
Abstract
Study Design:
A retrospective case-control study.
Objective:
Only a few studies have studied the incidence of new-onset SI joint pain following lumbar spine fusion surgery. We aimed to explore the association between new-onset SI joint pain following Transforaminal Lumbar Interbody Fusion (TLIF) for degenerative spine disorders and changes in spinopelvic parameters.
Methods:
A retrospective review of hospital records and imaging database of a tertiary care institute was done for patients who underwent TLIF from October 2018 to October 2019. The 354 patients who satisfied the eligibility criteria were divided into 2 groups(Group A, new-onset SI joint pain group, n = 34 and Group B, normal controls, n = 320). Symptomatic relief (>70% reduction in the VAS [Visual Analogue Scale] score) after 15 minutes of SI joint injection was considered diagnostic of SI joint pain. Clinical and radiological spinopelvic parameters were compared between the 2 groups.
Results:
Patients with postoperative SI joint pain (Group A) had significantly less preoperative and postoperative lumbar lordosis (p < 0.001) compared to the other group. Most of the patients in Group A had a cephalad migration of the apex postoperatively (30/34 patients) whereas majority of patients in group B had either predominant caudal migration (44/320 patients) or no migration of the lumbar apex (272/320 patients).
Conclusions:
The preoperative and postoperative lumbar lordosis are significantly less and the postoperative pelvic tilt is significantly high in patients with new-onset SI joint pain compared to the control group. The cephalad migration of the lumbar apex is significantly associated with new-onset SI joint pain.
Introduction
Chronic low back pain after spine surgery is a diagnostic and therapeutic challenge to a spine surgeon. Failed back syndrome is a term used to characterize chronic back/leg pain following a spine surgery. 1 Failed back syndrome can have numerous causes such as residual or recurrent disc herniation, persistent postoperative compression of a spinal nerve, altered joint mobility, joint instability, postoperative myofascial pain development, scar tissue (fibrosis), spinal muscular deconditioning, and psychosocial factors.2-4 Studies have reported 10% to 40% incidence of persistent pain following spine surgery.5-11
SI joint is the largest axial joint in the body and serves to transmit forces from the upper body to the lower limbs. 12 The movement within the SI joint is minimal. However, the joint is richly innervated and minimal strain to the joint may trigger pain. 13 SI joint has been identified as a potential pain generator in 1905 but has not been given enough attention later. 14 Lumbar spinal fusion can result in changes in the spinopelvic profile of the patient and undue stresses on the surrounding structures which include the SI joint. 15 Biomechanical studies also showed increased stress on the SI joint following lumbar fusion. 16 However, only a few studies have studied the incidence of new-onset SI joint pain following lumbar spine fusion surgery. Unoki et al. 17 in 2016 observed an incidence of 10.7% of new-onset SIJ pain in patients who had lumbosacral fusion. Yu Chau Lee et al. 18 in 2019 found a 12% incidence of new-onset SIJ pain following fusion. None of the studies have attempted to explore the association between new-onset SI joint pain and changes in spinopelvic parameters following Transforaminal Lumbar Interbody Fusion (TLIF).
Methodology
We aimed to explore the association between new-onset SI joint pain following lumbar spine fusion surgery for degenerative spine disorders and changes in spinopelvic parameters. The study has been conducted following the Principles of Helsinki. Informed consent has been obtained from all the patients involved in the study. A retrospective analysis of hospital records and imaging database of a tertiary care institute for patients who underwent TLIF surgery from October 2018 to October 2019 was performed. No institutional review board approval was necessary for retrospective studies conducted at the place of the study. The selection criteria included patients who had no preoperative suspected/confirmed sacroiliac joint pain, who underwent a primary TLIF surgery involving L4-L5/L5-S1 levels for degenerative spinal disorders, and whose follow-up details were available for at least 6 months postoperatively. Patients with documented neurological deficits/ cauda equina syndrome were excluded from the study. The included patients were divided into 2 groups Group A: Patients who had clinically suspected new-onset sacroiliac joint pain within 6 months postoperatively and confirmed by symptomatic relief with sacroiliac joint injections. Group B: Patients who had no clinical suspicion of sacroiliac joint pain or those who had no relief with sacroiliac joint injections.
