
Abstract
Study Design:
Retrospective cohort study.
Objective:
Preoperative anemia has been associated with an increased need for blood transfusions and postoperative complications. The effects of anemia on the outcomes of anterior cervical discectomy and fusion (ACDF) have not been explored. The present study aimed to evaluate the association between preoperative anemia and 30-day complications following ACDF surgery.
Methods:
Data from the American College of Surgeons National Surgical Quality Improvement Program (2005-2012) was used. Preoperative anemia was defined as hematocrit <39% for males and <36% for females. A bivariate analysis was performed on demographic and perioperative variables. Multivariable logistic regression models were employed, adjusting for patient variables, to identify independent risk factors for complications.
Results:
A total of 3500 patients were included of which 444 (12.7%) were anemic patients. Multivariate analysis was used to quantify the predictive power of anemia on key postoperative outcomes, while controlling for the other statistically significant. Preoperative anemia was found to be a statistically significant predictor of any complication (odds ratio [OR] = 1.853; 95% confidence interval [CI] = 1.17-2.934; P = .0086), pulmonary complications (OR = 3.269; 95% CI = 1.745-6.126; P = .0002), intraoperative blood transfusion (OR = 4.364; 95% CI = 1.48-12.866; P = 0.0076), return to operating theatre (OR = 2.655; 95% CI = 1.539-4.582; P = .0005), and length of hospital stay more than 5 days (OR = 2.151; 95% CI = 1.499-3.085; P < .0001).
Conclusion:
Preoperative anemia appears to be a significant predictor of perioperative complications, reoperation, and extended length of hospital stay in patients undergoing elective ACDF. Future studies should explore outcomes of treatment of preoperative anemia prior to surgery to determine the optimal management strategy.
Introduction
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed spinal procedures for patients with cervical radiculopathy and myelopathy. 1 -3 In appropriately selected patients, ACDF is a safe procedure with limited morbidity and can help relieve pain, neurological deficits, and improve functional outcomes. 4,5 In comparison to the posterior approach, the anterior approach provides the surgeon with direct exposure to the intervertebral discs to perform a direct decompression of anterior spinal pathology. 6 ACDF also minimizes surgical trauma to the paravertebral muscles that are required for stabilizing the spine, 7 -9 but can be associated with complications including dysphagia, hoarseness, hematoma, laryngeal nerve palsies, and neurological deficits. 10 -14
In the context of the increasing burden of health care costs for patients, hospitals, and third-party payers, there has been an increasing emphasis on identifying preoperative risk factors to optimize postoperative outcomes and reduce hospital readmissions and complications following ACDF surgery. One factor known to influence the outcomes of surgery is anemia, which is a common condition that becomes more prevalent with increasing age. Preoperative anemia has been associated with an increased need for blood transfusions and postoperative complications in various surgical procedures, including cardiac and spinal procedures. 15 -17 Spine surgery often requires blood transfusions due to the potential for blood loss, with more transfusions being associated with increased morbidity, 18,19 although ACDF is a procedure that uses a muscle-sparing approach and general low rates of blood loss. 20 There has also been previous reports suggesting that preoperative anemia is associated with prolonged hospital stays, increased postoperative complications, and 30-day mortality in some elective spinal procedures. 21 However, the effects of anemia on the perioperative outcomes of ACDF have not been specifically explored. Thus, the present study aimed to evaluate the association between preoperative anemia and 30-day complications following ACDF surgery.
