
Abstract
Study design
Randomised control study.
Objective
Different parenteral analgesics are used to alleviate post-operative pain after transforaminal lumbar interbody fusion (TLIF) but limited by their efficacy and side effects. We performed a RCT to evaluate the safety and efficacy of epidural Morphine-Bupivacaine on post-operative pain management after TLIF.
Methods
Consecutive patients (n=100) of TLIF were divided randomly into study (SG) and control groups (CG). At the end of procedure, SG (n=50) received epidural instillation of morphine 5 mg and bupivacaine .25% - 2 mL, along with 6 mL of .25% bupivacaine infiltration in the deep fascia before wound closure. The functional outcomes were assessed at regular intervals (4, 8, 12, 24, 36, 48, 72, 96 hours) with VAS, nausea and vomiting scale, Ramsay sedation scale and breakthrough analgesia needed, time to ambulation and other complications.
Results
The mean VAS score at 4 hours in SG was significantly less (1.16 ± .88) than the CG (3.32 ± 1.0) (P = .000). This significant difference was maintained at each time point during the first 48 hours (P < .004). Similarly, the mean NRS score in SG at 4 hours was 1.02 ± .89, and in CG 3.3 ± .69 (P = .0000) which was maintained at all intervals of assessment till 48 hours (P = .0137). The mean time to first ambulation was significantly less in the SG (4.46 ± 1.04 hours) than CG (11.64 ± 2.3 hours) (P < .001). There were no drug-related complications.
Conclusion
Epidural instillation of bupivacaine and morphine is safe and enables better pain relief in the initial 48 hours which helps in early mobilisation, and enhanced functional recovery.
Introduction
Currently, lumbar spinal fusion is one of the commonly performed spine surgical procedures. Between 2004 and 2015, the volume of elective lumbar fusion has increased by 62.3% (from 122,679 cases in 2004 to 199,140 in 2015) and maximum increases were noted for fusion for spondylolisthesis (111%) and degenerative scoliosis (183%). 1 With increasing surgeries, there has been tremendous increase in efforts to reduce the post-operative pain which otherwise can cause significant distress to the patient after spinal fusion procedure. Gerbarshagen et al. evaluated the pain intensity of 179 surgical procedures on the first post-operative day, and spinal fusion procedures ranked second among them. 2 The dissection of skin, subcutaneous tissue, deep fascia, paraspinal muscles, facet joints and posterior elements act as potent sources of pain after lumbar fusion procedure. Early mobilisation is essential for post-operative recovery, which however can be impeded by surgical site pain. 3 Delayed mobilisation due to ineffective post-operative analgesia can have a negative psychological impact on the patient and predisposes to problems of recumbency like respiratory complications, deep vein thrombosis and cardiac events. 4 Acute unrelieved post-operative pain also stimulates the autonomic nervous system resulting in release of catecholamines, post-operative cognitive dysfunction, and can potentially translate into persistent chronic pain in some individuals. 5
Multi-modal analgesia with synergistically acting drugs to regulate the pain has been the conventionally used method during the post-operative period. 6 Intravenous opioids, paracetamol and non-steroidal anti-inflammatory drugs are the commonly used drugs for post-operative analgesia. 6 However, parenteral and oral administration of these drugs, if used alone can be inadequate and in combination, can be associated with significant adverse effects like nausea, vomiting, dependence, respiratory depression, sedation and gastrointestinal disturbances. 7
Since the pain generators are originating from the spinal region, epidural space has been used as a potential drug-delivery route for pain relief. 8 Opioids are powerful analgesics and their unfavourable systemic side effects can be mitigated by local administration. Several studies have underscored the benefits of epidural morphine for pain relief in spine surgery.9–11 However, these studies have described its usage in the form of infusion pumps over 48 hours, which require constant monitoring and can be associated with catheter-related complications.9–12 In addition to its potent analgesic action, morphine also has a synergistic effect with local anaesthetics but their combined efficacy has not been tapped for post-surgical pain relief.13,14
For an intervention to be effectively used widely, it should be easy to administer, have less complications, require less monitoring, inexpensive and efficacious to the patient. Epidural instillation of morphine and bupivacaine is easy to administer and inexpensive. Non-randomised clinical studies have shown its efficacy in lumbar decompression surgeries. Hence, we performed a randomised control study to evaluate the safety and pain blockade after epidural instillation of bupivacaine and morphine, in patients who underwent open TLIF.