Evaluation of SI joint pain:
Clinical suspicion of postoperative SI joint pain was based on symptomatic back pain around the SI joint region with sitting intolerance/ difficulty turning around in bed and positive examination findings (local SI joint tenderness, Patrick test/FABER, Yeoman test). Clinically suspected patients were offered sacroiliac joint injections using a 22-gauge spinal needle and injection of intraarticular 1 cc bupivacaine and 40 mg Triamcinolone acetonide. The dimple at the top of the buttock indicates the position of the posterior superior iliac spine (Figure 1). The needle was inserted laterally and at a distance of 1.5 to 2.5 cm from S2 (the second sacral vertebra), at an oblique lateral angle of 45 degrees, and passed between the sacrum and the ilium until ligamentous resistance is felt. The injection was considered diagnostic of SI joint pain if the patient had symptomatic relief (>70%) after 15 minutes of the injection. The SI joint injections were repeated after 1 week if the symptoms recur after an initial symptomatic relief for a maximum of 3 injections.
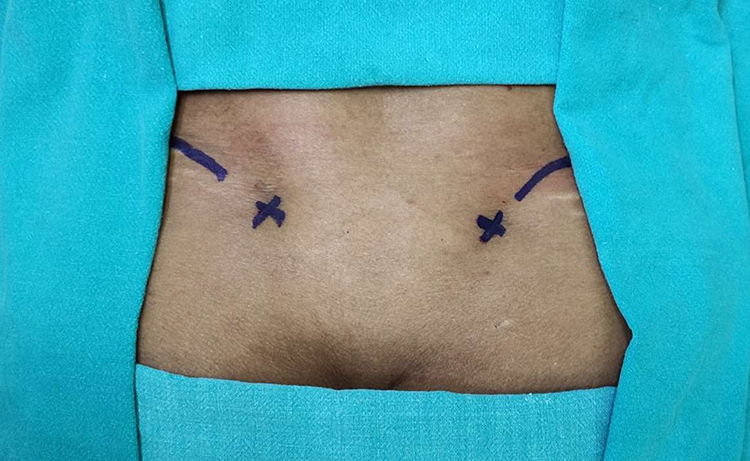
A clinical image of a patient’s lower back with markings showing the border of the iliac crest and the PSIS (marked with ‘x’). The dimple also corresponds to the PSIS. The needle is directed laterally at an oblique angle of 45 degrees.
Demographic details such as age and sex, type of surgery, VAS of back pain(preoperative and postoperative at each follow-up), location of pain(Back, buttock, thigh, leg), side(right, left, bilateral), time of presentation(in postoperative days), physical examination findings, relief with SI joint injections, number of SI joint injections given, preoperative and postoperative spinopelvic parameters such as pelvic incidence, sacral slope, pelvic tilt, total lumbar lordosis, and location of the lumbar apex(LLA) were calculated for both the groups(Figure 2). Radiological measurements were performed by 2 independent spine surgeons (>3 years of experience) and the average of the measurements considered for the analysis.
