
Abstract
Study Design:
Cross-sectional study.
Objectives:
To investigate the effects of pelvic compensation on standing balance in healthy volunteers.
Methods:
The 180 healthy volunteers were recruited at a basic health checkup. The inclusion criteria were: 1) age ≥ 65 years, 2) underwent a whole spine radiograph and stabilometry, 3) well-balanced standing posture with a sagittal vertical axis <50 mm, and 4) a visual analog scale of lower back pain of <20 mm. Based on the pelvic incidence (PI) and lumbar lordosis (LL) mismatch, subjects were divided into harmonious (PI–LL ≤ 10°) or unharmonious (PI–LL > 10°) groups.
Results:
Participants in the unharmonious group were significantly older compared with the harmonious group (70.2 ± 4.4 vs. 72.0 ± 4.6 years, P < .01). The PI minus LL values were −2.2° ± 7.5° and 16.6° ± 7.0° in the harmonious and unharmonious groups, respectively (P < .001). Anteroposterior LNG/TIME (average center of pressure sway speed) was significantly greater in the unharmonious group with both open and closed eyes (1.04 ± 0.38 cm/s vs. 1.25 ± 0.47 cm/s, P < .001 and 1.22 ± 0.54 cm/s vs. 1.58 ± 0.77 cm/s, P < .001, respectively). Lateral LNG/TIME was significantly greater in the unharmonious group only with closed eyes (1.24 ± 0.54 cm/s vs. 1.47 ± 0.79 cm/s, P = .03).
Conclusions:
Healthy elderly subjects with poor spinopelvic harmony had relatively unstable standing balance. The “cone of economy” was demonstrated, showing that unharmonious spinopelvic balance had a non-economic effect on standing.
Keywords
Introduction
The number of patients with adult spinal deformities requiring therapeutic interventions has been increasing recently. 1 Spinal deformities cause anterior trunk shifts, which lead to standing balance instability.2,3 Standing balance instability negatively impacts health-related quality of life. 1 In healthy subjects, the gravity line from the center of the auricle is located at the feet because humans have a balance cone (“cone of economy,” 4 CoE) with the feet as the fulcrum. 5 Spinal kyphosis causes the trunk to shift forward, 6 moving the center of gravity forward. Humans compensate for changes in spinal alignment by increasing posterior pelvic tilt and changing leg alignments to maintain the gravity line over the feet.7-10 However, this compensation requires a lot of energy,10,11 and the static standing equilibrium balance is worse.
The SRS–Schwab classification 12 is widely used to evaluate adult spinal deformities. A sagittal vertical axis (SVA) of less than 4 cm is considered non-pathologic and is consistent with the economic standing position within the concept of CoE. However, even within this non-pathologic range of SVA alignment, balance varies; some subjects maintain standing balance via spinopelvic compensation. Thus, even if the spine has a well-balanced static alignment, the standing balance may still be unstable in cases with spinopelvic compensation. Little is known about postural sway differences with or without spinopelvic compensation and the effects of spinopelvic compensation on the concept of CoE.
We hypothesized that standing stability is impaired in the presence of pelvic compensation, even in subjects with normal SVA. The aim of the current study was to investigate the effect of pelvic compensation on standing stability using whole spine radiographs and stabilometry (gravity sway test) in healthy volunteers. In addition, the concept of CoE was investigated with respect to spinopelvic compensation.
Materials and Methods
Study Population
This is a cross-sectional cohort study. The subjects were healthy volunteers who participated in a “basic health checkup” supported by the local government in 2018 and 2019. This checkup has been conducted annually in Yakumo, Hokkaido, Japan, for more than 30 years and is familiar to the local people.13-15 The checkup consists of voluntary orthopedic, physical, medical, and psychological examinations. The inclusion criteria in this study were as follows: 1) age 65 years or older and 2) underwent whole spine radiography and stabilometry. In addition, only subjects with a well-balanced standing posture indicated by an SVA of less than 50 mm were included. To eliminate the effects of back pain on standing posture, 16 only subjects with a visual analog scale (VAS) of <20 mm for lower back pain were included.
