
Abstract
Study Design:
Retrospective comparative analysis of prospective cohort.
Objective:
To determine whether sacroiliac (SI) screw fixation ipsilateral to hand dominance compared to bilateral fixation impacts personal hygiene (wiping) after toileting.
Methods:
Inclusion criteria were adult spinal deformity (ASD) patients with long arthrodesis (≥T12-pelvis) who had undergone primary unilateral or bilateral SI fixation with a minimum of 2-years-follow-up.
Results:
117 consecutive patients were included and separated into 2 groups: bilateral SI fixation (BL, n = 61) and unilateral SI fixation (UNI, n = 56), with no difference in age. Of UNI patients, 10.7% (6) performed personal hygiene with a different hand after surgery, compared to 6.6% (4) of patients who received BL fixation (P = 0.422). All UNI patients who switched hands were right-hand dominant, and 5/6 received right-sided fixation. There was no statistical difference found between number of levels fused (<8, 9-11, or >11 levels) and changes in personal hygiene habits. Over a third of patients from both groups had difficulty performing personal hygiene after fusion (UNI = 39.3% BL = 36.1%, P = 0.719).
Conclusion:
SI screws increase the difficulty of performing personal hygiene; yet, the side of unilateral screws does not significantly change personal hygiene habits when compared to bilateral screw placement. Moreover, the length of the construct does not have a significant impact on ability to perform personal hygiene, cause changes in habits, or require the assistance of another individual. However, among our sample of individuals, bilateral fixation did result in a higher rate of revision instrumentation.
Keywords
Introduction
Bilateral sacroiliac (SI) screws coupled with bilateral S1 screws have been shown to provide additional stability for lumbosacral constructs with a high fusion rate (95.1%) in high-grade spondylolisthesis. 1 Spinopelvic fixation, while sacrificing lumbosacral and sacroiliac motion, decreases the instances of implant failures, such as rod breakage, pseudarthroses, or neurological deficits. 2 Biomechanically, these constructs provide the strongest fixation, and also reduce strain on the S1 screws. 3
The impact on daily activities of SI screws has been previously studied.3-7 It has previously been shown that adult spinal deformity (ASD) patients with iliac screws significantly improve in all health related quality of life (HRQOL) parameters 2 years after surgery. 3 Studies have also shown that the use of a single iliac or S2-Alar-Iliac (S2AI) screw can provide equivalent outcomes and are biomechanically equivalent to bilateral spinopelvic fixation.8-11 An argument can be made that bilateral screws provide no added clinical benefit in most cases. Additionally, some ASD patients instrumented with bilateral SI screws complain of low back stiffness, buttock discomfort, and limitations of daily activities such as getting up from chairs or performing perineal care after toileting.3,6 By preserving motion in one sacroiliac joint, it is possible that this could influence a patient’s personal hygiene habits and ability to reach around to wipe. No study to date has examined whether laterality of a single SI screw fixation disrupts dominant hand usage in the ability of a patient to perform personal hygiene (wiping) after toileting, and to help direct surgeon placement of a unilateral screw.
Methods
Hypothesis
The authors’ hypothesis was that patients who received SI screw fixation ipsilateral to hand dominance would change toileting habits more than patients who received bilateral fixation.
Data Collection
Institutional review board (IRB) exemption was received prior to initiation of this study. Patient consent was obtained for inclusion in this study. A retrospective review of a prospectively collected database was queried. ASD patients with long arthrodesis (≥T12-pelvis) who had undergone primary unilateral or bilateral SI fixation with a minimum of 2-years-follow-up were included (Figures 1 and 2). All patients received traditional iliac screws with connectors. Both surgeons switched from bilateral to unilateral fixation, and this retrospective review examined patients from before and after that transition. The laterality of unilateral screws was also up to surgeon discretion – one always places right-sided SI screws, whereas the other choses laterality based on the lumbosacral fractional curve pattern. The diagnosis in all patients was multilevel degenerative spinal disease with associated spinal deformity of scoliosis, kyphosis, or both. The following preoperative, 1-year, and 2-year variables were collected prospectively: age, sex, number of instrumented levels, laterality of unilateral screws, complications, reoperations. Radiographic parameters including pelvic incidence (PI), sagittal vertical axis (SVA), and coronal balance were measured preoperatively and at 2 years postoperatively. Clinical outcome measures were assessed with visual analog scale (VAS) and Oswestry Disability Index (ODI).
