
Abstract
Study Design:
Survey.
Objectives:
To characterize national practices of and shortcomings surrounding intraoperative assessments of spinal alignment.
Methods:
Spine surgeons in the US were surveyed to analyze their experience with assessing spinal alignment intraoperatively.
Results:
108 US spine surgeons from 77 surgical centers with an average of 19.2
Conclusions:
Corrective surgery for spinal deformity is a complex procedure that requires a high level of expertise to perform safely. The majority of surveyed surgeons primarily rely on radiographs for intraoperative assessments of alignment. Despite the majority of surveyed surgical practices possessing navigation cameras, they are utilized only for a minority of spinal deformity cases. With the majority of surveyed surgeons reporting a need for improvement in technology to assess spinal alignment intraoperatively, 3 of the top design considerations should include workflow interruption, expense, and radiation exposure.
Keywords
Introduction
Spinal deformity affects both pediatric and adult patients, and occurs when the 3-dimensional curvature of the spine is imbalanced. Spinal deformity causes biomechanical inefficiency and can result in pain and reduced quality of life.1-4 Spinal alignment is assessed by a multitude of angular and distance-based measurements that have previously been correlated with disability and health-related quality of life scores, and in select patients, surgical correction of spinal alignment can offer pain relief and improved quality of life.1,5-8 However, these time-consuming and often invasive operations can be technically challenging, requiring a high degree of expertise to perform them safely.9,10 Complication rates associated with adult spinal deformity vary in the literature, but have been reported to be as high as 58% postoperatively, and include pseudoarthrosis, adjacent segment disease, and implant failure.11-15 Furthermore, approximately 62% of patients experience residual deformity postoperatively and up to 25% will need to undergo one or more revision surgery that, in addition to the negative impact on the patient, also results in compounding costs with decreased reimbursement.16-24 One of the key drivers for patients requiring revision operation is suboptimal postoperative alignment that deviates from preoperative goals. For example, Rothenfluh et al observed up to a 10-fold increased likelihood of revision surgeries for patients who experienced sagittal malalignment after undergoing lumbar fusion. 25 More specifically, postoperative malalignment has been shown to increase the likelihood of proximal junctional kyphosis, which occurs after up to 41% of spinal deformity surgical procedures, and—when severe enough—can lead to proximal junctional failure, which accounts for up to 17% of revision procedures.8,18,25-30
In an effort to decrease the rate of postoperative complications, a more recent area of focus in the field has deviated from a one-size-fits-all approach to alignment, and instead strives to establish patient-specific alignment parameters that incorporate variables such as patient demographics, disability scores, and frailty indices.31-33 As the field’s understanding of idealized alignment parameters continues to grow, so does the rate of these corrective procedures alongside the rapidly aging population in the US, with nearly a 3.5-fold increase in deformity operations over the course of just 7 years for patients over the age of 60 years.4,34,35
Limited research has focused on uncovering the surgeon’s perspective on the factors that contribute to the challenges of intraoperatively assessing spinal alignment and achieving preoperative goals by exploring the limitations of current technological offerings. This work presents the results of a national spine surgeon survey focused on the previously available technology for assessing spinal alignment perioperatively.
Methods
Utilizing Qualtrics software (Provo, Utah), a survey questionnaire (Supplement) was created and distributed to US spine surgeons in 2017. Following IRB approval, responses were gathered by either direct digital completion of the survey, or by inputting responses gathered by reading the questions to participants during in-person or virtual meetings.
Results
In total, 108 US-based spine surgeons from 77 different surgical practices across 29 states completed the survey. Respondents included 65 (60%) neurosurgeons and 43 (40%) orthopedic surgeons with an average of 19 years of spine surgical experience. The majority of participants had adult practices (73/108, 68%), 8 (7%) had pediatric practices, and 27 (25%) worked with both pediatric and adult patient populations. Additional demographics of survey participants are summarized in Table 1.
Participant Demographics.
