
Abstract
Study Design:
Retrospective pooled analysis of individual patient data.
Objectives:
Spinal chondroblastoma (CB) is a very rare pathology and its clinicopathological and prognostic features remain unclear. Here, we sought to characterize the clinicopathological data of a large spinal CB cohort and determine factors affecting the local recurrence-free survival (LRFS) and overall survival (OS) of patients.
Methods:
Electronic searches using Medline, Embase, Google Scholar and Wanfang databases were performed to identify eligible studies per predefined criteria. A retrospective review was also conducted to include additional patients at our center.
Results:
Twenty-seven studies from the literature and 8 patients from our local institute were identified, yielding a total of 61 patients for analysis. Overall, there were no differences in clinicopathological characteristics between the local and literature cohorts, except for absence or presence of spinal canal invasion by tumor on imagings and chicken-wire calcification in tumor tissues. Univariate Kaplan-Meier analysis revealed that previous treatment, preoperative or postoperative neurological deficits, type of tumor resection, secondary aneurysmal bone cyst (ABC), chicken-wire calcification and radiotherapy correlated closely with LRFS, though only type of tumor resection, chicken-wire calcification and radiotherapy were predictive of outcome based on multivariate Cox analysis. Analyzing OS, we found that a history of preoperative treatment, concurrent ABC, chicken-wire calcification, type of tumor resection and adjuvant radiotherapy had a significant association with survival, whereas only type of tumor resection remained statistically significant after adjusting for other covariables.
Conclusion:
These data may be helpful in prognostic risk stratification and individualized therapy decision making for patients.
Introduction
Chondroblastoma (CB) is a rare intermediate tumor of cartilage origin, with local aggressiveness as its main biological characteristic. CB most commonly affects the metaphysis of the long bone, with an incidence rate of less than 1% among all bone tumors. 1 The current treatment of choice for CB mainly relies on complete tumor resection. However, due to the locally infiltrative nature, achieving extensive resection of these tumors may be challenging during surgery. In addition, there is presently no effective drug therapy for CB, and radiotherapy may even cause malignant disease. 2 Therefore, recurrence of CB lesions is usually high after surgery, with significantly adverse effect on the long-term quality of life and survival of patients.
Prior studies have shown that the biological behavior of CB affects the clinical outcome of patients and that tumors located at the pelvis and proximal humerus are vulnerable to relapse following surgery.3,4 It has also been reported that patient age and cyst formation correlate significantly with CB recurrence after surgical resection.4-6 Recently, researchers have described the clinical characteristics of cranial CB in adults, finding that residual postoperative lesions were the most important factors affecting the disease recurrence of patients and that radiotherapy conferred no benefits in this population. 7
CB occurring in the spine is a very rare condition, accounting for only 1.4% of all CB cases. 8 Published data have suggested that spinal CB has a more aggressive phenotype and is more likely to relapse than its extremity variant.1,9-11 Although reports on spinal CB have been documented in the literature, most of them are single case reports or small case series. Therefore, the detailed clinicopathological features and complete range of prognostic factors in spinal CB remain unclear. Given the relatively poor prognosis of spinal CB, systematically summarizing its prognostic factors may help guide appropriate risk stratification and subsequent therapeutic optimization, thereby improving patient survival. In this study, we aimed to characterize the clinicopathological data of a large spinal CB cohort and determine predictive factors of local recurrence-free survival (LRFS) and overall survival (OS) of patients.
Methods and Materials
Literature Review
To identify eligible studies in the literature, we searched the MEDLINE, Embase, Google Scholar and Wanfang databases from inception to April 30, 2020. The keywords used were (“chondroblastoma” or “chondroblastomas” or “CB” or “CBs” or “ Codman’s tumor” or “Codman’s tumor”) and (“spine” or “spinal” or “vertebral” or “cervical spine” or “thoracic spine” or “lumbar spine”). To obtain comprehensive outcomes and avoid omissions, no other restrictions for the above search terms were used. Bibliographies of the included studies and existing systematic reviews were also manually checked for any potentially relevant citations that met the criteria. 12 The detailed search strategy is displayed in Figure 1. We included studies involving humans that reported histopathologically confirmed CB cases originally occurring in the spine. The exclusion criteria for the study included the following: CB cases not confirmed by pathological analysis; failing to provide survival data or any patient information; surgical tumor resection not performed.
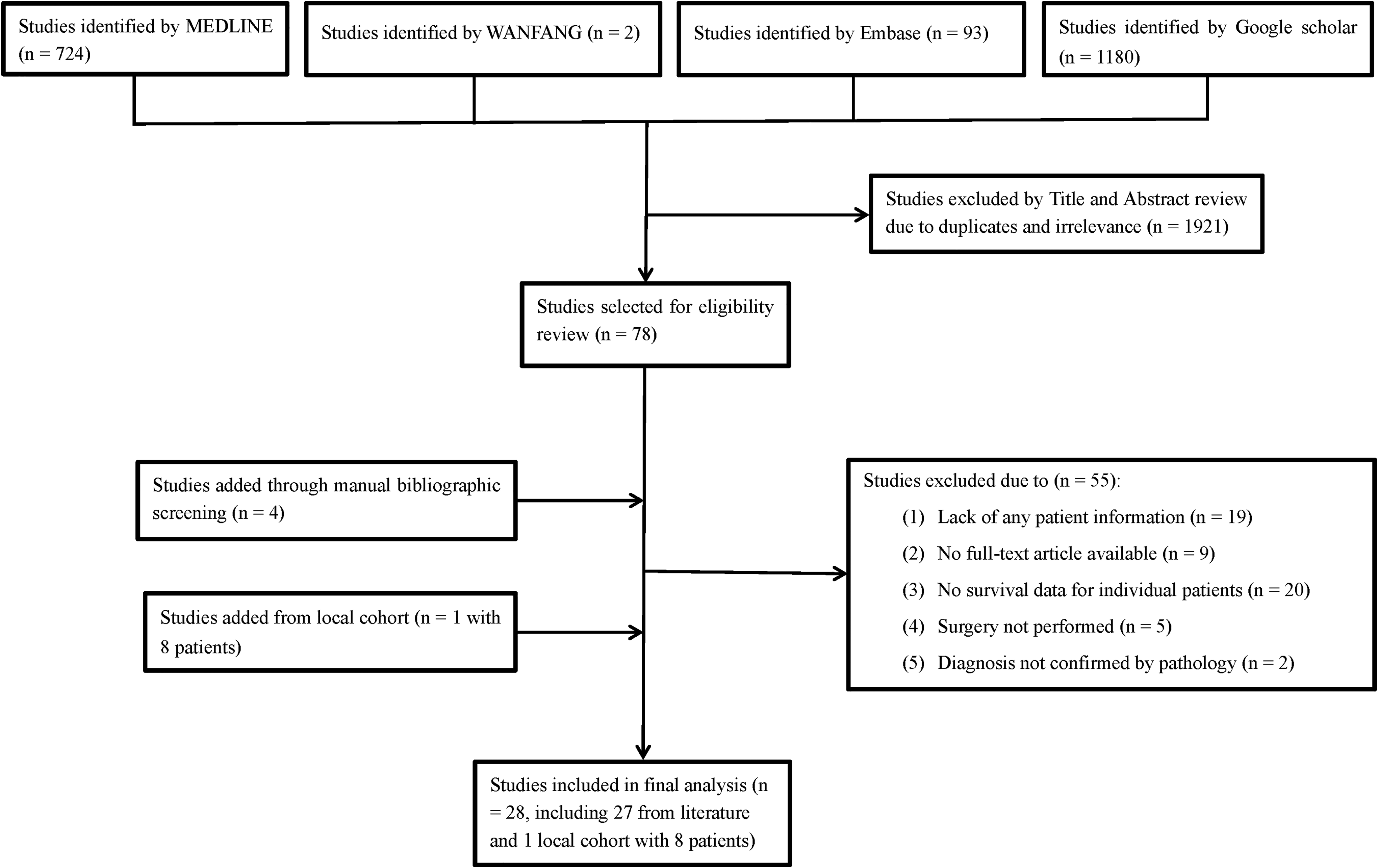
Flow diagram of literature search showing studies identified, included and excluded at each stage.
