
Abstract
Study design:
Systematic review and meta-analysis.
Objectives:
Cervical spine endoscopic discectomy and decompression have gained popularity in the last decade. This review aimed to shed light on the current outcomes of cervical spine endoscopic procedures for degenerative disc disease (DDD) and to calculate a pooled estimate of various outcome measures.
Methods:
We retrieved articles published in English related to endoscopic cervical spine procedures from 3 central databases from inception until September 2020. A subgroup analysis based on the anterior versus the posterior approach was performed.
Results:
Thirty-one articles fulfilled the eligibility criteria and included 1,410 patients. A successful outcome was observed in 91.3% (88.6-93.4%, P = 0.000). This percentage was lower for the anterior approach (89.6% [85.8-92.5%], P = 0.000) than for the posterior approach (94.2% [90.4-96.5%], P = 0.000). A higher percentage of poor outcomes was reported for the anterior approach (5.7% [3.2-10.1%], P = 0.000 vs. 2.3% [1-5.5%], P = 0.000 for the posterior approach). The overall complication rate was 7.2% (5.2-9.8%, P = 0.000). There was a slightly higher complication rate for the anterior approach (7.9% [4.5-13.3%], P = 0.000) than for the posterior approach (6.7% [4.4-10%], P = 0.000). The revision rate was 4.2% (2.6-6.8%, P = 0.000); and 4.2% (1.8-9.7%, P = 0.000) for the anterior approach and 4.00% (2.2-7.4%, P = 0.000) for the posterior approach.
Conclusions:
There is a higher success rate and lower complication rate with the posterior approach than with the anterior approach. However, high-quality randomized controlled trials are vital to evaluate the efficacy of these procedures.
Introduction
Degenerative disc disease (DDD) includes isolated neck pain, radiculopathy, myelopathy, or a combination of these conditions. 1 Neck pain due to DDD can affect up to 67% of people aged 50 years or older. 2 However, radiculopathy has a lower incidence than isolated neck pain. 1 It has been reported that the point prevalence of radiculopathy is 3.5/1000, with an annual incidence of 83/100,000. 1 Moreover, Radhakrishnan et al reported the incidence of radiculopathy as 107.3/100 000 in men and 63.5/100,000 in women, with the peak occurring in the fifth decade of life. 3 In addition, the incidence of hospitalization due to degenerative cervical myelopathy has been estimated to be 4.04/100,000. This is lower than the incidence of radiculopathy. 4
Most cases of isolated neck pain and radiculopathy improve with conservative measures, such as oral medications, physical therapy, and interventional pain management.1,5 Surgical intervention is usually reserved for cases of cervical myelopathy or failed conservative treatment.1,5,6 Surgical options include anterior cervical decompression with or without fusion or arthroplasty (ACDF/A) and posterior foraminotomy.1,5,6 Although ACDF/A provides a good outcome, potential complications include injury to the recurrent laryngeal nerve, postoperative dysphagia, adjacent level disease, perforation of the esophagus, hardware failure, and pseudoarthrosis. 5 Posterior foraminotomy may be an excellent option to prevent the aforementioned potential complications and reduce cost, as no implants are used. However, it carries a risk of kyphosis or loss of lordosis. 6 Therefore, the use of cervical endoscopic procedures to treat cervical radiculopathy secondary to DDD has become increasingly utilized in an attempt to achieve similar outcomes as open decompression while avoiding the complications associated with open surgery. 7
We aimed to perform a comprehensive review of all the available literature on cervical endoscopy for DDD and provide a quantitative summary estimate of the success rate and complications based on the type of approach. This analysis could provide guidance for spine surgeons when considering the adoption of this minimally invasive technique.
Materials and Methods
This study was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 8
Eligibility Criteria
The eligibility criteria included articles published in English concerning endoscopic procedures for the treatment of degenerative cervical pathologies, such as endoscopic discectomy and foraminotomy limited to the cervical spine. Articles published from 2003 (date of the first publication meeting the inclusion criteria) until September 2020 that had full text available for further analysis were included. In addition, a manual search and check of cross-references from the included articles were performed. Published studies dealing with standard open procedures (anterior cervical discectomy, corpectomy, fusion, and cervical arthroplasty), other minimally invasive procedures (minimally invasive instrumentation and laser ablation), other spine pathologies (tumor, infection, and trauma), and case reports were excluded.
Information Sources and Search Strategy
PubMed, Google Scholar, and Embase were used as information sources to retrieve all related articles. Search terms such as cervical spine, minimally invasive, discectomy, foraminotomy, and endoscopic procedures were used to perform the search. Titles and abstracts were screened to meet the eligibility criteria (Figure 1).
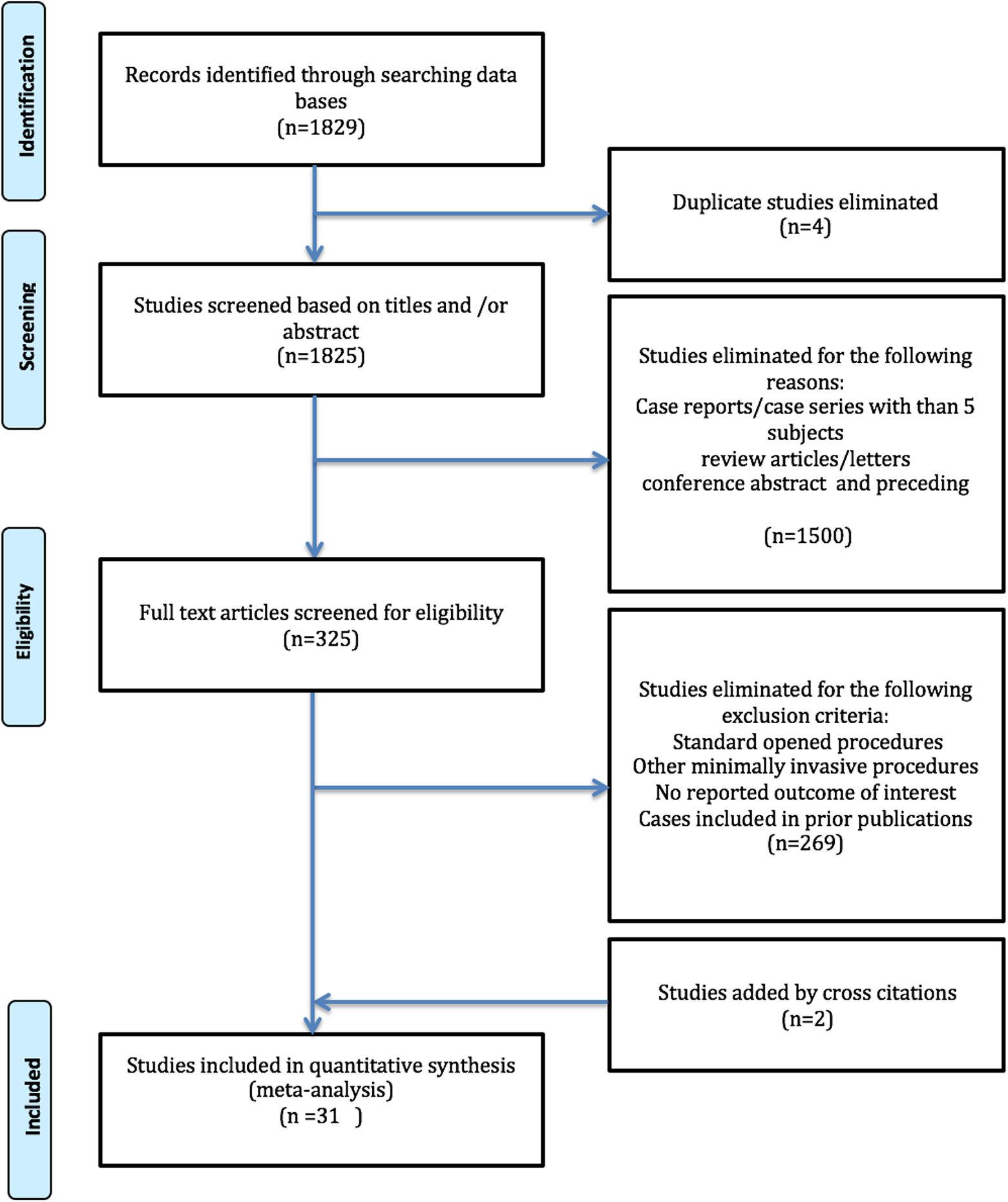
PRISMA flowchart of the search strategy illustrating the number of articles excluded at various stages.
