
Abstract
Study Design
Ambispective cohort study.
Objective
Canada has a government-funded universal health care system. The United States utilizes a multitier public and private system. The objective is to investigate differences in clinical outcomes between those surgically treated for lumbar disc herniation in a universal health care and multitier health system.
Methods
Surgical lumbar disc herniation patients enrolled in the Canadian Spine Outcome Research Network (CSORN) were compared with the surgical cohort enrolled in the Spine Patients Outcome Research Trial (SPORT) study. Baseline demographics and spine-related patient-reported outcomes (PROs) were compared at 3 months and 1 year post-operatively.
Results
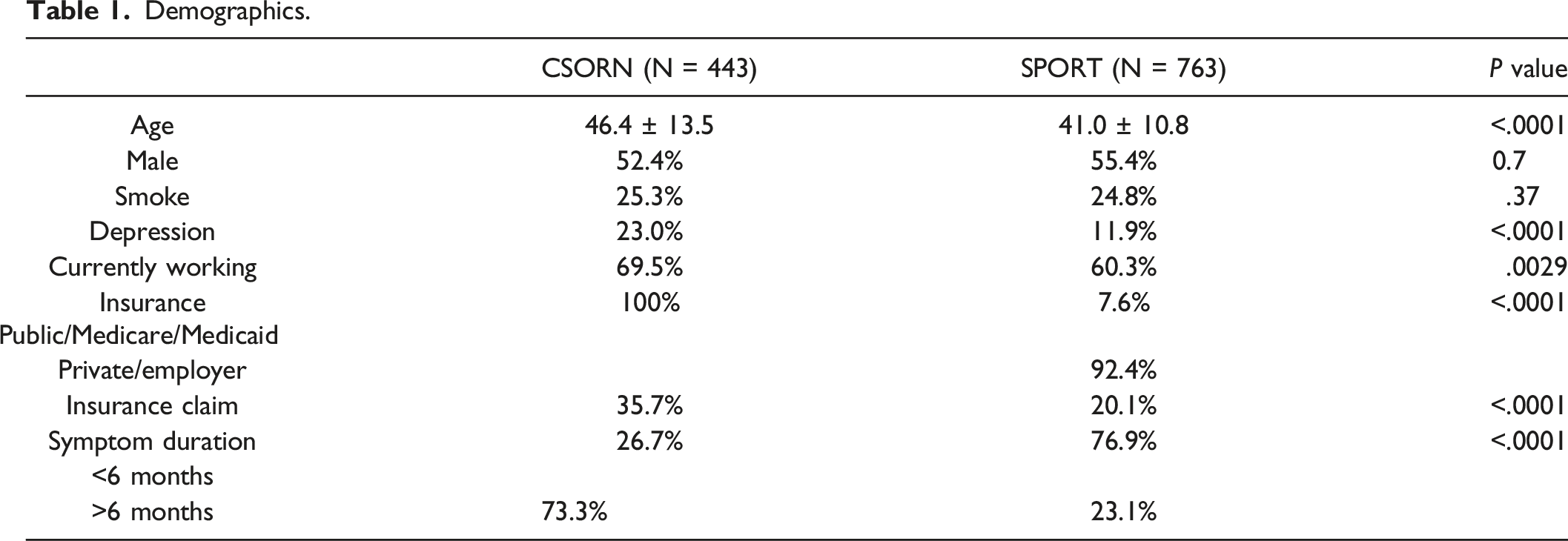
The CSORN cohort consisted of 443 patients; the SPORT cohort had 763 patients. Patients in the CSORN cohort were older (46.4 ± 13.5 vs 41.0 ± 10.8, P < .001) and were more likely to be employed (69.5% vs 60.3%, P = .003). The CSORN cohort demonstrated significantly greater rates of satisfaction after surgery at 3 months (87.2% vs 64.8%, P < .0001) and 1 year (85.6% vs 69.6%, P < .0001). Improvements in back and leg pain followed similar trajectories in the two cohorts, but there was less improvement on ODI in the CSORN cohort (P < .01). On multivariable logistic regression, the CSORN cohort was a significant independent predictor of patient satisfaction at 1-year follow-up (P < .001).