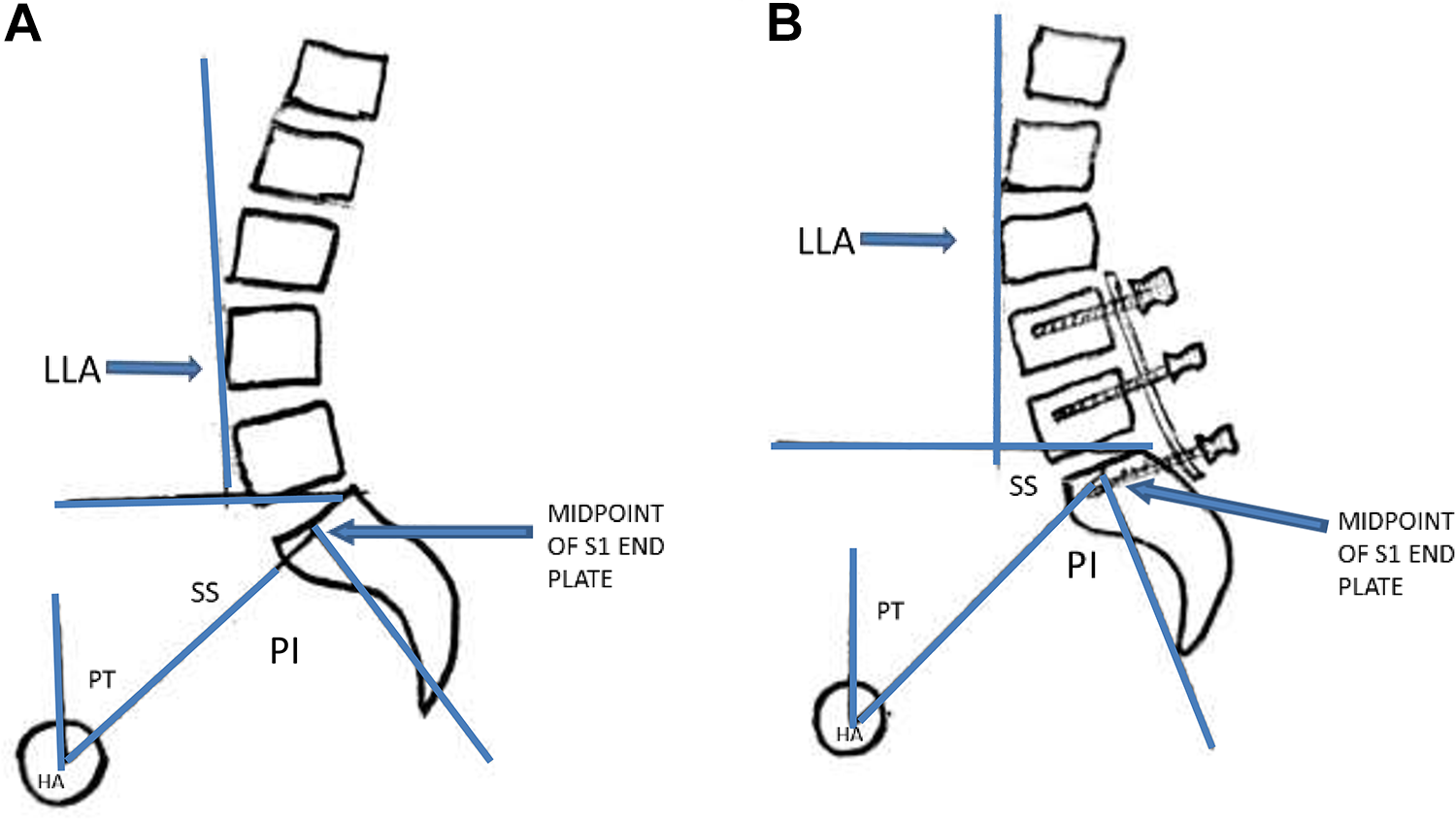
Illustrations depicting the pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), hip axis (HA) and location of lumbar apex (LLA). A vertical line drawn touching the most anterior part of the lumbar curve is used to identify the LLA. In figure 1a, the LLA was located at the body of L4. In figure 1b, after a 2 level TLIF, the LLA was shifted to the body of L3.
Statistical Analysis
Summary results on continuous measurements are presented as mean and standard deviation (SD) (Min-Max) and summary results on categorical measurements are presented as numbers (n) and percentages. Chi-square/Fisher exact test has been utilized to find the significant association between the study parameters of categorical scale. Independent samples t-test /Mann Whitney U-test has been utilized to find the significance of parameters on a continuous scale between 2 groups as per the distribution of data. Statistical analysis was performed using IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp. Statistical significance is assessed at a 5% level.
