls were matched for sex and age (± 3 years) to the early-onset OPLL group. The controls were randomly selected from patients who regularly visited or were admitted to our institutions and had no ossification of the spinal ligaments in the historical database of our institutions.
Demographics, comorbidities, and OPLL severity
Current BMI, comorbidities, and smoking habits were assessed. OPLL distribution (i.e., cervical and/or thoracic and/or lumbar spine), the presence or absence of coexisting ossification of the ligamentum flavum (OLF), age at symptom onset, treatment type (i.e., conservative or surgical), and family history of OPLL were recorded from OPLL patients.
Diet History Questionnaire
Dietary habits and nutrient intake levels were assessed using the simple brief-type self-administered diet history questionnaire (BDHQ).7-11 The BDHQ comprises 58 questions regarding food, beverage, and seasoning consumption during the preceding month, which enables the estimation of total energy intake and micronutrient intake. The items in the BDHQ were selected to represent products commonly consumed by Japanese people.
Study 2: Serological Validation of the Nutritional Questionnaire and Correlation Analysis and Multiple Regression Analysis Between Nutritional Factors and OPLL Severity
Patients and controls
Due to the rarity of the disease, it was expected that a single-center would not be able to recruit a sufficient number of early-onset OPLL patients; hence, we conducted a serological validation in a nationwide multicenter study in Japan. Because all early-onset OPLL patients had OPLL in the thoracic spine in Study 1, a total of 306 thoracic OPLL (T-OPLL) patients were recruited for Study 2. Since there is a possibility that dietary habits and nutritional conditions have changed in patients who have had OPLL for a long time, 77 eligible T-OPLL patients within 3 years of onset (32 men, 45 women) were included in the survey. That is, in Study 2, the difference between the age at symptom onset and the current age was within 3 years. In total, 101 non-OPLL controls were recruited. The inclusion and exclusion criteria for cases and controls were the same as those in Study 1.
Determination of serum vitamin A and vitamin B6 levels
Levels of serum vitamin A (retinol) (µg/dL) and vitamin B6 (pyridoxal-5-phosphate) (ng/mL) were measured using high-performance liquid chromatography (HPLC) at SRL Inc. (Tokyo, Japan). The preferred serum level of vitamin A for adults is 32.5 to 78.0 µg/dL. Asymptomatic deficiency is possible with 10.0 to 20.0 µg/dL. Severe deficiency is indicated at levels less than 10.0 µg/dL.12-15 Adults with proper nutrition have serum vitamin B6 levels of 5 to 50 ng/mL.12,16-18
Semi-quantitative evaluation of OPLL severity
To examine the association between serum vitamin levels and the ossification severity, the distribution of spinal ligamentous ossification, including OPLL, OLF, ossification of the anterior longitudinal ligament (OALL), and ossification of the supra/interspinous ligament (OSIL), was evaluated using whole-spine computed tomography (CT). To determine the severity of spinal ossification, the OPLL-, OLF-, OALL-, and OSIL-indices (defined as the sum of ossification prevalence at each vertebral body and intervertebral disc level) were calculated, according to a previously described method 19 with a slight modification. Massive, ossified regions (thickness ≥ 5 mm) were scored twice at each level. The analysis was performed independently by 3 board-certified spine surgeons (TE, MT, YH).
Statistical Analysis
Statistical analysis was performed using Bell Curve for Excel software version 3.10 (Social Survey Research Information Co., Ltd., Tokyo, Japan). Data are presented as the mean ± standard deviation (SD). P-values < 0.05 were considered statistically significant. The distribution of values was identified as not normal except for serum vitamin A. Differences in serum vitamin A levels between groups were analyzed using Student’s t-test. The Mann-Whitney test and Fisher’s exact test were used to compare the groups for the other values. Pearson’s correlation coefficient was used for the correlation analysis of serum vitamin levels and variables including ossification severity. The association of factors affecting the severity of thoracic OPLL was performed by multiple regression analysis.
Results
Study 1: Nutritional Surveillance by BDHQ
Baseline characteristics of the OPLL patients
Clinical characteristics of the 3 groups are shown in Table 1. The common OPLL group had an inconsistent disease background (i.e. current age, major areas of heterotopic spinal ligament ossification, and the severity of myelopathy); the majority of patients in this group comprised the elderly population. As it was difficult to imagine that the dietary habits of the elderly were similar to those of the young, we considered that comparing eating habits between the groups would be inappropriate due to the age bias. The data of the common OPLL group were analyzed as reference values. The prevalence of OPLL in the thoracic and lumbar spine in the early-onset OPLL group (100% and 38.5%, respectively) was higher than in the common OPLL group (35.7% and 12.5%, respectively). Current BMI in the early-onset OPLL group was significantly higher than that in the common OPLL and non-OPLL groups.
Clinical Characteristics of the OPLL Groups.
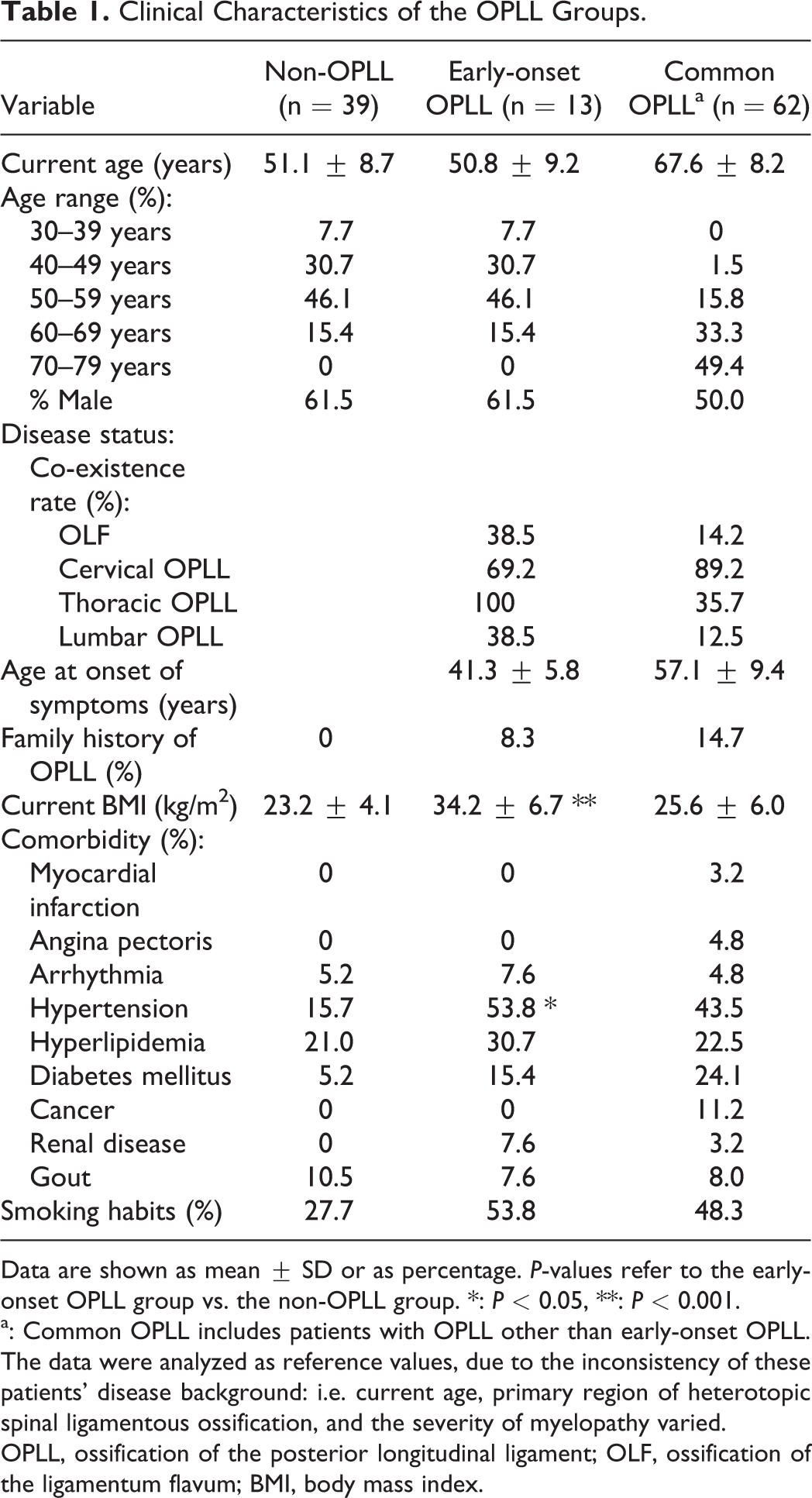
Data are shown as mean ± SD or as percentage. P-values refer to the early-onset OPLL group vs. the non-OPLL group. *: P < 0.05, **: P < 0.001.