Conclusions
Despite less improvement on ODI, patients enrolled in CSORN, as part of a universal health care system, reported higher rates of satisfaction at 3 months and 1 year post-operatively compared to patients enrolled within a multitier health system.
Introduction
The United States has a multitier health care system where patients obtain health insurance through private (employer provided/individually purchased) or public (Medicaid or Medicare) providers. 1 Patients can directly access specialist care without a primary physician referral. In contrast, the Canadian health care system is publicly funded and patients cannot access specialist care without an initial referral from their primary care provider. These distinct systems create unique challenges: rising health care costs and disparities in access to care are major concerns in the United States, whereas wait times for specialist care and surgery are additional significant issues in Canada.2-4
Health care systems can be compared on many levels with diverse objectives. One of the most important parameters is patient-reported outcomes (PROs) of patients with the same pathology treated in different health care systems. It is critical to the analysis that the cohorts are truly characteristic of the health care system they purport to represent. The Canadian Spine Outcomes and Research Network (CSORN) is a nationwide multicentre prospective clinical registry. It comprises observational data on patients with a variety of spinal conditions including lumbar disc herniation. 5 The Spine Patient Outcomes Research Trial (SPORT) for lumbar disc herniation was a multicenter prospective clinical trial conducted in the United States that compared surgical to non-surgical management of lumbar disc herniations and included both randomized and observational cohorts. 6
Given the significant differences between these health care systems, comparing PROs may provide insights into the impact of a health care delivery system on the perceived outcomes. The purpose of this study is to compare the PROs between patients undergoing surgical treatment for lumbar disc herniations in a universal vs multitier health system. Secondary outcomes include the determination of independent predictive factors of PROs.
Methods
Study Design
An ambispective analysis of prospectively collected data from the CSORN registry and SPORT trial for lumbar disc herniation was undertaken. The CSORN database consisted of consecutive adult patients (18 years and older) undergoing surgery for lumbar disc herniations between 2013 and 2017 who were available for one-year follow-up.
Canadian Spine Outcomes and Research Network is a network of spine surgeons from 16 tertiary care hospitals across Canada that prospectively enrolls consecutive patients referred to these centers. Data quality and performance are audited by a national database coordinator which sends quarterly reports to each hospital site. Data completion and follow-up rates are tracked in the reports to facilitate internal data validation at each site. Written informed consent is obtained from all participating patients. Patient identification is anonymized to ensure that patients in the Network cannot be individually identified. All participating sites obtained Research Ethics Board (REB) approval prior to any data collection. Decisions regarding data collection, storage, and analysis are independent of any particular company or commercial interest.
The SPORT data for patients undergoing surgery for lumbar disc herniations 6 was obtained with permission from the SPORT-working group. SPORT data comprised patients from both the randomized and observational cohorts.
Demographics
Age, sex, smoking status, employment, presence of a compensation/claim, insurance status, depression, and spine symptom duration were tabulated and compared. Depression was classified in a binary fashion and self-reported in the SPORT cohort while CSORN registry used the Patient Health Questionnaire (PHQ-9) to determine the presence depression. 7 Employment status was categorized as working or not working. Patients with worker compensation or medical-legal claims were both considered compensated. Insurance was either private/employer or Medicare/Medicaid/public. All patients in the CSORN cohort are publicly insured. Symptom duration, as reported by the patient at baseline assessment, was categorized as: less than 6 months and greater than 6 months.
Outcome measures
Patient-reported outcomes were obtained at baseline, 3 months, and 12 months post-operatively using the Oswestry Disability Index (ODI), 8 the Physical (PCS) and Mental Component Summary (MCS) summary of the SF-12 (CSORN) 9 or SF-36 10 (SPORT), and Euroquol 5-dimension index (EQ5D). 11 Direct comparison of PCS and MCS derived from either SF-12 or SF-36 questionnaires has previously been demonstrated to be valid.12,13 The numeric pain rating scale (NRS) determined the level of pain. The 6-point scale used in the SPORT studies was converted to a 10-point scale, as used in CSORN. Satisfaction in both cohorts was assessed using a 5-point scale of very dissatisfied, somewhat dissatisfied, neutral, somewhat satisfied, and very satisfied. Satisfaction was dichotemized to satisfied (somewhat/very satisfied) or unsatisfied (neutral, somewhat/very dissatisfied).
Statistical analysis
Baseline and demographic factors are presented as frequency distributions or mean and standard deviation. Differences in demographic and clinical factors were analyzed with the Mann–Whitney U test for continuous variables and Fisher exact test for categorical variables between the CSORN and SPORT cohorts. To assess changes in PROs over time and differences between the two cohorts over time, repeated measures analysis of variance (ANOVA) was used to assess these changes at baseline, 3 months, and 12 months post-operatively. Then, binary multivariable logistic regression, with satisfaction as the dependent variable, was used to determine independent predictors of satisfaction at 1 year post-operatively. As well, multivariable linear regression, with ODI as the dependent variable, was used to determine significant predictors of function 1 year after surgery. For the multivariable models, demographic factors on univariate analysis that met a threshold of P < .2 were then entered into each model and retention in the model was determined using backwards selection until only significant variables remained. A P value <.05 was used to determine statistical significance. Missing data were accounted for using a carry forward approach with last observation. Statistical analyses were conducted using R Studio (RStudio Inc., Boston, MA, USA) and SPSS software (version 25.0, IBM, Chicago, IL, USA). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) was used. 14
Results
Demographics
Demographics.
Baseline Patient-Reported Outcomes.
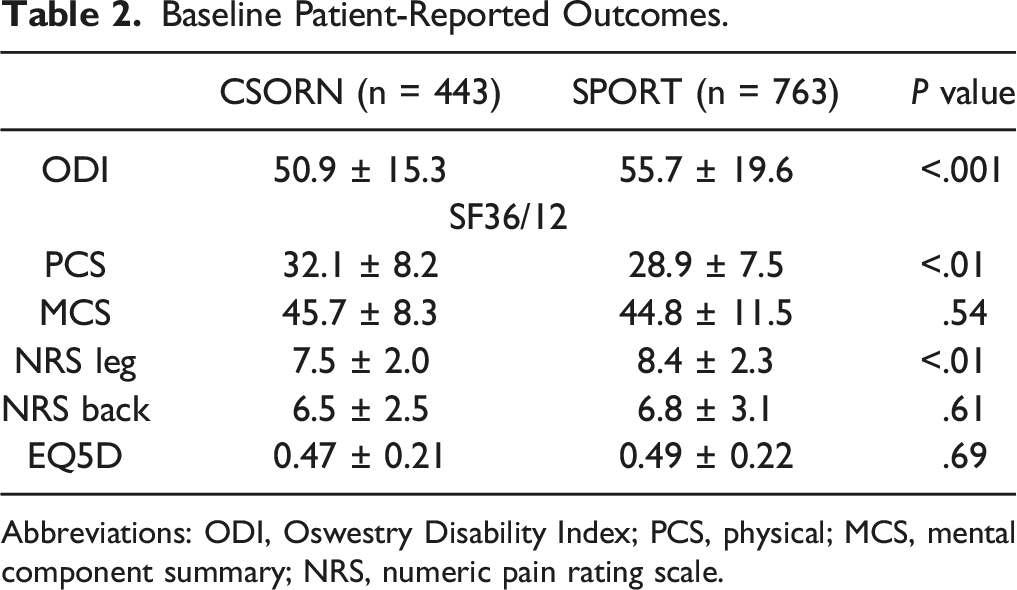
Abbreviations: ODI, Oswestry Disability Index; PCS, physical; MCS, mental component summary; NRS, numeric pain rating scale.
Patient-Reported Outcomes
Improvements in Disability, Pain, and Health-Related Quality of Life After Surgery for Lumbar Disc Herniation.
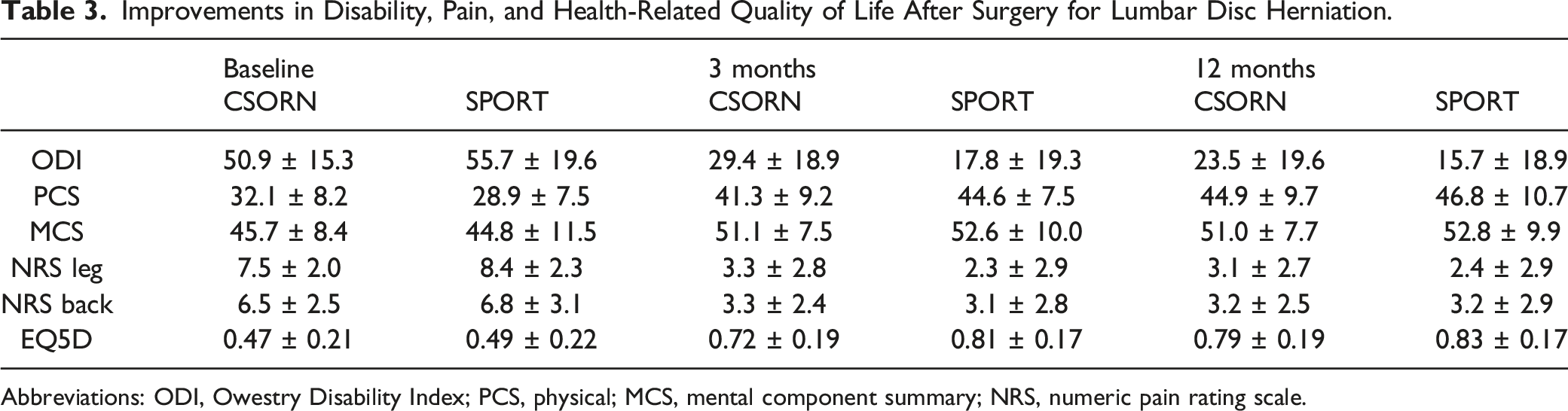
Abbreviations: ODI, Owestry Disability Index; PCS, physical; MCS, mental component summary; NRS, numeric pain rating scale.
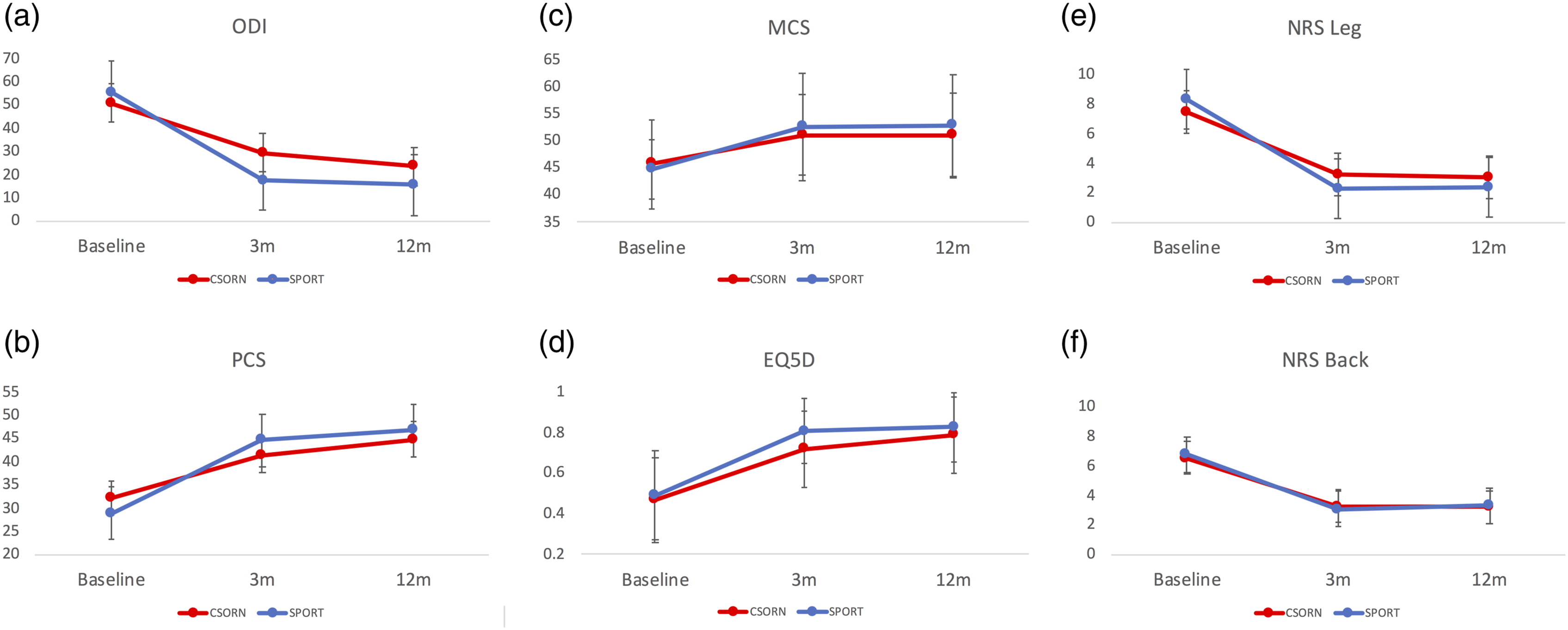
Time course of patient-reported outcomes after surgery for lumbar disc herniation. The time course of patient-reported outcomes on the Oswestry Disability Index (A), physical component summary of the SF36/12 (B), mental component summary of the SF36/12 (C), EQ5D (D), numeric rating scale of leg pain (E), and back pain (F). Blue lines represent the SPORT cohort, and red lines represent the CSORN cohort. Abbreviations: SPORT, Spine Patient Outcomes Research Trial; CSORN, Canadian Spine Outcomes and Research Network.
PCS scores significantly improved in both cohorts (F[2954] = 49.6, P < .001). There were improvements from baseline to 3 months post-operatively and then a more gradual improvement from 3 months to 1 year post-operatively (Figure 1B). The CSORN cohort had a higher baseline PCS score (difference: 3.2 ± .51, P < .01) while the SPORT cohort had higher PCS scores at 3 months (difference: 3.3 ± .65, P < .01) and 1 year (difference: 1.9 ± .68, P < .01), although these differences are small and not clinically relevant.
MCS scores also improved in both groups (F[2954] = 6.1, P < .001). There were no differences between groups at baseline but small clinically insignificant differences between the two cohorts at 3 months (1.5 ± .6, P = .02) and 1 year post-operatively (1.8 ± .58, P < .01). Both cohorts demonstrated improvement from baseline to 3 months and then plateaued by 1 year on the MCS, Figure 1C.
Baseline EQ5D scores were not different between the groups but the SPORT cohort had higher scores at 3 months (difference: .09 ± .11, P < .01). Both cohorts showed steep improvements from baseline to 3 months. The SPORT cohort plateaued between 3 months and 1 year, while the CSORN cohort demonstrated consistent slight improvement from 3 months to 1 year (Figure 1D). Overall EQ5D scores significantly improved in both groups (F[2936] = 10.7, P < .001).
Both the CSORN and SPORT cohorts had clinically significant improvements in the leg and back NRS scores (Leg: (F[2967] = 38.7, P < .001); Back: (F[2967] = 46.9, P < .001). NRS leg scores were higher for the SPORT cohort at baseline (difference: .9 ± .15, P < .001) but lower at 3 months and 1 year post-operatively (difference: 3 months 1.0 ± .19, 1 year .7 ± .2, P < .001). NRS back scores were not different between cohorts at any time point. In both SPORT and CSORN, the NRS leg and back scores rapidly improved from baseline to 3 months and then plateaued between 3 months and 1 year (Figure 1E and F).
Multivariable Linear Regression of Predictors of ODI at 1 Year Post-Operatively.
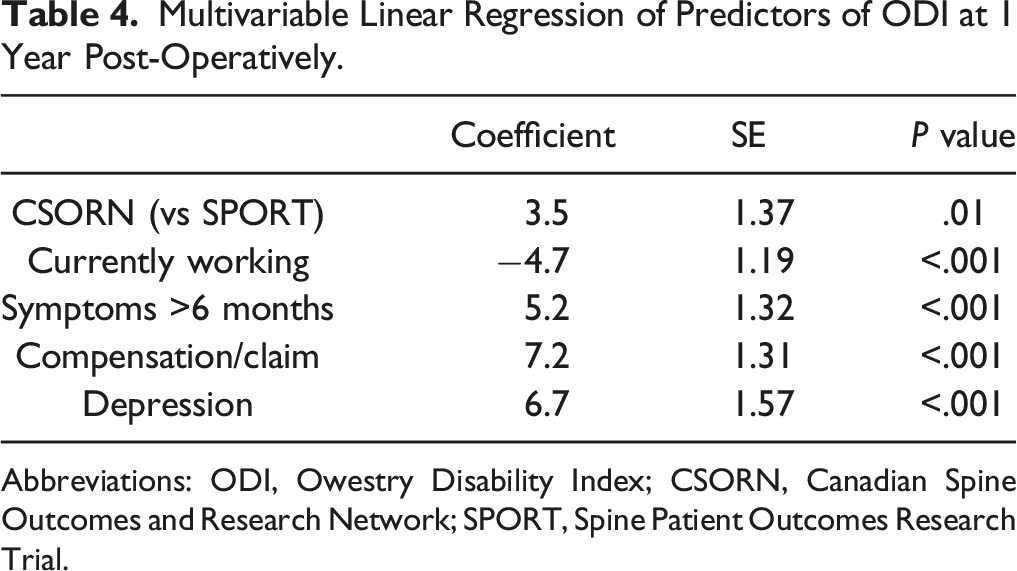
Abbreviations: ODI, Owestry Disability Index; CSORN, Canadian Spine Outcomes and Research Network; SPORT, Spine Patient Outcomes Research Trial.
Satisfaction
Patient Satisfaction.
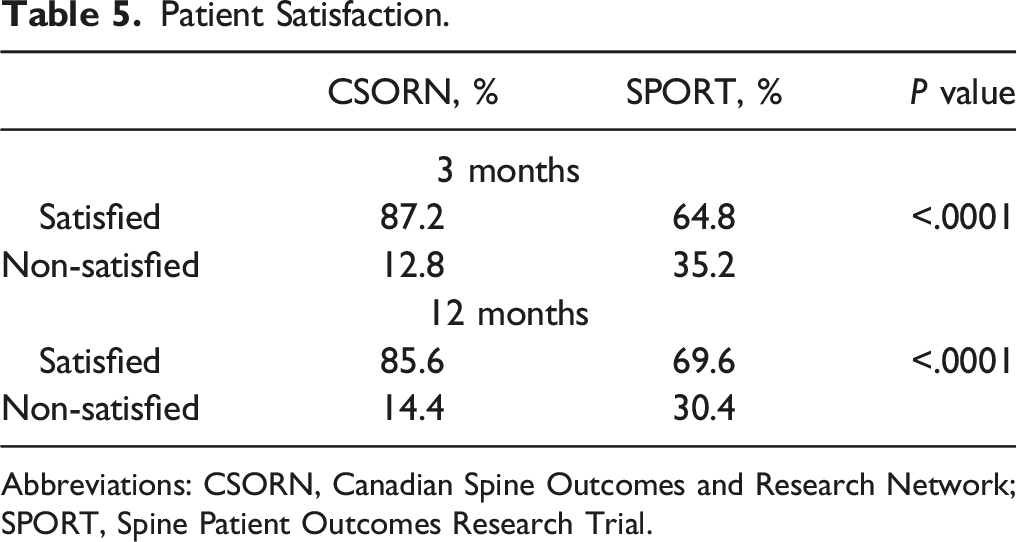
Abbreviations: CSORN, Canadian Spine Outcomes and Research Network; SPORT, Spine Patient Outcomes Research Trial.
Multivariable Logistic Regression of Predictors of Satisfaction at 1 Year Post-Operatively.
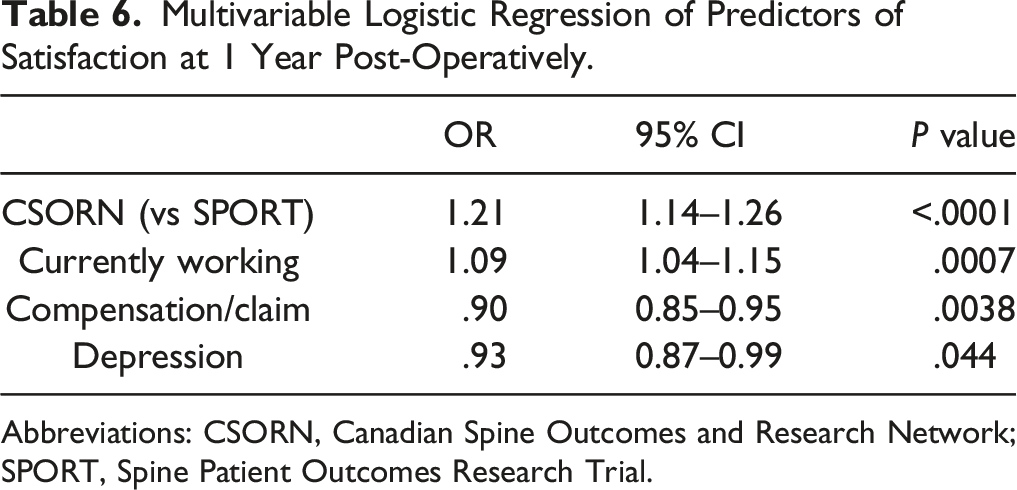
Abbreviations: CSORN, Canadian Spine Outcomes and Research Network; SPORT, Spine Patient Outcomes Research Trial.
Discussion
Our study has demonstrated some important differences in the post-operative outcome of lumbar disc surgery between the SPORT and CSORN cohorts. One may generalize that these cohorts are reflective of a difference between a multitier and single tier health care system. Data from the SPORT trials have been compared to the American College of Surgeons National Surgical Quality Improvement Program database and have been shown to be generalizable to the broader population. 15 Data from CSORN registry are derived from 16 tertiary spine centers in Canada, providing a reasonable representation of spinal surgery across the country in larger city-centers. Thus we feel that findings in both cohorts allow relatively broad comparisons between these patient populations.
The baseline PROs between the two cohorts in this study were similar, suggesting that observed outcome differences are not due to substantially different patient populations. There were differences at baseline on the ODI, PCS, and NRS leg, but these differences were small and unlikely to be clinically relevant. Significant post-operative improvements occurred for all PROs in the both cohorts at 3 months and 1 year. There were statistically significant differences between the CSORN and SPORT cohorts at 3 months and 1 year on PROs; however, these were small and unlikely to be of clinical impact. One exception may be differences between the two cohorts on the ODI. 16 Despite a higher initial baseline ODI, the SPORT cohort had significantly lower (better) ODI scores at 3 months and 1 year post-operatively (difference 12 and 8 points, respectively). Despite clinically and statistically significant improvements in both cohorts on the ODI, the CSORN cohort was independently associated with worse ODI scores on multivariable linear regression, as were an active compensation claim, symptoms greater than 6 months, and depression. It is possible that delays in specialist assessment and surgery may contribute to greater disability in the CSORN cohort. This is supported by the fact that the majority of SPORT patients were treated within 6 months of symptom onset (77%) compared to only 26% percent of CSORN patients. These delays in surgery for lumbar disc herniations may impact the extent to which patients can fully recover. 17 In contrast to the difference in PROs between cohorts, patients in the CSORN cohort had significantly higher rates of post-operative satisfaction post-operatively, and CSORN participation was an independent predictor of satisfaction 1 year after surgery for lumbar disc herniations, as was current employment. The presence of active worker’s compensation/medical-legal claims and depression were independent predictors of discontent at 1 year post-operatively.
There are several possible explanations for higher rates of satisfaction after lumbar disc surgery in Canada. While our study did not directly address patient expectations, previous work in a spinal surgery population demonstrated that unmet pre-operative expectations is associated with lower PROs.18,19 Patient expectations may differ between countries and standard PROs may not detect these differences. 20 In the United States, patients can access surgeons directly, and surgery is usually rapidly available if non-operative treatment fails. In contrast, Canadian patients require a referral from a physician to see a spine surgeon. The patient can wait to see the surgeon and then wait again until the surgeon has operative time available. 21 The cumulative effect can lead to lengthy delays.17,22 The dynamics of the health care system may drive patient expectations, which may impact satisfaction. A substantial portion of Canadian patients experienced symptoms for more than 2 years prior to surgery (35%) compared to only 3% in the SPORT cohort. Given the lengthy wait times for elective spine surgery in Canada there may be a self-selection bias towards satisfaction for those who endure the long wait while conversely the rapid access nature of surgery in the United States may lead to higher expectations.