Over the 2-year study period, 1082 subjects participated in the checkup and 180 subjects (age range 65-87 years, mean 70.7 ± 4.5 years, 78 males and 102 females) met the criteria for inclusion in the study (Figure 1). None of the study participants had central or peripheral nervous system dysfunction that could affect the stabilometry measurement pattern. Subjects with a coronal curve greater than 30° were excluded from the study. Data concerning balance and spinal alignment parameters from whole spine radiographs was collected. This study was approved by the Nagoya University Human Research Ethics Committee. All participants provided written informed consent, and the study protocol was approved by the Institutional Review Board of our University Graduate School of Medicine. The study was carried out in accordance with the principles of the Declaration of Helsinki.
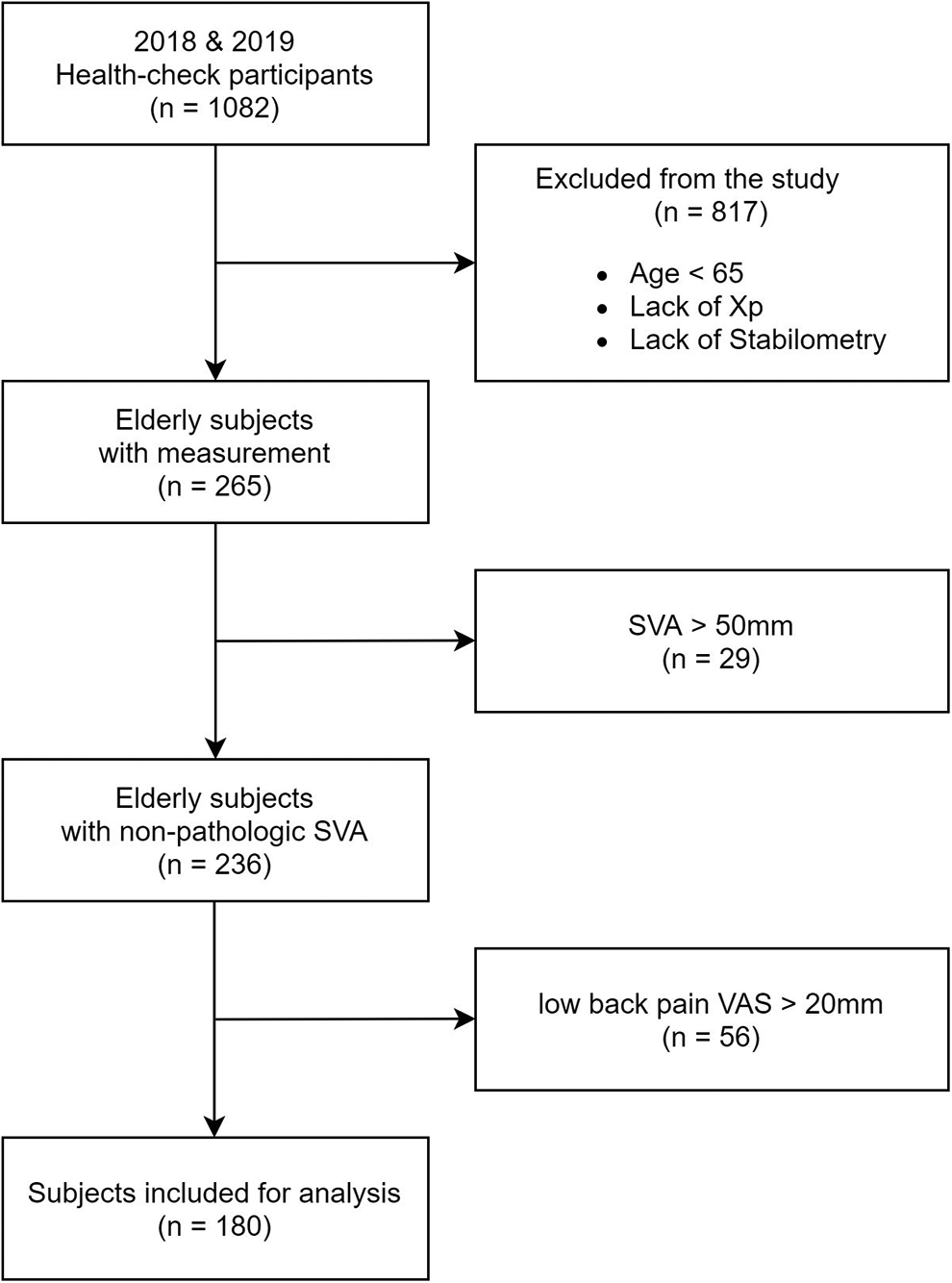
Flow diagram for subject selection.