a: Common OPLL includes patients with OPLL other than early-onset OPLL. The data were analyzed as reference values, due to the inconsistency of these patients’ disease background: i.e. current age, primary region of heterotopic spinal ligamentous ossification, and the severity of myelopathy varied.
OPLL, ossification of the posterior longitudinal ligament; OLF, ossification of the ligamentum flavum; BMI, body mass index.
Daily energy and micronutrient intakes estimated from the BDHQ
Comparative BDHQ-derived data concerning nutritional intake levels and food preferences are shown in Table 2 and Table 3, respectively. Despite a higher prevalence of severe obesity in the early-onset OPLL group, total energy intake was not significantly different among the 3 groups. Among 99 kinds of micronutrients, the intake levels of potassium, calcium, retinol, β-carotene, β-carotene equivalents, vitamin A (retinol equivalents), vitamin B6, and alcohol were significantly lower in the early-onset OPLL group than in the non-OPLL group.
Daily Energy and Micronutrient Intakes of the OPLL Groups.
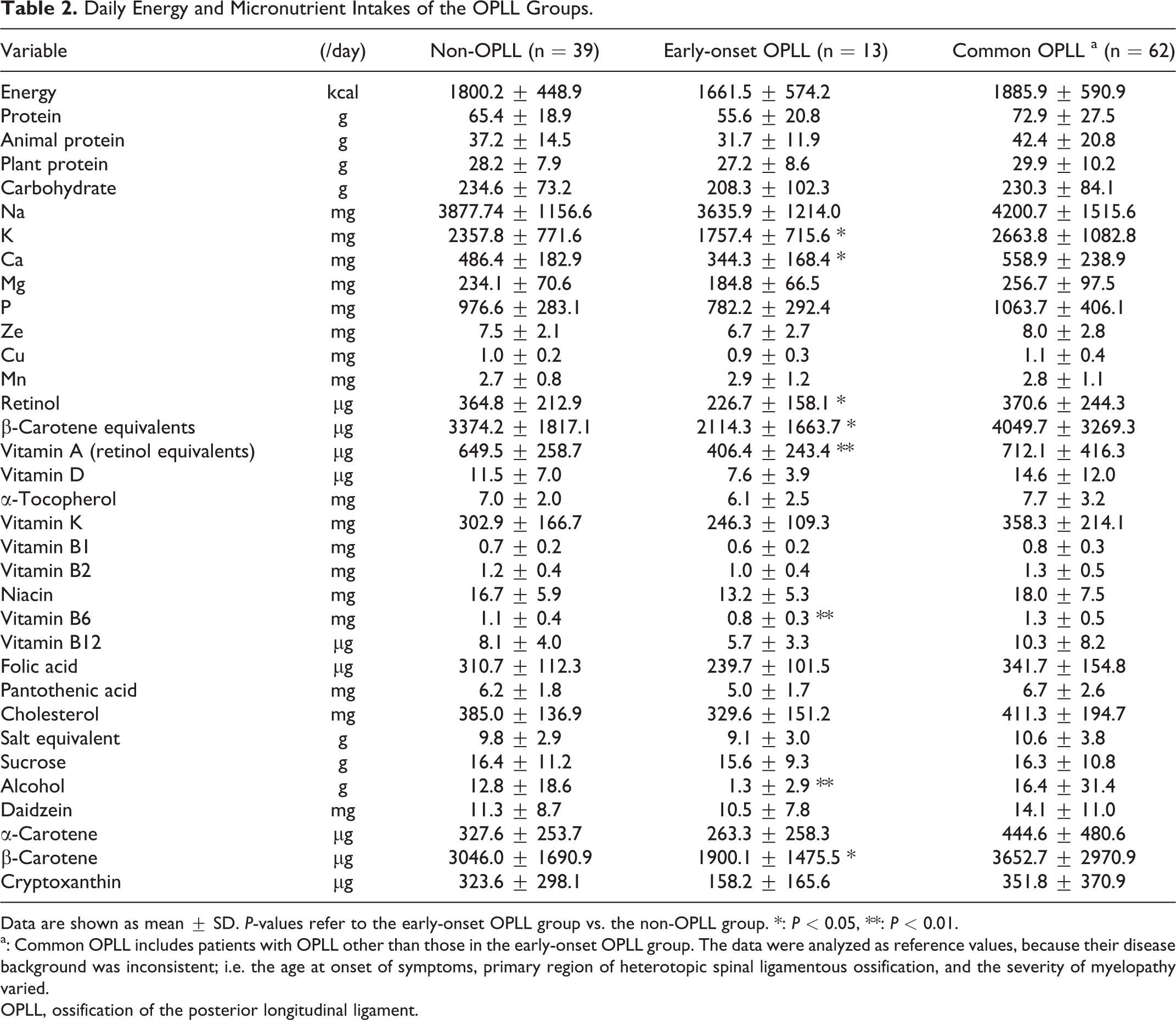
Data are shown as mean ± SD. P-values refer to the early-onset OPLL group vs. the non-OPLL group. *: P < 0.05, **: P < 0.01.
a: Common OPLL includes patients with OPLL other than those in the early-onset OPLL group. The data were analyzed as reference values, because their disease background was inconsistent; i.e. the age at onset of symptoms, primary region of heterotopic spinal ligamentous ossification, and the severity of myelopathy varied.