Methods
Patient Selection and Data Collection
Patient data collected in the period from 2005 to 2012 for the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database was used for the present study. The methodology for definition and collection of variables in the ACS-NSQIP database has been outlined previously. 5,22 -24 Inclusion criteria for adult surgical cases were identified based on the Current Procedural Terminology (CPT) codes for elective ACDF (CPT codes: 22551, 22554, and 63075). Exclusion criteria of the present study included those who underwent spinal deformity surgery, underweight (body mass index [BMI] < 18.5 kg/m2), dependent on ventilator, disseminated cancer, radiotherapy for malignancy within 90 days before operation, pregnancy, tumors of the central nervous system, chemotherapy for malignancy within 30 days before operation, emergency operations, preoperative systemic sepsis, nonelective surgery, acute renal failure, combined approaches, posterior approach (CPT: 22600), and patients with missing preoperative data. Patients were divided into 2 groups and compared: patients who had perioperative anemia versus those with no anemia. Preoperative anemia was defined as hematocrit <39% for males and <36% for females, as previously described. 25
Explanatory and Control Variables
Recorded patient characteristics were classified into the following groups: baseline demographics, preoperative medical comorbidities, operative variables, and morbidity. Patient demographics included age, gender, race (white, black, Hispanic, other), outpatient status, obesity status based on BMI, American Society of Anesthesiologists (ASA) score, diabetes, smoker, alcohol use, dyspnea, and functional dependence prior to surgery. Comorbidities included pulmonary comorbidity, cardiac morbidity, peripheral vascular disease, neuromuscular injury, stroke, steroid use, recent weight loss, and bleeding disorder. Preoperative laboratory values included albumin, hematocrit, partial thromboplastin time (PTT), and international normalized ratio. Multilevel fusions and operative time >4 hours were also reported.
A cardiac comorbidity was defined as a history of congestive heart failure (within 30 days before admission), myocardial infarction (within 6 months before admission), percutaneous coronary intervention, cardiac surgery, angina (within 1 month before admission), or use of hypertensive medication. A pulmonary comorbidity was defined as history of severe chronic obstructive pulmonary disease or current pneumonia. Peripheral vascular disease was defined as a history of revascularization or amputation for peripheral vascular conditions and rest pain. Smoking history (current smoker within 1 year) and chronic steroid use (regular use within 30 days before admission) were also assessed. Morbid obesity was defined as a BMI of ≥40 kg/m2.
Outcomes
The study outcomes included any complication, death, pulmonary, renal, central nervous system complications, peripheral nerve injury, cardiac complication, thromboembolism, sepsis/septic shock, intra-/postoperative blood transfusion, urinary tract infections, wound complications, and graft/flap failures. Other outcomes included return to operating room, unplanned reoperation (based on data from 2011-2012), unplanned readmission (based on data from 2011-2012), and length of stay (LOS) >5 days.
Statistical Analysis
A bivariate analysis was performed on patient demographic, preoperative, intraoperative, and postoperative characteristics using Pearson’s χ2 test. Fischer’s exact test was used where appropriate. Variables with a P < .2 in the univariate analysis were carried forward into the multivariable analysis. Multivariable logistic regression models were employed, adjusting for patient demographic, preoperative, and intraoperative variables, to identify independent risk factors for any complications, pulmonary complications, intraoperative/postoperative transfusions, return to operating room, and 30-day readmissions. Both regression models utilized a stepwise entry and removal criteria, set to a significance level of .05. SAS Studio Version 3.4 (SAS Institute Inc, Cary, NC) was used for all statistical analysis.
Results
Patient Demographics and Clinical Characteristics
A total of 3500 patients were included in this study and consisted of 444 (12.7%) anemic patients. There was no statistically significant difference between the nonanemic and anemic groups with regard to gender (female: 50.03% vs 52.93%; male: 49.97% vs 47.07%; P = .2542). There was also no significant difference in obesity (45.9% vs 40.99%; P = .0517), alcohol use (3.14% vs 3.38%; P = .79), or dyspnea (6.9% vs 7.43%; P = .6831). However, ASA score ≥3 (35.57% vs 52.7%; P < .0001), diabetes (13.61% vs 26.35%; P < .0001), and dependent functional status prior to surgery (1.9% vs 7.21%; P < .0001) were significantly greater in the anemic patient group. Smoking (34.85% vs 23.2%; P < .0001) was greater in the nonanemic group (Table 1).
Univariate Analysis of Demographics and Clinical Characteristics Comparing Those With and Without Preoperative Anemia.