Materials and Methods
The study was a prospective randomised control study performed in a tertiary care hospital after obtaining institutional review board approval and endorsement from the clinical trial registry (registration number CTRI/2019/01/023518AU). All consecutive patients who underwent TLIF surgery were included in the study. Standard indications included degenerative, lytic and dysplastic spondylolisthesis, and fusions for recurrent discs and instability. Patients with less than 20 years of age and more than 70 years of age, those with more than two-level fusion procedure, pre-operative neurological deficits with power less than MRC grade 3, and those with post-operative drain and intraoperative CSF leak, those having spinal tumours, trauma and infection and revision fusions were excluded from the study.
The sample size was calculated based on the effect size of .52 with Zα = .050, confidence interval = 1.96 to be minimum of 33 patients per group would be needed. Based on the population mean of VAC score, the achieved power value was .95 using SPSS vs 28.0. We recruited consecutively admitted patients planned for open transforaminal lumbar interbody fusion, after explaining the risks and benefits to the patients and obtaining an informed written consent (Figure 1 – CONSORT). Patients were randomised by computer-generated random numbers (www.randomiser.org) into the Study group (SG) and the Control group (CG). On the night before surgery, all patients received a standard multi-modal pre-emptive analgesia (one tablet each of paracetamol 1gm, aceclofenac 100 mg and pregabalin 75 mg). CONSORT diagram showing allocation of patients into study and control groups.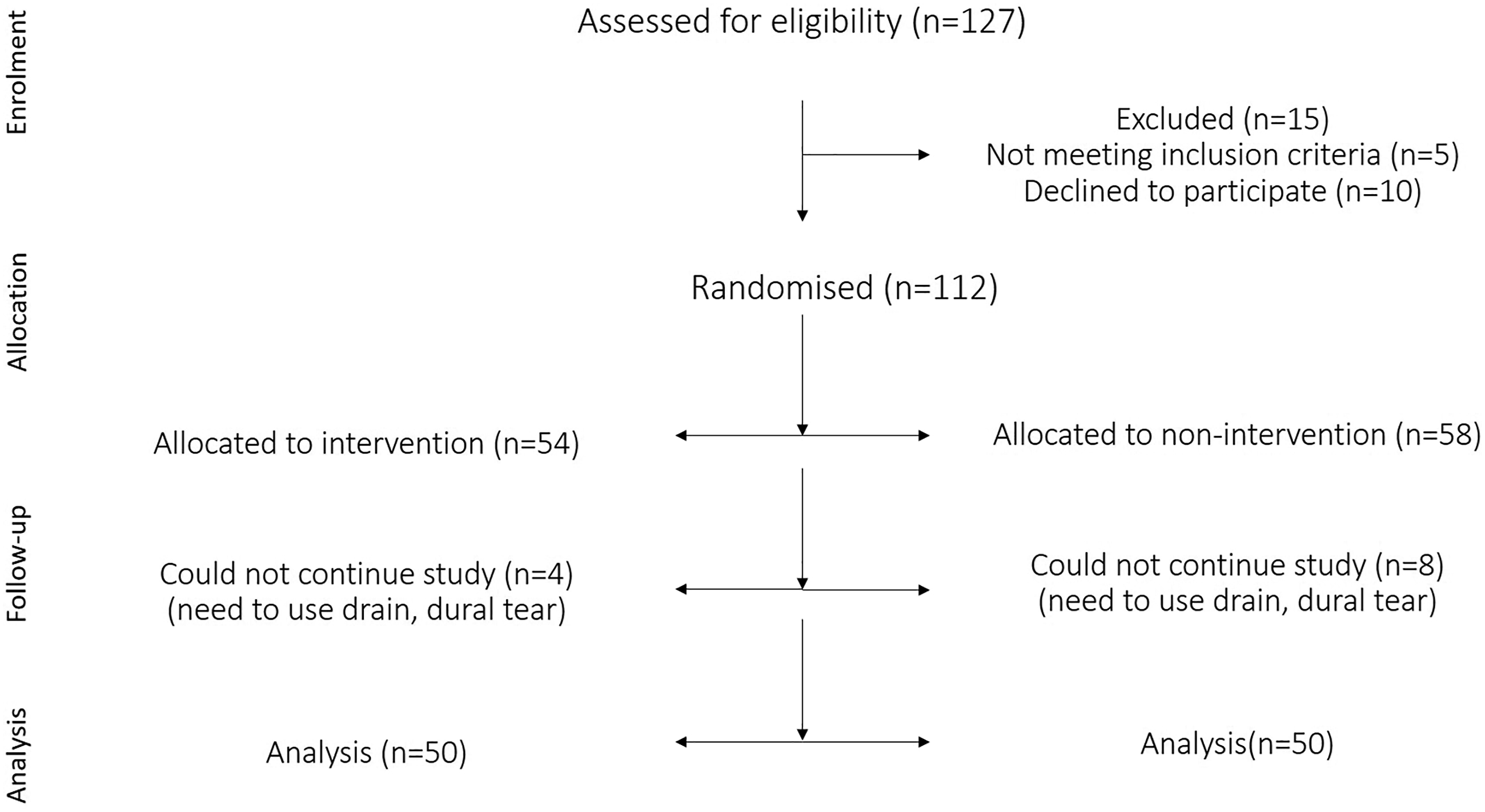
For the sake of uniformity, one of the authors performed all the surgeries and followed similar decompression and fusion techniques in both groups. Once the rods were placed and final tightening of the nuts were performed, complete haemostasis was achieved. At this stage, in patients of the study group (SG), morphine – 5 mg and bupivacaine .25% – 2 mL was instilled over the exposed dura. Then the muscles and fascia were approximated in layers without the use of any suction drain. Generally, a wound drain was avoided in all patients undergoing TLIF surgery. But when there is a risk of haematoma like patients on blood thinners, chronic liver disease, and persistent oozing despite haemostasis, a sub-fascial drain was placed, and such patients were excluded from the study fearing elution of