Two investigators independently selected studies according to the inclusion criteria and extracted clinical data for each patient. This data included the following: patient demographic information (age and sex), clinical characteristics (including duration of symptoms, preoperative and postoperative neurological status, number of segments involved and treatment history), imaging findings (whether the tumor invaded spinal canal), pathological features (whether the tumor had secondary aneurysmal bone cyst [ABC] and chicken-wire calcification]), treatments (such as type of surgery, surgical approach and whether patients received chemotherapy or adjuvant radiotherapy), endpoint events (local recurrence and death) and time to critical events. Discrepancies between the 2 reviewers were resolved through consensus. The primary data of interest was LRFS, which was defined as the time interval from date of surgery to the first local tumor recurrence, and OS, which was recorded as the length of time from tumor resection to death from any cause.
Local Cohort
A retrospective search of the pathology database was conducted to identify eligible spinal CB cases at our institution. This procedure was approved by our hospital ethical committee, and informed consent was obtained from each patient. A total of 8 patients with spinal CB who had undergone curative surgery at our institute between July 2002 and December 2017 were identified. All patients were followed-up with regular clinical and radiological examinations until December 2018. The diagnosis of CB was confirmed by two independent neuropathologists based on histological examination of hematoxylin and eosin-stained sections. Patient and tumor features, treatment history and clinical outcomes were obtained from medical records. Observations were censored when a patient was tumor-free (LRFS analysis) or alive (OS analysis).
Statistical Analysis
The “surv_cutpoint” function in the “survminer” package of R software (version 3.6.2, R Foundation for Statistical Computing, Vienna, Austria) was used to determine cut-off values for patient age and duration of symptoms in survival analysis, with OS as the outcome parameter. 13 Specifically, the cut-off was defined as the point with the minimum P value based on the log-rank test. To avoid overstating the statistical significance, the above P value was corrected according to a previously described method. 14 All other statistical analyses were performed using SPSS 17.0 (SPSS, IBM Inc., Armonk, New York, USA). Continuous data was analyzed by Student’s t test or one-way ANOVA, and the results are expressed as the mean ± standard deviation. Categorical data was analyzed by the chi-square test, and the results are summarized by the frequency or composition ratio. A univariate Kaplan-Meier curve by log-rank test was used to explore the relationship between clinicopathological factors and patient outcomes. A multivariate Cox proportional hazards model was used to assess independent prognostic factors of LRFS and OS after adjusting for other clinical predictors that were significant in our univariate survival analysis. All tests were two-sided, and P < 0.05 was considered to be statistically significant.
Results
Patient and Tumor Features
A total of 61 patients with spinal CB were included, including 8 from our institution and 53 from 27 eligible studies in the literature (Supplementary material).1, 8-11,15-36 The clinicopathological characteristics of the patients are summarized in Table 1. Overall, there were no differences in clinicopathological features between the local and literature cohorts, except for absence or presence of spinal canal invasion and chicken-wire calcification (Table 1). Most studies failed to offer complete clinical data. Age information was available for 54 patients, with an average age of 31.8 ± 15.4 years (range: 9-62 years old). Sex data was available for 58 patients, including 18 female and 40 male patients. Nine patients received therapeutic interventions before surgery. Of them, 4 underwent tumor radiotherapy and 1 open tumor biopsy; 4 were previously treated by surgery. Forty patients did not receive radiotherapy, whereas 12 patients did receive adjuvant radiotherapy, including 4 from our institution (all treated by conventional photon radiotherapy) and 8 reported in the literature (6 had an unknown type of radiotherapy, 1 received conventional photon radiotherapy, and 1 underwent combined conventional photon radiotherapy and cobalt-60 radiotherapy). In addition, we found that all patients (n = 12) who received radiotherapy had not TES resection, while most patients (19/30) who did not have radiotherapy failed to receive TES resection, and this difference was statistically significant (χ2 = 4.215, P = 0.040). Most studies did not provide information on chemotherapy, and this variable was therefore not included in subsequent analysis. The median LRFS of patients was 25 months, and the 1-year, 3-year and 5-year LRFS rates were 74%, 60%, and 41%, respectively. The median OS was 42 months, and the 3-year, 5-year and 10-year OS rates were 86%, 72% and 54%, respectively.