OPLL, ossification of the posterior longitudinal ligament.
Daily Food Intakes of the OPLL Groups.
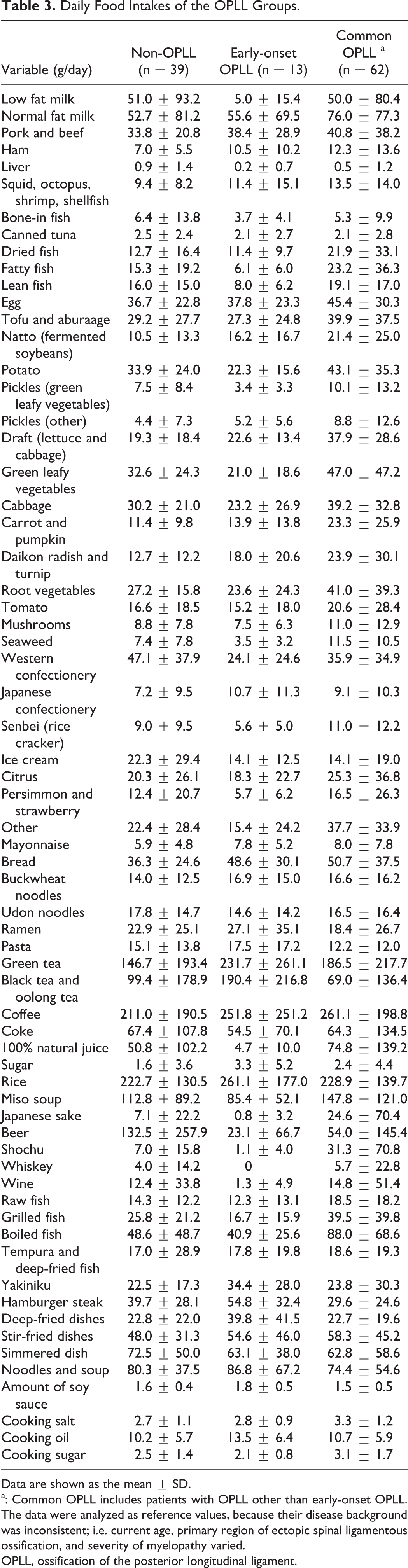
Data are shown as the mean ± SD.
a: Common OPLL includes patients with OPLL other than early-onset OPLL. The data were analyzed as reference values, because their disease background was inconsistent; i.e. current age, primary region of ectopic spinal ligamentous ossification, and severity of myelopathy varied.
OPLL, ossification of the posterior longitudinal ligament.
Study 2-1: Serological Validation
Baseline characteristics and disease status of the participants
Homeostasis of serum potassium and calcium is strictly maintained by the kidney, skeletal muscle and bone, etc. while electrolyte metabolism is strongly affected by factors other than diet. Conversely, intake of vitamins A and B6 is directly affected by diet, as vitamins are not synthesized in vivo. We speculated that a lack of intake or a reduced storage of these vitamins in the body is likely to positively affect heterotopic bone formation. We conducted a serological validation in a nationwide multicenter study in Japan.
Clinical characteristics of the T-OPLL and non-OPLL groups are shown in Table 4. The mean current age of the T-OPLL groups was 52.2 ± 12.9 years for men and 55.6 ± 10.7 years for women. The proportion of early-onset patients aged 50 years or younger was 46.8% (n = 15) in men and 26.6% (n = 12) in women. T-OPLL patients have a higher current BMI than that in non-OPLL controls. Current BMI in the non-OPLL group was comparable to the average BMI of the general Japanese population (men, 23.7 kg/m2; women, 22.4 kg/m2). 20 The prevalence of hypertension and diabetes mellitus in the T-OPLL group was significantly higher than that in the non-OPLL group regardless of sex, whereas the prevalence of hyperlipidemia was significantly higher in the female T-OPLL group than in the non-OPLL group.
Clinical Characteristics of Patients With the Thoracic OPLL in a Nationwide Multicenter Study in Japan.
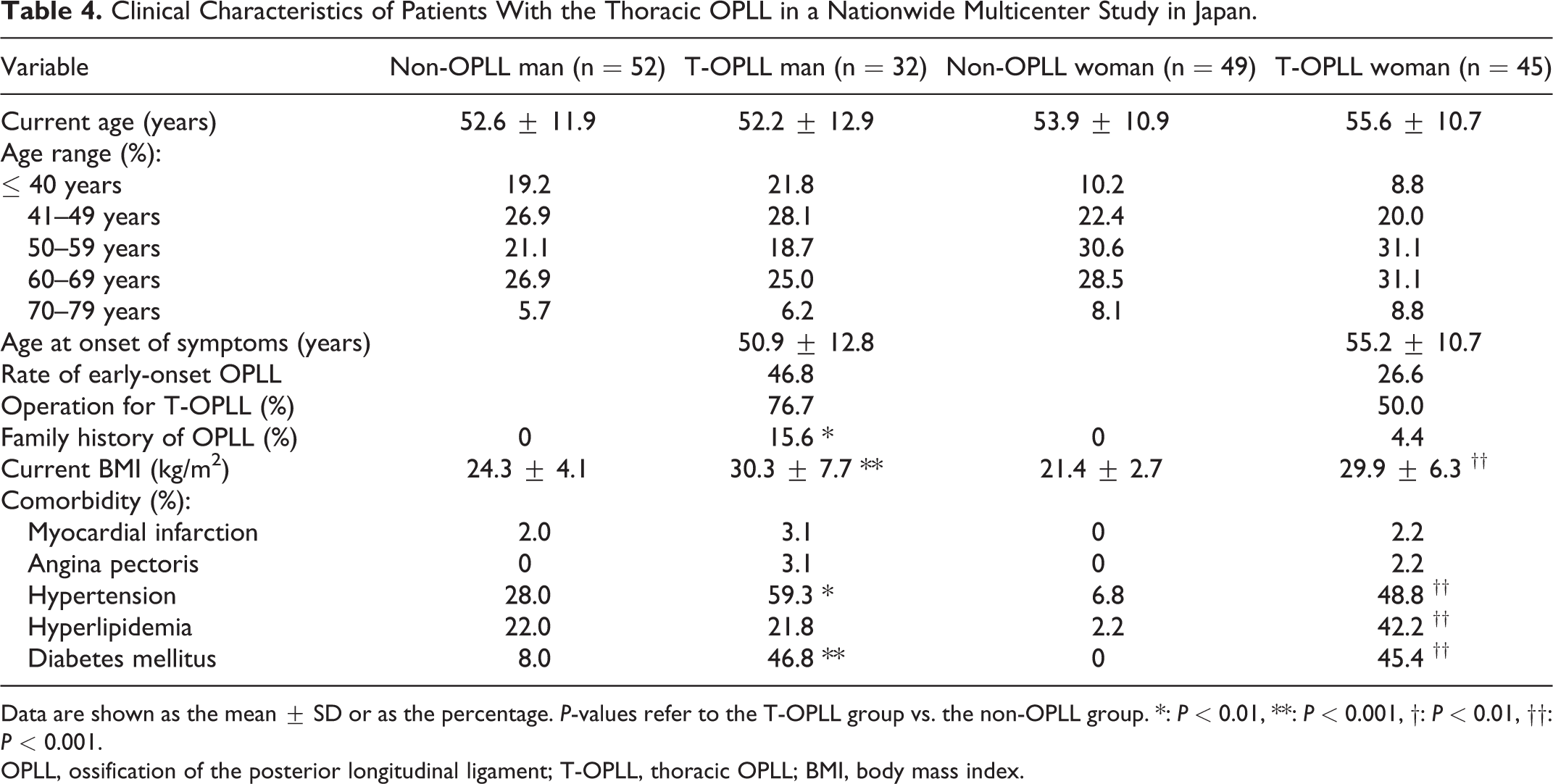
Data are shown as the mean ± SD or as the percentage. P-values refer to the T-OPLL group vs. the non-OPLL group. *: P < 0.01, **: P < 0.001, †: P < 0.01, ††: P < 0.001.