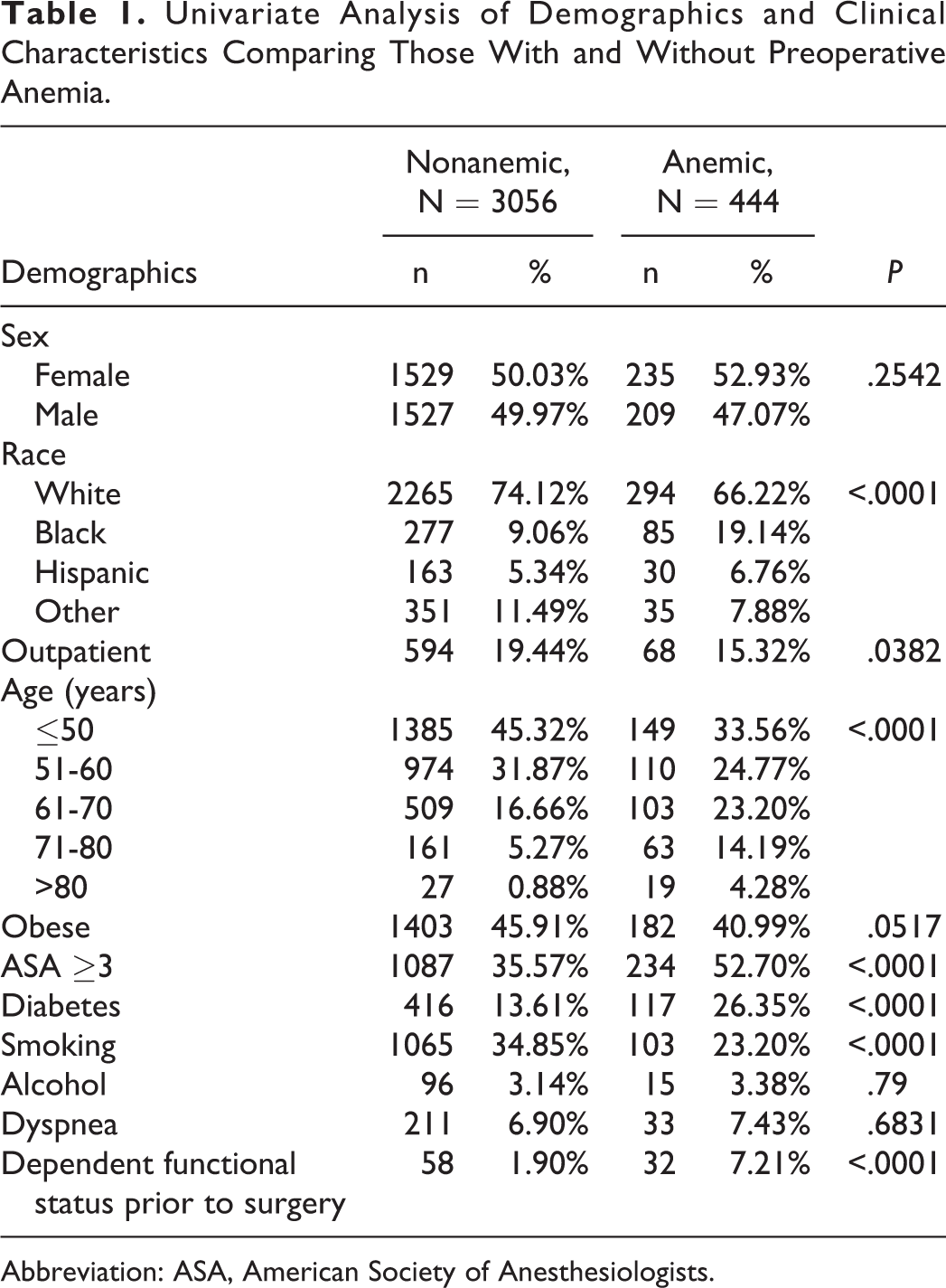
Abbreviation: ASA, American Society of Anesthesiologists.