Level of Evidence
The quality of the studies was evaluated by 2 independent reviewers using the Oxford Center of Evidence-Based Medicine (OCEBM) level of evidence scale. 9 Any disagreement was resolved by discussion.
Data Collection and Data Items
Data was recorded on an Excel spreadsheet using the following items to guide the collection process: journal, date of publication, sample size, study design, level of evidence, number of citations, and country. The perioperative variables included the type of procedure (diskectomy, foraminotomy, fusion), consistency of disc material (soft vs. hard), type of approach (anterior vs. posterior), means of estimated blood loss (EBL), operative time, hospital stay, postoperative analgesia use, rate of reoperation, and radiation exposure. The outcome variables were divided into clinical and radiological variables. The clinical variables included the pre- and postoperative visual analog scale (VAS) scores of the neck and arm and the pre- and postoperative neck disability index (NDI). The outcome-based modified Macnab, Hillebrand, or Odom criteria divided patients into excellent (no complaints, able to carry daily activity without complaint), good (intermittent discomfort, not significantly interfering with work), fair (subjective improvement; however, physical activity is limited considerably), and poor outcomes (no improvement or worse than preoperatively).10-12 A successful outcome was defined as the total number of patients with an excellent or good outcome. Complication and revision rates also were recorded.
Radiological data was extracted when available. When multiple points of outcome were reported, we used the score at the last follow-up. Cervical curvature measures such as the cervical angle (CA) are calculated using the tangential method between C2 and C7 in a neutral position. 6 The segmental angle (SA) was calculated using Cobb’s method in the operated segments. 6 The CA during flexion (CAF) and the CA during extension (CAE) were also included as radiologic outcome measures and were calculated the same as the CA. However, the position differed. 6 The cervical spine range of motion was also included. It was calculated by subtracting the CAE from CAF. 6 Likewise, the segmental range of motion was calculated by subtracting the segmental angle during extension (SAE) from the segmental angle during flexion (SAF). 6 To assess the cervical alignment, the C2 sagittal vertical axes (C2 SVA) and the T1 slope angle (T1 S CA) were used. 6 The C2 SVA is the extent between the C2 plumb line and the posterior corner of the C7 vertebra. The T1 S CA is the angle formed by a line drawn along the superior endplate of the T1 and a horizontal reference line. 13
Statistical Analysis
IMB SPSS version 23 was used for descriptive statistics to calculate the mean and frequency. Comprehensive meta-analysis software version 3 (CMA) was used for the weighted summary statistics for various outcome measures. We conducted a quantitative analysis by calculating the pooled mean difference for pre- and post-operative scores in the mean VAS neck, VAS arm, and NDI scores. None of the studies mentioned the correlation coeffect, so we used the Rosenthal conservative estimate of 0.7 to calculate the pooled estimates. A weighted percentage for the point estimates was used to calculate the 95% confidence interval for other outcomes. A P-value of < 0.05 was considered statistically significant for all measured outcomes.
Our pre-set hypothesis of heterogeneity mainly includes the type of approach (anterior or posterior). We used a random-effects model to account for heterogeneity among the studies. Further, we conducted a subgroup analysis based on the approach to account for some of the heterogeneity factors.
Heterogeneity among the studies was calculated using I2 statistics. We conducted a sensitivity analysis using the one-study-removed method to evaluate the stability of the results.
Results
Of the 1,829 articles identified through the database search, only 31 fulfilled the eligibility criteria (Table 1); a total of 1,410 patients were included. Not all studies mentioned all outcome measures of interest. Of the included studies, 76% (n = 22) were classified as having level III, 2 (6.5%) level II, and 7 (19.4%) level IV evidence. The predominant study designs of the included articles were a retrospective cohort comprising 71% (n = 22). Most of the studies were published between 2017-2019 (20 studies). However, the earliest publication on this topic was published in 2003. 14 More than 2/3 of the studies were published in the last 5 years (77.42%). A significant number of publications originated from China (41.93%, n = 13), followed by South Korea (25.8%, n = 8) and Germany (16.13%, n = 5). Table 1 summarizes the included studies.
Summary of the Included Studies.
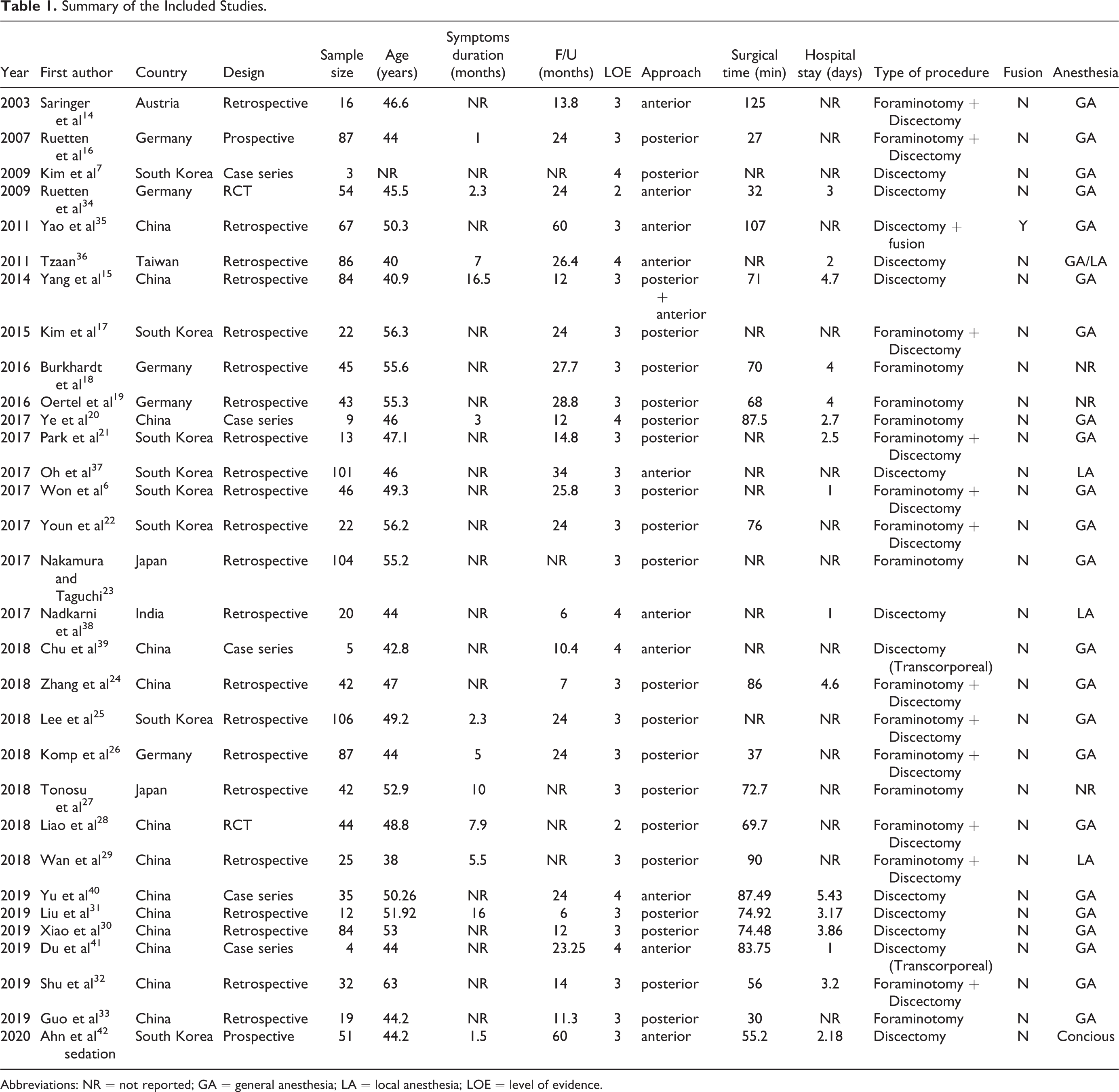
Abbreviations: NR = not reported; GA = general anesthesia; LA = local anesthesia; LOE = level of evidence.