Comparison of Baseline Characteristics Between Literature and Local Spinal Chondroblastoma Cohort (n = 61).a
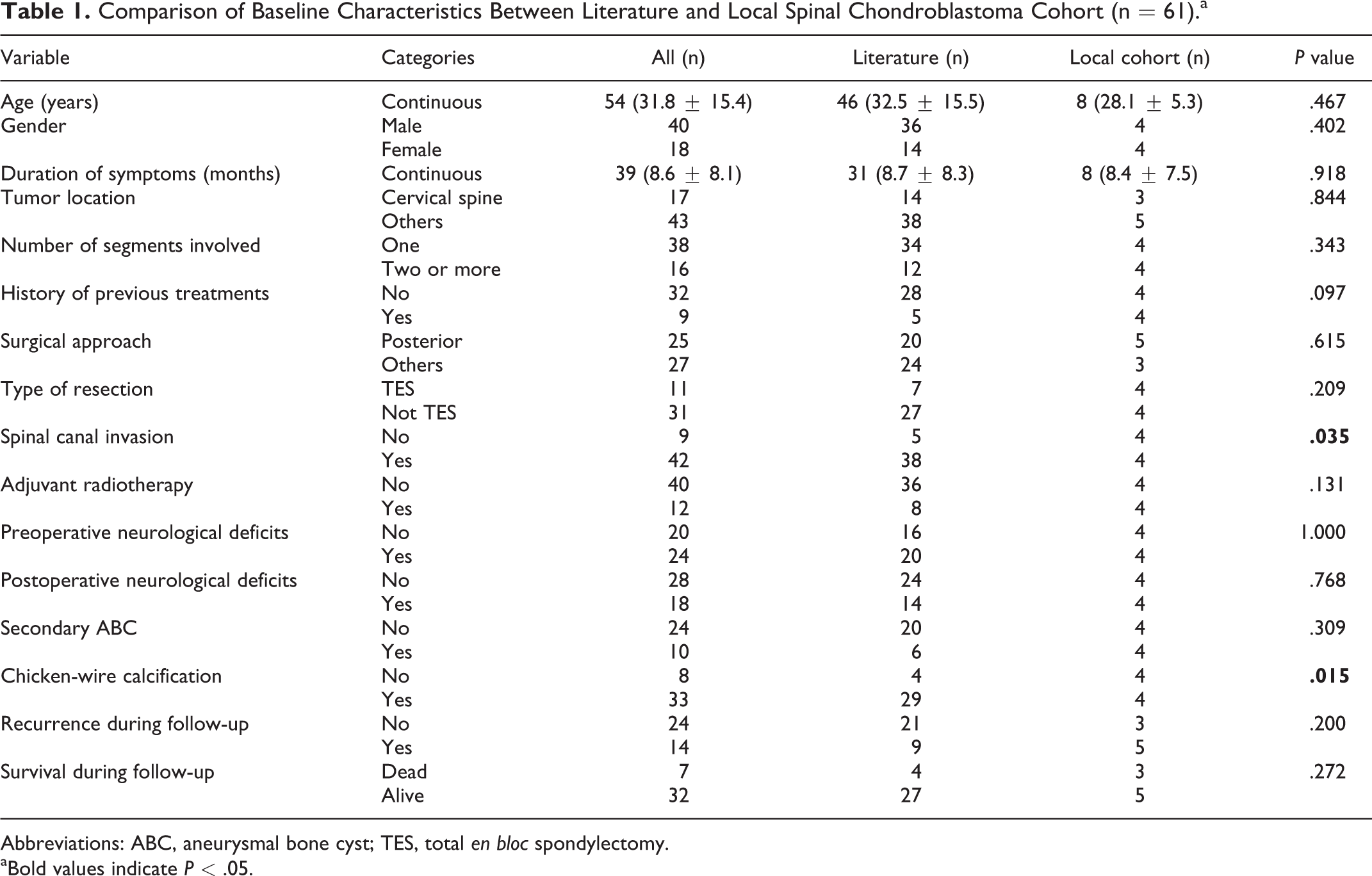
Abbreviations: ABC, aneurysmal bone cyst; TES, total en bloc spondylectomy.
aBold values indicate P < .05.
Univariate Analyses of Prognostic Factors in Patients With Spinal CB
The cut-off values for age and duration of symptoms used for survival analysis are depicted in Figure 2. Patients were divided into low (≤ cutoff) and high (> cutoff) groups according to these cut-off points. Univariate Kaplan-Meier analysis revealed a history of preoperative treatment, tumors with secondary ABC, adjuvant radiotherapy, and neurological deficits before or after surgery to correlate negatively with LRFS (Table 2 and Figure 3). However, patients with tumors harboring chicken-wire calcification and those who received total en bloc spondylectomy (TES) had better LRFS than their counterparts (Table 2 and Figure 3). No statistically significant correlations were observed between other studied variables and patient LRFS (Table 2).
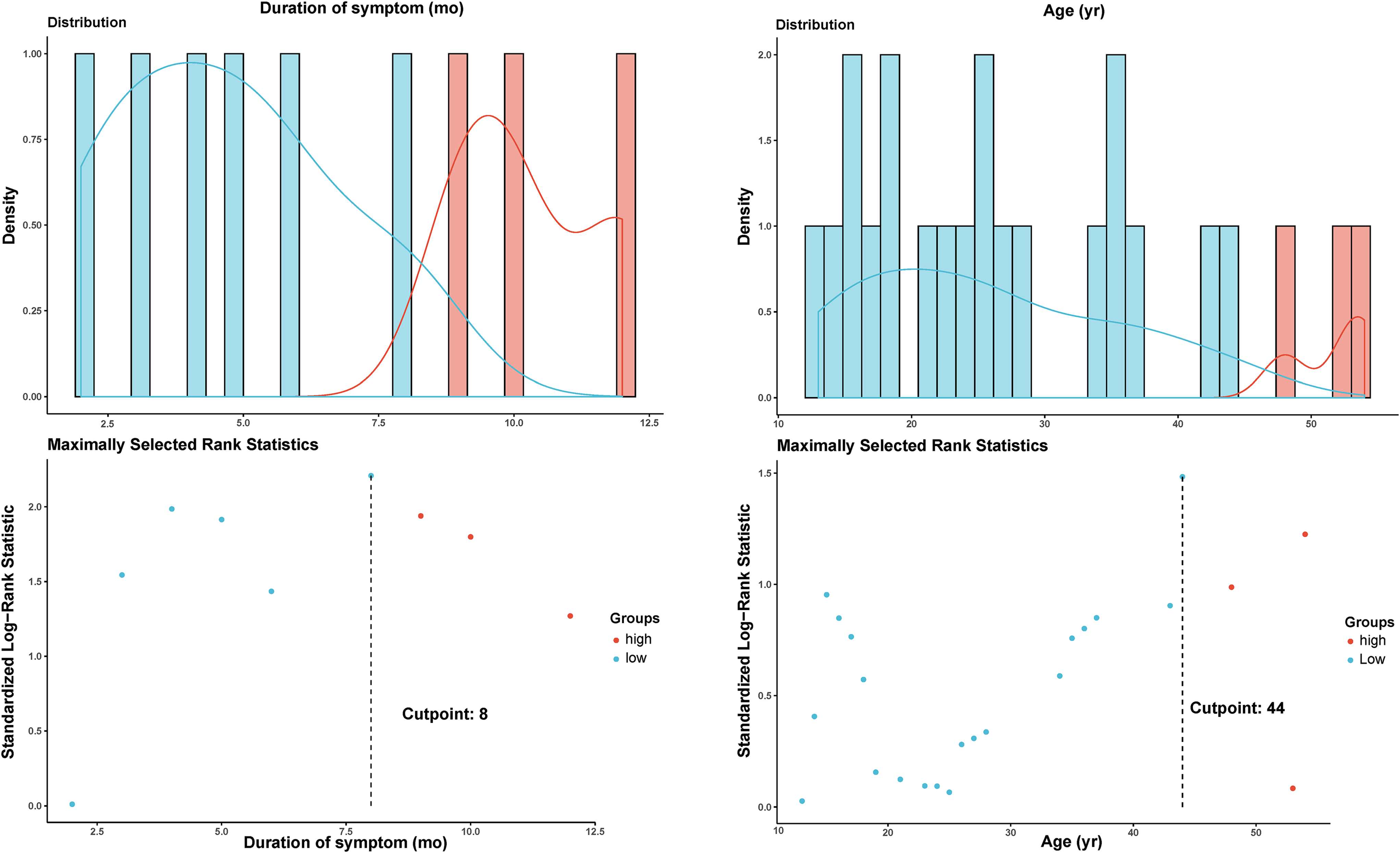
Cut-off determination by using maximally selected rank statistics for duration of symptoms (Left) and patient age (Right) in survival analysis, with the overall survival as the outcome parameter. Patients were divided into high-risk and low-risk groups according to the cut-off values.