Patient Comorbidities
Between the nonanemic and anemic groups, there was no significant difference in pulmonary comorbidities (3.5% vs 4.73%; P = .1976), peripheral vascular disease (0.85% vs 1.35%; P = .3004), and steroid usage (2.65% vs 3.60%; P = .253). However, cardiac comorbidities (43.0% vs 62.39%; P < .0001), stroke (1.77% vs 5.18%; P < .0001), neuromuscular injury (3.93% vs 6.98%; P = .0031), recent weight loss (0.20% vs 1.13%; P = .0011), and bleeding disorders (0.88% vs 2.03%; P = .0256) were significantly more prevalent in the anemic patient group (Table 2).
Comorbidities and Operative Variables for Those With and Without Preoperative Anemia.
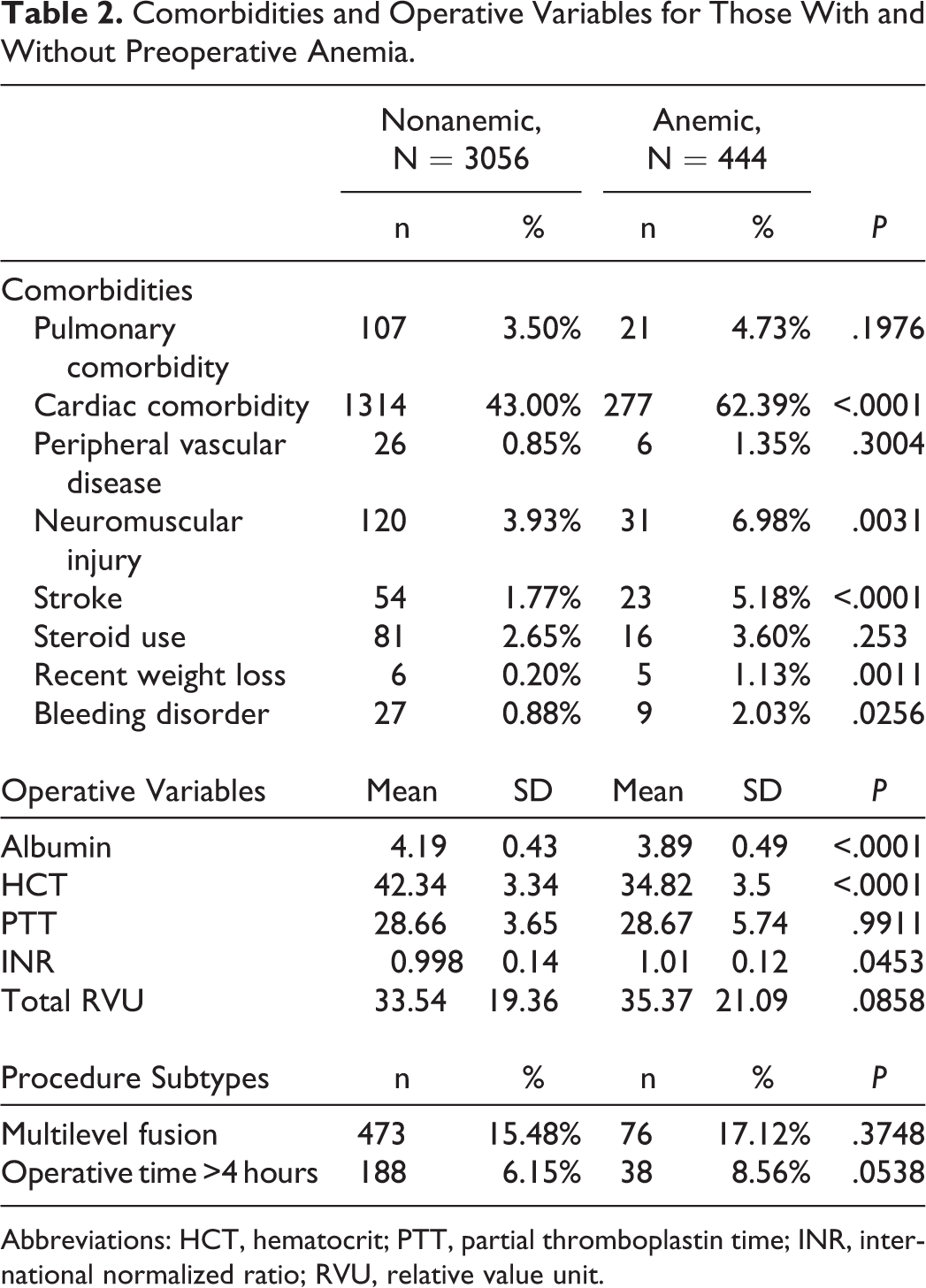
Abbreviations: HCT, hematocrit; PTT, partial thromboplastin time; INR, international normalized ratio; RVU, relative value unit.