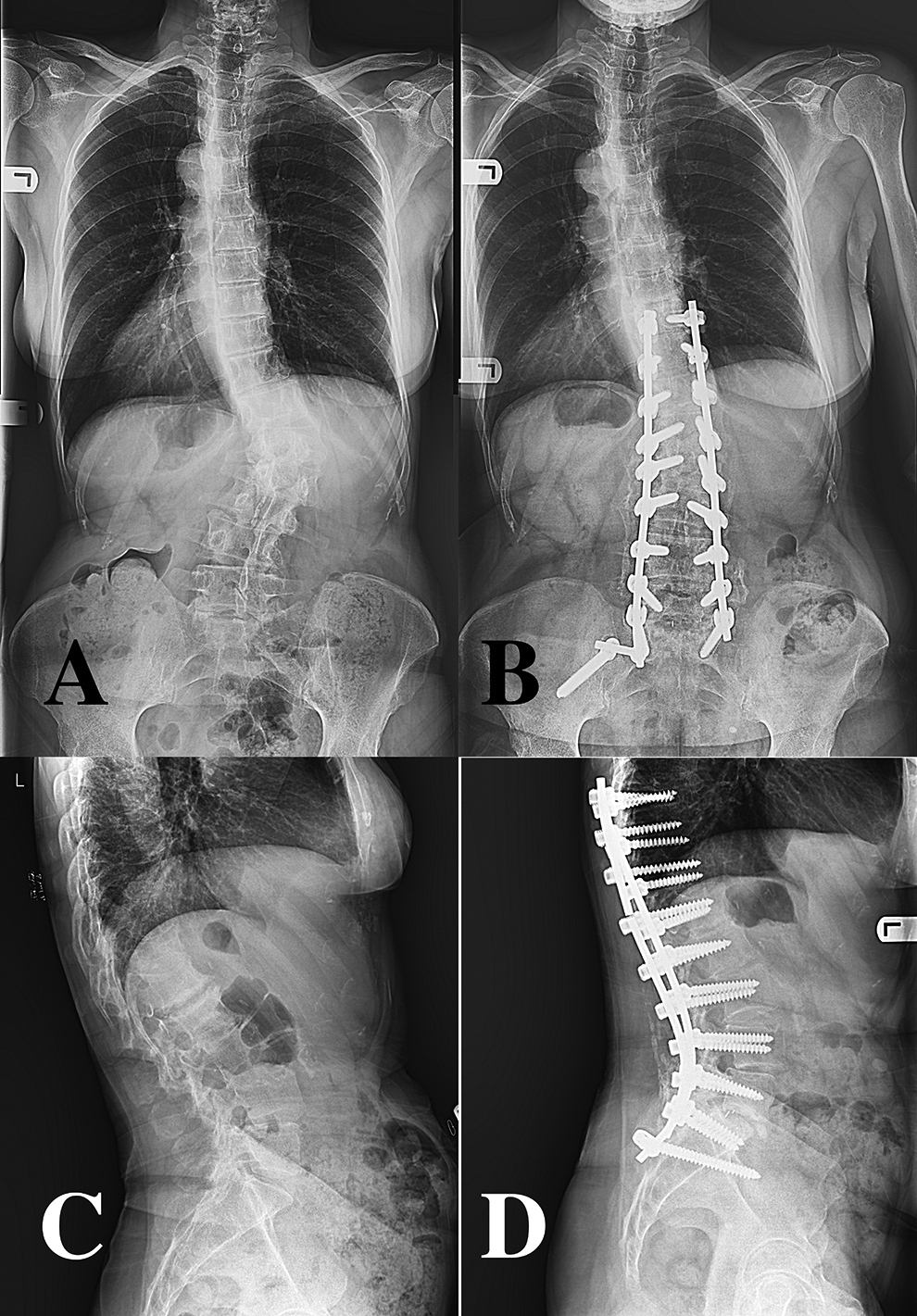
AP and lateral standing radiographs of the same patient preoperatively and at 2-year follow-up, with bilateral iliac fixation. A, Pre-operative long-standing AP radiograph of the spine with degenerative scoliosis, (B) 2-year post-operative long standing AP radiograph of the spine with bilateral iliac screws. C, Pre-operative long-standing lateral radiograph of the spine, (D) 2-year post-operative long standing AP radiograph of the spine with bilateral iliac screws.
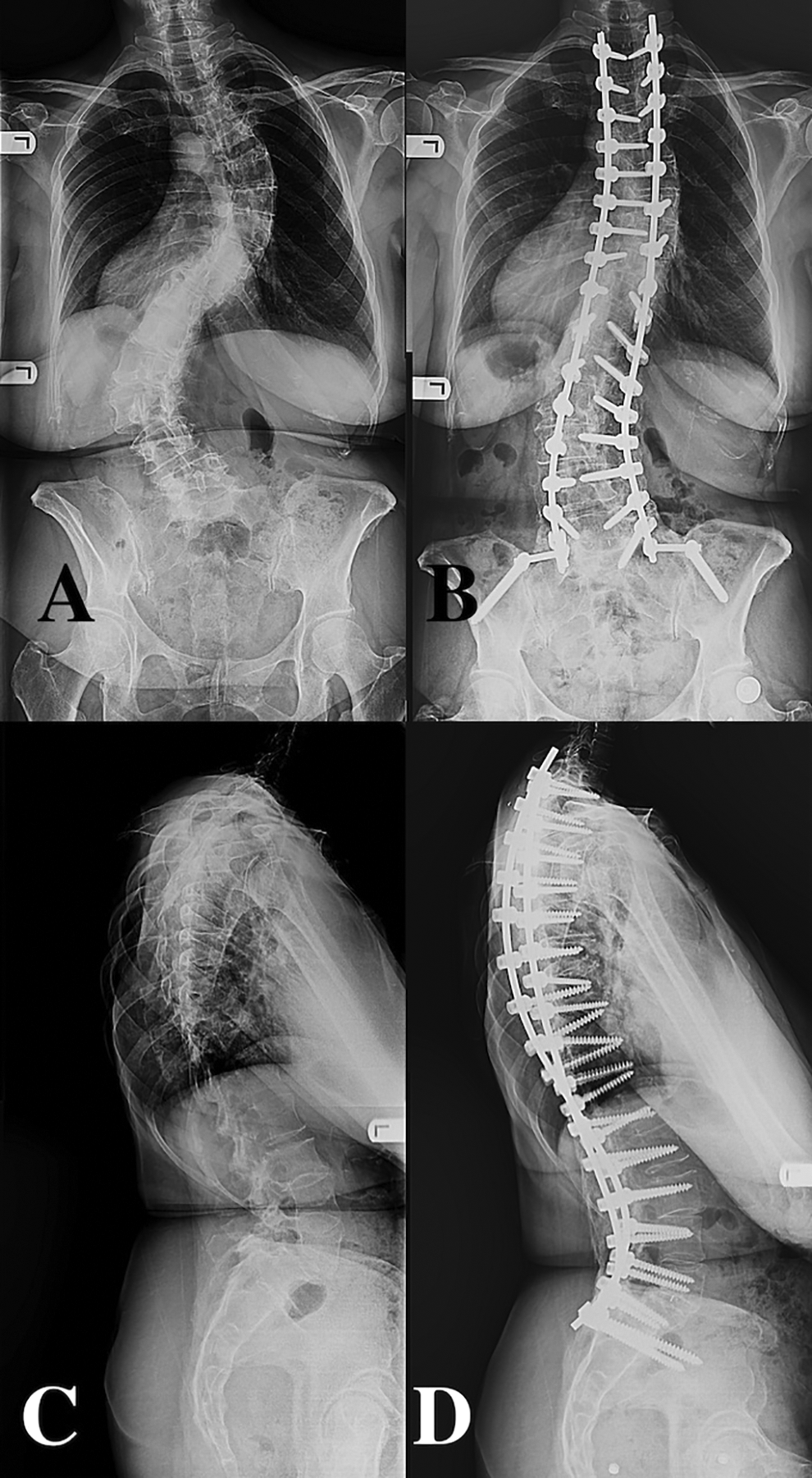
AP and lateral standing radiographs of the same patient preoperatively and at 2-year follow-up, with unilateral iliac fixation. A, Pre-operative long-standing AP radiograph of the spine with degenerative scoliosis, (B) 2-year post-operative long standing AP radiograph of the spine with unilateral iliac screw. C, Pre-operative long-standing lateral radiograph of the spine, (D) 2-year post-operative long standing AP radiograph of the spine with unilateral iliac screw.
Phone interviews were conducted after the final visit to determine hand-dominance and personal hygiene habits after toileting post-operatively (please see Appendix 1 for survey). Patients were first asked to rate their disability level before and after surgery on a scale 1 to 10 (1 = normal function, 10 = non-functional). They were then asked which hand was used to perform wiping habits after toileting pre-operatively and post-operatively. Additionally, patients were asked if there had been any other notable changes in their personal hygiene habits after toileting such as need for assistive devices or aids.
Data Analysis
Statistical analysis was performing utilizing Microsoft Excel (Redmond, WA) and Stata-IC (College Station, TX) with significance set at P < 0.05. Student t-tests were utilized for continuous variables and chi-squared tests were utilized were categorical variables.