Demographics
The mean age of the patients enrolled in the selected studies was 48.39 ± 5.72 years (38-63 years), and the mean follow-up time was 22 ± 13.63 months (6-60 months). Although symptom duration was not reported in a substantial proportion of the included articles, the summative result was 6.07 ± 6.06 months (1-16.5 months).
Operative Technique
One study included both anterior and posterior approaches (3.2%) 15 , 20 studies reported a posterior approach (64.5%),6,7,16-33 and 10 studies reported an anterior approach (32.3%).14,34-42 All studies involved foraminotomy or discectomy by removing a disk fragment. Only one study reported fusion with an anterior approach using an intervertebral cage and iliac crest graft. 35 Two studies documented anterior transcorporeal discectomy.39,41,43 The majority of the studies described the endoscopic procedure with general anesthesia. Only one study reported using local anesthesia for the posterior approach. 29
Three studies used local anesthesia or conscious sedation for the anterior approach.37,38,42 Tzaan used both local and general anesthesia for a cohort of 86 patients who underwent an anterior approach. 36 Not all studies used intraoperative neuromonitoring.
Perioperative Parameters
The mean EBL, operation time, and hospital stay were 5.6 ± 5.11 mL (0-10 mL), 69.35 ± 26.49 min (27-125 min), and 3.02 ± 1.37 days (1-5.43 days), respectively.
Postoperative analgesia use was reported only in one study, in which mean analgesic use was 9.14 days. No study reported the mean radiation exposure time. Only 5 studies reported the consistency of the resected disc material: soft in 4 studies (14%) and hard in one study (3.4%).
Outcome Assessment
VAS and NDI scores
Sixteen studies reported complete data on neck VAS scores. The difference in the mean neck VAS score was 4.38 (3.13-5.74, P = 0.000, I2 = 99.62). This indicated a high degree of heterogeneity. The mean reduction in VAS neck scores was 4.21 (1.60-6.81, P = 0.002) vs. 4.46 (2.73-6.19, P = 0.000) for the anterior vs. posterior approach. Fourteen studies reported complete data for the arm VAS score. This showed a higher degree of change compared to the neck VAS score. The mean difference was 5.80 (5.34-6.27, P = 0.000, I2 = 89.34) with a slightly better score for the anterior vs. posterior approach (6.13 [5.12-7.13], P = 0.000 vs. 5.69 [5.06-6.32], P = 0.000). Fourteen studies reported complete NDI score data. The mean difference in the score postoperatively compared to preoperatively was 24.14 (20.31-27.97, P = 0.000, I2 = 98.43). There was a higher mean score reduction with the anterior approach than with the posterior approach (27.14 [18.47-35.82] P = 0.000 vs. 23.32 [18.68-27.96], P = 0.000). Based on these data, it appears that there is a higher degree of reduction in the arm VAS scores compared to the neck VAS scores. This reduction was slightly better with the anterior approach. Neck disability scores improved more often with the anterior approach.
Clinical success
A successful outcome was defined as the total number of patients with excellent or good outcomes. This was reported in 14 studies. The summary estimate was 91.3% (88.6-93.4%, P = 0.000, I2 = 0.000). This percentage was lower for the anterior approach (89.6% [85.8-92.5%], P = 0.000 vs. the posterior approach (94.2% [90.4-96.5%], P = 0.000) (Figure 2).
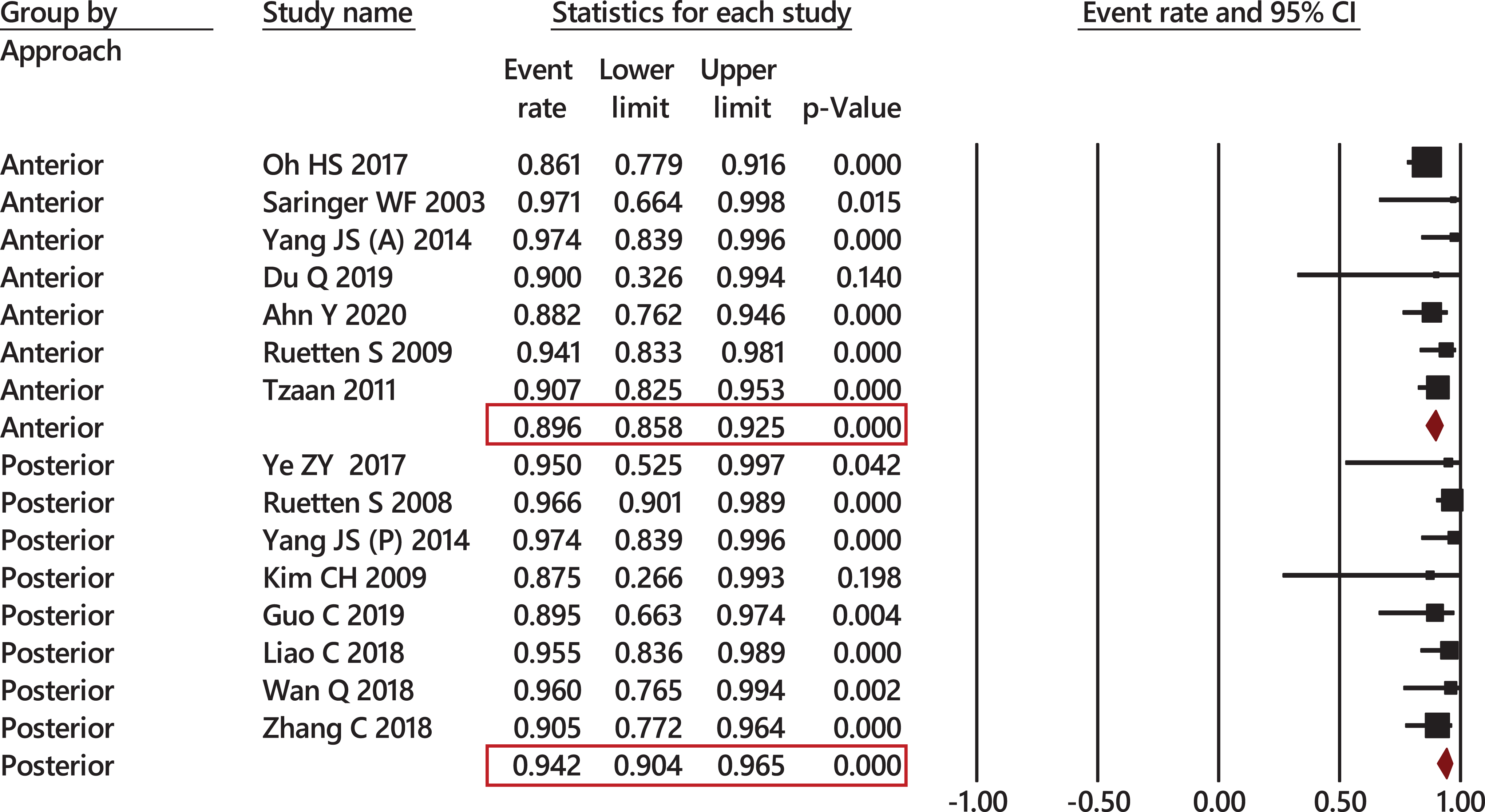
Forest plot showing rate of successful outcomes grouped by approach. The summary estimate was 91.3% (88.6-93.4%, P = 0.000, I2 = 0.000). This percentage was lower for the anterior approach (89.6% [85.8-92.5%], P = 0.000) compared to the posterior approach (94.2% [90.4-96.5%], P = 0.000).