Results
354 patients who underwent TLIF and satisfied the selection criteria were included in the analysis (Figure 3). 34 patients (9.6%) had documented new-onset sacroiliac joint pain postoperatively within 6 months (Group A) and 320 patients were included under Group B.
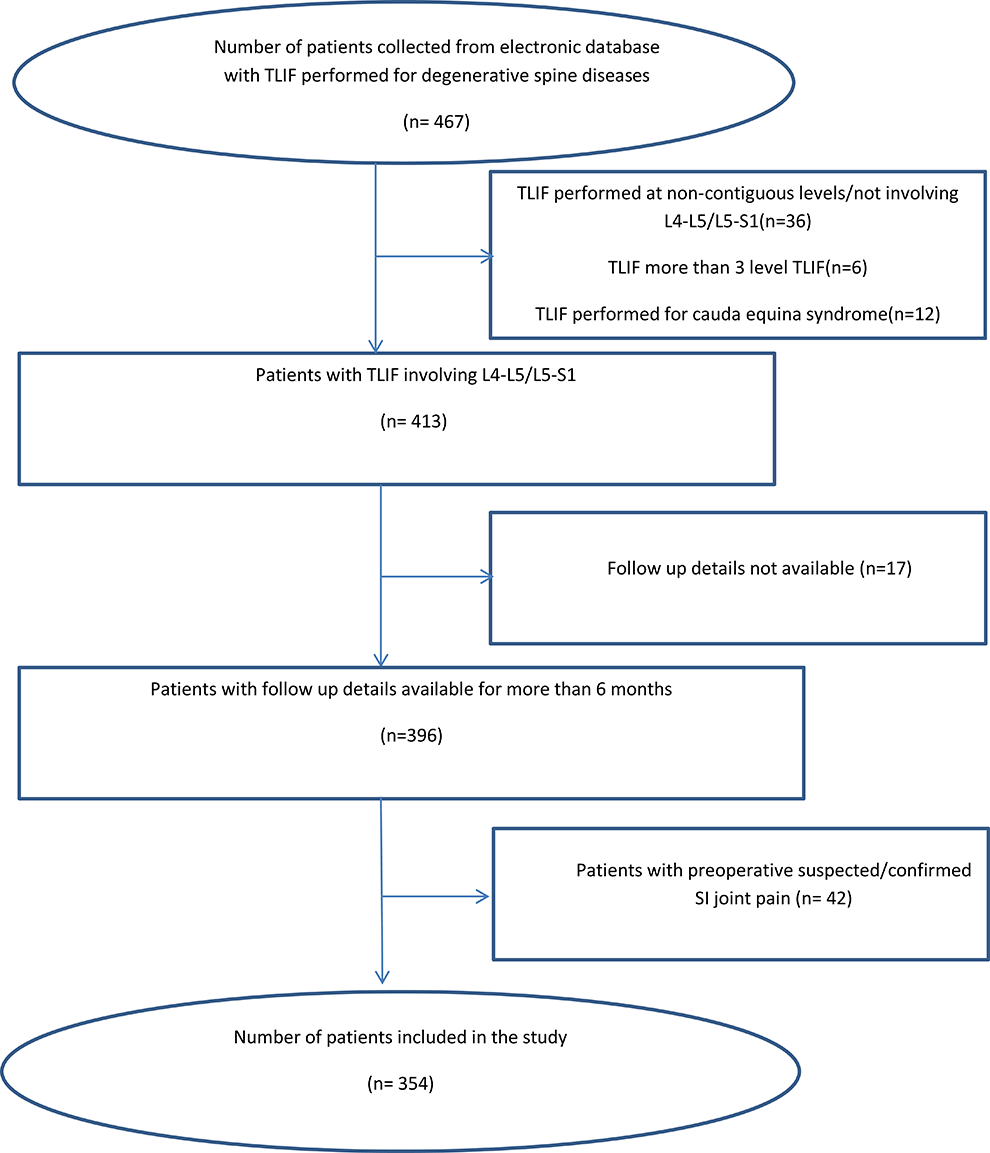
Flow chart followed for patient selection in the study.
