
Abstract
Study Design
Narrative literature review.
Objectives
To summarize the evidence for perioperative blood conservation for patients undergoing surgery for adult spine deformity.
Methods
A systematic literature review with narrative analysis was conducted to describe the evidence for blood conservation strategies before, during and after surgery for adult spine deformity. The evidence is critically analyzed and recommendation drawn.
Results
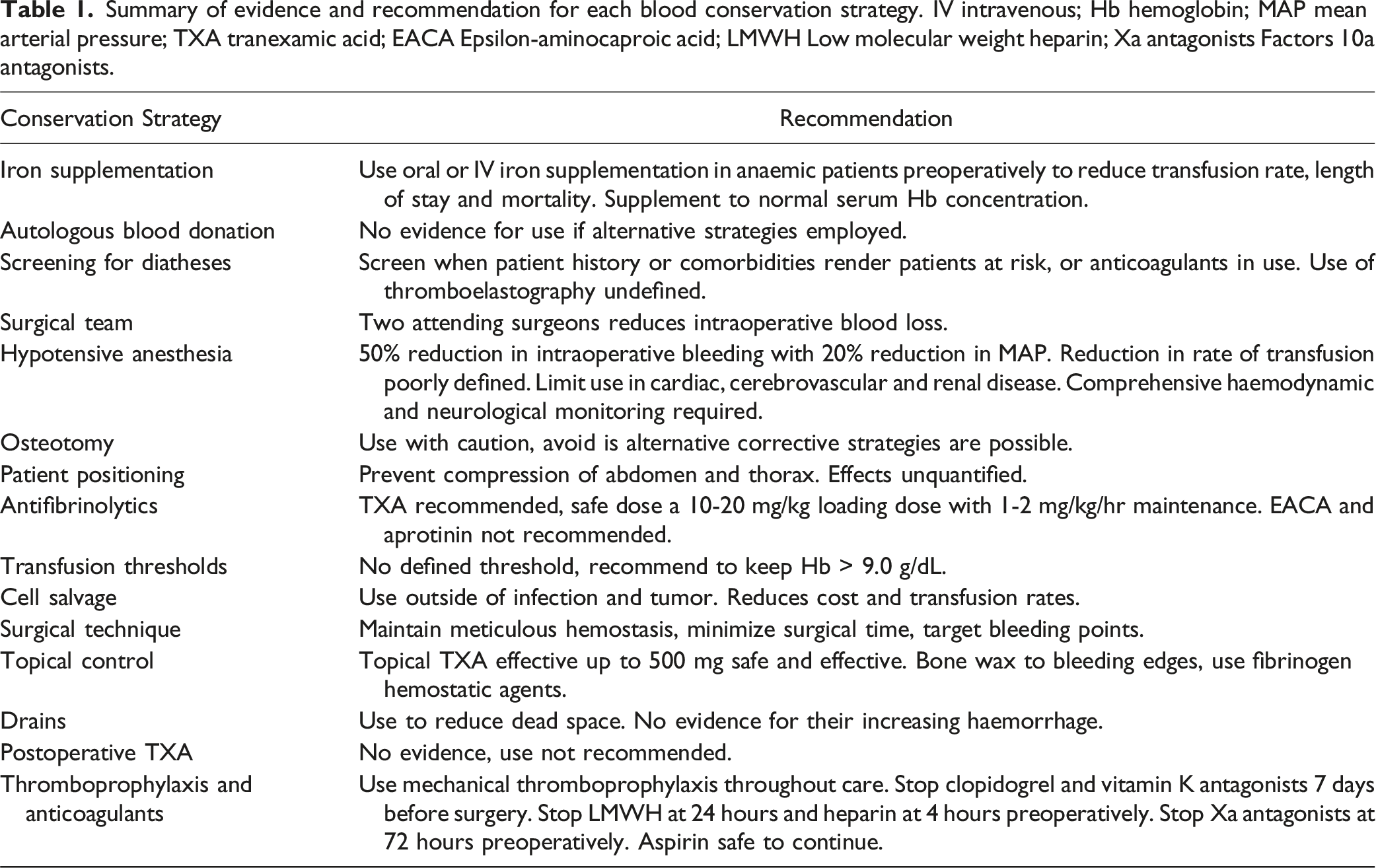
The evidence for iron supplementation, autologous blood donation, screening for diatheses, the constitution of the surgical team, hypotensive anaesthesia, osteotomy, patient positioning, antifibrinolytics, transfusion thresholds, cell salvage, surgical technique, topical hemostasis, postoperative drainage, postoperative tranexamic acid and the management of thromboprophylaxis and anticoagulants is critically evaluated. The management of haemorrhage in surgery for adult spine deformity is complex and multifaceted, requiring the surgeon to consider tactics in conservation at every stage of the process. There is a paucity of evidence for many techniques, whilst hypotensive anaesthesia, tranexamic acid, surgical team members and surgical duration have the most significant effects on blood loss and transfusion requirements.