Operative Variables
There was no statistically significant difference between the nonanemic and anemic group with regards to PTT, total relative value unit, and number of multilevel fusions, or operative time greater than 4 hours. However, albumin and hematocrit was significantly greater in the nonanemic patient group. The international normalized ratio was greater in the anemic patient group.
Complications
There were no statistically significant difference between the nonanemic group and anemic group with regard to cardiac complications (0.16% vs 045%; P = .2062), pulmonary embolism/deep vein thrombosis (0.52% vs 0.23%; P = .3982), urinary tract infection (0.46% vs 1.13%; P = .0735), would complications (0.69% vs 0.90%; P = .6173), and unplanned reoperations (1.02% vs 2.55%; P = .0653). For the anemic group there was a significant increase in any complication (2.65% vs 6.31%; P < .0001), death (0.2% vs 0.9%; P = .0093), pulmonary complication (0.95% vs 3.83%; P < .0001), renal complication (0.00% vs 0.23%; P = .0087), central nervous system complication (0.10% vs 0.68%; P = .006), peripheral nerve injury (0.07% vs 0.45%; P = .0249), sepsis (0.07% vs 0.45%; P = .0249), intraoperative blood transfusion return to operating theatre (1.37% vs 5.18%; P < .0001), unplanned readmission (2.83% vs 6.12%; P = .0148), and LOS longer than 5 days (4.45% vs 14.41%; P < .0001; Table 3).