We have previously compared the SPORT and CSORN cohorts for patients undergoing surgery for degenerative spondylolisthesis. 12 That study also showed the Canadian patients had higher rates of satisfaction. The rates at one year in the CSORN cohort were 88.2% for degenerative spondylolisthesis and 85.6% for lumbar disc herniation. Patients in the SPORT cohort had satisfaction rates of 71% for degenerative spondylolisthesis and 69% for lumbar disc herniation. Patients in both Canadian cohorts had a higher proportion with symptom durations greater than 6 months. For degenerative spondylolisthesis, it was 96% while for lumbar disc herniation it was 73%. This compares to 62% and 23%, respectively, in the SPORT cohorts. Despite longer symptom duration, Canadian patients consistently have higher rates of post-operative satisfaction. There are, in fact, lower rates of satisfaction in health care in America compared to several other countries. 23
The health care system is an important determinant of health.24,25 Meta-analyses 24 have demonstrated heterogeneity in health outcomes of between Canada and the United States with slightly more studies showing favorable outcomes for chronic conditions in Canada. Our findings of satisfaction for disc surgery are in line with the general satisfaction with physicians (90%) and hospital care (80%) across Canada. 26 The structure of the Canadian health care systems may contribute to the findings in our study as well as to differences between Canada and the United States noted in previous research.23,26 In Canada, a universal health care system, funded by the government, allows relative equity of resource distribution. In contrast, the United States has a multitier system, largely reliant on for-profit insurance companies to provide access to care. These differences have led to unique challenges, with ever-increasing and frequently unacceptable wait times for elective surgery in Canada and rising costs in the Unites States severely impacting individual patients and the system at large.
Compared to patients in the United States, patients in Canada face longer waits for surgery and have longer symptom duration. Nevertheless, they have higher rates of satisfaction after surgery for lumbar disc herniations and lumbar degenerative spondylolisthesis. There are, however, negative consequences to lengthy wait times for elective surgery. Recent work by Adogwa et al 27 shows that longer wait times are associated with significantly higher costs due to additional procedures, such as nerve root blocks, that may reduce symptoms but not treat the underlying problem. In addition to the increased financial burden to both patients and the health care system, increasing wait times are associated with less potential for improvement in PROs. 22 Together, increased costs and decreased PROs reduce the value of spine surgery. Given the rising costs of spine surgery, balancing the cost for spinal surgery with optimal patient outcomes is essential. 28
There are several limitations with the present study. First, our data may suggest that satisfaction after lumbar disc surgery is due to the system of health care delivery but we cannot establish a direct relationship. Second, available data analyzed the patient’s self-report of symptom duration, which can be biased by patient recall. Third, the SPORT trials were concluded a decade earlier than the data derived from CSORN, introducing a potential bias due to changes in practice although this is less likely in the lumbar disc surgery where there have been few significant technical advances. Furthermore, selection bias may be present as patients from the SPORT trial were enrolled in a randomized controlled trial and are likely more heavily scrutinized than in clinical practice. Despite this limitation both data sets are derived from multiple centers and comprise the highest quality available data from each respective country from which to make comparisons. Fourth, the presence of patient comorbidities or recurrent disc herniations was not available preventing a comparison between the cohorts and therefore adding an element of uncertainty. Last, we could not determine patient expectations prior to surgery and so could not examine how they might impact post-operative PROs.
Conclusion
Following surgery for lumbar disc herniation, patients in a universal health care system had significantly higher rates of satisfaction but worse disability scores on the ODI despite similar baseline demographic measures. Additionally, the universal health care system was an independent predictor of patient satisfaction one year after surgery. These data highlight the importance of the health care delivery context on PROs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.