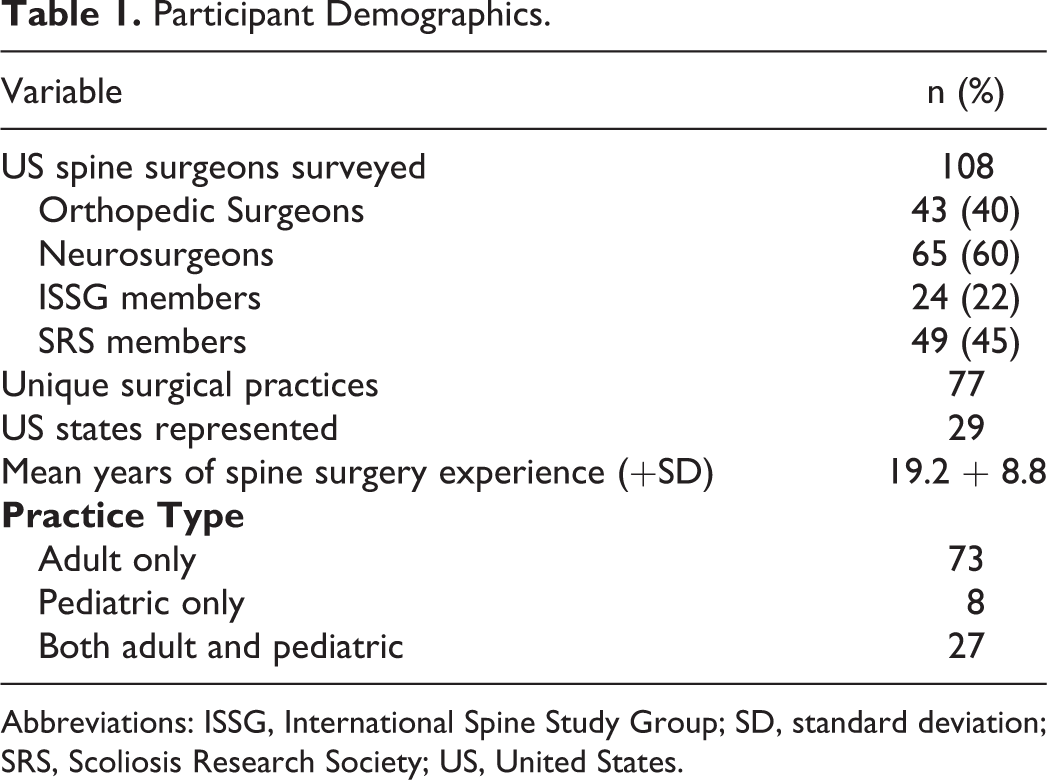
Abbreviations: ISSG, International Spine Study Group; SD, standard deviation; SRS, Scoliosis Research Society; US, United States.
With respect to preoperative assessment methods (Table 2), 88% of survey respondents (95/108) had used quantitative measurements of standing radiographs, and 41% (44/108) had prior experience with Surgimap. Those who used Surgimap on average reported only using it for approximately 40% of their deformity cases. Additional free text response included citing the use of flexion and extension radiographs for preoperative planning. With respect to intraoperative measures of alignment, the method most commonly used was C-arm or Spot radiographs (84%, 91/108), while only 40% (43/108) had previously used intraoperative full-length radiographs and only 20% (22/108) had utilized the T-bar. A few of the free text responses also indicated use of UNiD rods by Medicrea and intraoperative computed tomography (CT). 88% of respondents (93/106) reported that their surgical centers possessed a surgical navigation camera, and of the 68 (63%) who reported using surgical navigation systems for deformity cases, they did so on average for 40% of their deformity cases.
Utilization of Alignment Assessment Methods.