Excellent outcomes were achieved in 72.5% (60.7-81.9%, P = 0.000, I2 = 85.17). There was a lower rate of excellent outcome for the anterior approach than for the posterior approach (61.1% [44.9-75.2%], P = 0.177, vs. 79.9% [67.8-88.3%], P = 0.000) (Figure 3).
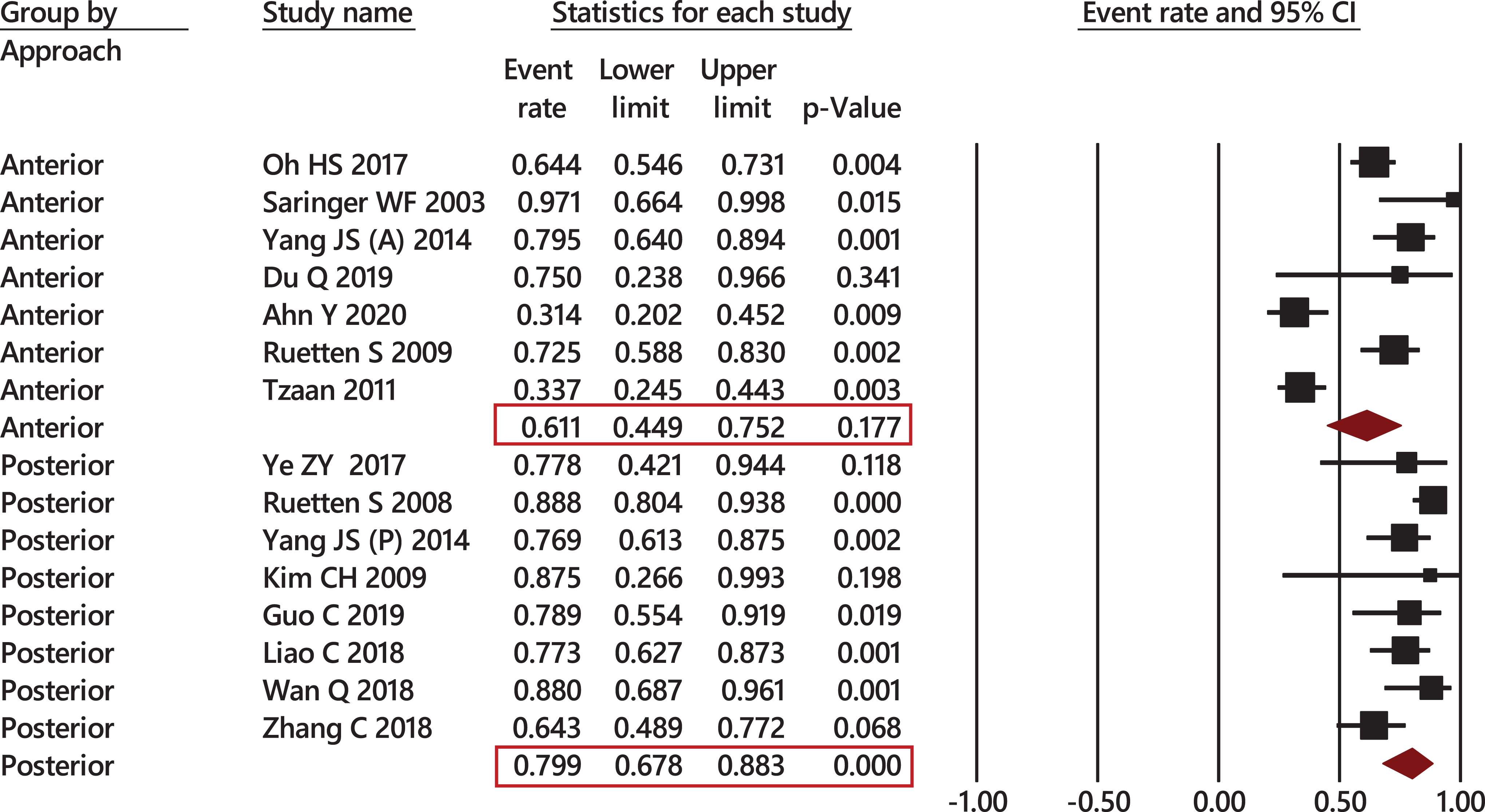
Forest plot showing rate of excellent outcomes grouped by approach. Excellent outcomes were achieved in 72.5% (60.7-81.9%, P = 0.000, I2 = 85.17) of cases. There was a lower success rate for the anterior approach compared to the posterior approach (61.1% [44.9-75.2%], P = 0.177 vs. 79.9% [67.8-88.3], P = 0.000).
A good outcome was seen in 21.4% (13.7-31.8%, P = 0.000, I2 = 83.21) of cases (anterior: 30.5% [18.4-46.1%], P = 0.016 vs. posterior: 15.3% [8.5%-26%], P = 0.000) (Figure 4). A fair outcome was seen in 5.8% (4.00-8.2%, P = 0.000, I2 = 0.00) of cases (anterior: 5.7% [3.6-9%], P = 0.000 vs. posterior: 5.8% [3.3-10%], P = 0.000
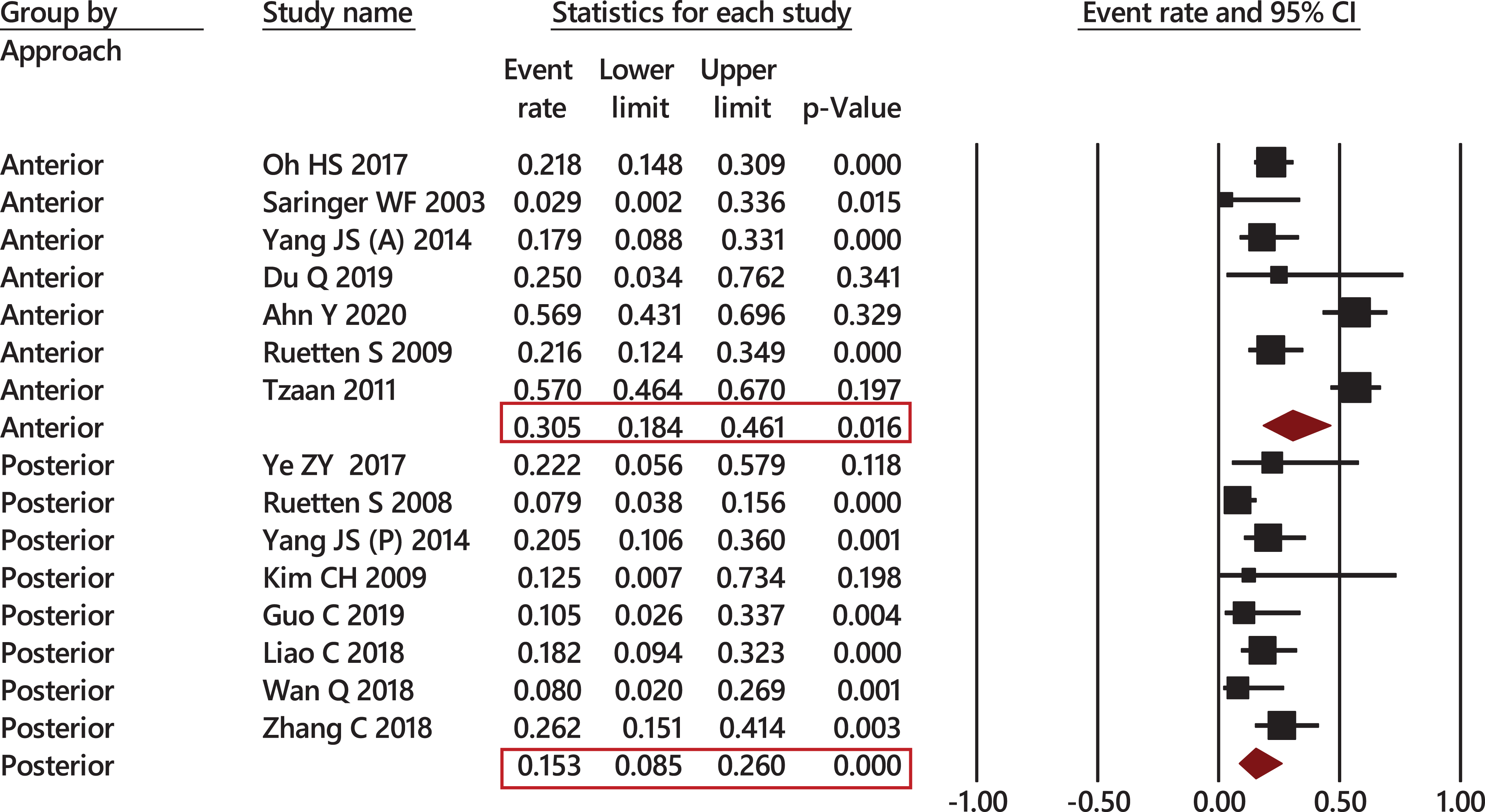
Forest plot showing rate of good outcomes grouped by the approach. Good outcomes were seen in 21.4% (13.7-31.8%, P = 0.000, I2 = 83.21) of cases, with 30.5% (18.4-46.1%, P = 0.016) in the anterior approach vs. 15.3% (8.5-26%, P = 0.000) in the posterior approach.