drug into the drain. After closing the fascia, 6 mL of .25% bupivacaine was infiltrated in the deep fascia followed by closure of the subcutaneous tissue and skin. The aim was to block all potential pain generators which could incite pain in the immediate post-operative period. This was similar to the cocktail of drugs used in peri-articular infiltration after total knee replacement. 15 Patients of the control group (CG) neither received installation nor infiltration intraoperatively. Similar post-operative protocol for analgesia was followed in both the groups (3 doses of intravenous paracetamol during the first 24 hours, followed by 3 daily doses of oral paracetamol 1000 mg, aceclofenac 100 mg twice a day and one tablet of pregabalin 75 mg at bedtime for next 3 days) while tramadol 100 mg was used for breakthrough analgesia.
The outcomes were measured by a spine fellow who was not involved either in randomisation nor in statistical analysis. The primary outcome was post-operative pain and was measured by visual analogue score (VAS), Numeric pain intensity score (NRS) at regular intervals (4hrs, 8hrs, 12hrs, 18hrs, 24hrs, 36hrs, 48hrs, 72 hrs and 96hrs) till 96 hours. Adverse effects were measured using post-operative nausea vomiting (PONV) score and Ramsay sedation score. Other parameters like number of days of hospital stay, urinary retention, time for ambulation, number of doses of breakthrough analgesia required were also compared in both the groups.
Statistical Analysis
Continuous variables were presented as mean ± SD and their differences were analysed using SPSS vs 27.0 and R-packages 4.0.3 (2020-10-10). Categorical data was represented as percentage. To adequately control the occurrence of Type-I error, assessment of normality was done using Shapiro–Wilk (SW) test and Kolmogorov–Smirnov (KS) test. Since our sample group had a minimum of 50 subjects, Shapiro–Wilk test was considered to state the normality of the data. The result of SW test rejecting null hypothesis, a nonparametric Mann–Whitney U-test was applied to calculate significant differences between the pain scores – VAC, NPI, (post-operative nausea vomiting) PONV, sedation levels, at 4 hr, 8 hr, 12 hr, 18 hr, 24 hr, 36 hr, 48 hr, 72 hr, 96 hr and other outcomes such as: need for tramadol, time-taken for mobilisation, duration of hospital stay and urinary retention. A 2 proportion z-test was used to analyse the significance of male: female proportions in control and cases. Two-tailed alpha was set at .05 for all the tests.