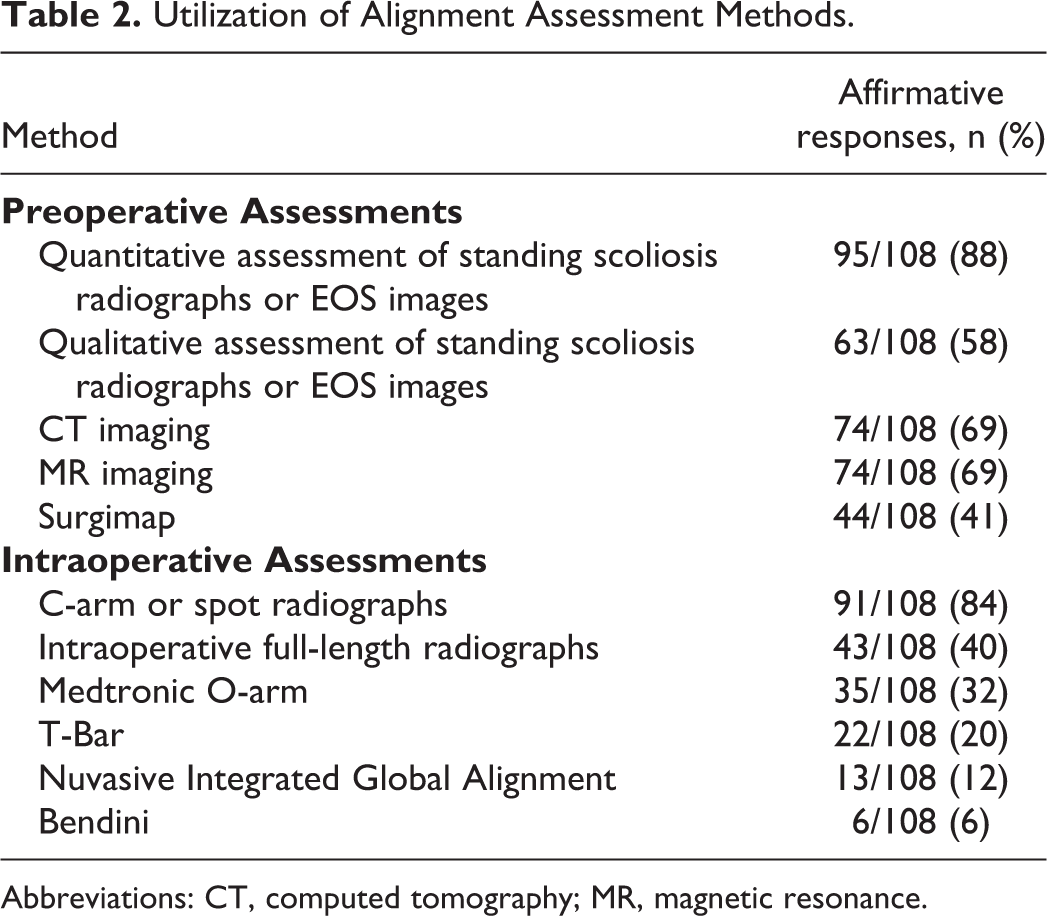
Abbreviations: CT, computed tomography; MR, magnetic resonance.
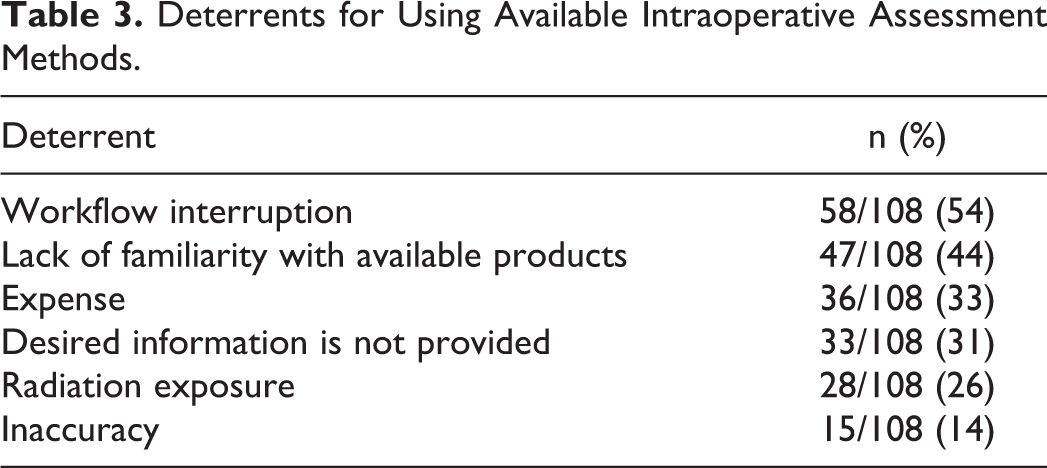
Table 3 summarizes deterrents for utilizing currently available methods for intraoperative assessment of spinal alignment. The most prominent deterrent, reported by 54% of respondents (58/108), was interruption to the surgical workflow. 33% (36/108) cited expense and 31% (33/108) reported that the quantified information they want to see is not provided by current technology. For 26% of respondents (28/108), added intraoperative radiation exposure was also a deterrent for radiation-based imaging assessment techniques. On average, respondents reported overall satisfaction with current methods of intraoperative assessment of sagittal and coronal alignment as a 5.8 and 6.1 out of 10, respectively. The factors for which unsatisfactory postoperative alignment results were most often attributed were general inability to assess alignment intraoperatively (average of 40% of cases) and inability to visualize critical landmarks for measurements intraoperatively (average of 31% of cases). Ultimately, 87% of respondents (82/94) reported a need for improvement in the current capabilities in making intraoperative assessments of spinal alignment.
Deterrents for Using Available Intraoperative Assessment Methods.
Discussion
Spinal deformity affects both adult and pediatric patients, and results in decreased quality of life. The number of surgical procedures to correct such deformity is growing rapidly alongside the aging population in the United States.2,4,34,35 These technically complex procedures require significant expertise and are associated with high rates of postoperative deformity, and a sizeable number of revision operations.9,10,16-19 In addition to improving quality of life, successful correction of spinal imbalance has been shown to reduce the need for costly revision procedures.19,22,23,25 Furthermore, increasing emphasis has been placed on determining patient-specific alignment goals based on an array of variables.31-33 In this light, improving the surgeon’s ability to accurately assess alignment intraoperatively and thereby titrate their deformity corrections to meet preoperative goals—stands to not only improve patients’ postoperative quality of life, but also to reduce known postoperative complications including proximal junctional kyphosis and the currently high rates of revision operations.
Our national survey confirmed that the ability to assess spinal alignment intraoperatively is a current clinical shortcoming in need of improvement. In addition, we ascertained the top factors that deter surgeons from using available technology to assess alignment intraoperatively. Survey respondents represented a diverse cross section of the country’s spine surgeons, including individuals trained in both Neurosurgery and Orthopedics. More than half of the participants were members of either the Scoliosis Research Society or International Spine Study Group. As expected, the most prominently used method to assess alignment both pre- and intraoperatively was radiography. As is often the case with obtaining intraoperative radiographs, workflow interruption was reported to be the most prominent deterrent of making intraoperative measurements. After lack of familiarity with available technology, the 3 main deterrents for using technology were expense, not being provided with the desired alignment information, and added radiation exposure. As expected, surgical navigation cameras were nearly ubiquitous, available at over 88% of centers, but only 63% of respondents reported using surgical navigation. Of those who did use these cameras, it was for an average of 40% of their deformity cases. Although this represents an increase from the 11% routine usage of surgical navigation reported in 2013 by Härtl et al, it is likely a more modest increase than it appears due to our survey respondents reporting only using navigation for a minority of their cases. 36 The primary reported factor responsible for unsatisfactory postoperative alignment results was the inability to assess alignment intraoperatively, and 87% of respondents ultimately reported the need for improvement in current capabilities of making intraoperative assessments of spinal alignment.
Supplemental Material
Supplemental Material, sj-tif-1-gsj-10.1177_21925682211037273 - Trends in Intraoperative Assessment of Spinal Alignment: A Survey of Spine Surgeons in the United States
Supplemental Material, sj-tif-1-gsj-10.1177_21925682211037273 for Trends in Intraoperative Assessment of Spinal Alignment: A Survey of Spine Surgeons in the United States by David M. Gullotti, Amir H. Soltanianzadeh, Saki Fujita, Miguel Inserni, Edward Ruppel, Nicholas G. Franconi, Corinna Zygourakis, Themistocles Protopsaltis, Sheng-Fu Larry Lo, Daniel M. Sciubba and Nicholas Theodore in Global Spine Journal
Footnotes
Authors’ Note
David M. Gullotti and Amir H. Soltanianzadeh contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Each author of this manuscript is affiliated with Spine Align, LLC, either as founders, employees, advisory board members, or consultants. The survey data was collected prior to the company’s incorporation.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.