X-Ray Evaluation
Whole spine radiographs were taken in a freestanding position with the fingers resting on the clavicles. 17 The measured parameters are shown in Figure 2. Spinopelvic parameters included lumbar lordosis (LL), thoracic kyphosis (TK), pelvic tilt (PT), and pelvic incidence (PI). Sagittal inclination parameters included SVA and the T1-pelvic angle (TPA). LL was defined as the angle between the T12-L5 vertebrae, and PI was defined as the angle between the center of the femoral head and the vertical line of the sacral superior margin. SVA was defined as the horizontal offset from the posterior-upper ridge of S1 to the vertebral body of C7. Based on the threshold between good and poor balance established in previous studies, an SVA <50 mm was considered a well-balanced standing posture. 12 In addition, Schwab et al 12 set a PI minus LL value of 10° or more as one criterion for poor balance in spinopelvic harmony. Thus, in this study, we divided the subjects into 2 groups defined by the PI minus LL value: harmonious (PI–LL ≤ 10°) or unharmonious (PI–LL >10°).
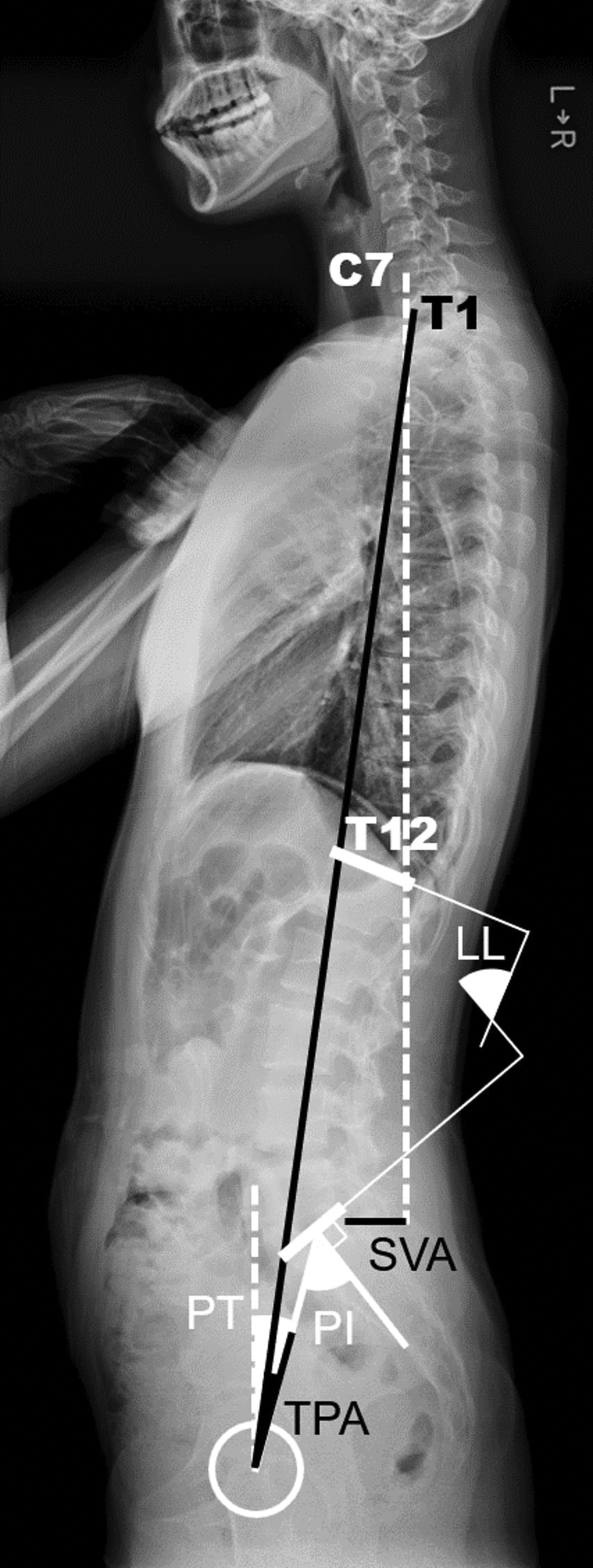
Whole spine X-ray evaluation. The dashed lines indicate vertical lines.