Results
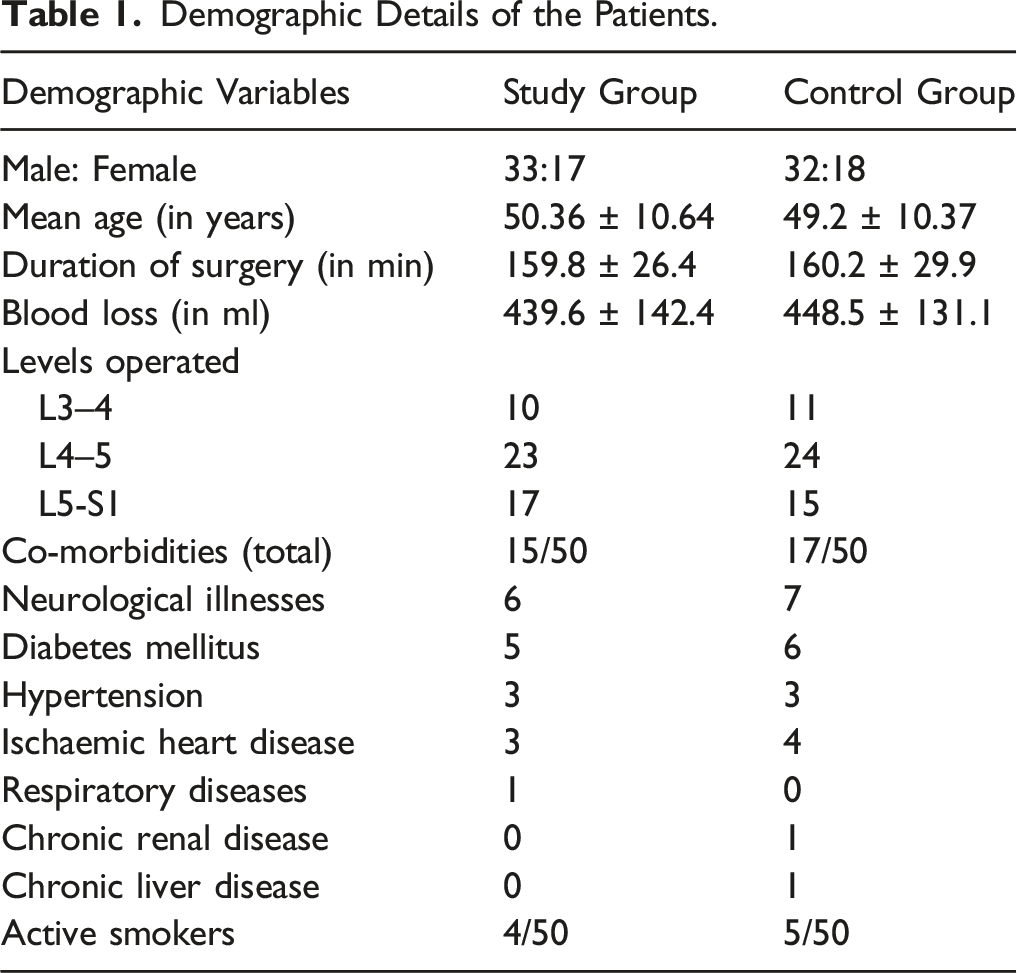
Demographic Details of the Patients.
Shows the Mean Values of the Different Parameters Studied at Different Time Intervals in the Control Group and Study Group and the Statistical Differences Observed (P values).