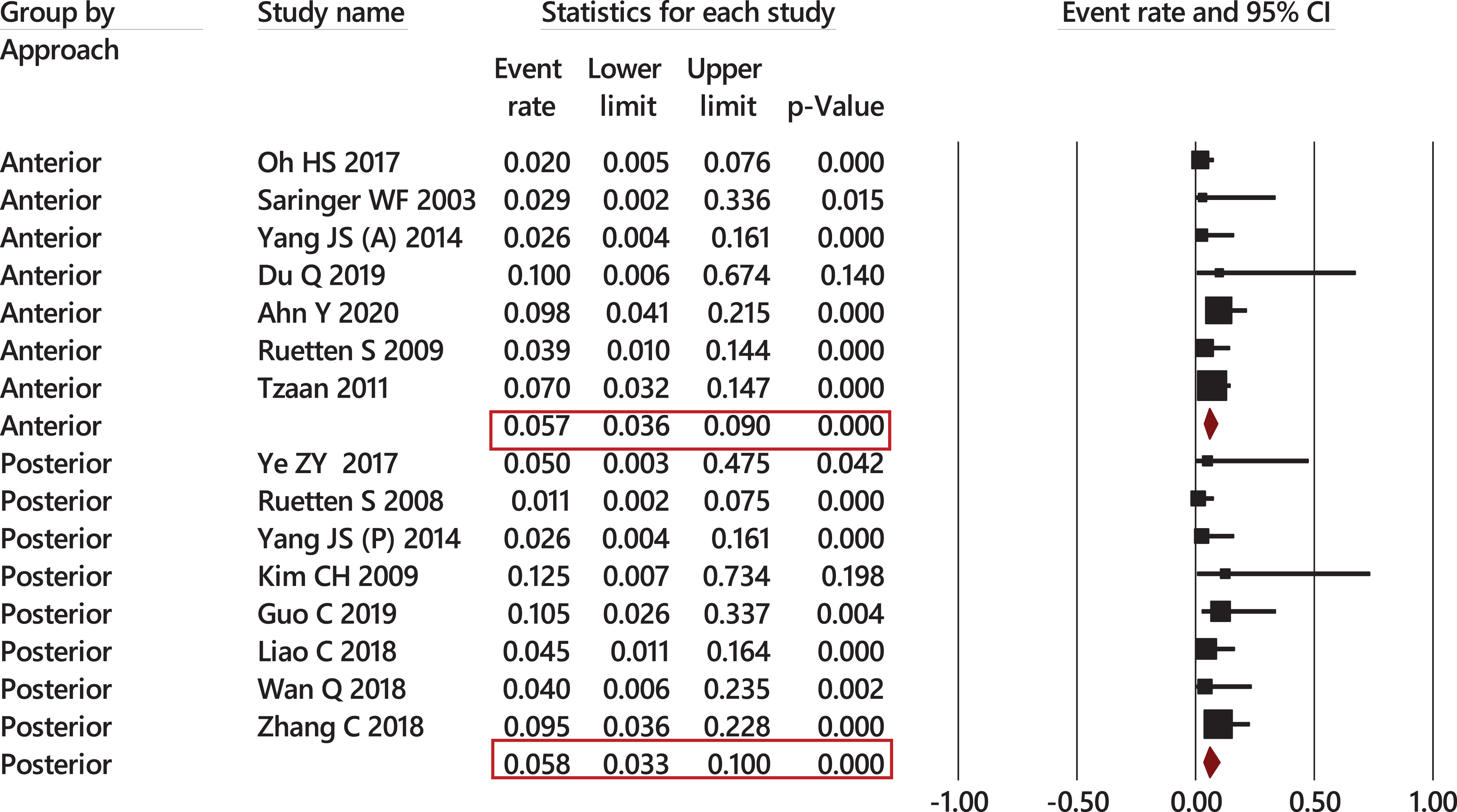
Forest plot showing rate of fair outcomes grouped by approach. A total of 5.8% (4.00-8.2%, P = 0.000, I2 = 0.00) of cases had fair outcomes (5.7% [3.6-9%], P = 0.000 in anterior approach vs. 5.8% [3.3-10%], P = 0.000 in posterior approach).
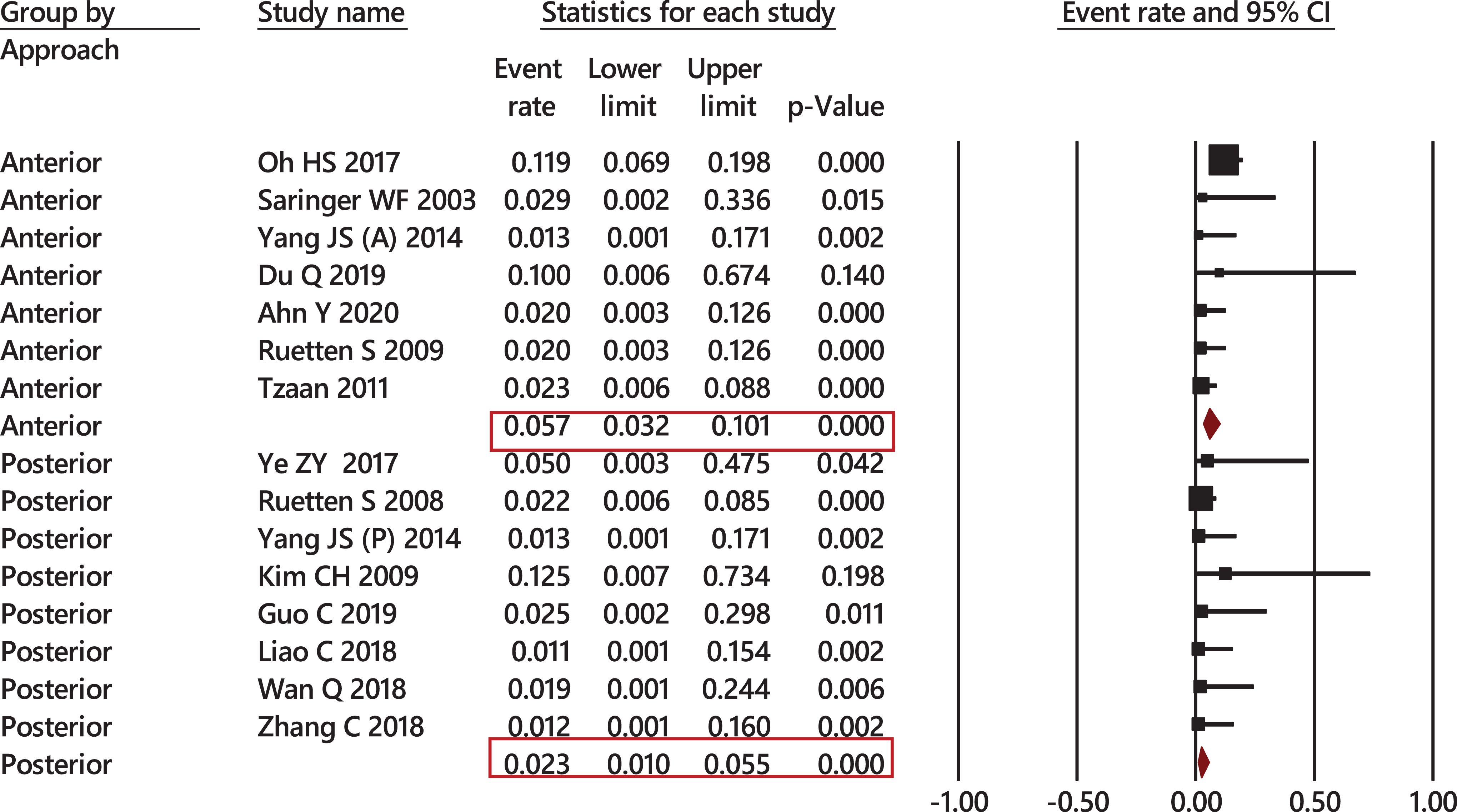
Forest plot showing rate of poor outcomes grouped by approach. Only 3.4% of cases had poor outcomes (1.9-6.2, P = 0.000, I2 = 28.2). A higher percentage of poor outcomes of 5.7% (3.2-10.1%, P = 0.000) was reported for the anterior approach compared to 2.3% (1-5.5%, P = 0.000) for the posterior approach.