Stabilometry
Postural stability was measured using a G-620 stability force platform (Anima Corp., Tokyo, Japan) designed to evaluate the movement of the center of pressure (COP), indicating the center of gravity, in the horizontal plane using 3 vertical load sensors at the corners of an isosceles triangle. The measurement procedure is described in detail elsewhere.18,19 All participants were instructed to stand on the footplate without shoes and with their arms at their sides and feet close together (Figure 3). The stabilometry (gravity sway test) test was performed twice for 30 seconds each with eyes open or closed and the COP track signal was recorded on a microcomputer at a frequency of 20 Hz (Figure 4). 17 Seven parameters indicative of postural sway were extracted from the COP time series: 1) time track length (LNG/TIME), 2) lateral time track length (X LNG/TIME), 3) anteroposterior time track length (Y LNG/TIME), 4) envelope area (ENV AREA), 5) rectangular area (REC AREA), 6) lateral sway center deviation (DEVX), and 7) anteroposterior sway center deviation (DEVY). LNG/TIME represents the average value of the COP sway speed during the measurement time. The ENV AREA represents the inner area enclosed by the outermost outline of the COP track. The REC AREA represents the rectangular area enclosed by the maximum width of each axis. The sway center deviation is the deviation between the center of both soles and the center of gravity. Therefore, DEVX and DEVY represent the average position of COP from its origin.

Stabilometry at the basic health checkup. The test environment was set up so that no visual or auditory stimuli were applied to the subject. During the eye-opening test, the subject was instructed to gaze at a single point.
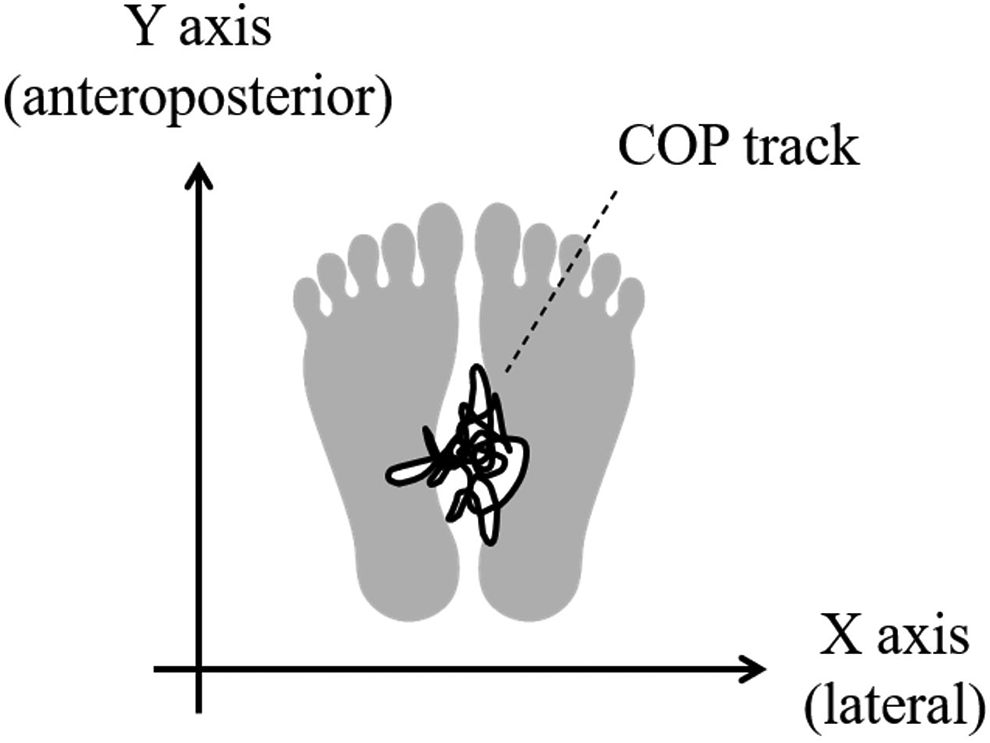
Schematic diagram of stabilometry. The gravity sway meter records the COP track.
Statistical Analysis
Data is presented as mean ± standard deviation. Fisher’s exact test was used for gender comparisons, and Wilcoxon’s rank-sum test was used for other comparisons. Statistical analyses were performed using R version 4.0.0 (http://www.R-project.org). A P < .05 was considered a significant difference.