Univariate Analyses of Prognostic Factors for Lrfs in Patients With Spinal Chondroblastoma.a
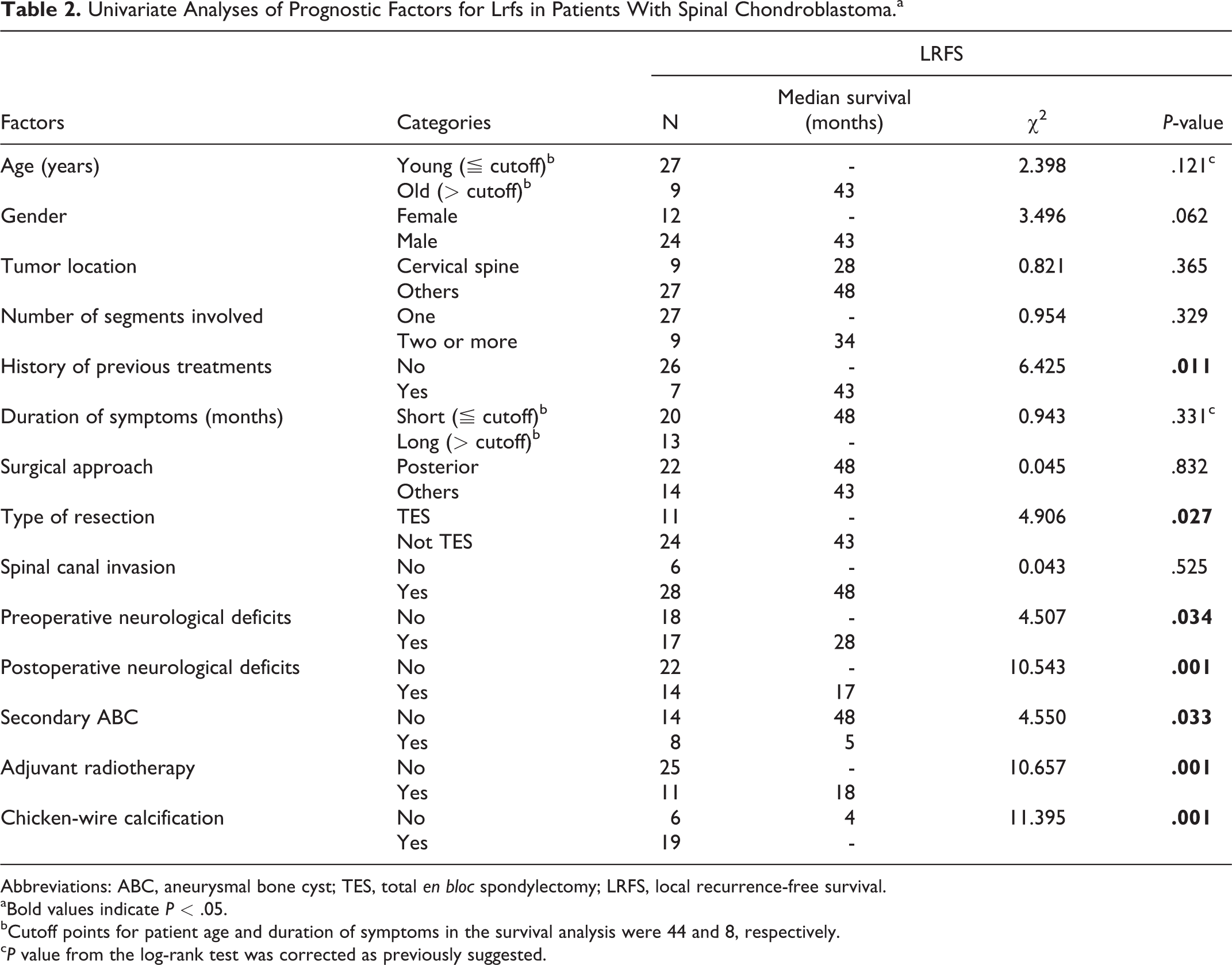
Abbreviations: ABC, aneurysmal bone cyst; TES, total en bloc spondylectomy; LRFS, local recurrence-free survival.
aBold values indicate P < .05.
bCutoff points for patient age and duration of symptoms in the survival analysis were 44 and 8, respectively.
cP value from the log-rank test was corrected as previously suggested.