The mean (± SD) age of the patients (211 males,143 females) was 63.21±7.5 years. There was no difference in the age distribution between the 2 groups (p = 0.359). The comparison of variables between the 2 groups has been provided in Table 1.
Comparison of Various Parameters in Patients Who Underwent TLIF Between The Patients With Postoperative SI Joint Pain and Normal Controls.a
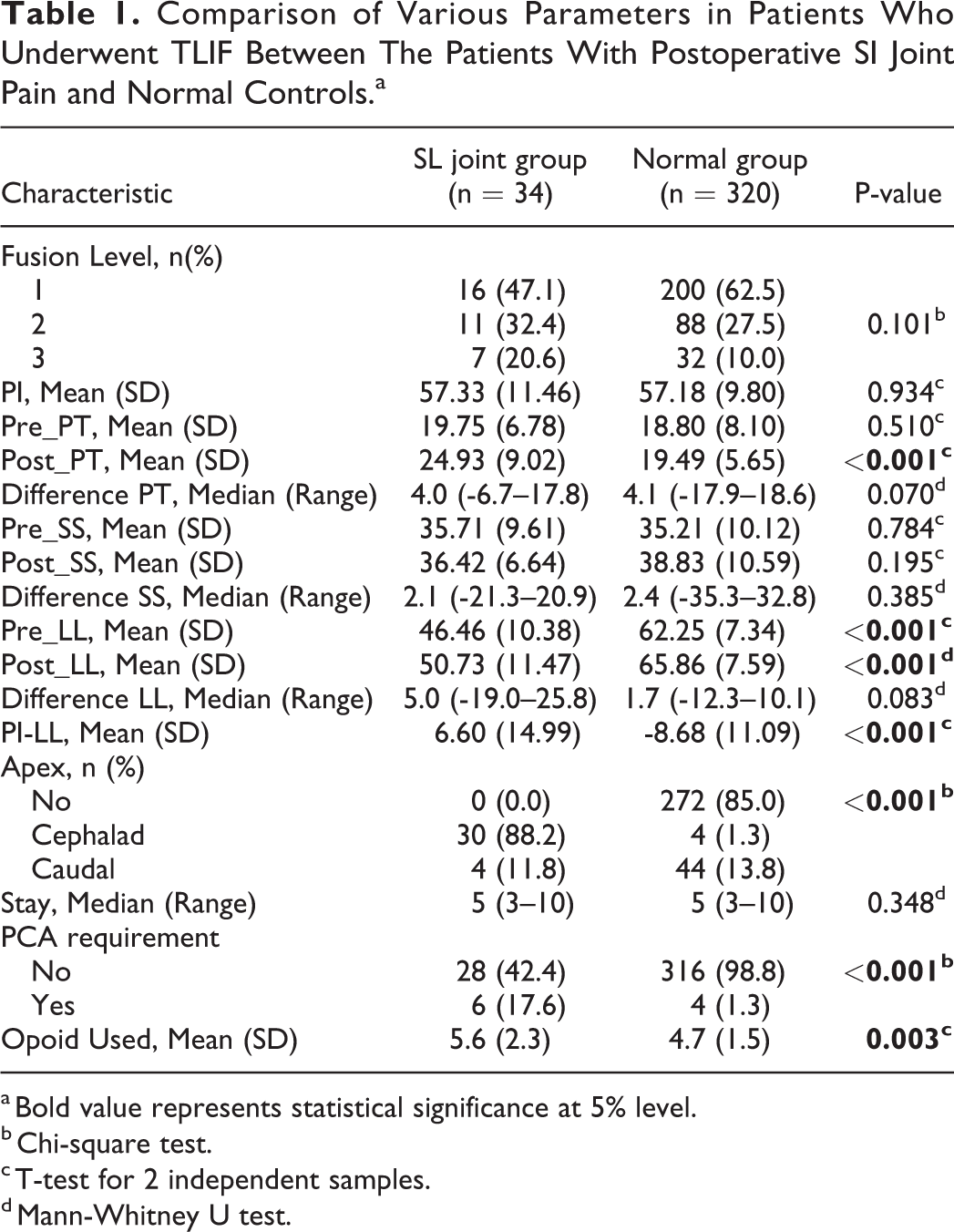
a Bold value represents statistical significance at 5% level.
b Chi-square test.
c T-test for 2 independent samples.
d Mann-Whitney U test.
The Number of Fusion Levels
216 patients underwent a one-level TLIF (L4/L5 or L5/S1), 99 patients underwent 2 levels TLIF and 37 patients underwent 3 levels TLIF. The number of fusion levels was not significantly different between those who had postoperative SI joint pain versus those who did not.
Spino-Pelvic Parameters
Patients with postoperative SI joint pain (Group A) had significantly less preoperative and postoperative lumbar lordosis (p < 0.001) compared to the other group. However, both the groups had similar magnitudes of change in lordosis after surgery (p = 0.083). The patients in Group A had a greater postoperative pelvic tilt (PT) compared to Group B (p < 0.001). Other spinopelvic parameters were not significantly different between the 2 groups. Though mean PI-LL values were <9 degrees in both groups, patients with SI joint pain had significantly higher values compared to the other group (p < 0.001).
Location of LLA
The LLA changed postoperatively in all the patients in group A whereas 272 patients in group B had no change in LLA postoperatively (p < 0.001). Patients with postoperative SI joint pain had a predominant cephalad migration of the LLA postoperatively (30/34 patients) whereas the other group had predominant caudal migration (44/320 patients) or no migration of the LLA(272/320 patients) postoperatively.
Morbidity
The mean hospital stay was not significantly different between the 2 groups (p = 0.348). However, patients with postoperative SI joint pain had a greater requirement of PCA (p < 0.001) or opioids (p = 0.003).
Discussion
A proper evaluation of preoperative and postoperative spinopelvic parameters can guide the treating surgeon to identify the patients at risk for postoperative SI joint pain and help in better management of the condition. We observed that preoperative lumbar lordosis was significantly less in patients with new-onset SI joint pain after TLIF compared to normal controls. However, the change in lumbar lordosis after TLIF was not significantly associated with new-onset SI joint pain. Also, a cephalad migration of the LLA was found to have a significant positive association with new-onset SI joint pain.
Our incidence of new-onset SI joint pain after fusion surgery (9.6%) is less compared to the previously reported studies by Unoki et al 17 (10.7%) and Lee et al 18 (12%). SI joint has been reported as a major source of pain in failed back syndrome. Patients may be treated surgically for radiological findings of lumbar canal stenosis/intervertebral disc prolapse when the origin of the pain is located in the SI joint. This can be a reason for persistent pain after spine surgery. Also, new-onset sacroiliitis can also be a source of pain postoperatively. Katz et al. 19 reported that sacroiliitis was the cause of persistent back pain after lumbosacral fusion in 32% of patients. In another study by Maigne et al, 20 35% of patients with persistent symptoms after spinal fusion originated from the SI joint. We excluded patients with preoperative SI joint pain through a careful clinical evaluation by a team of experienced spine surgeons. Hence, the possibility of missing a preoperative SI joint pathology is minimal.
Another possible cause of SI joint pain after lumbar fusion surgery is the increased stress on the adjacent segments after lumbar or lumbosacral fusion surgery. In such a case, a longer segment fusion should possibly cause more stress on the SI joint. Ivanov et al 16 in their biomechanical study reported that a longer construct led to greater stress at the SI joint. However, Lee et al 18 reported that there was only a marginal difference in the incidence of SI joint pain between 1 level fusion compared to >/- 4 level fusion. We observed that the number of fusion levels did not have any significant association with the incidence of new onset SI joint pain. Bone grafting from the PSIS has also been reported to be a cause for postoperative SI joint pain because of the damage to posterosuperior sacroiliac ligaments. 21 None of our patients underwent harvesting of bone graft from PSIS.
In our study, preoperative pelvic tilt was similar but the postoperative pelvic tilt was significantly higher in the SI joint group compared to the normal controls. These findings have also been reported by Shin et al 21 after posterior lumbar interbody fusion surgeries. The increased pelvic tilt is a compensatory mechanism at the spine and pelvis used to maintain the sagittal balance of the spine. The increased pelvic tilt is reported to result in greater energy expenditure, pain, and poor surgical outcomes. Lazennec et al 22 also reported that increased pelvic tilt was associated with increased postoperative pain.
We observed that both preoperative and postoperative lumbar lordosis are significantly lesser in patients with postoperative SI joint pain compared to the normal controls. Loss of lumbar lordosis has been reported to have a close relationship with back pain after fusion. 23 Shin et al 21 found no association between lumbar lordosis and SI joint pain. Loss of lumbar lordosis is a part of the disease process and has been reported to result in pain and sagittal imbalance. Hence, increased strain on the spinopelvic construct could be a possible reason for the SI joint pain. However, the reason for the manifestation of SI joint pain postoperatively only is not clear. Surgery could have acted as a trigger leading to further weakening of back musculature.
The relationship of the LLA to the onset of SI joint pain has not been reported previously. Recent studies have reported that it is essential to understand the detailed contour of lumbar lordosis rather than the overall lumbar lordosis.24-26 The LLA can change the shape of the lumbar spine.24-26 Roussouly et al 24 proposed a classification of various shapes of the lumbar spine with varying LLA. Identification of the proper LLA is essential to recreate the lumbar alignment. The significance of cephalad migration of the LLA in 88.2% of patients in the SI joint group compared to just 1.3% of patients in the normal group is yet to be established. Since the fusion surgeries addressed the lower arc of lumbar lordosis, improper restoration of lumbar lordosis at these levels during surgery may have resulted in cephalad migration of the LLA (Figure 2 and 4). Hence, addressing the segmental lordosis in addition to the overall lumbar lordosis may reduce the chance of new-onset SI joint pain.