Results
A total of 117 consecutive patients were included and separated into 2 groups: bilateral SI fixation (BL, n = 61) and unilateral SI fixation (UNI, n = 56). Patients were similar between groups in terms of age (average 66.4 years old) and gender ratio. Average body mass index (BMI) was 25.3 kg/m2 in the UNI group and 25.4 kg/m2 in the BL group (P = 0.442). Follow-up was significantly longer in the UNI group (81.2 months) compared to the BL group (68.0 months) (P = 0.0303). The difference in length of posterior spinal fusion construct between the 2 groups trended toward significance (UNI 9.5 levels v. BL 10.4 levels, P = 0.0884) (Table 1).
Patient Demographics and Characteristics.
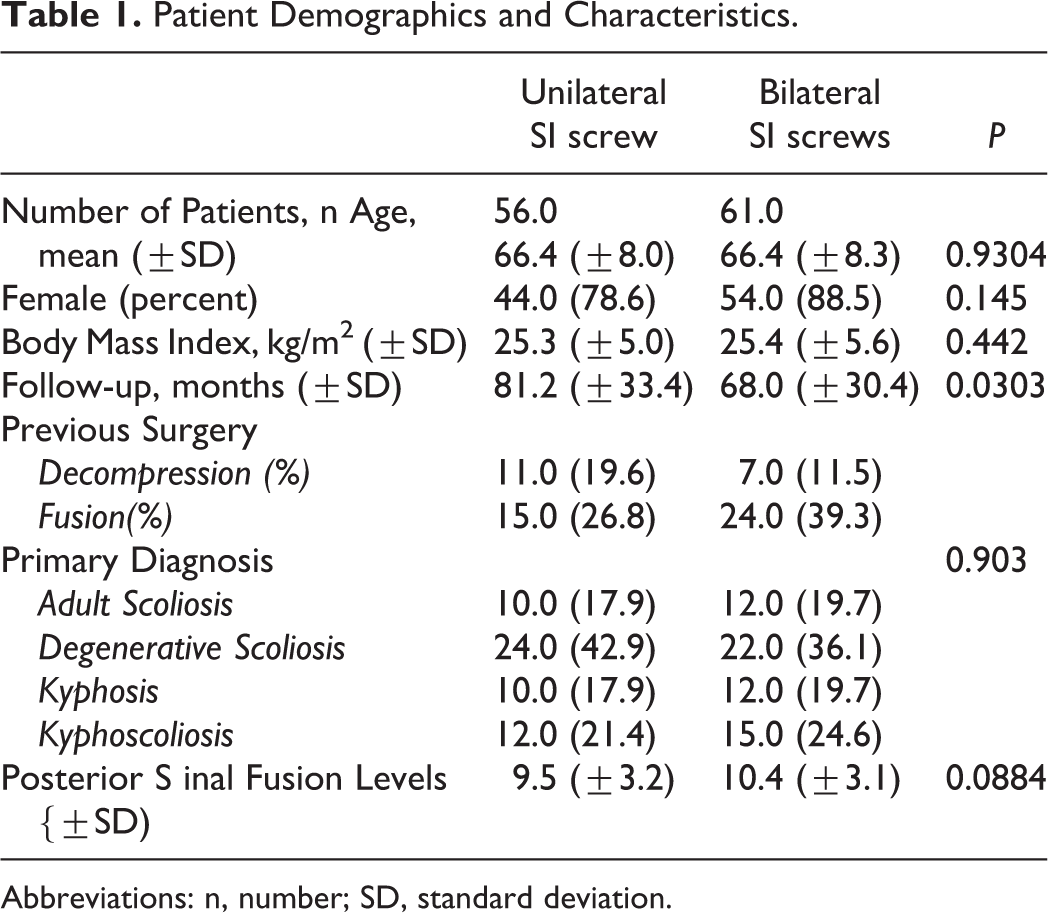
Abbreviations: n, number; SD, standard deviation.
Of the UNI patients, 51 (91.1%) were right-hand-dominant (RHD), 3 (5.4%) were left-hand-dominant (LHD), and 2 (3.5%) were ambidextrous (Table 2). All patients performed personal hygiene after toileting with their dominant hand pre-operatively. Similarly, 58 (95.1%) BL patients were RHD, 2 (3.3%) LHD, and 1 (1.6%) ambidextrous. There was no significant difference in this distribution (P = 0.68). Forty-six (82.1%) of UNI patients received right-sided fixation (Table 2). Of UNI patients, 10.7% (6) changed hands used to perform personal hygiene after surgery, compared to 6.6% (4) of patients who received BL fixation (P = 0.422). One BL patient was unable to perform personal hygiene by himself after surgery. All UNI patients who switched hands were RHD, and 5/6 received right-sided fixation.
Patient Handedness, and Hand Used When Performing Personal Bathroom Hygiene.a
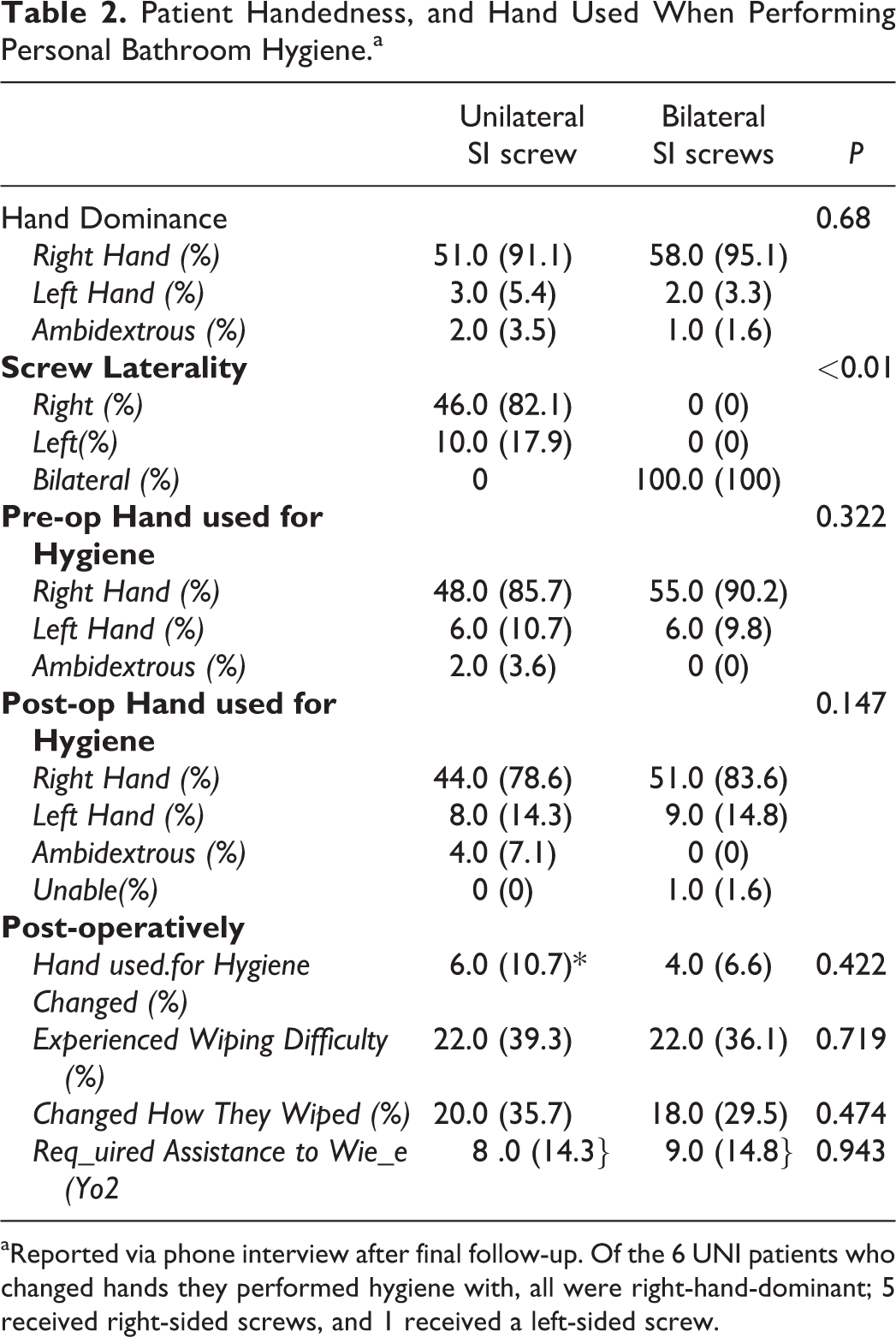
aReported via phone interview after final follow-up. Of the 6 UNI patients who changed hands they performed hygiene with, all were right-hand-dominant; 5 received right-sided screws, and 1 received a left-sided screw.
Notably, over a third of patients from both groups had persistent difficulty with personal hygiene after fusion (UNI = 22 (39.3%); BL = 22 (36.1%), P = 0.719, Table 2). Twenty (35.7%) of UNI patients and 18 (29.5%) of BL patients (P = 0.474) had to adjust their personal hygiene habits after surgery. This included the use of “reacher” devices. Fourteen percent of patients from both groups required assistance performing personal hygiene after fusion (P = 0.943).
Clinical outcome measures consisting of ODI and VAS were collected preoperatively and at the 1- and 2-year follow-up visits. Both groups improved in VAS and ODI at 1-year and 2-year compared to pre-op, but there was no significant difference in the improvement between the groups. Radiographical measures from long-standing radiographs were collected pre-operatively and at the 2-year follow-up visit. Pelvic incidence was similar in both groups, 57.2º and 57.5º in UNI and BL, respectively. Sagittal balance improved in both groups from pre-op to 2-year post-op, from 7.1 cm to 5.9 cm in UNI and from 7.9 cm to 6.3 cm in BL. Coronal balance in the UNI group on average changed from 2.6 cm preoperatively to 2.7 cm postoperatively, whereas in the BL group this improved from 3.4 cm to 2.4 cm postoperatively. However, no statistical differences were found between the 2 groups in preoperative or postoperative ODI, VAS, or coronal and sagittal balance (Table 3). There was no statistical difference found between number of levels fused (<8, 9-11, or >11 levels) and changes in personal hygiene habits (Table 4).
VAS, ODL and Radiographic Measurements.
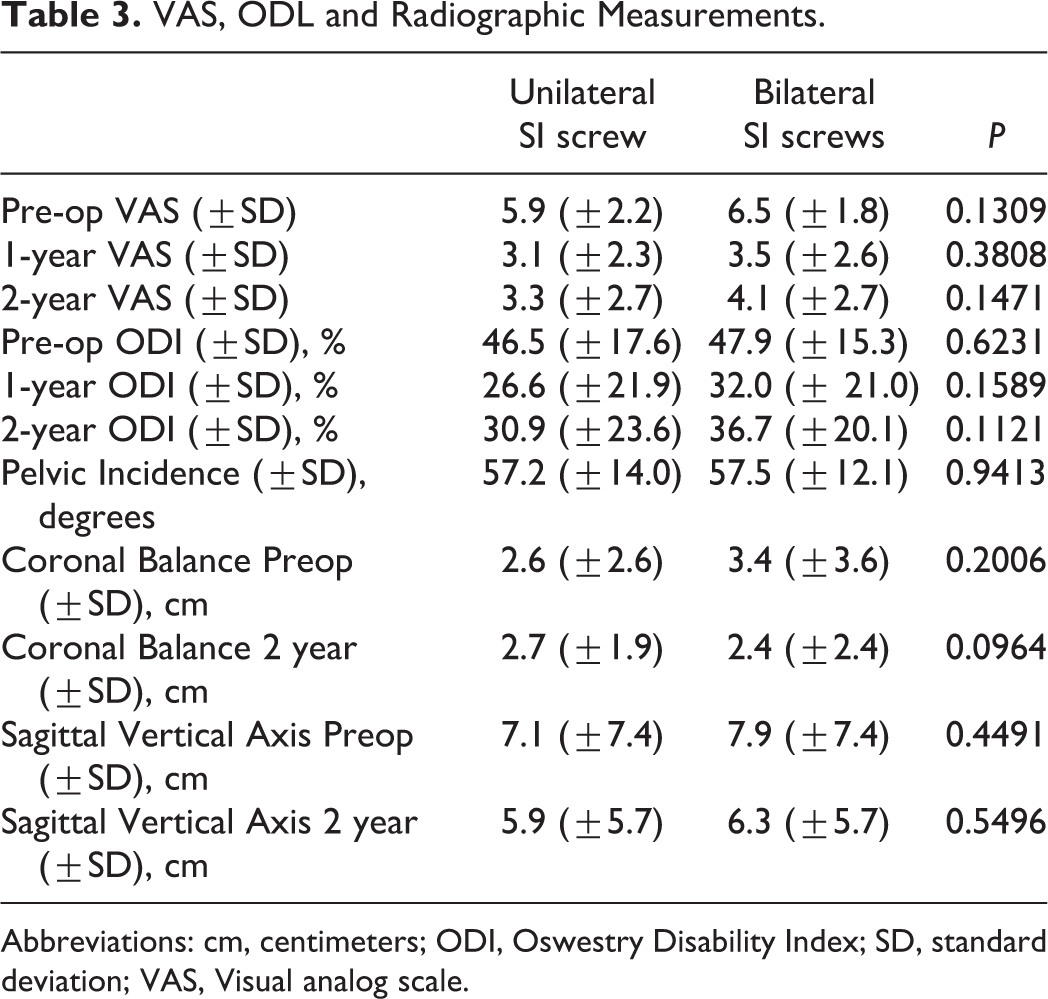
Abbreviations: cm, centimeters; ODI, Oswestry Disability Index; SD, standard deviation; VAS, Visual analog scale.
Length of Fusion Construct and Ability to Perform Personal Hygiene.

Over one-fourth of UNI patients (15, 26.8%) and over one-third of BL patients (21, 34.4%) required additional surgeries, including hardware removal, iliac screw removal, additional decompression, fusion revision/extension, and irrigation/debridement (P = 0.371, Table 5). There was a significantly higher rate of revision instrumentation in the BL cohort (29.5% v. 14.3%, P = 0.048). These revisions surgeries were mostly due to a higher rate of nonunions and rod fractures in the BL group (nonunions: 3 v. 15, P = 0.004; rod fracture 3.v. 17, P = 0.001; UNI and BL, respectively). Other causes of additional surgery, including hardware removal, iliac screw removal, additional decompression, and irrigation/debridement were not different between the 2 groups.
Additional Surgeries and Postoperative Complications.
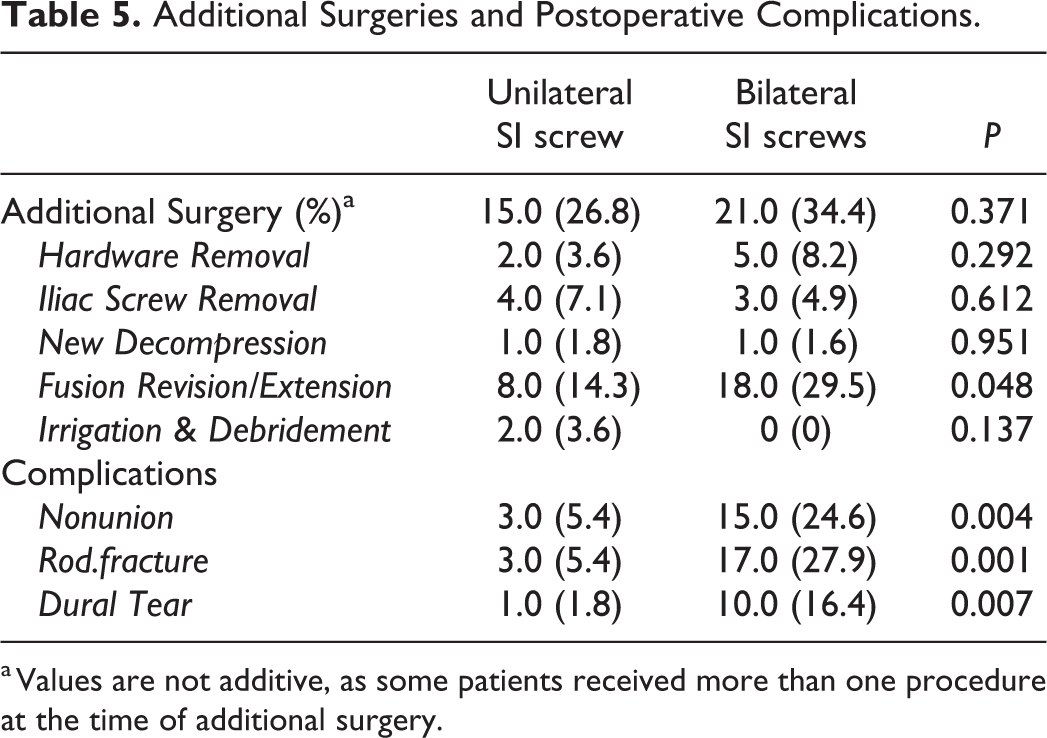
a Values are not additive, as some patients received more than one procedure at the time of additional surgery.
Discussion
Bilateral SI screw fixation is known to be an effective method of achieving stabilization in ASD patients; however, there are inherent limitations to the procedure related to patient function. Patients undergoing arthrodesis of the lumbar spine report significant improvements in both pain and function compared to non-operative therapy. 12 Unfortunately, the beneficial effect of spinopelvic fusion may be offset by limitations induced on the patient’s ability to perform activities of daily living (ADLs) such as performing personal hygiene. Studies have also shown that the use of a single iliac or S2AI screw can provide equivalent outcomes and are biomechanically equivalent to bilateral spinopelvic fixation, and this ultimately led to the change in practice demonstrated in this study. 8 –11 The objective of this study was to determine if UNI SI screw fixation significantly altered a patient’s ability to perform personal hygiene after toileting as determined by functional hand dominance in comparison to BL SI screw fixation. The data presented concludes that there is an overall increase in difficulty with performing personal hygiene in patients that undergo UNI or BL SI screw fixation; however, the side of the UNI screw does not appear to significantly impact performance compared to BL fixation. Of note, out of 6 UNI screw patients that switched hand dominance, 5 were RHD and received right sided UNI screws.