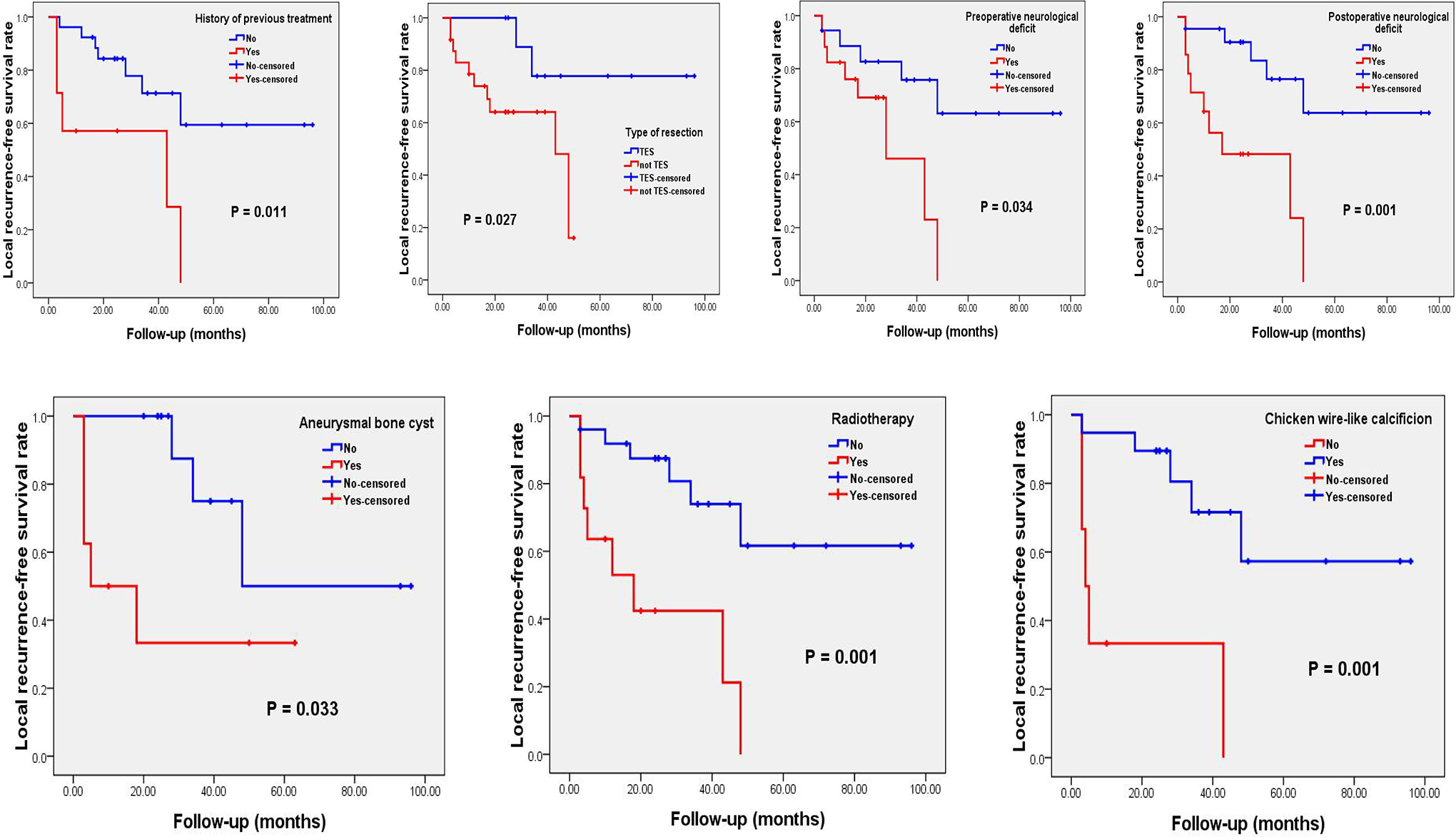
Kaplan-Meier curves of local recurrence-free survival of spinal chondroblastoma patients, stratified by history of previous treatment (P = 0.011 via log-rank test), type of surgical resection (P = 0.027), neurological deficits before surgery (P = 0.034), neurological deficits after surgery (P = 0.001), secondary aneurysmal bone cyst (P = 0.033), adjuvant radiotherapy (P = 0.001) and chicken-wire calcification (P = 0.001).
Similarly, in the analysis of OS, we found that patients having preoperative treatment, secondary ABC and adjuvant radiotherapy experienced shorter survival times than those without these conditions (Table 3 and Figure 4). However, the occurrence of chicken-wire calcification and TES resection of tumors was associated with excellent OS (Table 3 and Figure 4). No statistically significant correlations were observed between OS and other parameters studied (Table 3).
Univariate Analyses of Prognostic Factors for OS in Patients With Spinal Chondroblastoma.a
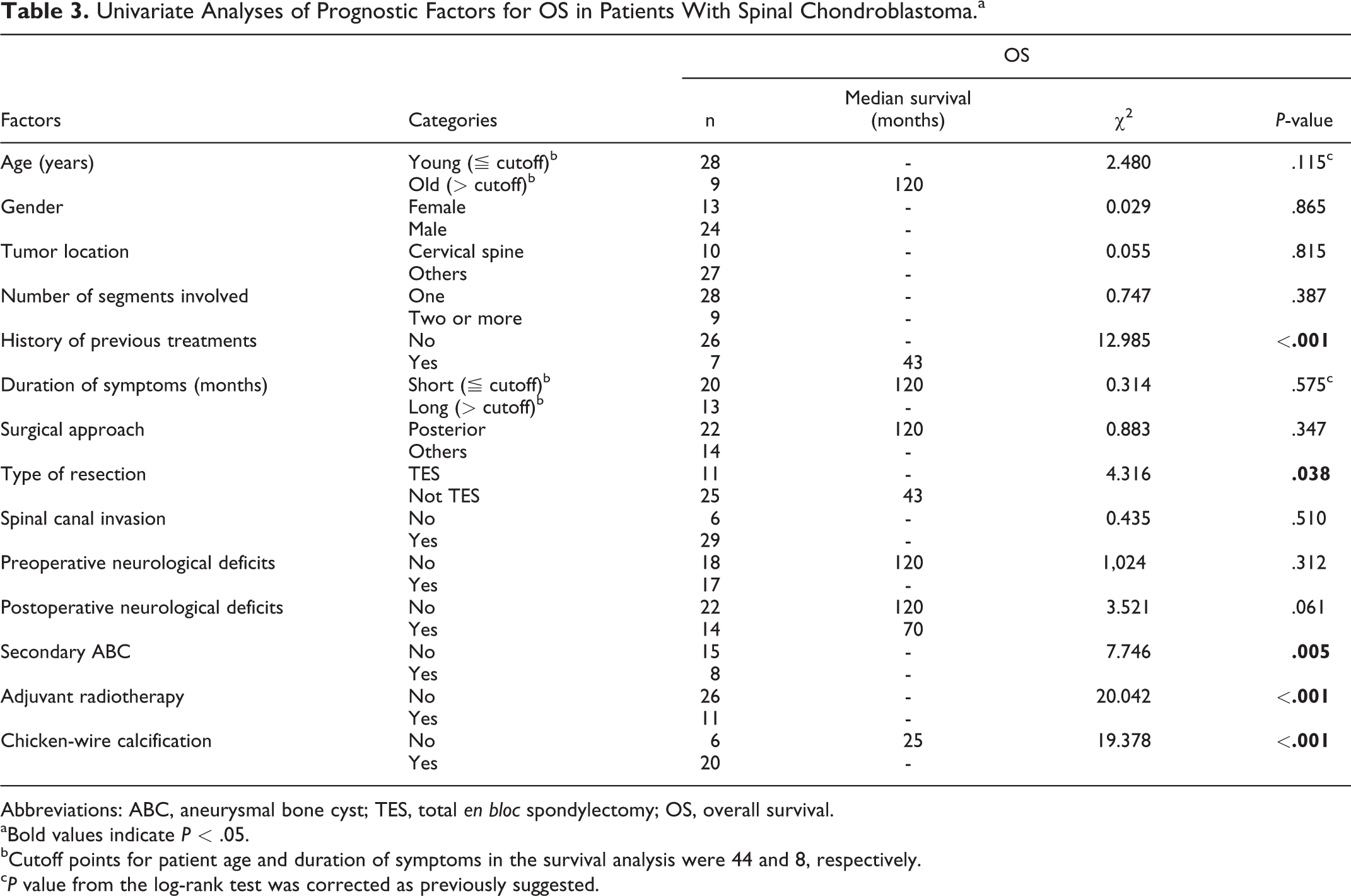
Abbreviations: ABC, aneurysmal bone cyst; TES, total en bloc spondylectomy; OS, overall survival.
aBold values indicate P < .05.
bCutoff points for patient age and duration of symptoms in the survival analysis were 44 and 8, respectively.
cP value from the log-rank test was corrected as previously suggested.
