
Abstract
The heterotopic mesenteric ossification, also known as myositis ossificans, is a rare form of heterotopic ossification, a metaplastic phenomenon where new bone is formed in the mesenteric base, generally after abdominal trauma (surgical or other). The pathophysiology of heterotopic mesenteric ossification is unknown; clinical presentation is not specific, with vague abdominal symptoms, uncertain radiological findings, and often regular laboratory exams. No consensus exists on the best possible approach, although it might well be both medical and surgical. We reviewed the clinical history of a 28-year-old man with a recent motor vehicle accident who was admitted to our surgical unit with symptoms consistent with a small bowel obstruction; after surgery, a diagnosis of myositis ossificans was surprisingly made.
Introduction
Heterotopic ossification (HO) is a metaplastic phenomenon in which new bone is formed outside the skeleton, in tissues that do not usually ossify. 1 It can be conceived as an aberrant tissue repair and is increasingly recognized as a common complication after trauma, surgery, and other local or systemic insults. Onset of ossification of mesenchymal tissues following orthopaedic surgery, trauma, and prolonged immobilization has been well described, 2 although intra-abdominal findings remain relatively rare. 3 Genetic forms of HO, such as fibrodysplasia ossificans progressiva and progressive osseous heteroplasia, are usually clinically evident since birth and continue to advance throughout life.4,5 Non-hereditary HO, instead, is limited and often arises in the context of trauma, arthropathies, or age-related pathologies. The heterotopic mesenteric ossification, also known as myositis ossificans, is a rare and benign form of HO, where a new budding of an ossifying pseudotumor develops in the mesenteric root, generally after abdominal trauma, whether surgical or of other type. 6 Heterotopic mesenteric ossification (HMO) was described for the first time by Wilson et al. 7 in 1999. HMO likely occurs in mid- to late adulthood and shows a preference for male patients.8,9 Many patients present with bowel obstruction, and a history of prior abdominal surgery or trauma is almost always reported. HMO has no malignant potential, but it may recur. 10 The pathophysiology of HMO remains unknown; the mechanisms include humoral factors, target cells, and genetic predisposition. Less than 40 cases have been reported in the literature. Herein, we describe one rare case of HO of the mesentery in a 28-year-old man who presented with bowel obstruction.
Case report
A 28-year-old man with no noticeable past medical history was hospitalized for widespread abdominal pain and vomiting at our emergency surgical unit. Three weeks before he had been involved in a motor vehicle accident and was admitted with a diagnosis of blunt thoracic and abdominal trauma; the treatment was conservative, and the patient was discharged after 7 days from hospitalization without need for blood transfusion. Our examination revealed moderate abdominal distention with pronounced tenderness in the lower quadrants, and blood examination showed only mild leucocytosis. An abdominal X-ray showed soft bowel distension with air–fluid levels. A computed tomography (CT) scan was then performed, which showed some calcifications within the mesentery root (Figure 1), gastric dilatation, distension with multiple air–fluid levels of the small bowel. In the right iliac fossa, there was an ileal loop with frankly thickened walls and signs of parietal suffering at a full-to-empty passage. Free fluid was sparsely evident in all the recesses of the abdominal cavity.

Calcification in the mesenteric root at CT scan.
Moreover, several apparently hyperplastic-reactive nodes were present along the mesentery root. Calcifications were not present at a previous CT scan performed in another hospital after the trauma hospitalization. After informed consent the patient was prepared for surgery, and initially a laparoscopic approach was hypothesized but not allowed due to a severe desaturation episode during the intubation. During the exploratory laparotomy, we identified a bulky and hardened mass of the small bowel arising within the mesenteric root and retracting the visceral peritoneum, with a frank malignant appearance. Consequently, a wide resection of the involved intestinal tract with the relevant mesenteric root was performed. Another similar small thickened nodule was removed from the peritoneum of the left iliac fossa. The postoperative course was regular, and the patient was discharged after 5 days in complete wellness and restored bowel functions. A 10% formalin solution was used to fix surgical samples for the routine histological examination. Final pathology report described thickened intestinal wall, due to diffuse oedema and areas of proliferating fibroblasts, mainly localized within the mesentery. Fibroblasts were arranged in thin bundles within a myxoid stroma with a lymphoid plasma cell and eosinophils background component. Atypia was unremarkable. The mesentery of the resected intestinal tract was almost entirely occupied by areas of bone-like metaplasia with naïve bone islands and deposition of calcium. These findings were consistent with the diagnosis of HMO (intra-abdominal myositis ossificans). Histological findings are shown in Figure 2.