OPLL, ossification of the posterior longitudinal ligament; T-OPLL, thoracic OPLL; BMI, body mass index.
Comparison of the serum vitamin a and vitamin b6 levels in the T-OPLL and non-OPLL groups
We compared serum levels of vitamin A and vitamin B6 between the T-OPLL and non-OPLL groups by age at the time of investigation (< 50 years vs. ≥ 50 years). The serum vitamin A and vitamin B6 levels were significantly lower in the T-OPLL group than in the non-OPLL group, regardless of sex and age, except for serum vitamin A levels in women over 50 years old (Figure 1). The serum vitamin A and vitamin B6 levels in the man T-OPLL patients showed a negative correlation with current BMI (Table 5). By contrast, serum vitamin A and vitamin B6 levels in the non-OPLL group did not correlate with BMI, regardless of sex (Table 5).
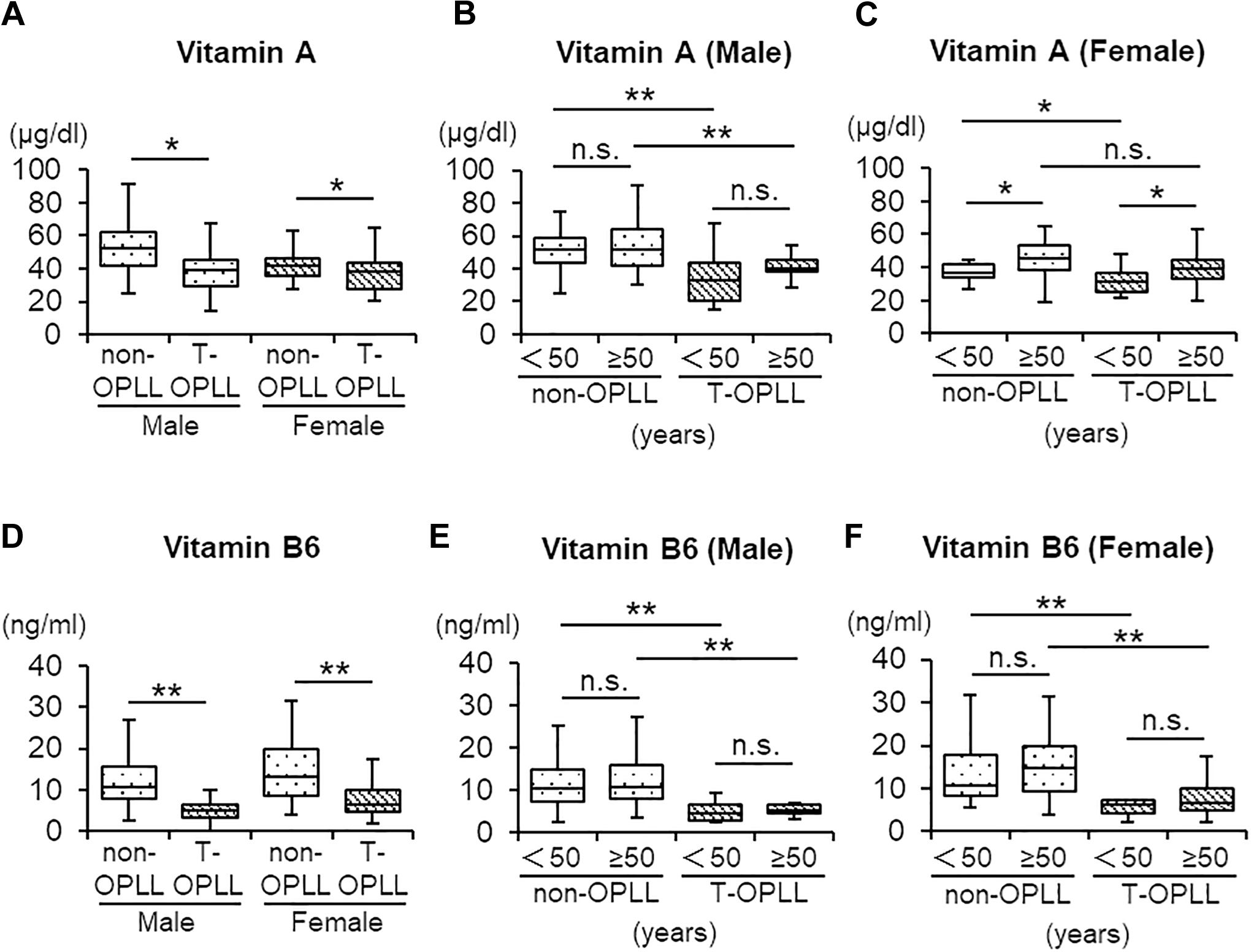
Association of the serum vitamin levels and OPLL between the thoracic OPLL and non-OPLL groups. A and D, Vitamin A (retinol) and vitamin B6 (pyridoxal-5-phosphate). B and C, Vitamin A categorized by < 50 years and ≥ 50 years of age (current age). E and F, Vitamin B6 categorized by < 50 years and ≥ 50 years of age. *: P < 0.05, **: P < 0.01, n.s.: not significant OPLL: ossification of the posterior longitudinal ligament; T-OPLL: thoracic OPLL.