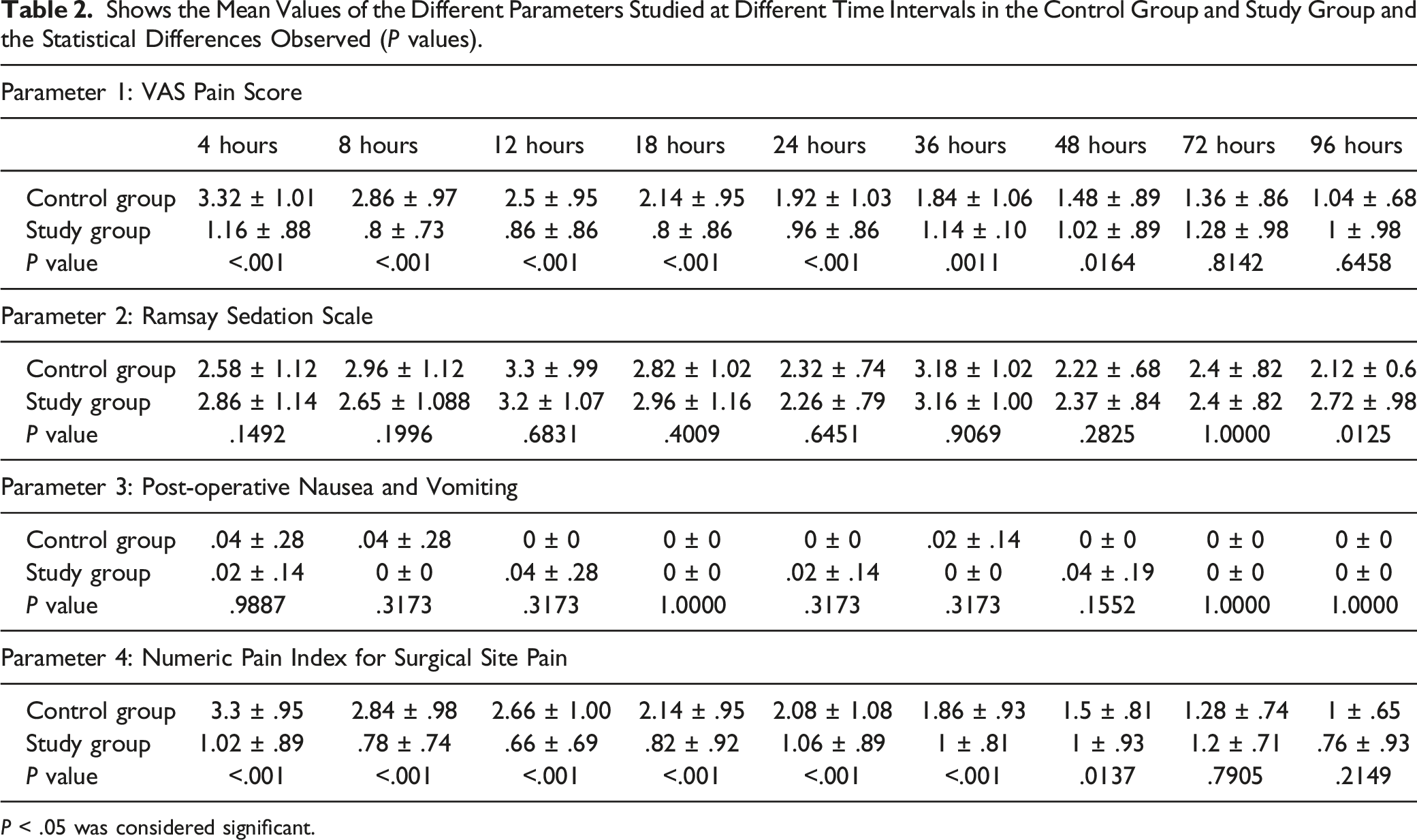
P < .05 was considered significant.
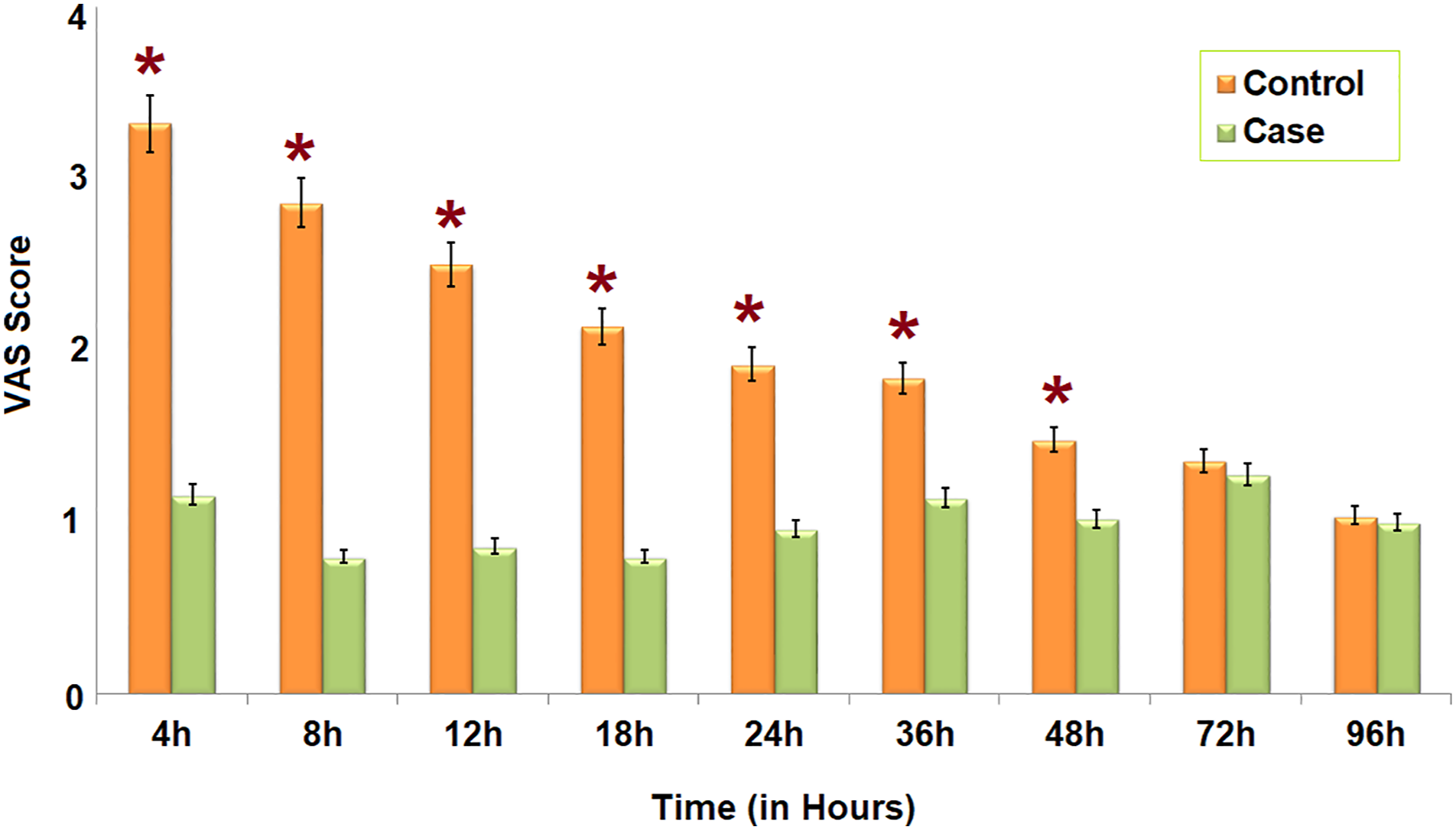
A: The VAS scores in the study group (green) and the control group (orange) at different time intervals in the post-operative period. At every time point in the first 48 hours, the pain relief is significantly better in the study group.
There was no significant difference in post-operative nausea and vomiting score, and Ramsay sedation scale between the 2 groups (Table 2). No complications related to epidural bupivacaine in the form of transient numbness or weakness, or systemic effects of morphine such as vomiting and respiratory difficulty were documented.
The mean time to first ambulation was significantly less in the study group being 4.46 ± 1.04 hours, when compared to the control group (11.64 ± 2.3) hours in CG (P < .001). Eleven patients of the CG needed tramadol as breakthrough analgesia, while only 2 patients of the SG required it (P = .008). Four patients of the study group and 5 patients of the control group developed urinary retention requiring catheterisation which was not statistically significant. Mean hospital stay for the SG was 75.32 ± 24.06 hours which was less than that of the control group (84.42 ± 19 hours) (P = .05).
Discussion
Our randomised controlled study has indicated that a combination of epidural morphine and bupivacaine provides immediate and adequate post-operative analgesia after spinal fusion surgery and its benefits are maintained even up to 48 hours. There were added advantages of ease of administration, no side effects like nausea, vomiting, respiratory depression, no requirement of continuous monitoring and early ambulation.