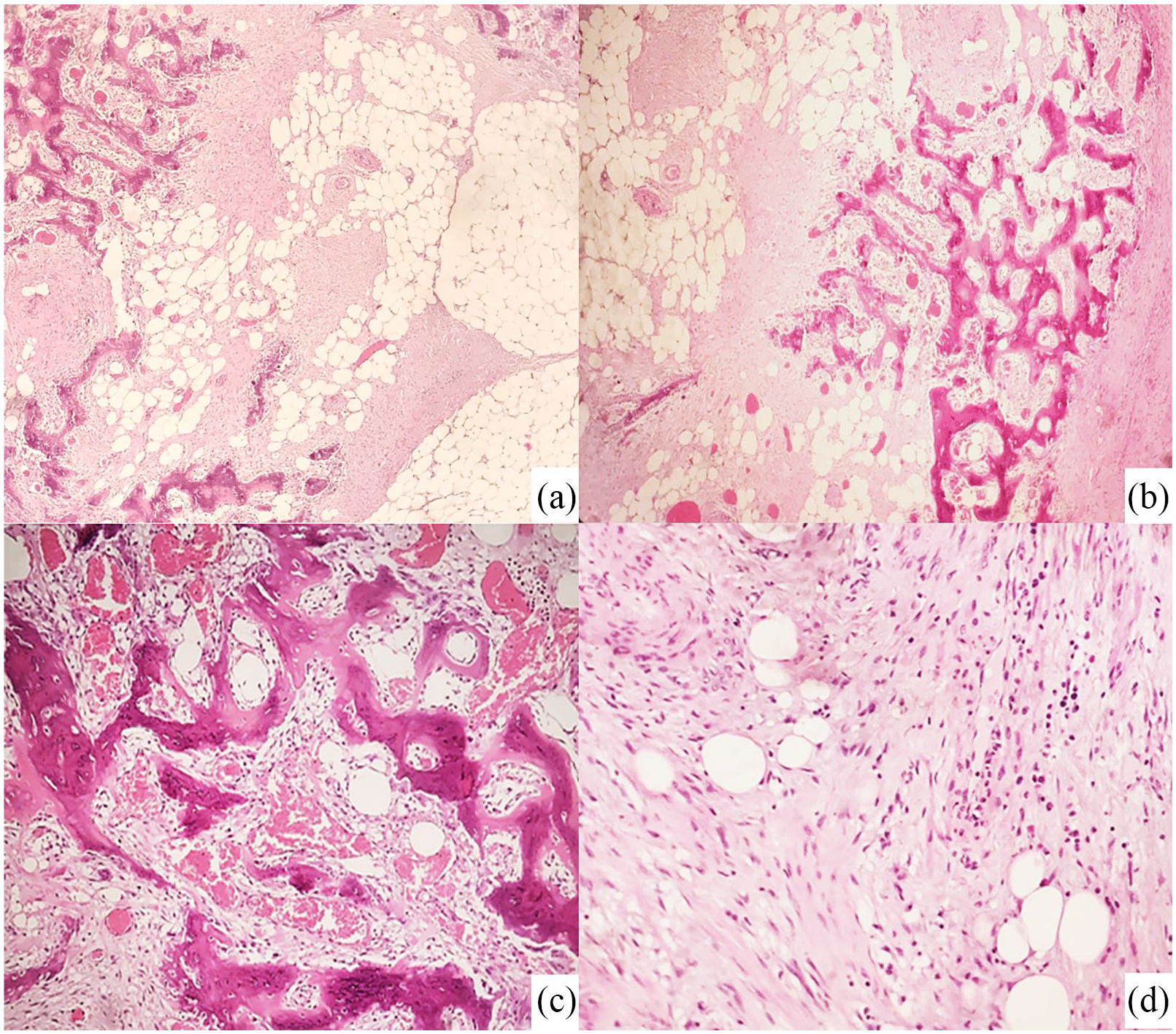
(a) and (b) Areas of bone-like metaplasia occupied mesentery with naïve bone islands and deposition of calcium. (c) Vascular congestion and (d) areas of proliferating fibroblasts arranged in thin bundles of myxoid stroma. Atypia was unremarkable. Hematoxylin and eosin stain: (a) 10×, (b) 10×, (c) 20×, and (d) 20×.