Correlation Coefficients for the Serum Levels of Vitamin A (retinol) and Vitamin B6 (Pyridoxal-5-Phosphate) in the Non-OPLL and Thoracic OPLL Groups.
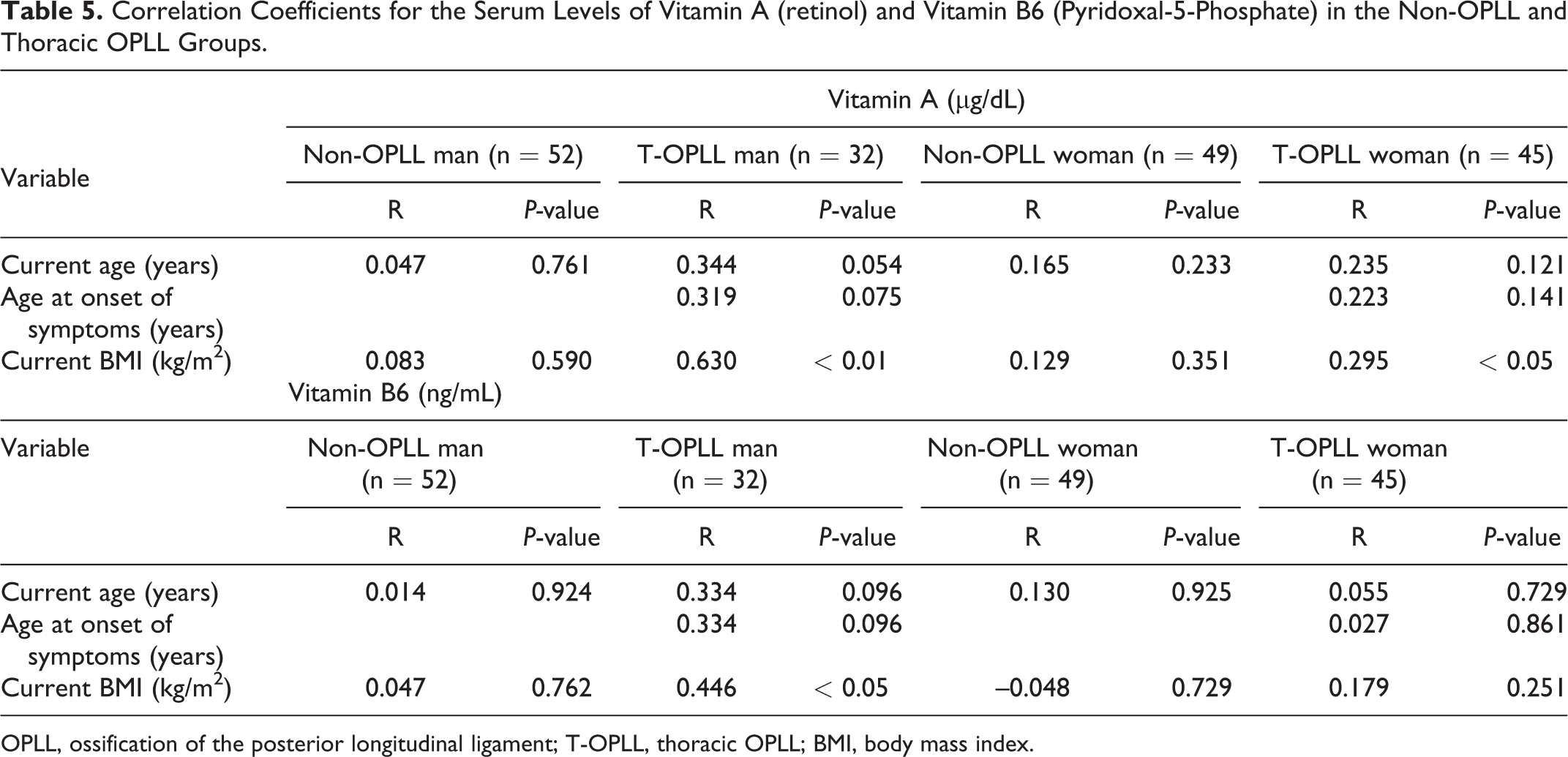
OPLL, ossification of the posterior longitudinal ligament; T-OPLL, thoracic OPLL; BMI, body mass index.
Study 2-2: The Severity of the Heterotopic Ossification of the Spinal Ligaments and its Correlation With Serum Vitamin A and Vitamin B6 Levels
We then analyzed the correlations between serum vitamin A and vitamin B6 levels and the severity of the spinal ligamentous ossification (Figure 2). In male patients, serum vitamin A levels negatively correlated with the severity of the T-OPLL index (Table 6). Serum vitamin A level in patients under 50 years of age showed a stronger negative correlation with the T-OPLL index than in patients over 50 years of age (Table 7). Serum vitamin B6 levels also negatively correlated with the total ossification index, the OALL-index, and T-OALL-index (Table 6). In patients over 50 years of age, serum vitamin B6 level negatively correlated with the T-OALL index, but that in patients below 50 years of age positively correlated with the T-OALL index (Table 7). In female patients, serum vitamin A levels did not correlate with the OPLL index. Serum vitamin B6 level positively correlated with the cervical OALL-index (Table 6). In patients over 50 years of age, serum vitamin B6 level negatively correlated with the T-OALL-index, but that in patients below 50 years of age did not correlate with the T-OALL-index (Table 7).