Complication and revision rate
Twenty-nine studies reported complication rates. The overall complication rate was 7.2% (5.2-9.8%, P = 0.000, I2 = 49.4). There was a slightly higher complication rate for the anterior approach compared to the posterior approach (7.9% [4.5-13.3%)] P = 0.000 vs. 6.7% [4.4-10%], P = 0.000) (Figure 7).
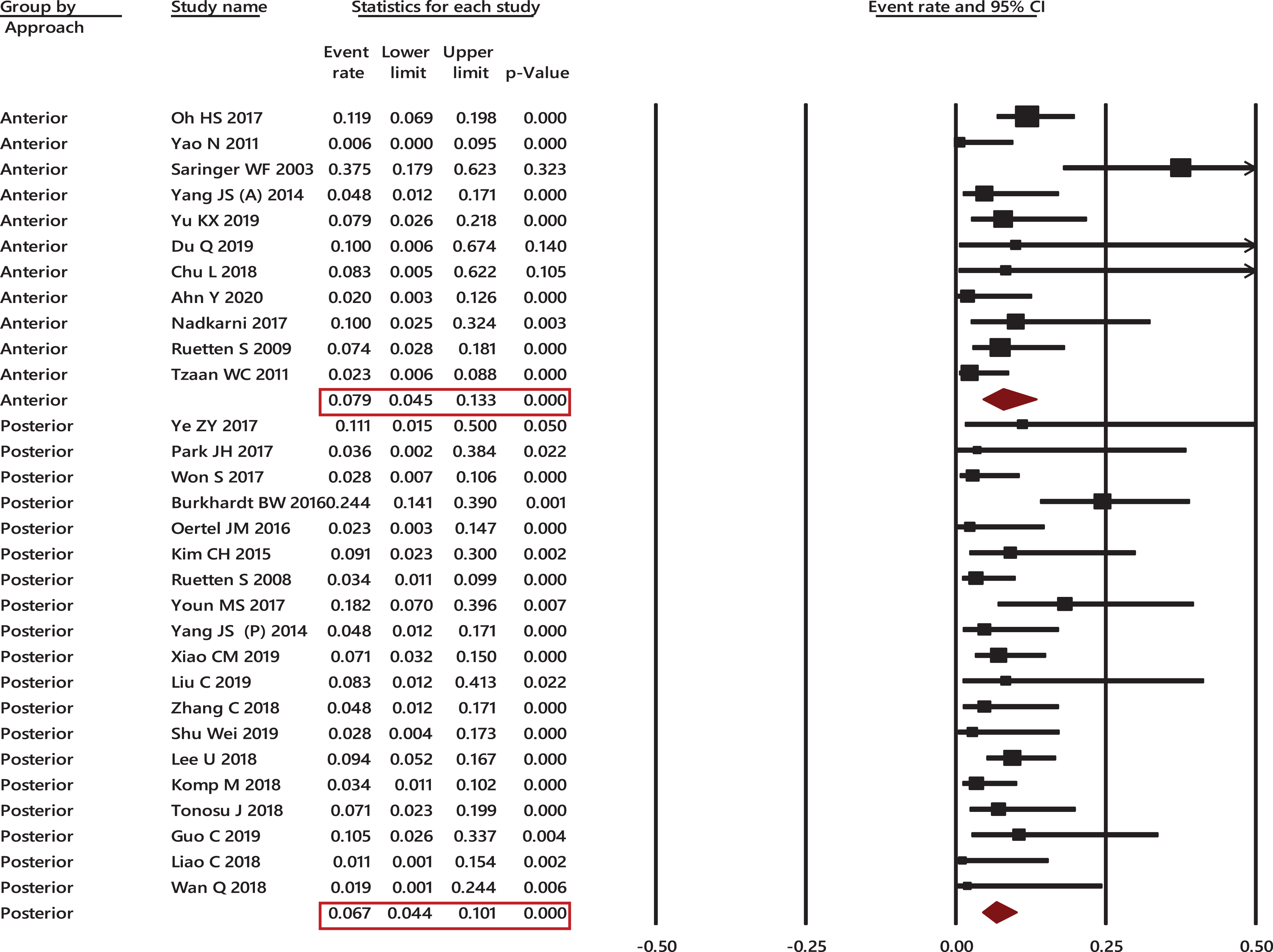
Forest plot showing rate of complication grouped by approach. The overall complication rate was 7.2% (5.2-9.8%, P = 0.000, I2 = 49.4), with a slightly higher complication rate for the anterior approach compared to the posterior (7.9% [4.5-13.3%], P = 0.000 vs. 6.7% [4.4%-10%], P = 0.000).
Twenty-three studies reported complete data regarding revision rates. The revision rate was 4.2% (2.6-6.8%, P = 000, I2 = 57.04). This indicated moderate heterogeneity. Almost a similar revision rate among the anterior vs. posterior approach was observed (4.2% [1.8-9.7%], P = 0.000 vs. 4.00% [2.2-7.4%], P = 0.000) (Figure 8).