Discussion
Ossification of soft tissues following orthopaedic surgery, trauma, and prolonged immobilization has been well described; however, an intra-abdominal presentation is rare. HMO or intra-abdominal myositis ossificans is a subgroup of HO, in which a bone-like pseudotumor develops within the base of the mesentery; abnormal ossification may also be produced over the parietal peritoneum, as seen in our case, or again in the mesocolon or abdominal surgical incisions. 6 Reports presented in the literature suggest that for the HMO cases, a history of prior abdominal surgery or trauma is almost always present, as in our case. Merrell et al. 11 reported the interesting case of HO involving hip and mesentery, occurred 10 months after orthopaedic and abdominal surgery after a polytrauma event involving the pelvic ring and bowel injuries. As about the pathogenesis, HO may possibly be consequent to immature multipotent mesenchymal cells differentiating into osteoblasts or chondroblasts as a reaction to local injury, thereby producing bone areas formation. 2 This process might require some further input, like among others vessel congestion, edema, inflammation and secretion of local osteoinductive factors. 12 Amalfitano et al. 13 suggested a mechanism of endochondral bone formation to explain the development of HMO, with no obvious mutations in known genes that cause hereditary conditions of HO. Ranganathan et al. 14 hypothesized that this condition may be related to evolution of progenitor cells to osteogenic precursor cells thereby promoting cell-mediated interactions with the tissue microenvironment and conditioned by local oxygen tension, pH, availability of micronutrients, and mechanical stimuli. By large ectopic bone formation is mainly influenced by four factors. First, the need of a triggering event, like a trigger, that in our case was a blunt trauma during a car accident. Second, an encoding sign must emanate from the injury site although involved agents are unknown yet. Third, a necessary supply of mesenchymal cells must be hypothesized with a potential to differentiate into other types of cells, including chondroblasts or osteoblasts, if the right signal has been transmitted from the site of the injury. Finally, a permissive environment is paramount for this biological cascade to occur.15,16 Traumatic injuries are well-known causes of increased systemic inflammation that can lead to HO, as confirmed in a recent review by Meyers et al. 17 reporting several experimental models. Nonetheless, how the inflammatory cascade actually modulates development of an HO requires further research. HMO seems to have a strong male preponderance (men to women ratio of 15:1), 18 with ages ranging from 22 to 80 years old, mostly middle-aged individuals, and one case described in a child.19,20 In our case, the age of the patient was on average. Onset may become clinically evident weeks to years after abdominal surgery or trauma. Its presentation may not be specific, with vague abdominal symptoms. Patients usually present with symptoms of small bowel obstruction such as vague abdominal pain, nausea, and vomiting. Laboratory exams are often normal, with possibly elevated alkaline phosphatase likely reflecting an increased osteoblastic activity during heterotopic bone formation. 18 Preoperative diagnosis of HMO is difficult due to its rarity and occurrence of radiological confounders. Radiologically, several findings like mesenteric ossification, osseous neoplasia, oral contrast leakage, calcified abdominal cysts or neoplasms due to dystrophic calcification, extravasations or active bleeding might become challenging to properly distinguish from HMO, particularly in urgent clinical settings; also early stages of the disease show only a slight increase in soft tissue density.3,21 CT scans may also provide some evidence, like multiple linear branching opacities with trabecular ossifications 22 within the mesentery, the omentum or close to the surgical incision. In our case, for instance, there were diffuse mesenteric calcifications. An extremely high index of suspicion is required for an accurate preoperative diagnosis, and nonetheless, it is usually made intraoperatively. Once the right diagnosis is made, it has an excellent prognosis, with no evidence of malignant potential. At histology, a differential diagnosis is required to rule out sarcomas, which exhibit high cellularity, evident atypia and increased mitoses, aggressive histopathological changes most evident at the periphery of the lesion. 6 Treatment of HMO may be both medical and surgical, depending on the patient’s clinical condition and the extension of ossification. Because HMO is closely related to surgical interventions, surgical procedures have to be spared whenever possible for a proved benign, non-invasive condition, where surgical aggression may imply a high risk of recurrence.9,23 Surgery should be limited to those cases of clear-cut bowel obstruction in frankly symptomatic patients. In these cases, complete excision of bone formations is required. When surgery is unavoidable, local radiotherapy or treatment with bisphosphonates, cimetidine, or non-steroidal anti-inflammatory agents may help prevent recurrence,9,18,24 although these last measures require further investigation.
Conclusion
In summary, HMO is a rare presentation that can occur after trauma or abdominal surgery and can cause severe complications such as bowel obstruction. Predictive factors that could foresee which among patients, trauma or surgery types will progress to HMO formation have not yet been defined. HMO is a rare condition and is difficult to reach a consensus on the best possible approach. Altogether it is likely better to avoid surgery, if any possible, reminding its close relationship to surgery and high risk of recurrence. A therapeutic plan needs be individualized, depending on the patient’s clinical condition and the extent of ossification. At present, we believe that surgical therapy must be reserved to patients with evident abdominal symptoms, especially bowel obstruction.
In contrast, asymptomatic patients should be observed with frequent radiological examinations accounting for the progression of the disease. Radiologists, surgeons, and pathologists should keep in mind this entity and try to formulate a correct pre-operative diagnosis, avoiding misdiagnosis of benign or malignant soft tissue tumour and unnecessary interventions for a benign condition. Further studies are needed for understanding the exact pathogenesis and to formulate prophylactic or treatment strategies.
Footnotes
Acknowledgements
The authors thank Dr Luca Reggiani Bonetti and Dr Giulio Rossi for their precise and comprehensive histological slides review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient.