
Abstract
Study Design:
Systematic review.
Objectives:
We performed this systematic overview on overlapping meta-analyses that analyzed the role of platelet-rich plasma(PRP) in enhancing spinal fusion and identify which study provides the current best evidence on the topic and generate recommendations for the same.
Materials and Methods:
We conducted independent and duplicate electronic database searches in PubMed, Web of Science, Embase, Cochrane Database of Systematic Reviews, and Database of Abstracts of Reviews of Effects till October-2020 for meta-analyses that analyzed the role of PRP in spinal fusion procedures. Methodological quality assessment was made using Oxford Levels of Evidence, AMSTAR scoring, and AMSTAR 2 grades. We then utilized the Jadad decision algorithm to identify the study with highest quality to represent the current best evidence to generate recommendations.
Results:
3 meta-analyses fulfilling the eligibility criteria were included. The AMSTAR scores of included studies varied from 5-8(mean:6.3) and all included studies had critically low reliability in their summary of results due to their methodological flaws according to AMSTAR 2 grades. The current best evidence showed that utilization of PRP was not associated with significant improvement in patient-reported outcomes such as Visual Analog Score for pain compared to the standard fusion procedure. Moreover, PRP was found to be associated with lower fusion rates.
Conclusion:
Based on this systematic overview, the effectiveness of PRP as a biological agent in augmenting spinal fusion is limited. Current evidence does not support the use of PRP as an adjuvant to enhance spinal fusion.
Keywords
Introduction
Spinal fusion remains the most commonly done operative procedure in the spine for treating spinal fractures, degenerative diseases, and deformity correction. 1 Despite its common use, around 10% of the patient experience fusion failure resulting in pseudoarthrosis which remains a serious complication. 2 Variety of measures have been employed to augment the spinal fusion rates. Despite improved instrumentation and fusion techniques, 3 allogenic bone products, and bone graft extenders were also used as a scaffold to enhance the fusion rates. 4 However, apart from using these scaffolds, to further enhance the fusion rates, biologics with osteoinductive potential such as mesenchymal stem cells (MSCs), recombinant bone morphogenic proteins (rhBMPs), and platelet-rich plasma (PRP) were used in the regenerative regimen to enhance fusion.5-7
Based on various preclinical and in-vitro studies,8,9 PRP has been considered as an autologous product with an array of growth factors such as platelet-derived growth factor (PDGF), transforming growth factor (TGF), insulin-like growth factor (IGF), epidermal growth factor (EGF), epithelial cell growth factor (EGR), and hepatocyte growth factor (HGF) with osteoinductive properties.10-12 PRP has been efficaciously used in various medical specialties like dermatology, oral dentistry, sports medicine, and ophthalmology.13,14 But the use of PRP to enhance spinal fusion has been a topic of debate. Kubota et al. 15 performed a randomized controlled trial and found the PRP group to attain a higher posterolateral lumbar fusion rate compared to the control group. Similarly, Tarantino et al. 16 in their prospective cohort study established the osteoinductive effect of PRP by using a cancellous bone substitute soaked with PRP for posterolateral fusion procedure. On the other hand, Feiz-Erfan et al. 17 performed a double-blinded RCT with platelet-gel concentrate and did not find a consistent effect in enhancing the anterior cervical fusion rate compared to the controls. Similar inconsistency was also noted in a prospective study by Jenis et al. 18 in using autogenous growth factors in the lumbar spinal fusion procedure.
Recently, multiple meta-analyses have been published in this regard analyzing the effectiveness of PRP in enhancing spinal fusion.19-21 However, these overlapping meta-analyses further added to the controversy due to their inconsistent results and conflicting conclusions because of the variability in the primary studies included for meta-analysis. Every meta-analysis suffered from a limited pooled sample size. The objective of this systematic overview of the overlapping meta-analyses is to generate recommendations on the use of PRP in spinal fusion procedures from available literature. Discordant systematic reviews have a major impact on developing guidelines. They add up to confusion. We have used Jadad Decision algorithm, an adjunct decision tool, to resolve such conflicts and arrive at the best possible evidence from the available literature. This study also identifies the potential limitations in the existing literature and help directing future research.