Results
Table 1 shows the characteristics and X-ray parameters for the harmonious and unharmonious groups. Age was significantly higher in the unharmonious group compared to the age in the harmonious group (70.2 ± 4.4 vs. 72.0 ± 4.6 years, P < .01). No significant difference in the VAS value for lower back pain was observed. The unharmonious group had significantly greater PI (46.0° ± 9.9° vs. 55.9° ± 14.2°, P < .001), significantly smaller TK (26.9° ± 8.7° vs. 18.2° ± 8.2°, P < .001), significantly smaller LL (48.2° ± 10.0° vs. 39.3° ± 14.3°, P < .001), and significantly greater PT (14.3° ± 6.7° vs. 26.6° ± 7.4°, P < .001) compared with these parameters in the harmonious group. In addition, SVA (5.8 ± 25.1 vs. 13.3 ± 22.1 mm, P < .001) and TPA (8.9° ± 5.8° vs. 20.8° ± 6.5°, P < .001) were significantly greater in the unharmonious group compared with SVA and TPA in the harmonious group.
Subjects’ Backgrounds and X-Ray Evaluations.a
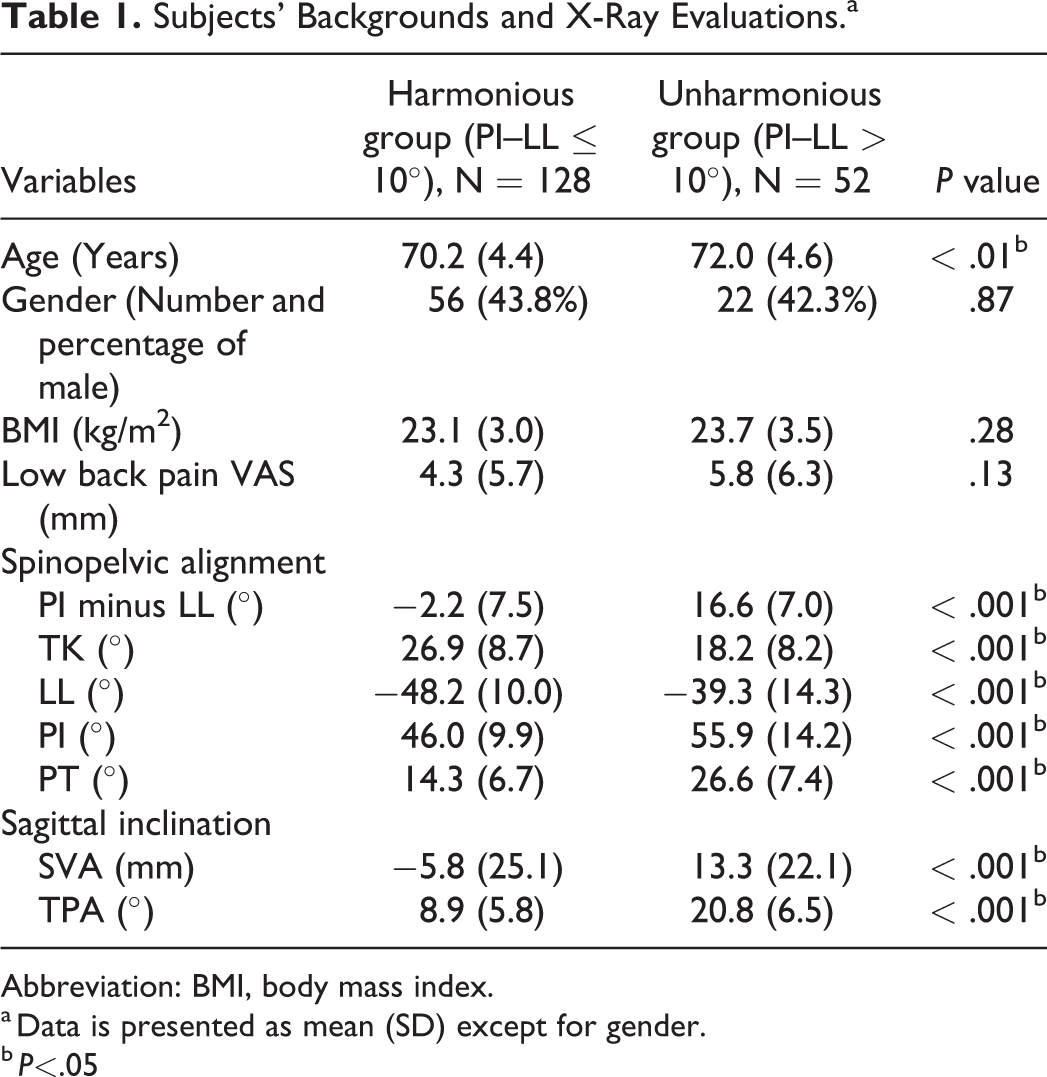
Abbreviation: BMI, body mass index.