Conclusions
The astute surgeon must consider strategies to prevent excessive haemorrhage in the pre- intra- and postoperative phases of care. Although some commonly used techniques have robust evidence, others may be at best poorly evidenced, and at worst ineffective. Surgeons should consider the members of the operative team, minimizing surgical time, preoperative correction of anemia, hypotensive anesthesia and the use of intravenous and topical tranexamic acid at a minimum.
Keywords
Introduction
Surgery for adult spine deformity (ASD) is a large undertaking for both the patient and the surgeon for many reasons. Although some risks are unavoidable, others such as bleeding can be controlled. 1 This is important, because the consequences of haemorrhage, ranging from physiologic instability to neurological injury, come with morbidity and an increased risk of complications.
Replacing intravascular volume with crystalloids reduces oxygen delivery to already compromised organs and neurological structures, whereas transfusing allogenic blood, a constrained resource, brings a risk of adverse transfusion related reaction. Therefore, strategies to pre-empt blood loss through patient optimization, and preventing bleeding with modifications to anesthetic and surgical techniques have become necessarily routine. In this article, the evidence for several of these techniques and the future of haemorrhage management in ASD surgery is explored.
Pre-Operative
Iron Supplementation
Prior to adult spine deformity surgery, safe and effective spinal units will carry out preoperative assessments of a patient’s fitness for their procedure. Data from these assessments suggests that 30% of patients scheduled for adult spine deformity are anaemic (pre-operative anaemia, POA). Further analysis shows that POA is accompanied with a higher risk of transfusion, complication and mortality which persists through to the 90th post-operative day.2-10 Fortunately, if patients are treated for POA, the risk of adverse events is reduced and the length of stay shortens.11,12 There are several options for managing POA, the most common of which is iron supplementation, which can reduce allogenic transfusion by up to 39%.5,11,13-15 In contrast however, the PREVENTT trial and a 2019 Cochrane review failed to show that iron supplementation reduces the need for transfusion when compared to a placebo.16,17
The lead time for iron supplementation prior to surgery has yet to be defined, and whether oral preparations have the same efficacy as IV iron at reduced cost and inconvenience remains unknown. Future studies will need to investigate how iron deficiency affects the long-term outcomes in ASD patients specifically, and how IV or oral iron supplementation can be most advantageously employed.
Autologous Blood Donation
Preoperative autologous blood donation (PABD) has fallen from favor since the introduction of cell salvage. Approximately 92% of patients are suitable for PABD, with some calculating that if used, 47.8% of patients could avoid subsequent allogenic transfusion.18-22 Unfortunately PABD programs are costly to set up and maintain, and increase the likelihood of POA and major perioperative cardiac events.19,23,24 Each unit of collected blood has a limited lifespan which causes 30% to be discarded before use. 25 Combining PABD with iron supplementation and other conservation strategies may be useful, but future work should focus on deciding when it is necessary.
Screening for Diatheses
Screening for coagulopathy has a poor positive predictive value and studies have shown that investigations are not superior to patient questionnaires in identifying patients at risk of clinically relevant bleeding.26-31 Combined with the low prevalence of bleeding disorders, the inadequacy of these tests is reflected in anesthesia guidelines which recommend point-of-care testing when suspicion, liver dysfunction or anticoagulant use require it.32-37 Nonetheless, a study of 9295 patients showed that elevated INR and APTT and low platelets are independent predictors of adverse outcomes including stroke and death in patients undergoing posterior lumbar fusion, concluding that patients should be pre-operatively tested for coagulopathy. 38
Thromboelastography, which assesses clot formation in whole blood to detect deficiencies in coagulation factors and platelets, can guide the intraoperative supplementation of coagulation components. 39 Its role in spine surgery may increase as availability and understanding of its indications grows.