Materials & Methods
We present herewith a systematic overview which was being performed by duly cohering to the guidelines of the Back Review Group of Cochrane Collaboration 22 and aim to report the same based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 23
Search Strategy
Two reviewers conducted an independent literature search for systematic reviews with meta-analysis evaluating the role of PRP in spinal fusion. Electronic database search was conducted in PubMed, Web of Science, Embase, Cochrane Database of Systematic Reviews (CDSR), and the Database of Abstracts of Reviews of Effects (DARE) till October 2020. Our search was neither restricted to any particular language nor confined to a specific period. We designed our electronic search strategy following the Peer Review of Electronic Search Strategy (PRESS) guidelines. 24 The major keywords used for the search were as follows: “PRP”, “Platelet-Rich Plasma”, “Spine”, “Fusion”, “Spinal Fusion”, “Randomized Controlled Trial”, “Systematic Review”, “Meta-analysis” together with Boolean operators such as “AND”, “OR” and “NOT”. We made a manual search of the key journals and also searched the reference list of the selected articles to identify studies not identified in the primary search. We also made a search in the International prospective register of systematic reviews (PROSPERO) for any ongoing potential review that is nearing completion on the subject. We included and analyzed all the studies meeting the inclusion criteria. Any discrepancy between the reviewers was resolved through discussion until a consensus was obtained.
Eligibility Criteria
Reviews were included if they satisfied the following criteria. Systematic review with a meta-analysis that analyzed the role of PRP in spinal surgeries. Should have analyzed at least one of the outcomes such as the fusion rate, time to fusion, fusion density, pain relief using measures like the Visual Analog Scale (VAS) score, functional outcome using scores like the Oswestry Disability Index (ODI) and adverse events.
Exclusion Criteria
We Excluded narrative reviews, correspondence articles, systematic reviews without data pooling or meta-analysis, systematic reviews with mixed intervention groups being analyzed. Besides, we excluded pre-clinical studies, studies on animal models, and cadaveric studies on the subject.
Data Extraction
Data were extracted from the meta-analysis included in the analysis by 2 reviewers independently. Notably, the data extracted from the studies were as follows: first author, date of last literature search, year and journal of publication, number, and nature of studies included, language restrictions, inclusion/exclusion criteria, databases involved in literature search, software used for analysis, whether subgroup or sensitivity analysis, Grading of Recommendations Assessment, Development, and Evaluation (GRADE) summary, publication bias analysis, conflict of interest, I2 statistic value of the variables in each meta-analysis. Disagreements were settled by consensus.
Quality Assessment
The methodological quality of the included reviews was evaluated using the Oxford Levels of Evidence. 25 Besides, we also used the Assessment of Multiple Systematic Reviews (AMSTAR) 26 and its updated grading tool AMSTAR 2 27 to assess their methodological robustness with good validity and reliability. 28 Two reviewers independently assessed the methodological quality of the included studies. Disagreements were settled by consensus.
Heterogeneity Assessment
I2 test was used for heterogeneity assessment. 29 When I2 > 50% and p < 0.1, heterogeneity is deemed to exist among the included trials and the reviewers evaluated whether the studies have utilized sensitivity or subgroup analysis to assess the causes of heterogeneity and strengthen the robustness of the pooled data.
Application of Jadad Decision Algorithm
The variability in the findings among the included meta-analysis was interpreted with the help of the Jadad decision algorithm as shown in Figure 1. As per Jadad et al., 30 the possible reasons for discordance in the results among the included studies include differences in study question, their inclusion and exclusion criteria, assessment of quality, data pooling and extraction, and statistical analysis. Currently, this is the commonly used algorithm for generating recommendations among the meta-analysis with discordant results.31-34 Two reviewers independently used this algorithm to arrive at a single meta-analysis which represents the current best evidence to generate recommendations.
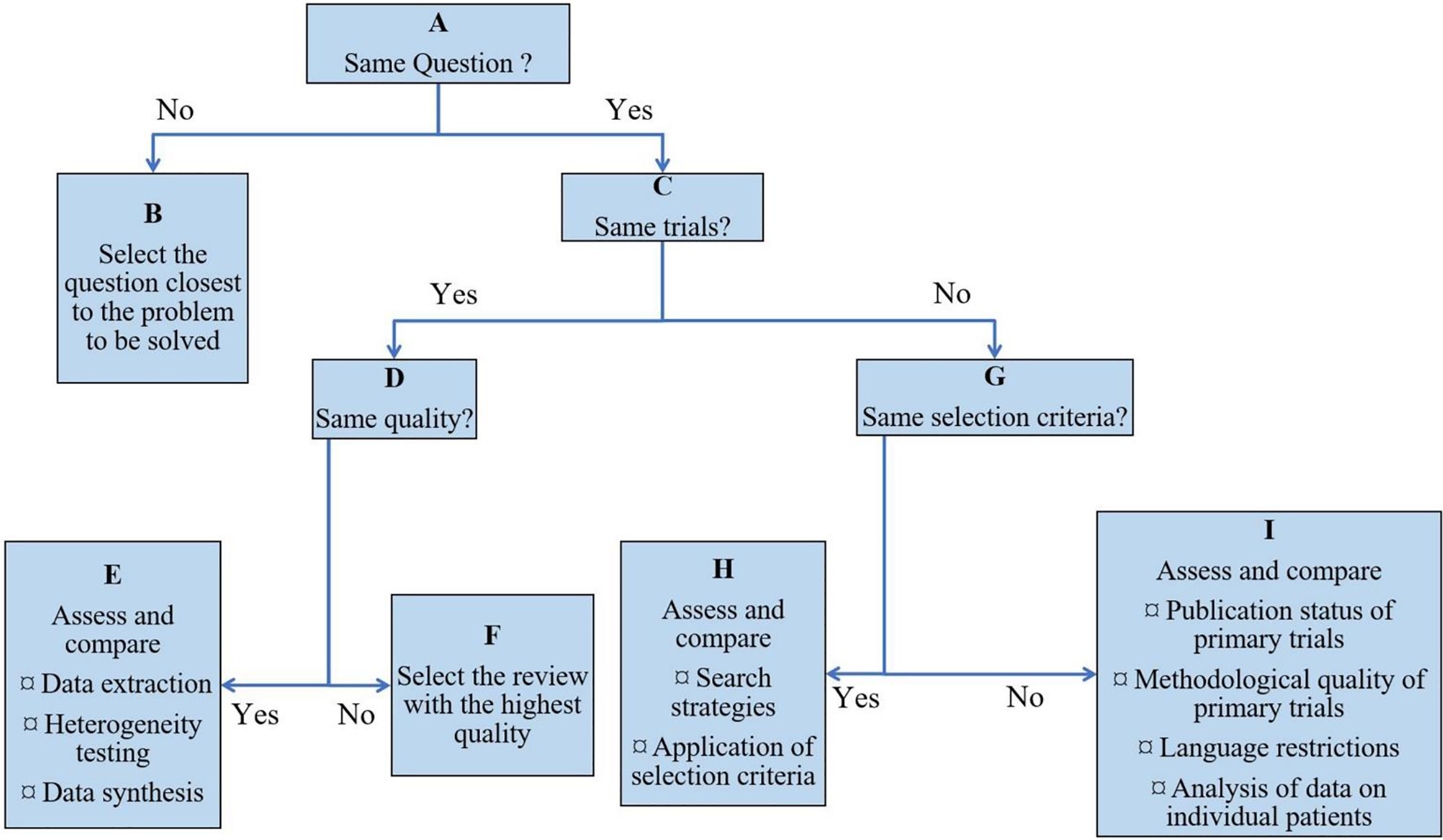
The Jadad decision algorithm.
Results
Search Results
A comprehensive search of the electronic database generated 64 articles and they were subjected to an initial screen for removing duplicate articles which resulted in 48 articles. Upon title and abstract screening of the resultant 48 articles, we excluded 42 articles. Therefore, 6 articles qualified for reviewing the full-text. On full-text review by both the reviewers 3 of them were excluded. A list of excluded articles with reasons was given in Supplementary File 1. Finally, 3 meta-analyses were included in this systematic overview.19-21 These overlapping meta-analyses were published in different journals in 2020 and the number of included studies ranged from 11 to 14 as shown in Table 1. The publication years of the included studies in these meta-analyses ranged between 2003 and 2019 as shown in Table 2. A PRISMA flow diagram for study selection into the systematic overview has been depicted in Figure 2.