Morbidity Univariate Analysis Between Cohorts.
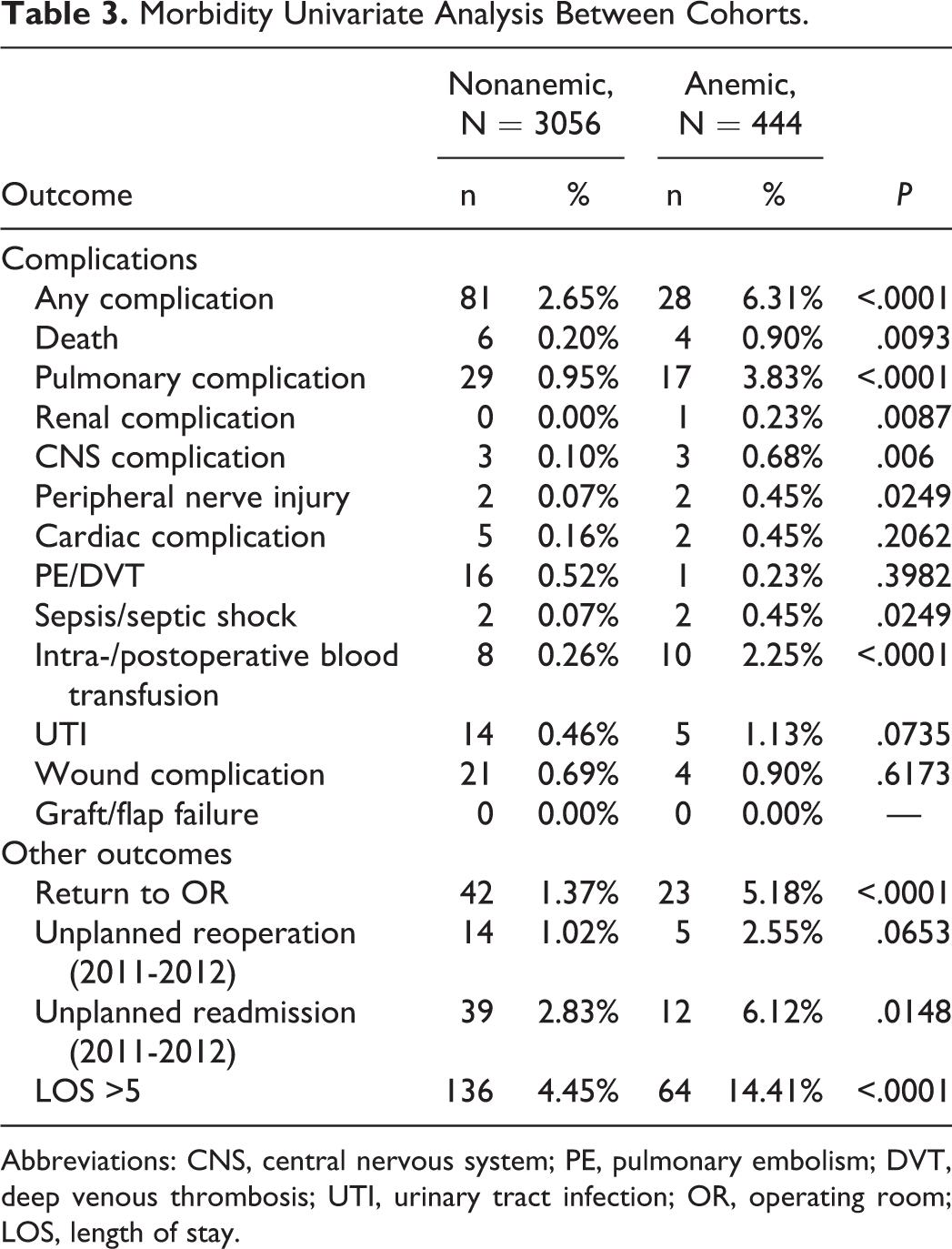
Abbreviations: CNS, central nervous system; PE, pulmonary embolism; DVT, deep venous thrombosis; UTI, urinary tract infection; OR, operating room; LOS, length of stay.
Multivariate Analysis
Multivariate analysis was used to quantify the predictive power of anemia on key postoperative outcomes, while controlling for the other statistically significant variables identified through the univariate analysis. Preoperative anemia was found to be a statistically significant predictor of any complication (odds ratio [OR] = 1.8; 95% confidence interval [CI] = 1.1-2.8; P = .018), pulmonary complications (OR = 3.3; 95% CI = 1.7-6.1; P = .0002), intraoperative blood transfusion (OR = 5.9; 95% CI = 2.0-17.0; P = .001), return to operating theatre (OR = 2.7; 95% CI = 1.6-4.7; P = .0004), and LOS greater than 5 days (OR = 2.3; 95% CI = 1.6-3.2; P < .0001; Table 4).
Multivariable Regression Analysis Analyzing Anemia as a Risk Factor for Complications, N= 3500.