Current recommendations rely on clinical suspicion to identify those at risk of bleeding with judicious use of clotting studies. It may be that point of care tests may be more useful and should be employed more often than they are now, and future work should focus on correlating these tests with objective measurements of peri-operative blood loss and transfusion.
Special Considerations for Jehovah’s Witnesses
The Jehovah’s Witnesses are a Christian denomination that may decline transfusion on the basis of the prohibited consumption of blood. 40 Each patient’s beliefs vary, and so every case should be judged on its own merits as the acceptability of products varies; nonetheless, a strategy for preventing and managing haemorrhage in this specific group is vital.
Haemodilution and staged procedures were historically used to control haemorrhage in this patient group.41-43 In recent times, preoperative erythropoietin, iron supplementation, hypotensive anaesthesia, haemodilution, cell salvage, antifibrinolytics, recombinant factor VII, platelet-phoresis and a less invasive surgical technique have each been employed with varying efficacy.44-49
Defining a threshold for transfusion is difficult because the safe lower limit of haemoglobin in elective spine patients, particularly where preexisting neurological dysfunction is present, is unknown. 43 Further, hemoglobin levels would be expected to drop in the days following surgery, such that intra-operative hemoglobin levels may not be reflective of post-operative transfusion requirements. In future, the value of different intraoperative techniques and postoperative haemoglobin and oxygenation protocols in this group need defining.
Surgical Team
The composition of the surgical team influences the outcomes of surgery. Although training is essential, spine surgeries with trainee involvement are associated with an OR of 2.80 of transfusion. 50 As a result, there is a trend towards 2 attending operating, which reduces the duration of surgery, length of stay, complications and blood loss by up to 80%.51-53
Intraoperative
Hypotensive Anesthesia
Controlled hypotension during anaesthesia is now routine practice.54,55 Although recent work has shown that a 20% reduction in mean arterial pressure (MAP) contributes to a 50% reduction in blood loss in adult spinal procedures, the role of hypotensive anaesthesia in reducing blood transfusion requirements remains debated.56-60 Whereas some analyses have shown a 45% reduction in transfusion requirements with hypotensive anaesthesia, others have suggested that the reduction in transfusion is only 6%, leaving the issue unreconciled.56,61,62
It may be that confounders, such as reduced surgical duration because of improved surgical visibility, are responsible for the reduction in bleeding. This mechanism is important to elucidate because hypotensive anaesthesia is not without risk. Although there has been no proven association with postoperative thrombosis, patients vulnerable to ischemia such as those with cardiac, cerebrovascular and renal disease are at risk of injury with a low perfusion pressure.24,55,63 Similarly, hypotensive anaesthesia brings a risk of spinal cord, optic and vestibulocochlear nerve injury through hypoperfusion.64,65
To control these risks, neurophysiologic and precise anesthetic monitoring is essential, to facilitate a rapid response to an adverse systemic response.55,63,66,67 Nonetheless, a method to balance the individual risks of hypotensive anaesthesia when used in conjunction with other blood preservation techniques is yet to be defined. Forthcoming investigations need to quantify the role of hypotensive anaesthesia so that aggressive spine surgery can be considered in patients with comorbidities that would normally preclude its use.
Neuromonitoring Signal Changes and Post-Operative Neurological Deficits
Anaemia, which diminishes the potential for blood to transport oxygen to the tissues, has a close relationship with changes to neuromonitoring signals and post-operative neurological function.68,69 Low oxygen carrying capacity is itself an important cause of intraoperative neuromonitoring events, though its contribution to the vulnerability of to the changes observed through stretching the spinal cord, direct trauma or underperfusion is equally critical. In the preoperative phase, correcting anaemia anticipates this through maximizing the oxygen carrying potential of the blood in advance of correction maneuvers, and anticipates the need for intraoperative blood transfusion in response to neuromonitoring changes. Similarly, volume resuscitation fails to improve the oxygen carrying capacity of the circulation, thus simply restoring MAP without addressing the oxygen capacity though increasing haematocrit is unlikely to provide an adequate response. 69
The risk of anaemia is not obviated in the postoperative phase. Although transfusion thresholds remain debated across spinal surgery, postoperative anaemia, particularly in the setting of a intraoperative loss of signals, benefits from actively increasing the circulating haemoglobin to improve end organ oxygen delivery when neurological deficits are observed and other causes of deterioration excluded. 70 Although the risk of transfusion is associated with an increased risk of adverse consequences, this must be tempered with the consequences of neglected neurological deficit. 71
Osteotomy
Osteotomy often causes significant haemorrhage, although with pedicle subtraction osteotomy (PSO) having a similar success and complication rate as a vertebral column resection (VCR), the evidence for the more extensive osteotomy is becoming less convincing.72-76 More recent methods for addressing deformity, such as lateral interbody fusion and MIS techniques are associated with less bleeding. 77 As a result of this risk of bleeding in addition to neurological risks associated with their use, osteotomy should be used with caution and alternatives should be sought when possible.