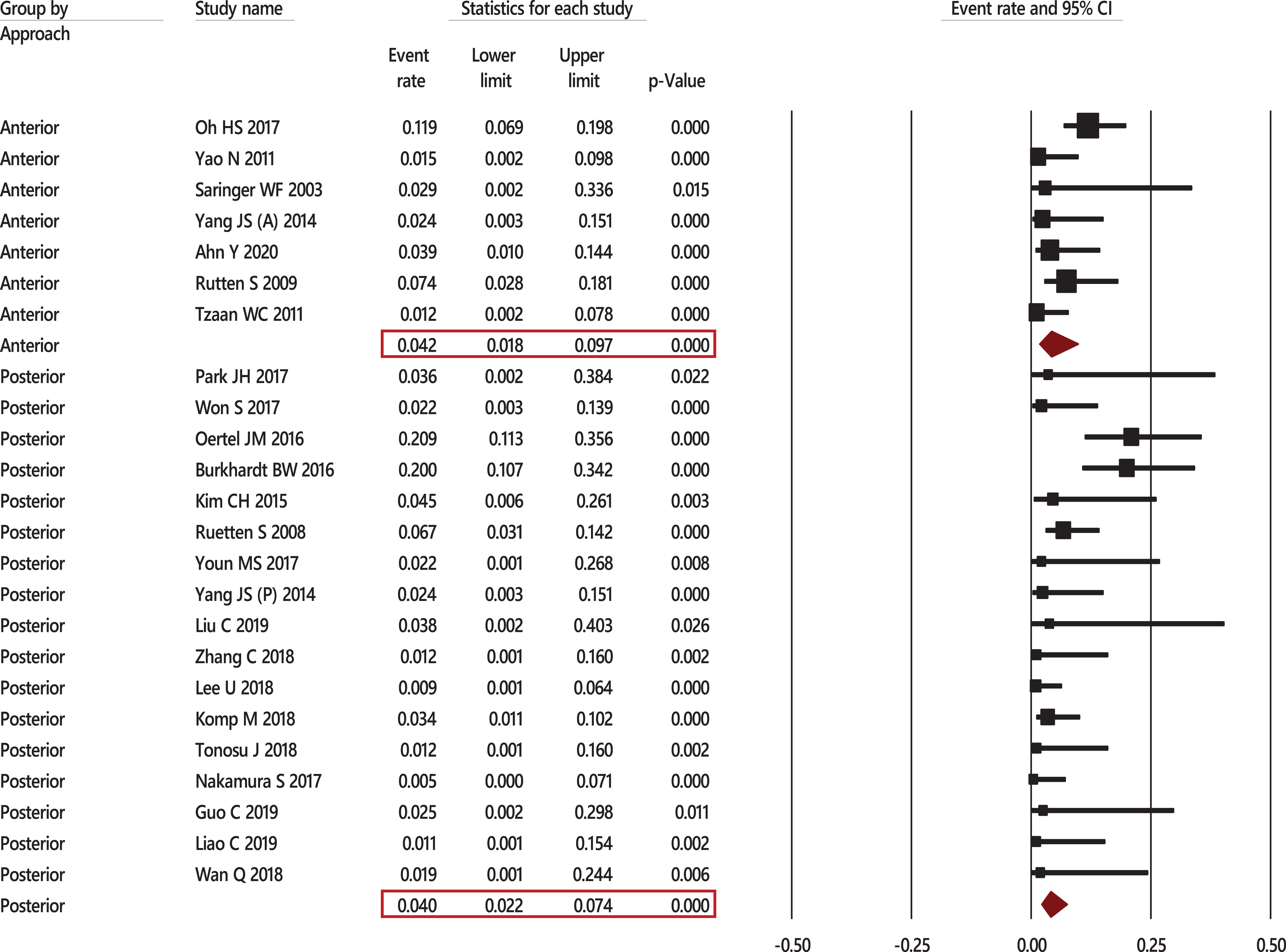
Forest plot showing rate of revision surgery grouped by approach. The revision rate was 4.2% (2.6-6.8%, P = 000, I2 = 57.04). This indicated moderate heterogeneity. There was an approximately similar revision rate among the anterior vs. the posterior approach (4.2% [1.8-9.7%], P = 0.000 vs. 4.00% [2.2-7.4%], P = 0.000).
We conducted a sensitivity analysis using the one-study-removed method for all outcome measures of interest and found no difference in the calculated outcomes. This indicated the strength of the findings.
Radiological Outcome
Only 10 studies reported radiological outcomes. The most commonly used parameters were CA, SA, and disk height. However, there was significant variation in reporting methods, and missing data made creating a pooled estimate unfeasible. Five studies reported changes in disk height, and 4 of these showed a reduction in disk height postoperatively. Only one study showed an increased disk height after the anterior approach. In this approach, patients underwent fusion in addition to discectomy. 35
Discussion
This meta-analysis included 1,140 patients. Most of the publications were reported in the past 5 years, which indicates an increased interest in minimally invasive spinal procedures. Our analysis aimed to summarize the current evidence, both qualitatively and quantitatively, for full endoscopic cervical foraminotomies or discectomies. Moreover, we performed a subgroup analysis concerning the anterior versus posterior approach to address certain heterogeneity factors.
We found that the length of stay was 3.02 ± 1.37 days (1-5.43 days), the means of the EBL was 5.6 ± 5.11 mL (0-10 mL), and the operative time was 69.35 ± 26.49 min (27-125). Ahn et al compared percutaneous cervical discectomy vs. ACDF. The endoscopy group showed statistically significantly shorter mean operative times, hospital stays, and return to work times (55.2 ± 18 min vs. 124.53 ± 35.68 min, 2.18 ± 1.16 days vs. 5.23 ± 2.93 days, and 3.14 ± 1.08 weeks vs. 10.84 ± 3.12 weeks) respectively. 42
Various techniques have been reported in the literature regarding minimally invasive cervical spine disease. In general, these approaches can be divided into anterior and posterior approaches. The anterior approach can be performed as fully endoscopic or as a hybrid (micro-endoscopic) technique. It can also be performed as a discectomy and fusion or as a transcorporeal approach to maintain the disk space integrity. A posterior approach could also be performed: as microscopic, full endoscopic, or microendoscopic. Both foraminotomy and discectomy could be achieved through this route. These procedures can be performed under local anesthesia or conscious sedation. Five studies selected this type of anesthesia.
Posterior Endoscopic Cervical Foraminotomy With or Without Discectomy (PECF ± D)
In our review, one study included both anterior and posterior approaches (3.2%). Most studies, 20 (64.5%), reported a posterior approach. This procedure has been recommended due to its beneficial outcome that preserves motion and provides postoperative spinal stability. 22 Furthermore, this type of procedure decreases the amount of tissue trauma and its’ consequences while achieving the outcome of standard procedures.19,44 However, only one study reported this approach using local anesthesia. 29 This is most likely due to the patient’s discomfort and difficulty maintaining a stable prone position without head fixation.
Indications for this procedure included neck pain with cervical radiculopathy in patients who failed at least 6 weeks of conservative management.6,22 Moreover, the endoscopic procedure requirements include cervical radiculopathy due to single-level affection with a laterally projecting disc that is documented by imaging with no history of cervical spine surgery at the index level.6,22 In the examined articles, the authors excluded cases with evident segmental instabilities or deformities, isolated neck pain that did not correlate with magnetic resonance imaging findings, multilevel disc herniation, previous surgery at the same target segment, suspected infection, and/or tumors.6,22
It was interesting to observe a higher success rate and lower complication rate in the posterior approach in comparison with the anterior approach. However, the indications are different for the anterior than for the posterior approach. This outcome measure is more robust than the mean difference in VAS and NDI scores in the pooled analysis. It showed only a slight difference in favor of the anterior approach. The pooled success rate for the posterior approach was 94.2% (90.4-96.5%, P = 0.000) with complication rates of 6.7% (4.4-10%, P = 0.000) and a revision rate of 4.00% (2.2-7.4%, P = 0.000).
A randomized controlled study carried out by Ruetten et al (to compare the full-endoscopic posterior foraminotomy technique with conventional ACDF in 100 patients) showed a significant improvement in postoperative pain (P < 0.001) in both groups. 44 In addition, they reported that the postoperative work disability was 19 days for the full-endoscopic posterior foraminotomy compared to 34 days for the ACDF group (P < 0.01). 44 Thus, full-endoscopic posterior foraminotomy has shown a reduced operating and postoperative rehabilitation time compared to ACDF. 44 However, the authors did not provide objective statistical values and comparison groups to examine this claim. Most authors of the included studies did not comment on the consistency of disc material, whether hard or soft, or if PECD would suffice for the treatment of herniated disc disease.