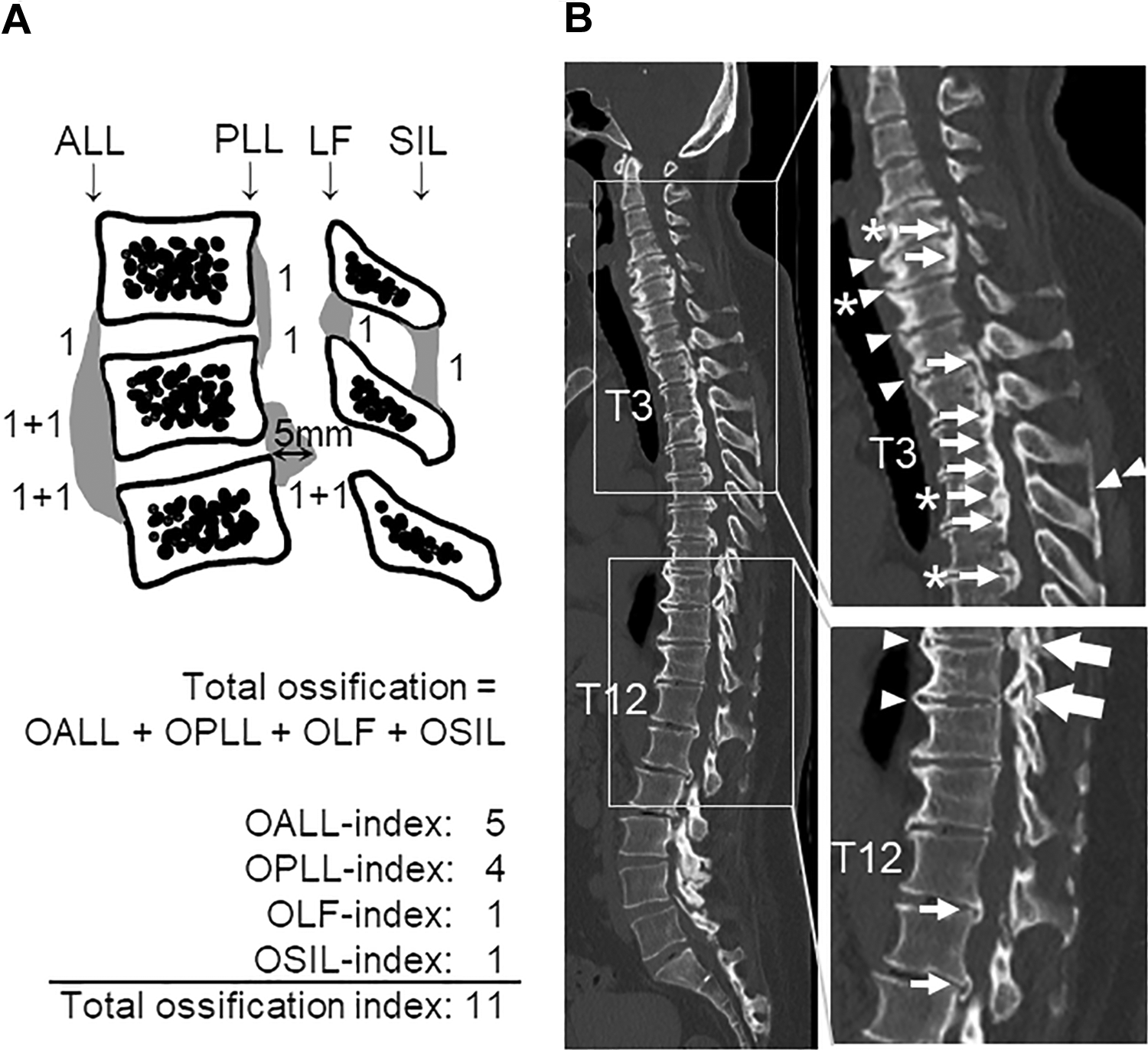
A representative case of heterotopic ossification of spinal ligaments. A and B, The ossification index determines the severity of ossification by scoring ligamentous ossification, including OALL (arrowhead), OLF (thick arrow), OPLL (thin arrow), and OSIL (double arrowhead) in each vertebra and intervertebral disc as 1 point. Asterisks indicate massive ossifications (thickness ≥ 5 mm), which are scored as 2 points. OALL, ossification of the anterior longitudinal ligament; OLF, ossification of the ligamentum flavum; OPLL, ossification of the posterior longitudinal ligament; OSIL, ossification of the supra/interspinous ligament; ALL, the anterior longitudinal ligament; PLL, the posterior longitudinal ligament; LF, the ligamentum flavum; SIL, the supra/interspinous ligament.
Correlation of the Serum Levels of Vitamin A (retinol) and Vitamin B6 (Pyridoxal-5-Phosphate) With Heterotopic Spinal Ligamentous Ossification in Patients With Thoracic OPLL.
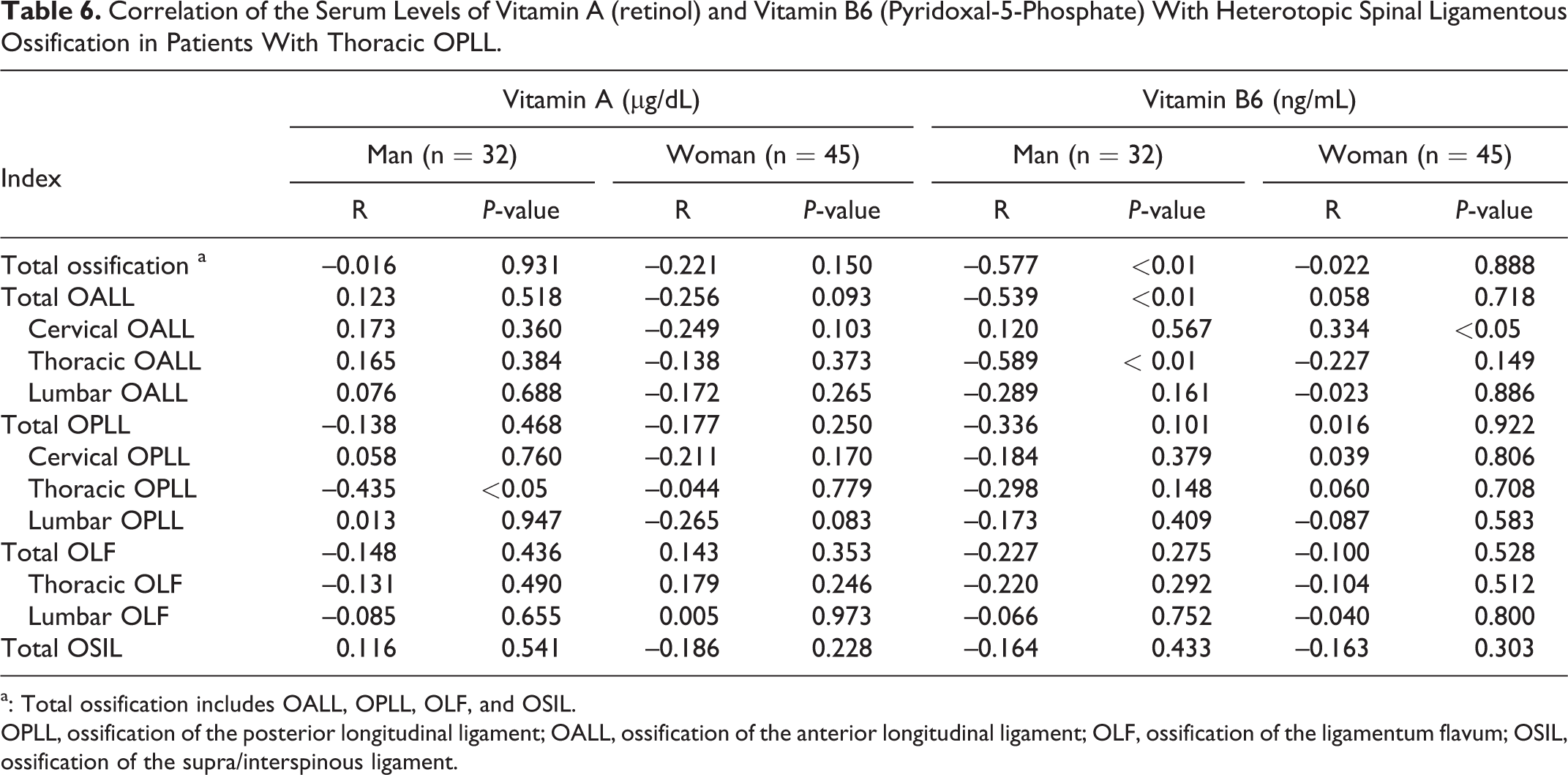
a: Total ossification includes OALL, OPLL, OLF, and OSIL.