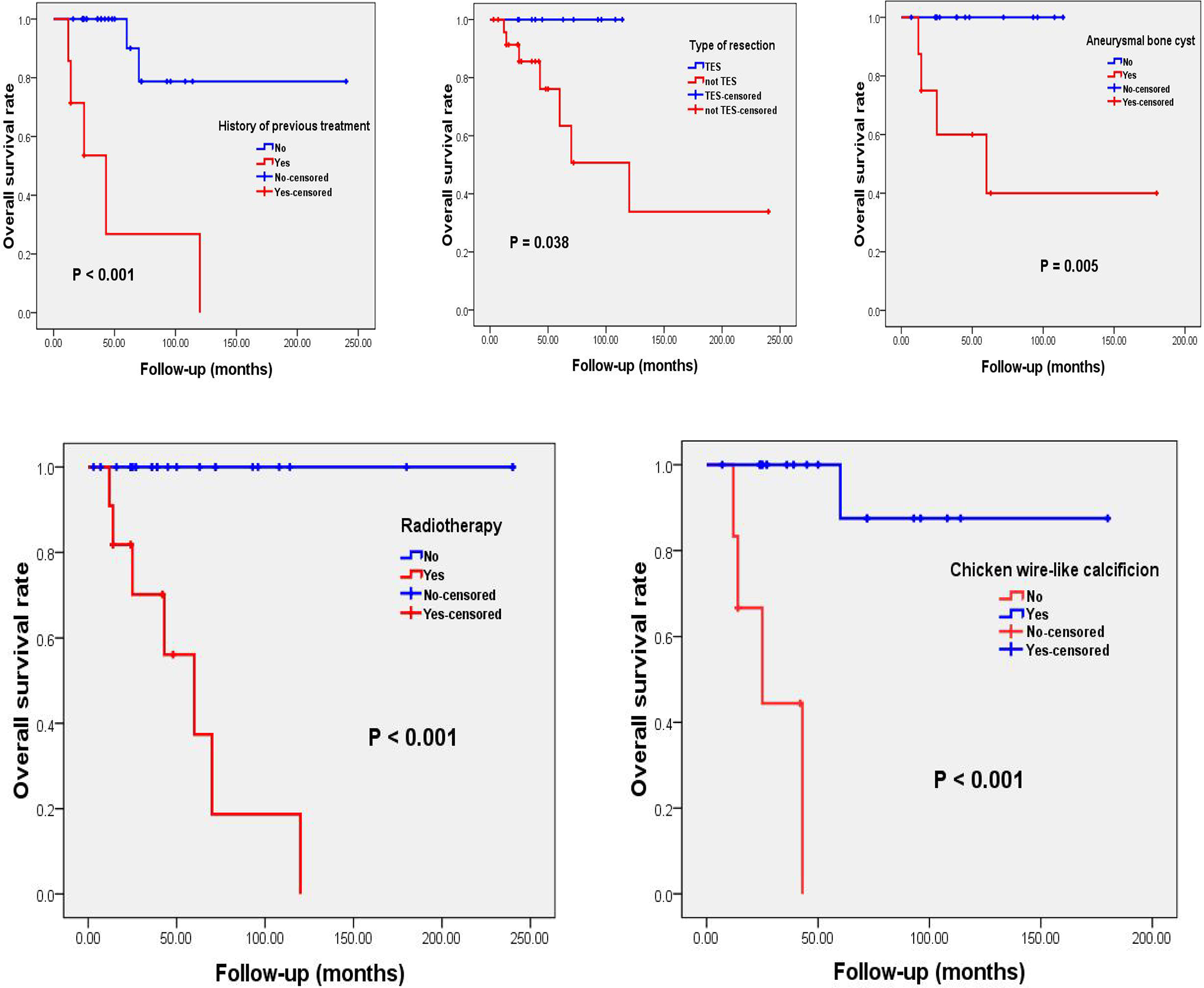
Kaplan-Meier curves of overall survival of spinal chondroblastoma patients, stratified by history of previous treatment (P < 0.001 via log-rank test), type of surgical resection (P = 0.038), secondary aneurysmal bone cyst (P = 0.005), adjuvant radiotherapy (P < 0.001) and chicken-wire calcification (P < 0.001).
Multivariate Analyses of Prognostic Factors in Patients with Spinal CB
Cox multivariate analysis showed that TES resection and the presence of chicken-wire calcification were significantly associated with better LRFS; adjuvant radiotherapy independently predicted poor LRFS (Figure 5). This analysis also revealed that TES resection of tumors was an independent predictor of good OS (Figure 6).