Anterior Endoscopic Cervical Discectomy
One study included both anterior and posterior approaches (3.2%), and only 10 studies (32.3%) reported an anterior approach. This procedure was indicated for patients with single-level myelopathy, radiculopathy, or myeloradiculopathy that failed conservative management.14,35,45 Patients with ossification of the posterior longitudinal ligament (OPLL) of a solitary type were also treated with this procedure.14,35,45 However, patients with apparent instabilities or deformities are poor candidates for the procedure, such as patients with infections or tumors. Such patients generally require open surgery.14,35,45
Only one study reported a fusion through the anterior approach, with the only complication being adjacent segment disease. 35 The remaining studies only documented foraminotomy or minimal removal of the herniated disk material. Two studies chose the trancorporeal approach.39,41,43
The endoscopic variant is considered a motion-preserving approach for the cervical spine. It protects the disc from surgical damage. It is better for lesions located behind the vertebral body compared to the anterior transdiscal approach. 17
Surgical indications were consistent across the studies. They included failed conservative therapy for at least 6 weeks, single-level soft herniation, and/or neurological findings that correlated with findings on imaging studies.39,41,43 Several surgical contraindications have been suggested, such as disc migration, disc herniation with foraminal stenosis, calcified herniated discs, obesity, previous surgery at the same level, and myelopathy.39,41,43
A successful outcome was obtained in 89.6% (85.8-92.5%, P = 0.000) of cases using the anterior approach, which is less than that seen with the posterior approach; additionally, anterior approach carried slightly higher complication rate compared to the posterior approach 7.9% (4.5-13.3%, P = 0.000). A similar revision rate among the anterior vs. posterior approach was 4.2% (1.8-9.7%, P = 0.000) vs. 4.00% (2.2-7.4%, P = 0.000).
Won et al found that using minimally invasive techniques would improve cervical curvature in patients with cervical lordosis less than 10. 6 Similarly, an increase in SL values following the posterior endoscopic approach indicated an improvement in lordosis.22,24 Although the mechanism is unknown, they speculated that the preoperative presence of hypo-lordosis or kyphosis in the selected patient population was functional rather than a structural change in response to radiculopathy. Thus, the alleviation of pain was the main reason for lordosis restoration. 6 In their study, Kim et al demonstrated that an SA of 1.45 (kyphotic SA) was a risk factor for a poor outcome. 17
Yang et al compared anterior and posterior approaches and found a mean height disk reduction of 1 mm with the anterior approach compared to 0.5 mm with the posterior approach (P < 0.005). No patient developed kyphosis or instability. 15 Disk height and vertebral body height reduction were observed by Yu et al at a follow-up of 2 years with no effect on the degree of kyphosis or instability. 40 Ruetters et al 2009 compared ACDF with the anterior endoscopic approach. Four patients in the ACDF group (8.35%) and 6 patients in the endoscopic group (11.8%) had increased kyphosis postoperatively, with a significant reduction in disk height in both groups. 34
Most of the included studies did not report radiographic outcome measures. These are vital in evaluating the efficacy of minimally invasive approaches.
In 2015, McAnany et al conducted a meta-analysis comparing open vs. minimally invasive (MIS) posterior cervical foraminotomy. 46 They included 3 MIS studies and 6 open studies and concluded that there was no significant difference in the outcome measured by the Odom criteria. Only one of the included studies was a fully endoscopic technique. A successful outcome was reported in 92.7% of patients in the open surgery group vs. 94.9% in the MIS group (P = 0.418). In our meta-analysis, which included only the endoscopic approach, we found similar findings. The clinical success rate was 91.3% (88.6-93.4%, P = 0.000). 34 This percentage was lower for the anterior approach (89.6% [85.8 92.5%], P = 0.000) than for the posterior approach (94.2% [90.4-96.5%], P = 0.000).
In this meta-analysis, the overall complication rate was 7.2% (5.2-9.8%, P = 0.000), with a slightly higher complication rate for the anterior approach (7.9% [4.5-13.3%], P = 0.000 vs. 6.7% [4.4%-10%], P = 0.000). This is a higher value; however, it includes all minor and major complications. Most of the reported complications were transient hypoesthesia or weakness.
One study of the anterior approach reported a major complication during exposure of the carotid artery resulting in arterial injury, dissection, and stroke. 36
In 2019, Tacconi reported a meta-analysis of hybrid endoscopic anterior cervical discectomy and fusion. Access was achieved microscopically to avoid access complications such as vascular injuries. 47 The success rate was 88%, the recurrence rate was 3%, and the revision rate was 5%. Access-related complications were <0.3%. Four of these studies included laser discectomy through anterior endoscopy. Thus, we did not include these in our analysis. 47
In our meta-analysis, the revision rate was 4.2% (2.6-6.8%, P = 0.00), with a similar rate for the anterior vs. posterior approach (4.2% [1.8-9.7%], P = 0.000 vs. 4.00% [2.2-7.4%], P = 0.000).
Overall, these data suggest that the minimally invasive endoscopic approach is a safe and effective procedure with a higher success rate for the posterior compared to the anterior approach. This is true when the outcome is measured as a clinical success based on the modified Macnab, Hilibrand, or Odom criteria. Moreover, the revision rate is generally the same regardless of the approach used. In our analysis, we also calculated the pooled analysis for the mean difference in VAS scores for arm and neck and neck disability scores. Our meta-analysis revealed a high degree of heterogeneity for VAS and NDI scores, even when grouped by approach. Both the anterior and posterior approaches showed significant improvement in VAS arm, VAS neck, and NDI scores, with the pooled analysis showing a higher degree of reduction in arm scores than the neck VAS scores. There was a slightly better reduction in scores with the anterior approach. However, this is a less robust outcome measure as it calculates the mean difference in scores rather than calculating each patient’s outcome separately.
Anterior approach might worsen degenerative changes because the approach violates healthy disk tissue, unlike the posterior approach, where mostly foraminotomy is sufficient to relieve the compression. One exception is using Transcorporeal discectomy to avoid violating healthy disk material. In one study that compared these 2 approaches, Yang et al observed more reduction in disk height with the anterior approach, contributing to the observed less favorable outcome with the anterior endoscopic approach compared to the posterior approach. 15
Limitations
The main limitation of this study is the level of evidece of the included studies and the inherent heterogeneity among the studies. There were differences in minor technical details (foraminotomy, discectomy, fusion, or no fusion), various centers experiences, and a different method of reporting outcomes with various follow-up points. Some follow-up points were only 6 months. This limits the long-term data, particularly for the recurrence and revision rates and late complications such as adjacent level degeneration. However, this meta-analysis provides the best available evidence for the use of endoscopy for treating cervical spine degenerative diseases. It includes a subgroup analysis for the anterior vs. posterior approach. High-quality randomized controlled trials are vital for evaluating this evolving technique. There were various factors of heterogeneity among the included studies. These factors might be difficult to offset even when conducting a subgroup analysis using a random effect model and conforming to the stability of the results with sensitivity analysis. Even though subgroup analysis addressed some of the heterogeneity factors, the result should be interpreted with caution as performing subgroup analysis might lower the power of analysis, lead to confounding and false-positive results.
Randomized controlled trials with an arm-to-arm comparison, rigorous selection criteria, long-term follow-up, unified outcome assessment tools, and detailed radiological outcome measures are essential to obtain an improved conclusion regarding the safety and efficacy of spinal endoscopy.
Conclusions
There is an expanded use among spine surgeons of cervical endoscopy for radicular pain due to herniated cervical disk. There is a higher success rate and lower complication rate associated with the posterior approach compared to the anterior approach. Both approaches showed significant improvement in the VAS arm, VAS neck, and NDI scores, and the revision rates were similar between the 2 approaches. There was a minor but significant reduction in disk height postoperatively. Whether this translates to a higher possibility of recurrence, deformity, and kyphosis is yet to be investigated. Our study is the first to present a meta-analysis addressing the outcomes of endoscopic techniques based on the type of approach. This meta-analysis demonstrates the safety of both anterior and posterior cervical endoscopy approaches for disk herniation. However, further studies are needed to compare these 2 techniques prospectively due to the heterogeneity and small sample size of the included studies.
Footnotes
Authors’ Note
All authors provided intellectual contribution to this manuscript. Soha A. Alomar, Saleh S. Baeesa, and Yazid Maghrabi wrote the manuscript. Soha A. Alomar and Yazid Maghrabi analyzed and interpreted the patient data. All authors reviewed, edited the document, and read and approved the final manuscript. This study doesn’t need ethical approval since it contains publically available date. No human subjects were included in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.