OPLL, ossification of the posterior longitudinal ligament; OALL, ossification of the anterior longitudinal ligament; OLF, ossification of the ligamentum flavum; OSIL, ossification of the supra/interspinous ligament.
The Serum Levels of Vitamin A (retinol) and Vitamin B6 (Pyridoxal-5-Phosphate) and OALL- and OPLL Index in Patients With the Thoracic OPLL.
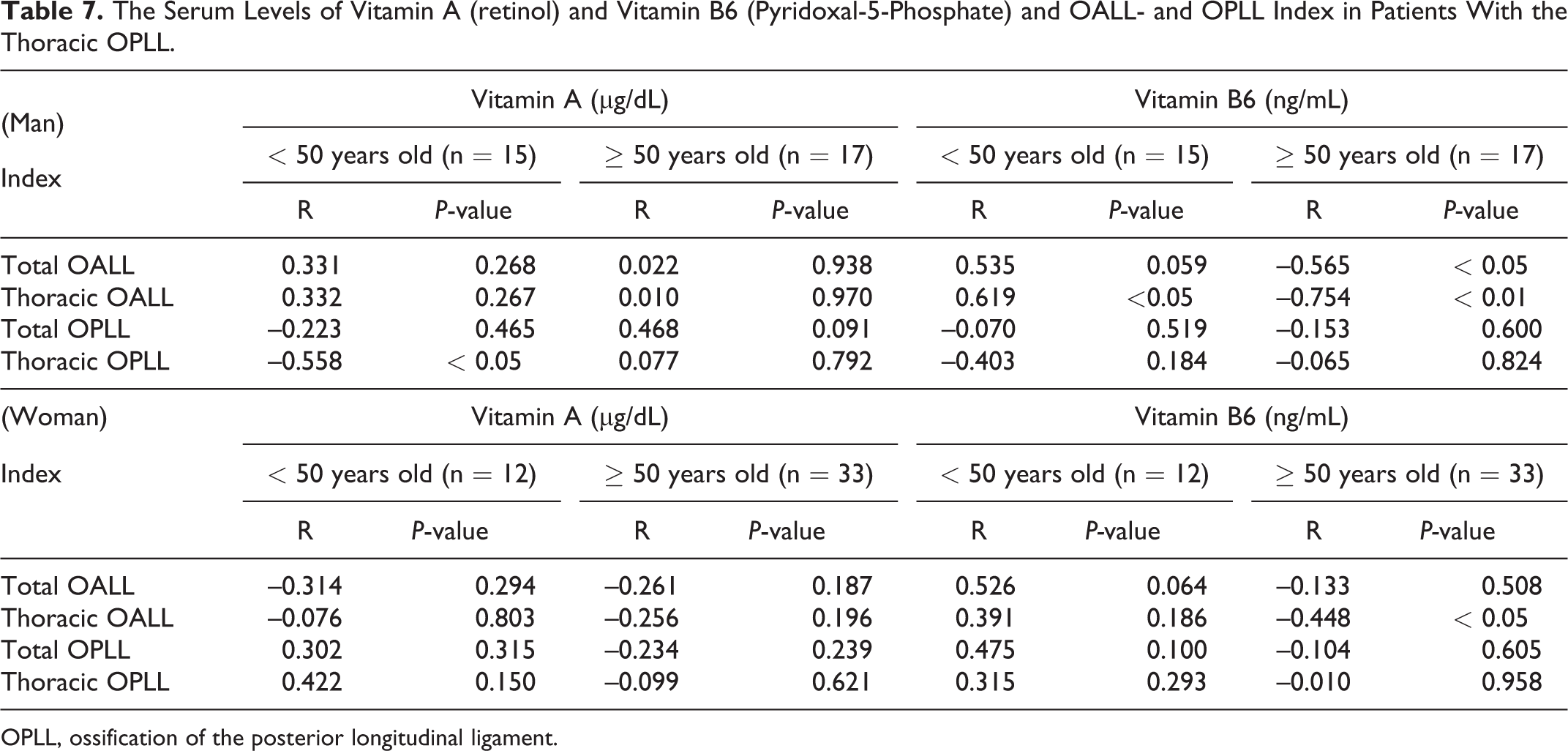
OPLL, ossification of the posterior longitudinal ligament.
Study 2-3: The Association of Exacerbating Factors Affecting the T-OPLL Severity
Finally, we performed a multiple regression analysis to identify factors for the severity of T-OPLL (Table 8). In male patients, a significant association with the T-OPLL index was found in age at onset of symptoms (P = 0.012) and serum vitamin A level (P = 0.041) (adjusted coefficient of determination [R2]: 0.332, variance inflation factor [VIF]): 1.11). In female patients, no significant association with the T-OPLL index was found.
The Association Between the T-OPLL Index and Variables by Multiple Regression Analysis in Patients With Thoracic OPLL.
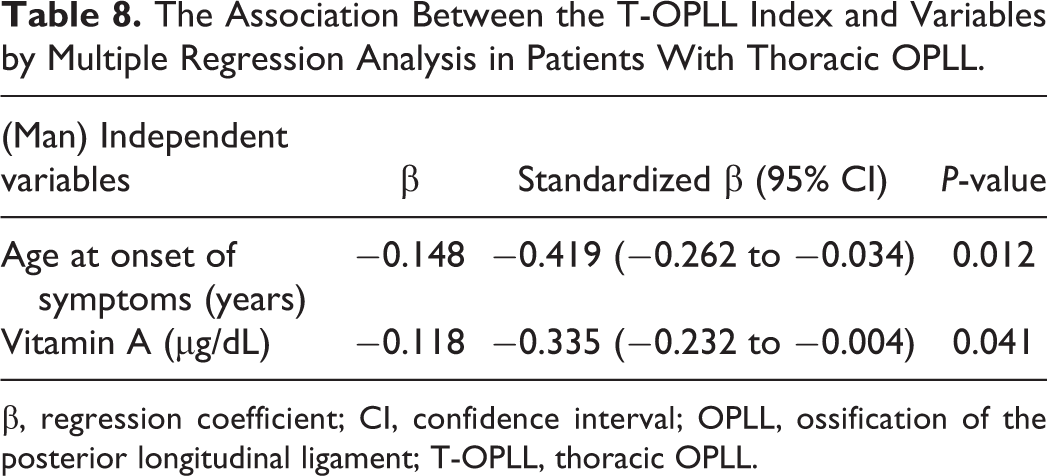
β, regression coefficient; CI, confidence interval; OPLL, ossification of the posterior longitudinal ligament; T-OPLL, thoracic OPLL.