Patient Positioning
Patient positioning has an often-overlooked influence on intraoperative bleeding. Prone positioning over bolsters, sparing compression of the abdomen and thorax is important to avoid increased venous bleeding.78,79 However, the effect of patient positioning on haemorrhage in ASD surgery remains unquantified.79-81
Antifibrinolytics
Antifibrinolytics including tranexamic acid (TXA), epsilon-aminocaproic acid (EACA) and aprotinin have been used in the perioperative period to reduce intraoperative bleeding and the need for post-operative transfusion.
TXA reversibly inhibits fibrinolysis which is associated with less blood loss and transfusion volume in ASD surgery without an increased risk of thromboembolism.82,83 With its safe profile, it is the most widely utilized antifibrinolytic in ASD surgery. Nonetheless, controversy surrounding the most effective dosing regimen persists.84-90
In response, the relative efficacy of high or low dose TXA has been investigated. Whilst the majority of these have been within the adolescent population, Raman et al showed that a 10-20 mg/kg loading dose with 1-2 mg/kg/hr maintenance was more effective at reducing blood loss and transfusion than a loading dose of 30-50 mg/kg with 1-10 mg/kg/hr maintenance. 91 Similarly Hasan et al conducted a prospective, randomised trial showing that a high dose regime (30 mg/kg loading dose followed by 10 mg/kg/h maintenance) showed a similar intraoperative blood loss to a lower dose of 10 mg/kg TXA loading dose followed by 1 mg/kg/h infusion when treating adolescent scoliosis. 92
Tumber at al. went on to study a retrospective cohort comparing a loading dose of less than 30 mg/kg against a higher dose, both with maintenance doses of 10 mg/kg/hr, finding that the higher dose showed significantly lower blood loss and transfusion rate. 93 Even higher doses of up to 50 mg/kg loading and 20 mg/hr maintenance have been shown to be safe and practical, with the highest doses subject to ongoing investigation.94,95
To avoid the toxic effects of TXA at very high doses, including atrial fibrillation and myocardial infarction, the topical use of TXA has been studied.91,94 A 2021 metanalysis of 609 patients from Boston has shown that topical TXA maintains a higher postoperative haemoglobin, reduced postoperative blood loss (though not significantly intraoperative blood loss), reduced length of stay, drain output, and postoperative transfusion. 87 The dose used within the review varied, however the authors concluded that low dose topical TXA, in the range of 250-500 mg is as effective as 1-3 g when measured by postoperative blood loss. 87
A less commonly used alternative to TXA is epsilon-aminocaproic acid (EACA), a lysine analogue that prevents fibrin degradation. Ramkiran et al showed in a randomised trial of 36 patients that 100 mg/kg leading dose followed by a 10 mg/kg/hr maintenance leads to a 17.7% reduction in blood loss and 45.6% less transfusion, though these results were both inferior to those seen with a TXA dose of 50 mg/kg loading and 10 mg/kg/hr maintenance. 84 A recent metanalysis shows that EACA appears to be a safe, with no significant respiratory or wound complications, though it does appear to be a less effective alternative to TXA. 96
Aprotinin is a protease inhibitor that was initially envisaged for use in hyperfibrinolytic states. However, it was subsequently found to be associated with an increased risk of renal failure myocardial infarction, heart failure and mortality, and as such its use has since been restricted by the Food and Drug Administration. 97 Whilst in use, aprotinin appeared to be as effective at EACA and TXA in reducing intraoperative blood loss, though not effective in reducing postoperative bleeding or incidence of transfusion. 86 Following the early termination of the BART study, which showed higher than expected mortality in aprotinin use in cardiac surgery, it is no longer recommended for use. 98
Transfusion Thresholds
Thresholds for transfusion in adult spine deformity have not been defined, though a serum hemoglobin less than 8-10 g/dL in spine surgery in general is associated with a higher adjusted risk of perioperative morbidity.71,99 Unfortunately, surgery for ASD is often associated with high blood loss, especially in females with a lower starting hemoglobin concentration.100,101 A nadir of <9.0 g/dL leads to a greater change in hemoglobin after surgery, received a postoperative blood transfusion, and have a longer length of stay. 101
Few studies have compared preemptive and reactive approaches to transfusion for ASD patients in the perioperative period and it may be that patients with a lower preoperative hemoglobin concentration benefit from earlier transfusion. Further study is needed to define specific transfusion thresholds based upon patient comorbidities.
Cell Salvage
Cell salvage devices collect intraoperative blood and render it suitable for reinfusion.102,103 Whilst there are no absolute contraindications its use, it is avoided in infection or tumor due to the risk of seeding disease.104-107 Cell salvage has been shown to reduce the incidence of allogenic blood transfusion after deformity surgery by 18-33%; and when transfusion is required, the volume of blood required has been shown to be less by .3-1 unit per patient.108-110 Yang et al carried out an analysis of its use in 124 patients, finding that cell salvage was most effective in avoiding allogenic transfusion when estimated blood loss was 15 mls/kg or less, with declining effectiveness at higher volumes. 111 In a further development, evidence suggests that under 614 mls of blood loss, cell salvage is of no benefit 112 Despite its cost, cell savage has become a mainstay in ASD surgery and provides autologous transfusion to the patient directly in the operating room, saving up to $422 per case. 112 Generally, following filtering, approximately one third of the blood loss volume is reconstituted in a form that is suitable and safe for transfusion.
Surgical Technique
Among the most important factors in blood conservation during spine surgery is surgical technique. Minimizing blood loss requires careful, real-time decision-making, efficiency, and skill. Prior to incision, the surgeon should have a plan for each step of the surgery, including which equipment and hemostatic agents to use. Operative time closely correlates with blood loss and therefore efficiency and elimination of unnecessary delays is critical.113,114
Pre-operative infiltration of epinephrine prior to incision with cautery is effective and shows no increase in wound complications. 115 Anatomical planes and subperiosteal dissection should be used with the diligent use of retractors to prevent oozing, bring good visualization, and limit soft tissue injury to the paraspinal muscles. Bony bleeding can be substantial and can be minimized with hemostatic agents and direct pressure application of bone wax. The surgeon has numerous options from which to choose when performing osteotomy, such as drill bits, osteotomes, punches, or an ultrasonic scalpel, each of which has pros and cons for hemostasis and efficiency. Ultimately, the most important factors in minimizing blood loss are the surgeon’s attention to detail, addressing sources of bleeding and the timely completion of the procedure.
Local Pharmacology
Bone wax, gelatin hemostatic sponges, thrombin, cellulose and fibrin sealants are all used to control local hemorrhage with rare complications.116-118 Hemostatic sponges derived from gelatin, collagen, cellulose or polysaccharides need a functioning coagulation cascade (so may have limited use in the depleted patient) and can swell resulting in neurological compromise.119-124 Others contain fibrinogen and thrombin to actively produce a fibrin clot and are effective in coagulopathy122,125-129 In the future, the relative effectiveness and risks of using each of these needs to be defined.
Postoperative
Drains
Few studies have addressed the role of postoperative drains in ASD patients undergoing surgery for spinal deformity. Across less extensive spinal procedures there is a positive association with perioperative blood loss, transfusion, rates of wound soakage and wound aspirations when drains are used.130,131 The data suggest that patients undergoing surgery for ASD require drainage for a mean of 4.9 days with an average total output of 1.9 L. Complications included deep wound infections in 2.3%, and sterile seroma and hematoma in 1.1% each suggesting that adult spine deformity surgery, especially if accompanied by the use of BMP, may warrant use of postoperative drains. 132
In some settings, retransfusion of the collected blood has been shown to reduce post-operative transfusion by up to 68%, however this does not appear to consistently apply in ASD.133-135 Ultimately, although retransfusion may have a limited role there is little evidence for the role of drains in controlling hemorrhage and their importance in reducing dead space and hemorrhage is not thoroughly understood.