Pain and stiffness are the predominant limitations that restrict a patient’s ability to perform personal hygiene post-operatively. Both measures are documented by subjective patient reporting and limitations in patient comfort, as even range of motion measurements may be restricted by patient tolerance. Therefore, optimizing patient reported outcomes and the patients’ impression of their functional status post-operatively is vital in achieving a successful procedure. To the authors’ knowledge, this study was the first to examine 1) the effect of UNI versus BL SI screws connected to long spinal constructs on toileting habits and 2) whether the laterality of a UNI SI screw changes toileting habits. Sciubba et al found that patients with constructs ending in the lower thoracic or thoracolumbar junction, reported significant decreases in their ability to dress and bath the lower half of their body. 13 Bafus et al analyzed the ability of patients to perform perineal hygiene after thoracic fusion to L5 or the sacrum and found that 36.0% reported difficulty with previously tolerated tasks, which is similar to our findings. 14 In addition, Hamilton et al reported that among patients undergoing spinopelvic instrumentation 15.0%, 19.0%, and 42.0% experienced mild, moderate, or severe sexual dysfunction, respectively, following the procedure. 15 The data presented here showed that more than 10% of patients required the assistance of another individual in toileting after undergoing SI screw placement regardless of UNI or BL fixation. Existing literature on the subject matter clearly shows a detrimental impact to patient independence. It is unclear the degree to which these adverse effects weigh against expected pain relief and restoration of spinal alignment with the procedure. These limitations should be discussed with patients during pre-operative encounters in the hope that anticipated changes in ADL function do not unexpectedly hinder the patient’s notion of a successful surgical outcome.
Surgical value is a familiar concept to surgeons practicing in the United States. The value of a procedure can be estimated by quality, as it relates to the patient’s outcome, per the cost of the procedure. The intent of surgical treatment for ASD patients is reduction of pain and maintenance or improvement of functional status. This study examined the patient’s rating of their own disability status, using VAS and ODI as surrogates for quality. There are multiple other validated metrics within the literature that help to give a procedure quality based on the patients experience and overall satisfaction, however, ODI and VAS have been validated within our study population. 16 Hart et al found that patients self-reported limitations due to lumbar pain and stiffness correlated well with the ODI. 17 Despite different technical considerations between unilateral and bilateral SI screw fixation, our data showed no difference in the change in VAS or ODI between the 2 treatments groups pre- and post-operatively. Considering ODI as a measure for functional limitation, our data suggests no difference between the 2 groups. It is important to note that despite over a third of patients having difficulties in performing personal hygiene after toileting, overall ODI improvement suggests that patient function improved overall as a result of surgery which offset the functional personal hygiene limitations that developed post-operatively.
The pattern of patients that did switch hand dominance when performing toileting after undergoing UNI fixation is worth review. Out of the 6 UNI patients that changed hand dominance, 5 were previously performing perineal hygiene RHD and switched to LHD after undergoing UNI right-sided SI screws. This is in comparison to one patient that was RHD and switched to LHD after receiving left sided UNI screw fixation. Interestingly, no left-handed individuals changed their hand of preference, although this may be due to the low number of LHD patients in our study group.
Limitations to this study include its retrospective nature which relies on patient recall in determining their pre-operative disability. Another possible co-founder is that there was on average just under one fusion level difference between the 2 groups, although this did not reach significance. Patients struggling with functional limitations post-operatively may under-estimate their pre-operative disability. Although our data was comprised of a relatively small group of patients, it compares well to the existing literature on metrics and the authors’ find that this study is sufficient to answer our hypothesis. It is apparent that a large number of patients undergoing fusion experience difficulty with toileting after long spinopelvic fusions; however, it does not appear that there is a linear response. Bilateral fixation does not appear to impact ability to perform hygiene to a greater degree than UNI fixation. In addition, there does not appear to be a clear link between side of UNI SI screw fixation and alteration of personal hygiene habits.
Conclusion
SI screws increase the difficulty of performing personal hygiene; yet, the side of unilateral screws does not significantly change personal hygiene habits when compared to bilateral screw placement. Moreover, the length of the construct does not have a significant impact on ability to perform personal hygiene, cause changes in habits, or require the assistance of another individual. However, among our sample of individuals, bilateral fixation did result in a higher rate of revision instrumentation.
Supplemental Material
Supplemental material - Does Laterality Matter? The Effect of Unilateral v. Bilateral Sacroiliac Screw Fixation on Personal Hygiene
Supplemental material for Does Laterality Matter? The Effect of Unilateral v. Bilateral Sacroiliac Screw Fixation on Personal Hygiene by David G. Deckey, Matthew T. Gulbrandsen, Nathaniel B. Hinckley, Nina Lara, Cory K. Mayfield, Justin L. Makovicka, Biodun Adeniyi and Michael S. Chang in Global Spine Journal
Footnotes
Authors’ Note
Institutional review board (IRB) exemption was received prior to initiation of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.