Discussion
We found that unbalanced dietary habits in patients with early-onset OPLL are associated with the development or exacerbation of OPLL. Among the 99 micronutrients evaluated, potassium, calcium, vitamin A, and vitamin B6 were identified as deficient in patients with early-onset OPLL relative to non-OPLL controls. Previous studies reported that patients with cervical OPLL prefer salt-rich and/or plant protein-rich diets6,21; however, such preferences were not observed in this study either in patients with common cervical OPLL or early-onset OPLL.
The lower dietary intake of vitamins A and B6 in patients with early-onset OPLL was serologically verified. In T-OPLL patients below 50 years of age, serum vitamin A and vitamin B6 levels were significantly lower than those in the non-OPLL controls regardless of sex. Especially in male patients, young age of onset and low serum vitamin A levels were associated with the severity of T-OPLL. These results supported the possibility that vitamin A deficiency resulting from unbalanced dietary habits is associated with the development or progression of OPLL in early-onset OPLL patients.
Lower serum vitamin A level accelerates the progress of heterotopic ossification through enhancing endochondral ossification. This idea is supported by the following observations: 1) retinoic signaling is a strong chondrogenesis inhibitor22,23; and 2) nuclear retinoic acid receptor agonists suppress heterotopic ossification through the inhibition of endochondral ossification24-26 and OPLL occurs through endochondral ossification of the hypertrophied fibrous tissue. 27 Thus, vitamin A deficiency might attenuate the suppressive effect on the OPLL exacerbation. Vitamin A deficiency is also associated with chronic inflammation and insulin resistance, 28 and it has been speculated that insulin resistance is involved in OPLL exacerbation.29,30 Interestingly, in the 1980s, some case series reported that patients receiving long-term 13 cis-retinoic acids for psoriasis often developed heterotopic spinal ossification (OALL or OPLL),31-33 indicating that excessive vitamin A intake promotes OPLL. However, our data showed that none of the OPLL patients had an excessive intake of vitamin A, and none of them showed abnormally high serum vitamin A levels, suggesting that hypervitaminosis A is not associated with the development of primary OPLL. There is a possibility that the frequent occurrence of spinal ligament ossification in patients with psoriasis, which was reported in the 1980s, maybe due to spondylitis associated with psoriasis, not due to vitamin A.
Whether vitamin B6 deficiency is associated with heterotopic spinal ligamentous ossification was inconclusive from the results of this study. Serum vitamin B6 levels did not correlate with the severity of T-OPLL. In both men and women, serum vitamin B6 levels negatively correlated with the severity of T-OALL in patients over 50 years of age, but not in early-onset patients. Thus, vitamin B6 deficiency may be involved in late-onset rather than early-onset heterotopic spinal ossification. Type I collagen, a major component of the extracellular matrix, is susceptible to glycation because of its long half-life. 34 Vitamin B6 is an essential coenzyme of lysyl oxidase, which catalyzes the physiological cross-linking of collagen. 35 Vitamin B6 deficiency is known to decrease physiological cross-linking, ultimately leading to connective tissue degradation such as arteriosclerosis and impaired bone quality.35-37 Therefore, a vitamin B6 deficiency might make the spinal ligaments less flexible and more susceptible to micro-damage of the collagen fibers, which in turn leads to local inflammation, thereby promoting heterotopic endochondral ossification in the spinal ligaments.
This study has some limitations. First, a self-administered diet history questionnaire might over- or underestimate actual nutritional intake because the total nutritional consumption was calculated based on the memory of the intake frequency of certain foods. However, the BDHQ was developed for a detailed and quantitative investigation of Japanese nutrient and food intake; moreover, it has been widely used in many nutritional epidemiological studies.7-11 Second, the correlations between vitamin A deficiencies and the OPLL severity do not necessarily imply that such deficiencies actually play a role in the pathogenesis of OPLL; therefore, further preclinical animal studies and/or human clinical trials are needed to clarify whether vitamin A supplementation has therapeutic effects against ossification. Third, the study did not match BMI or other factors as potential confounders between cases and controls. It was difficult to enroll BMI-matched control patients because severely obese patients are quite rare in the general Japanese population (BMI > 30 kg/m2, 3.8%; BMI > 35 kg/m2, 0.5%). 20 Therefore, it was difficult to enroll BMI-matched control patients in a hospital-based case-control study. Finally, the present study consisted of 2 different designs and was based on the data from different populations. Serological and CT data of T-OPLL patients were collected from a nationwide multicenter study in Japan. However, BDHQ and serological data of controls were collected from patients in a single region of Japan. Although the mean BMI of control patients was similar to that of the general Japanese population, the risk of selection bias linked to the selection of controls must be considered.
In conclusion, this study showed that vitamin A deficiency resulting from unbalanced dietary habits is associated with the development or exacerbation of OPLL in patients with early-onset OPLL. Our findings suggest that genetic factors and nutritional imbalance interact with the causes of severe obesity, lifestyle-related diseases, and spinal ligamentous ossification in this class of patients. Our findings also suggest that improvement of nutritional imbalance might suppress ossification in this limited type of OPLL. Vitamin A and some of their related molecules could be considered as potential therapeutic targets for halting the development or exacerbation of heterotopic ossification.
Footnotes
Authors’ Note
Masahiko Takahata: Conceptualization, Methodology, Writing—Original draft, Supervision, Project administration, Funding acquisition. Tsutomu Endo: Formal analysis, Investigation, Writing—Original draft, Funding acquisition. Shiro Imagama: Investigation, Writing—Review & Editing. Satoshi Kato: Investigation, Writing—Review & Editing. Takashi Kaito: Investigation, Writing—Review & Editing. Hiroaki Sakai: Investigation, Writing—Review & Editing. Shiro Ikegawa: Writing—Review & Editing. Yoshiharu Kawaguchi: Investigation, Writing—Review & Editing. Masahiro Kanayama: Investigation, Writing—Review & Editing. Yuichiro Hisada: Investigation, Writing—Review & Editing. Yoshinao Koike: Investigation, Writing—Review & Editing. Kei Ando: Investigation, Writing—Review & Editing. Kazuyoshi Kobayashi: Investigation, Writing—Review & Editing. Itaru Oda: Investigation, Writing—Review & Editing. Kazufumi Okada: Formal analysis, Writing—Review & Editing, Ryo Takagi: Formal analysis, Writing—Review & Editing, Norimasa Iwasaki: Writing—Review & Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Kondou Kinen Medical Foundation, Grant-in-Aid for Scientific Research (C) from the Ministry of Education, Culture, Sports, Science and Technology [grant number 19K09566]; and Health, Labour and Welfare Science Research Grants for research on rare and intractable diseases [grant number H29-nanchi-ippan-040]. The funding sources had no involvement in the collection, analysis and interpretation of data and the writing of the report, and the decision to submit the article for publication.