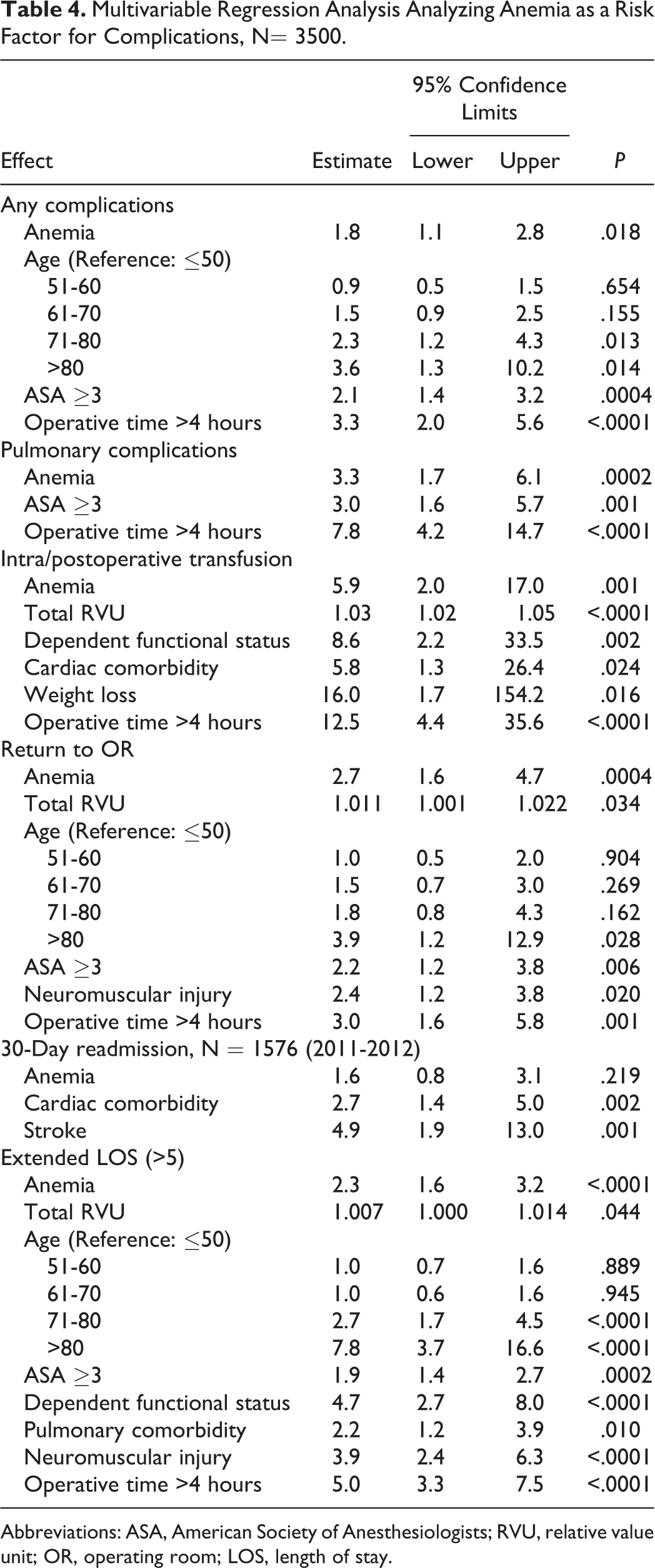
Abbreviations: ASA, American Society of Anesthesiologists; RVU, relative value unit; OR, operating room; LOS, length of stay.
Discussion
ACDF is a common procedure used for cervical disc herniations and spondylosis with 80% to 90% of success rate in relieving radicular symptoms. 26,27 Elective ACDF is considered a relatively low-risk procedure. 1 -3 However some complications can occur such as postoperative dysphagia, postoperative wound hematoma, recurrent laryngeal nerve palsy, and dural tears. 12 With the ageing population, many ACDF patients are elderly and have morbidities that can detrimentally affect outcomes of surgery and increase the risk of postoperative complication. As such, preoperative variables like anemia are becoming increasing important to consider as a potential indicator of patient suitability for surgery or predictor of postoperative complications. 28 However, to date there have been few studies examining the specific role of preoperative anemia on the outcomes of ACDF. Our study of 3500 patients demonstrated that preoperative anemia was a significant predictor of any postoperative complication, pulmonary complications, increased need for blood transfusions, an increase propensity for postsurgical reoperation, and 30-day hospital readmission. These results may be useful in assisting preoperative risk stratification of patients undergoing ACDF and may identify those who may need a higher level of care.