Post-Operative Tranexamic Acid
To date, only a single study has explored the use of TXA after spine surgery. This study suggested that after major spine surgery with osteotomy and decortication, continuous low-dose postoperative TXA was not associated with reduced drain output and there was no increase in the incidence of thromboembolic events. 136 Unfortunately, the dose used in their study was low and a prospective dose response study controlling for intraoperative factors is warranted to establish the safety and efficacy of higher dose postoperative TXA in major spine surgery.
Thromboprophylaxis
Pooled estimates suggest a DVT incidence of 4% and a bleeding risk between .1 and 30% across spine surgery, though a consensus regarding thromboprophylaxis remains absent.137-144 When mechanical and chemical thromboprophylaxis are used in combination, the risk of DVT and PE falls to .7% and .1% respectively. 144 However, thromboprophylaxis is not without risk. When low molecular weight heparin is used, the bleeding related complications occur in 4% of cases, which includes an incidence of compressive epidural hematoma requiring surgery of .30%.142-144
To reduce the risk of symptomatic thrombosis, guidelines suggest an individual assessment of risk and early mobilization.145-147 Only the American College of Chest Physicians specifically advocates for mechanical prophylaxis with additional chemical prophylaxis in high-risk patients.146-149 Future work needs to compare the methods of thromboembolism following deformity surgery. In those patients using antiplatelet or anticoagulant drugs preoperatively, opinions vary. Several guidelines exist, which suggest holding low molecular weight heparin, whereas others suggest no difference in bleeding or postoperative hematoma formation if it is continued.150-152 In a survey of 40 spinal surgeons published in 2018, 55% continued preoperative heparin through the perioperative period, but did stop clopidogrel, rivaroxiban and vitamin K antagonists between 2 and 7 days preoperatively. 153 There appears to be much variation in evidence and opinion in preoperative anticoagulation, which has yet to be resolved.
Managing Anticoagulants
Antiplatelet, coumarins, heparins and direct oral anticoagulants (DOACs) use is endemic amongst patients with ASD. With each drug having a different half-life, balancing the perioperative risk of bleeding with thrombosis can be convoluted.
Two of the most common anticoagulants used are aspirin (a platelet inhibitor) and clopidogrel (an inhibitor of platelet aggregation). Aspirin exerts its irreversible effect within one hour of ingestion whereas clopidogrel takes 24 hours. Both need 7 days to be metabolized. 154 Recent meta-analysis shows that the risk of bleeding is not increased when aspirin is continued through surgery, and if aspirin is stopped, paradoxical withdrawal hypercoagulability can occur.155-157 Both drugs can usually be restarted after 24 hours postoperatively.
Coumarins inhibit vitamin K dependent clotting factors (II, IIV, XI, X, Protein C, Protein S), and are influenced by genetic differences, interactions and serum albumin concentration. Typically, these drugs are stopped at least 5 days preoperatively, however the return of normal clotting needs to be confirmed through laboratory studies.158,159 Warfarin can typically be restarted 24 hours postoperatively provided intraoperative hemostasis is achieved. 160 Intravenous heparin should be stopped 4 hours, subcutaneous at 8 hours and low molecular weight heparin at 24 hours preoperatively. 161 They can usually be restarted at 2, 24 and 24 hours respectively.
The perioperative management of DOACs depends on their indication, individual bleeding risk and characteristics of the individual drug. 162 DOACs are increasingly used because of their low incidence of interactions, predictable onset and offset and the freedom from laboratory monitoring. A common example is Rivaroxaban, a direct factor Xa inhibitor, which starts working 4 hours after ingestion and has an effect for 48 hours. DOACs should be stopped 72 hours preoperatively and can be restarted 6-12 h after surgery in low risk and 48-72 h in high risk of bleeding risk.163,164
Randomized controlled trials regarding managing anticoagulants in ASD surgery are missing and so decisions are left to the treating surgeon. Although guidelines exist, more detailed studies are needed to ensure that surgery is proceeding as safely as possible whilst minimizing the risk of hypercoagulability to the patient. 163
Conclusion
Summary of evidence and recommendation for each blood conservation strategy. IV intravenous; Hb hemoglobin; MAP mean arterial pressure; TXA tranexamic acid; EACA Epsilon-aminocaproic acid; LMWH Low molecular weight heparin; Xa antagonists Factors 10a antagonists.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SJL is a Consultant for Stryker, Medtronic and AOSpine, and receives payment for lectures and travel for meetings from Medtronic, Stryker, AOSpine, L&K and Depuy. The remaining authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.