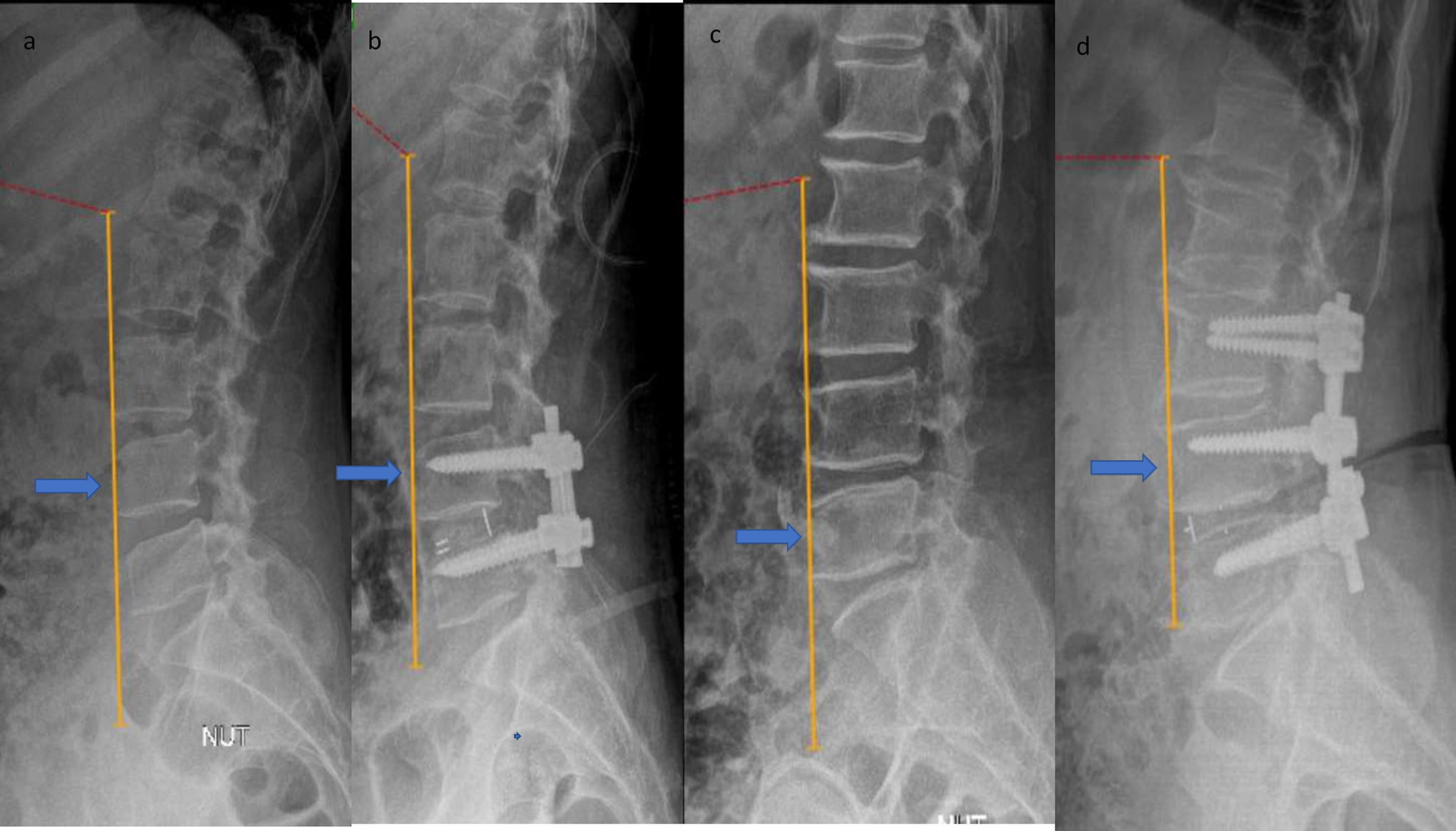
Preoperative(3a) and postoperative(3b) X rays of a patient who underwent a single level TLIF. The LLA was maintained at L4 in both the images and the patient had no new onset SI joint pain. Preoperative(3c) and postoperative(3d) X rays of a patient who underwent a 2 level TLIF. The LLA was located at L5 preoperatively and shifted to L4 postoperatively. The patient had new onset SI joint pain postoperatively and underwent 3 SI joint infiltrations.
Various techniques have been described in the literature to administer SI joint injections. Fluoroscopy, computed tomography (CT), magnetic resonance imaging (MRI), and Ultrasound are various modalities to administer guided SI joint injections to improve the success rates of gaining intraarticular location.27-29 Unguided sacroiliac injections have also been reported as an easy and effective treatment for SI joint pain. 30 However, fluoroscopy remains the gold standard for administering SI joint injections. We have given unguided SI joint injections to all the patients included in our study. Performing fluoroscopic guided SI joint injections may have altered the outcomes of our study.
Limitations
There are some limitations to the study. There may be a false positive analgesic response to the SI joint injection. However, the mean(+/-SD) number of injections was 1.82(+/-1.03) which meant that more patients underwent more than one SI joint injection. This improves the diagnostic accuracy of the injections. Also, errors in radiological measurement of spinopelvic parameters are possible.
Conclusions
New-onset SI joint pain is a common cause of morbidity after TLIF surgery with an incidence of 9.6%. The preoperative and postoperative lumbar lordosis are significantly lesser and the postoperative pelvic tilt is significantly higher in patients with new-onset SI joint pain compared to those who do not have postoperative SI joint pain. The cephalad migration of the LLA is significantly associated with new-onset SI joint pain.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.