Spinal fusion surgery provides significant improvement in instability-back pain and relieves radicular pain and thus enables patients to regain mobility with decreased pain. However, post-operative surgical pain after fusion surgery can be severely disabling especially during the initial 3 days. 16 The pain during the immediate post-operative period is secondary to nociceptive stimulation and it is characterised by remissions and sudden exacerbations.6,16 Improper control of surgical pain has a gamut of after-effects – leads to urinary retention, prolonged use of analgesics, more extended hospital stay, increased expenses, deep vein thrombosis and occasionally cardiac ischaemia. Hence, pain management is a crucial aspect of patient care during the post-operative period and a tremendous amount of research and effort has been performed in this subject. Currently, multi-modal analgesia initiated pre-emptively is the most commonly accepted standard form of care. 7 Though parenteral drugs – NSAIDS, and paracetamol are the main workhorses for pain relief, they are often found inadequate and there is an increasing reliance on parenteral opioids. But parenteral opioids are associated with increased side effects, risks of long-term usage and dependence and hence several measures to obviate its usage have been developed.17,18
One of the key measures is to tap the advantages of opioids by using them topically at the surgical site. While topical opioids retain all the important pain-relieving effects of opioids in general, they are significantly devoid of the systemic side effects of opioids such as respiratory depression, nausea and vomiting. Hence, the administration of local opioids either epidurally or intrathecally gained in popularity. Epidural administration of the morphine for back pain was initially used by Beher et al 19 and subsequently several authors have used it in their case series.20–23 An important limitation of such studies is that they are non-randomised, inadequately powered, usage in low pain intense surgeries such as laminectomy and the use of epidural catheter pumps with their attendant risks like catheter pull-out, breakage and infection. Further the risks of respiratory depression and other side effects have been highlighted by some authors which restricted its common usage.24,25 In our study, we have used low dose morphine (5 mg) epidurally as a direct instillation over the dura without the need for catheter and pumps. Our results also indicate that the risks of respiratory depression are unfounded in the dose that we used.
Our study is the first to evaluate a combination of local instillation of epidural morphine and bupivacaine as a cocktail for post-operative pain control after fusion. Bupivacaine is a long-acting amino-amide local anaesthetic agent which provides analgesia through inhibition of voltage-gated sodium channels and depolarisation of sensory nerves. It provides substantial and immediate post-operative pain relief, especially after procedures requiring extensive soft-tissue dissection and retraction as seen in a lumbar interbody fusion. The synergistic effect of morphine and bupivacaine for pain relief has been described before and its effective usage is described in our study.13,14 A single dose of epidural morphine provides consistent pain relief up to 24 hours and its synergistic use with bupivacaine can extend this benefit up to 48 hours. The first 24 to 48 hours are the maximum painful period after a spine surgery and adequate control of pain during this period enables positive psychological feeling, early ambulation and prospects of early return to home. In our study, the mean time to first ambulation was significantly less in the study group (4.46 ± 1.04 hours, vs 11.64 ± 2.3 hours).
Intraoperative epidural instillation is a safe, simple and low skill procedure and is performed under direct vision. We used 5 mg of morphine at 1 mg/mL concentration along with 2 mL of .25% bupivacaine along with 6 mL of .25% bupivacaine for infiltration of deep fascia. Post-operative VAS and NRS scores were significantly better in the study group in the first 48 hours. This enabled quick rehabilitation in the absence of any prominent side effects. The main strengths of our study include its robust design (adequately powered, randomized, single-surgeon series with a blinded observer). However, the technique cannot be used if there is a pre-existing neurological deficit, dural tear during the surgery and if there is a need to use a surgical drain at the end of the procedure. The study has a few limitations. The mean age of the study group was relatively young and hence the effects of epidural morphine in elderly patients (>70 years) could not be studied. The time to mobilisation was mainly decided on the patient’s pain relief and in elderly patients, more objective methods like TUG test should be applied before mobilisation. Further, the long-term effects of these drugs on functional outcomes can also be evaluated in future studies.
To conclude, we note that the epidural instillation of cocktail of bupivacaine and morphine with perifascial bupivacaine infiltration provides better pain relief in the crucial initial 48 hours after surgery. This also helped in early mobilisation of the patients, which could potentially help in enhanced post-operative recovery and improved functional outcomes.
Footnotes
Acknowledgments
The authors would like to acknowledge and thank Ms Sharon Miracle Nayagam for her guidance in statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was funded by the Ganga Orthopaedic Research and Education Foundation (GOREF).