a Data is presented as mean (SD) except for gender.
b P<.05
Table 2 shows the stabilometry parameters for the 2 groups measured with both opened and closed eyes. Y LNG/TIME (anteroposterior) was significantly greater in the unharmonious group with both opened and closed eyes compared with Y LNG/TIME in the harmonious group (1.04 ± 0.38 vs. 1.25 ± 0.47, P < .001 and 1.22 ± 0.54 vs. 1.58 ± 0.77, P < .001, respectively). However, X LNG/TIME (lateral) was only significantly greater in the unharmonious group with closed eyes (1.06 ± 0.40 vs. 1.18 ± 0.48, P = .09 and 1.24 ± 0.54 vs. 1.47 ± 0.79, P = .03, respectively). LNG/TIME, ENV AREA, and REC AREA were also all significantly greater in the unharmonious group with both open and closed eyes compared to these parameters in the harmonious group. No significant differences in DEVX and DEVY were detected between the 2 groups.
Measurements of Stabilometry.a
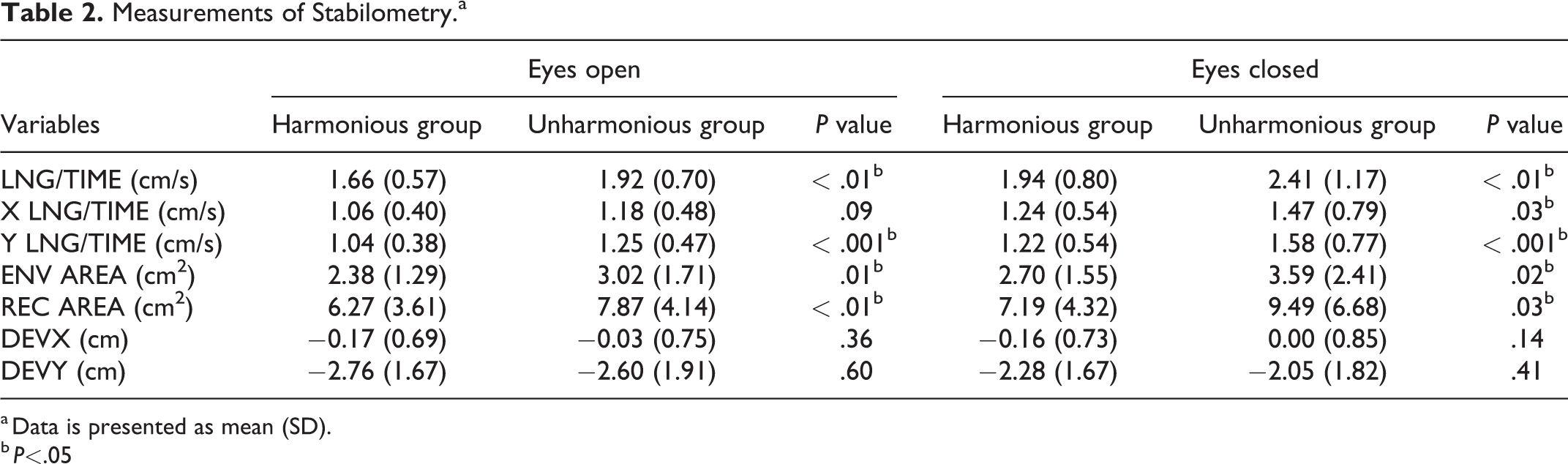
a Data is presented as mean (SD).
b P<.05
In summary, the COP track length was significantly longer in the unharmonious group than in the harmonious group and the differences in the anteroposterior direction were significant in both open and closed eye examinations. There was no difference in the center of gravity deviation between the 2 groups both in the anteroposterior and lateral directions.