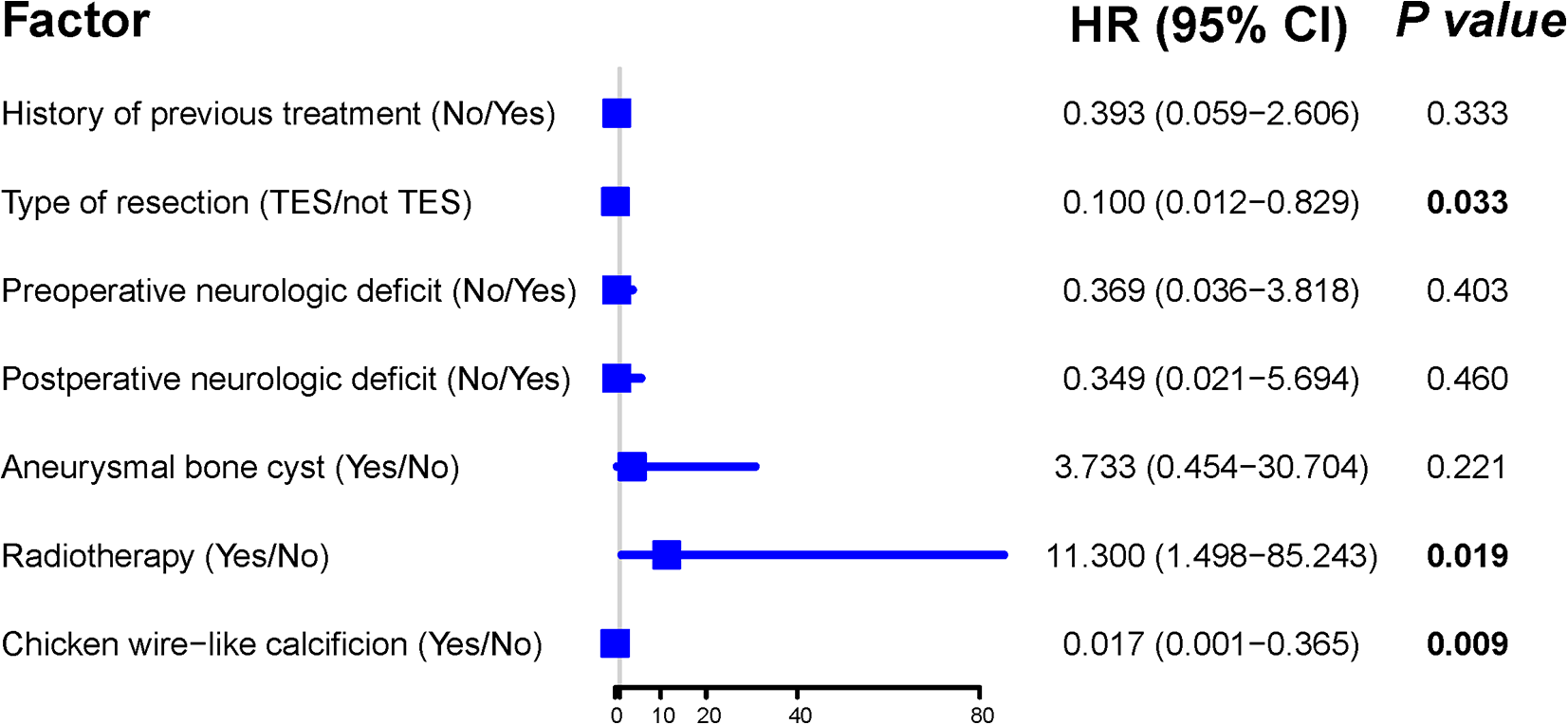
Multivariate Cox regression model for local recurrence-free survival of patients with spinal chondroblastoma.
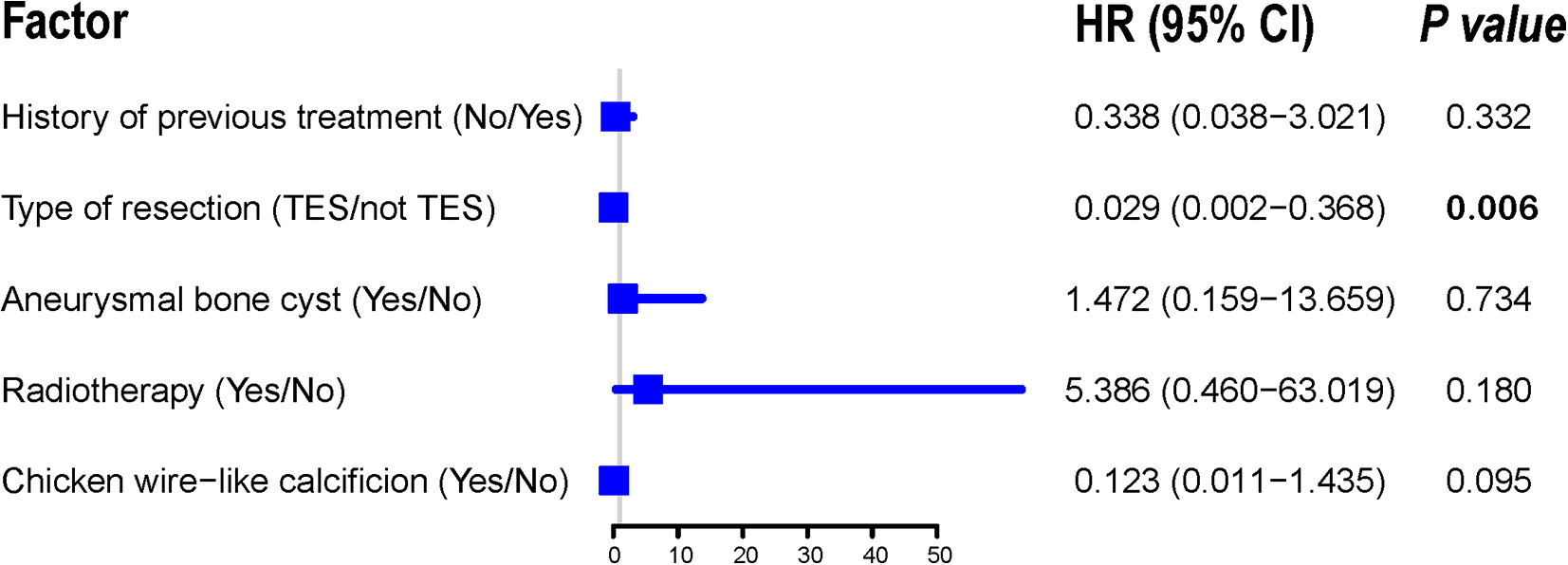
Multivariate Cox regression model for overall survival of patients With spinal chondroblastoma.
Discussion
In this study, we performed an integrated analysis of the clinicopathological characteristics and prognostic factors in a large number of spinal CB patients. We found that a history of preoperative treatment, tumor resection pattern, neurological status before and after surgery, adjuvant radiotherapy, and absence or presence of secondary ABC and chicken-wire calcification in CB tissues were closely related to LRFS and/or OS of patients. Although the type of tumor resection could independently predict both LRFS and OS, adjuvant radiotherapy and chicken-wire calcification were the only independent prognostic factors for LRFS. These data may contribute to a comprehensive understanding of the prognostic characteristics in spinal CB and may also be helpful in prognostic risk stratification and personalized therapy decision making for patients.
Our study revealed that patients with neurological deficits had shorter LRFS than those who were neurologically normal. This result can be explained by the fact that the occurrence of neurological defects may hint at a wide extent of tumor infiltration or the proximity of tumors to key nervous structures, for which it can be difficult to achieve complete resection, with a consequent increase in tumor recurrence after surgery.7,15 In addition, neurological dysfunctions and other related complications in these patients may compromise their antitumor immune response and promote tumor relapse.37-39
The presence of chicken-wire calcification in eosinophilic cartilage-like matrix is not uncommon in CB, 40 and this tissue feature also has diagnostic value.5,41 Interestingly, our study revealed that the appearance of chicken-wire calcification in spinal CB tissues portended good clinical outcomes, similar to findings in the literature reporting that calcification correlates positively with the overall survival of colorectal cancer patients after chemotherapy. 42 By contrast, however, in an analysis of 103 cases of extracraniofacial CB, the authors found that chicken-wire calcification had no significant effect on patient survival. 5 This inconsistency may be caused by the different tumor locations analyzed and the small sample size in our study, thus leading to low statistical power. Calcification primarily manifests as the deposition of calcium salts and minerals in nature. Previous studies have shown that osteopontin is involved in regulation of the calcification process. 43 Moreover, it has been confirmed that osteopontin can promote the growth, invasion and metastasis of various malignant tumors. 44 Based on this data, we speculate that the relationship between spinal CB calcification and encouraging patient outcome may be attributed to the downregulation of osteopontin expression in tumor tissues and the resulting less aggressive phenotype. Our future study will measure the expression of osteopontin in CB tissues and investigate its effect on the biological behavior of this tumor. In addition, our analysis found a significantly shorter survival for spinal CB patients with secondary ABC. This finding was in agreement with a literature report, claiming an increased risk of tumor recurrence after surgery under this condition. 45 One possible explanation is that CB combined with ABC may generate a more aggressive disease, which further aggravates bone destruction and accelerates tumor invasion into surrounding tissues, 3 thus leading to poor outcomes. Noticeably, our multivariate analysis did not find secondary ABC to be an independent prognostic factor of clinical outcomes (Figure 5 and Figure 6), suggesting that the effect of other variables on CB prognosis could be greater than this parameter.