We found that the rate of any complication (minor or major) were 2.65% for nonanemic and 6.31% for anemic patients, which are comparable to other studies in elective spinal surgery. 21,29 Although major complications are rare, they can be catastrophic and warrant careful patient assessment to minimize perioperative morbidity. Some of the severe complications of ACDF include sepsis, deep vein thrombosis/pulmonary embolism, peripheral nerve injury, myocardial infarction, acute kidney injury, and esophageal laceration. 1,26,27,29,30 One of the consequences of major complications is the need for intubation and ventilator support for respiratory compromise. We found anemia to be a significant predictor of pulmonary complications, which includes pneumonia and need for intubation or ventilation. Reoperation is another important consequence that can arise directly or indirectly from the complications of surgery. Anemia was a significant predictor of return to the operating room for ACDF, which has been associated with increased mortality rates. 31 Along with that anemia was associated with an increased length of hospital stay, an important marker of hospital costs and predictor of adverse outcomes in high-risk spinal surgery. 32,33 Given that in most cases minimal blood loss and transfusions are required for ACDF surgery, 34,35 the association between anemia with complications in this study suggests that anemia may be a proxy variable that indicates patients’ general poor health, rather than having a direct bearing on surgery itself. Anemia is multifactorial and more so related to patient comorbidities, which include some confounders that could not be accounted for in the present multivariable analysis.
Although not a primary focus of the present article, other predictors of perioperative outcomes were identified. The ASA score is a subjective assessment of a patient’s preoperative health. We found that an ASA grade ≥3 was a significant predictor of increased length of hospital stay, return to operating room, pulmonary complications, and total complications. In this context, preoperative anemia may be similar to ASA class scores in that it may represent an overall indication of poor health in the patient, thus associated with complications following ACDF surgery. Thus, we suggest that anemia along with the ASA grade should be used when assessing operative risks in patients undergoing elective surgeries.
Although there are multiple studies implicating the influence of preoperative anemia on outcomes of noncardiac procedures, very few have involved spinal surgery. A study of 8015 patients undergoing elective cranial neurosurgery identified preoperative anemia to be independently associated with 30-day mortality and morbidity. 36 Seicean and colleagues 21 performed a similar analysis on 24 473 elective spinal surgeries and identified anemia as a predictor of all complications. The authors also concluded that mild and moderate anemia was associated with prolonged length of hospitalization, increased complications, and 30-day mortality. Interestingly, severe anemia was not associated with any outcomes of interest. The authors suggested inadequate sample size, physiological adjustment, and surgeon technique were responsible for this finding. 21 To the best of the authors’ knowledge, this is the first study examining the effects of anemia on perioperative outcomes in ACDF. Our findings are consistent with other studies of anemia and perioperative outcomes in noncardiac surgery. 16,17,21,36
Limitations
Our study has several limitations. First, the article was an observational study and thus we could not establish causation. However, we did capture and control for multiple covariates in our multivariate models. Second, the follow-up period was only 30 days, which prevents the extrapolation of conclusions beyond this time period. Also only hematocrit data and not hemoglobin data was available in our database. However, the World Health Organization defines anemia using both units and thus we used hematocrit levels. Furthermore, the database did not allow for stratifying different subtypes of anemia, including severity. The study is also an analysis of prospective records collected in a database and is subject to recording errors. Last, it is important to note that the main complications of ACDF are approach-related, such as dysphagia, hoarseness, and laryngeal nerve palsy. However, these endpoints were not collected in the NSQIP database and thus we could not include this is our analysis.
Conclusions
This is the first large multicenter study of prospectively collected data analyzing the effects of anemia on perioperative outcomes in ACDF. Preoperative anemia appears to be a significant predictor of perioperative complications, reoperation, and extended length of hospital stay in patients undergoing elective ACDF. Future studies should explore outcomes of treatment of preoperative anemia prior to surgery to determine the optimal management strategy.
Footnotes
Authors’ Note
This study was qualified as exempt by the Mount Sinai Hospital Institutional Review Board. The article does not contain information about medical device(s)/drug(s).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.