Discussion
The current study compared standing stability between subjects with or without harmonious spinopelvic balance in the standing position. Although only subjects with well-postured SVA (<5 cm) were investigated, unharmonious spinopelvic balance was associated with significantly unstable standing balance in the anteroposterior direction measured with both opened and closed eye stabilometry. Even in subjects with well-postured SVA, compensatory effects cause unharmonious spinopelvic balance and the standing position becomes unstable. More energy is required to maintain an unstable standing position. Thus, these results support the concept of CoE and demonstrate that the compensatory effects of spinopelvic imbalance in healthy subjects require large amounts of energy, even in individuals with well-postured SVA.
Although significant progress in measuring and interpreting radiographic spinal alignment has been made in recent years, the relationship between spinal alignment, balance, and center of gravity sway and the clinical significance of these relationships are still poorly understood. Dubousset 4 proposed the concept of CoE to describe a standing posture that minimizes energy consumption. Haddas et al20,21 dynamically analyzed balance in adult degenerative scoliosis (ADS) to quantify CoE using 3D human motion capture. Haddas showed that “coronal” instability correlated with increasing SVA in ADS patients. In contrast, the present study consisted of only healthy subjects “without scoliosis.” In this case, PI–LL mismatch subjects increased the anteroposterior instability rather than the lateral instability. Our data indicate that anteroposterior destabilization appears first in elderly subjects with PI–LL mismatch without scoliosis.
Even though the majority of subjects in this study had normal stabilometry, the unharmonious group had significantly increased track length and area. Imaoka et al 22 investigated the standard values for stabilometry in the general population. In this study, the mean stabilometry values in the unharmonious group were within the mean + 1 SD of the values in the Imaoka data. 22 The elderly subjects in the unharmonious group had an increased track length, especially in the anteroposterior direction. Subjects with PI–LL mismatch maintained the standing posture with compensatory mechanisms like larger PT. In these subjects, the sagittal plane balance returned the anterior tilt of the trunk to the posterior direction, although the average SVA difference between harmonious and unharmonious groups was only 8 mm. This correction is reflected in the center of gravity sway in the anteroposterior direction.
Our data showed that PI–LL mismatch increases the “cone” size. Because DEVX and DEVY (deviation between the center of both soles and the center of gravity position) were not significantly different between the 2 groups, the center of gravity position was preserved in the unharmonious group. For example, patients with ADS have a forward tilt of the trunk and a forward shift of the center of gravity. 2 This forward shift of the sway center generally suggests an anterior tilt of the trunk due to decreased activity of the antigravity muscles. However, the subjects in this study did not show such a shift of the center point. Since the current study recruited only subjects with non-pathologic SVA values, these data indicate that the subjects in the present study had a larger cone in the unharmonious group compared with the cone in the harmonious group, even though the center of gravity (apex of the cone) was maintained in the standing position (Figure 5). Intuitively, maintaining balance with a relatively large cone requires more energy and is uneconomical. Thus, the unharmonious group subjects were able to maintain their posture; however, they might be expending more energy for compensation.