As spinal CB is usually aggressive,17,23,24 surgical treatment is necessary in clinical practice.5,10,20 However, studies have pointed out that the risk of tumor recurrence can be high when residual CB lesions remain after surgery. 7 Therefore, to reduce postoperative recurrence and achieve good disease control, most researchers currently recommend removing the tumor tissue as completely as possible.5,10,20 This is consistent with our findings, showing that complete tumor resection was linked with favorable LRFS and OS of patients. A recent study on spinal CB reported similar results. 15
Another major finding of this study was that adjuvant radiotherapy seemed to promote spinal CB progression and thus reduce patient survival. Similarly, several studies have demonstrated that radiotherapy failed to improve CB prognosis and might even induce malignant transformation of the tumor to sarcoma.2,7,15 Nonetheless, most of the included studies did not provide detailed radiotherapy data for patients, which may distort the true effect of radiotherapy on patient outcomes. Furthermore, previous observations have also shown that radiotherapy does not accelerate spinal CB progression, 26 and it has been suggested that radiotherapy may be a treatment option for patients with postoperative disease recurrence and those who cannot be treated with surgery. 9 Additionally, it should be noted that the poor survival for patients with radiotherapy in our study could be likely caused by the fact that they were all treated by not TES resection. Given these findings, we believe that future studies with large samples (especially including more patients who received radiotherapy) and complete radiotherapy data are strongly needed to clarify the impact of adjuvant radiotherapy on spinal CB prognosis. Published data have proven that radiotherapy can induce senescence-like changes in tumor-associated fibroblasts, which are able to sustain an active tumor microenvironment and promote tumor progression. 46 Additionally, it has been suggested that radiation therapy can cause the formation of new stem cells from malignant tissues.47,48 Altogether, this data may provide an explanatory basis for the worse survival of patients undergoing radiotherapy in this study. Subsequent studies using single-cell transcriptomics sequencing with tumor tissue samples of spinal CB patients before and after radiotherapy may be helpful in disclosing the precise mechanism by which radiotherapy impacts CB progression.
In addition, our study found that a history of preoperative treatment could significantly affect clinical outcome. This phenomenon is easy to understand, considering that preceding radiotherapy can induce biological malignancy of the tumor 2 and that previous tumor resection may lead to residual lesions and unclear tumor borders. Both situations can make subsequent treatments difficult, thereby resulting in poor patient survival. However, it should be noted that most studies did not record the specific treatment options the patients received before surgery; therefore, we were not able to evaluate the relationship between the type of treatment approaches and spinal CB prognosis.
Limitations
In this study, we included two different cohorts (one from literature and the other from local institute) to present clinical characteristics of spinal CB, which may have introduced heterogeneities into the pooled analysis. We did this because spinal CB is a rare entity and collecting sufficient data for analysis in a single institute is challenging. In fact, this method is currently widely used in the literature and is an effective tool especially for the investigation of rare disease. Nevertheless, to reduce the heterogeneities between studies, allow for comparability and then enable statistical analysis, we obtained complete and objective patient information (this data cannot have variations among studies, such as age, sex, duration of symptoms, etc.), and also simplified criteria for subjective variable grouping in subsequent analysis (only divided into yes or no for most categorical variables). Moreover, most of the included studies did not provide incomplete clinicopathological information for patients, which may lead to bias in our results. In addition, not including Cochrane Library in our literature search may lead to omission of relevant citations. Finally, our current study was still not able to define the prognostic role of adjuvant radiotherapy in CB as we only included a small number of patients with radiotherapy who were all treated by not TES resection. Future prospective studies with large samples and complete patient data are still needed to confirm the current findings.
Conclusions
The present study involved a pooled analysis of the prognostic factors in a large number of spinal CB patients. We found that treatment history, neurological function, type of tumor resection, adjuvant radiotherapy, and absence or presence of secondary ABC and chicken wire-like calcification were closely associated with patient outcomes. This data may be helpful in prognostic risk stratification and in guiding therapeutic optimization for patients.
Supplemental Material
Supplemental Material, sj-doc-1-gsj-10.1177_21925682211005732 - Clinicopathological and Prognostic Characteristics in Spinal Chondroblastomas: A Pooled Analysis of Individual Patient Data From a Single Institute and 27 Studies
Supplemental Material, sj-doc-1-gsj-10.1177_21925682211005732 for Clinicopathological and Prognostic Characteristics in Spinal Chondroblastomas: A Pooled Analysis of Individual Patient Data From a Single Institute and 27 Studies by Bo-Wen Zheng, Wei Huang, Fu-Sheng Liu, Tao-Lan Zhang, Xiao-Bin Wang, Jing Li, Guo-Hua Lv, Yi-Guo Yan and Ming-Xiang Zou in Global Spine Journal
Footnotes
Acknowledgments
We thank Dr. Yi Jiang and Dr. Xiao-Ling She from Department of Pathology, The Second Xiangya Hospital, Central South University for pathological analysis of the study. We also thank American Journal Experts for assistance in preparation of this manuscript.
Author Contribution
All authors participated in data acquisition. BWZ, GHL, JL and MXZ contributed to the conception and design of the study. BWZ, WH, TLZ and MXZ did the data analysis and interpretation. BWZ, WH, YGY, TLZ, XBW and MXZ contributed to drafting and revision of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (81 802 211 to XBW, 81 871 821 to JL and 82 002 364 to MXZ), Natural Science Foundation of Hunan Province (2019JJ50542 to TLZ) and Project for Clinical Research of Hunan Provincial Health Commission (20 201 978 to TLZ and 20 201 956 to MXZ).
Ethics Approval and Consent to Participate
The study protocol was approved by the Institutional Review Board at The Second Xiangya Hospital, Central South University, Hunan, P.R. China. Written informed consent was obtained from each patient for publication of this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.