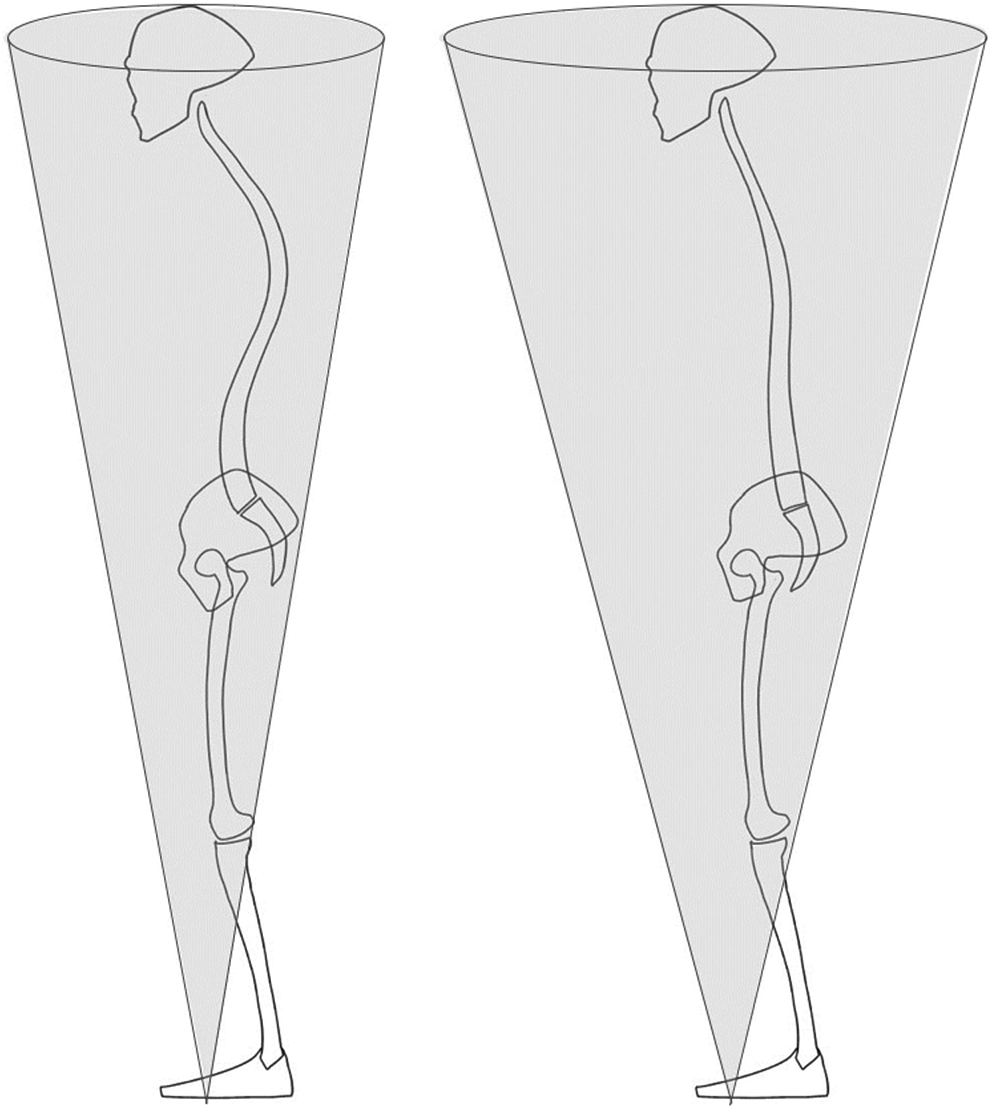
Schematic diagram of the balance cone in the harmonious and unharmonious groups. Subjects in the unharmonious group (right) were able to maintain the center of gravity point using compensation; however, their cones were larger than that of the harmonious group subjects (left).
In addition to static standing balance in the current study, PI–LL mismatch is associated with unstable walking balance. Gait disturbance is often seen in ASD due to fatigue and back pain. Gait velocity and stride were significantly worse in patients with ASD than in healthy volunteers, and increased trunk anteversion and left–right asymmetry were reported in ground reaction force during gait.23,24 With respect to correlation between gait and clinical outcomes in ASD, weak correlation between the preoperative gait velocity and SRS22r function score as well as moderate correlation between the postoperative SRS22r satisfaction and gait velocity were reported. Arima et al 23 showed that trunk forward tilt during walking was associated with PI–LL mismatch. The discrepancy between walking and standing was significantly great in cases with severe PI–LL mismatch (>40°); preoperative gait analysis was recommended in these cases due to the difficulty of recording the gait of all patients with ASD. It may be necessary to extend the upper instrumented vertebra (UIV) to the upper thoracic vertebrae in patients with large trunk forward shifts during walking. However, since there is no established method of surgical strategy based on the results of preoperative gait analysis, gait analysis might not be essential before surgery at this time. As evident from the standing instability observed in our present study, PI–LL mismatch is significantly associated with unstable body balance during standing and walking; thus, a good surgical correction is mandatory to achieve sufficient clinical outcome.
This study has several limitations. The number of cases was relatively small and the lower extremity alignment 25 was not measured. Future large-scale investigations regarding whole body alignment are necessary to validate the current results.
In conclusion, healthy elderly subjects with poor spinopelvic balance had relatively more unstable standing balance compared to those with well-balanced spinopelvic parameters. Furthermore, the increase in sway was more significant in the anteroposterior direction in subjects with poor spinopelvic balance, indicating the influence of compensatory effects in the sagittal plane. Thus, the current study demonstrates the concept of “cone of economy” and shows that unharmonious spinopelvic balance has a non-economic effect on static standing.
Footnotes
Acknowledgments
The authors are grateful to the staff of the Comprehensive Health Care Program held in Yakumo, Hokkaido, and to Ms. Aya Hemmi and Ms. Hiromi Mio at Nagoya University for their assistance throughout this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from JSPS KAKENHI (Grant no. 18K09102).