Characteristics of the Included Studies.

Primary Studies Included in Each Meta-Analysis.
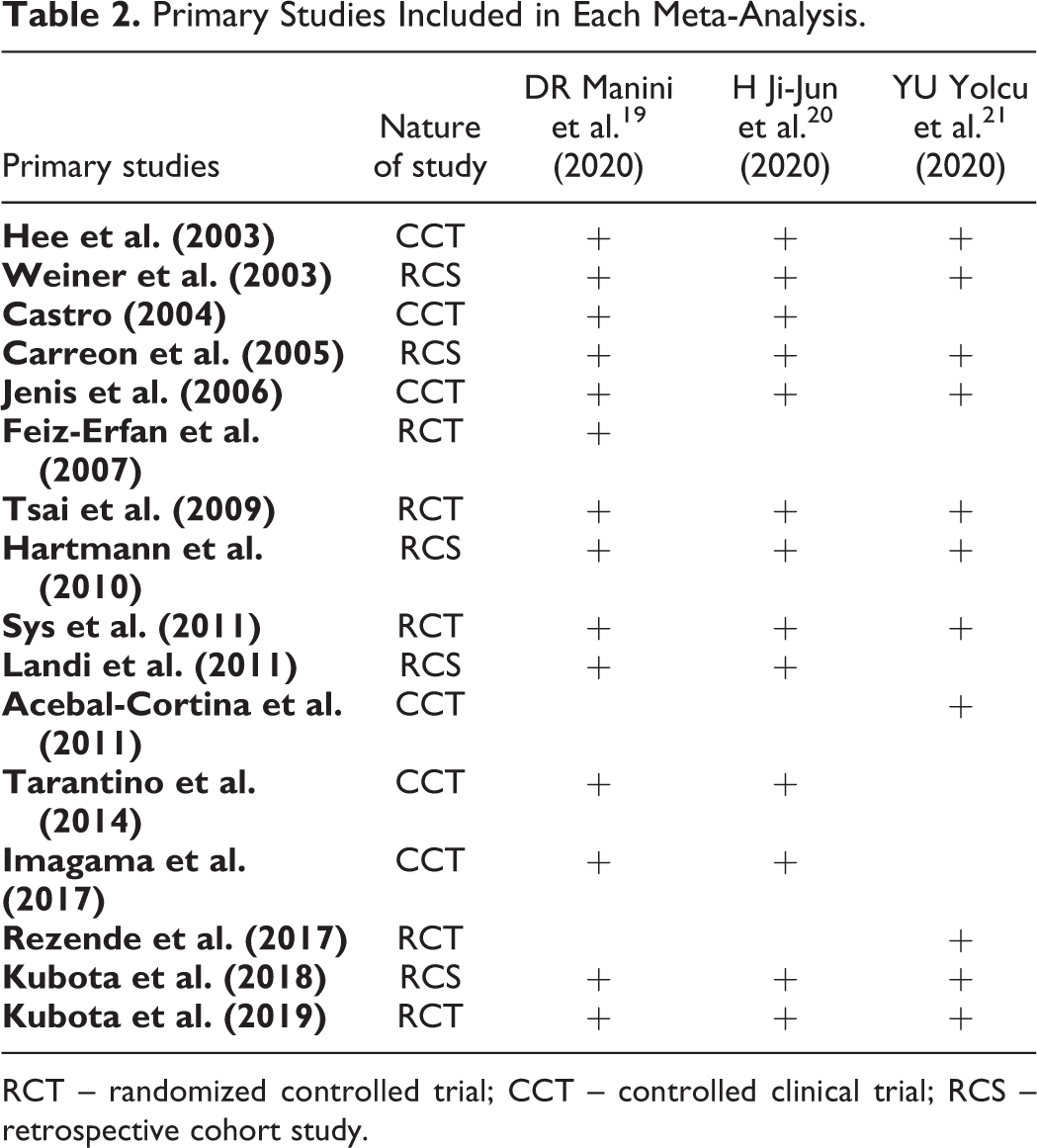
RCT – randomized controlled trial; CCT – controlled clinical trial; RCS – retrospective cohort study.
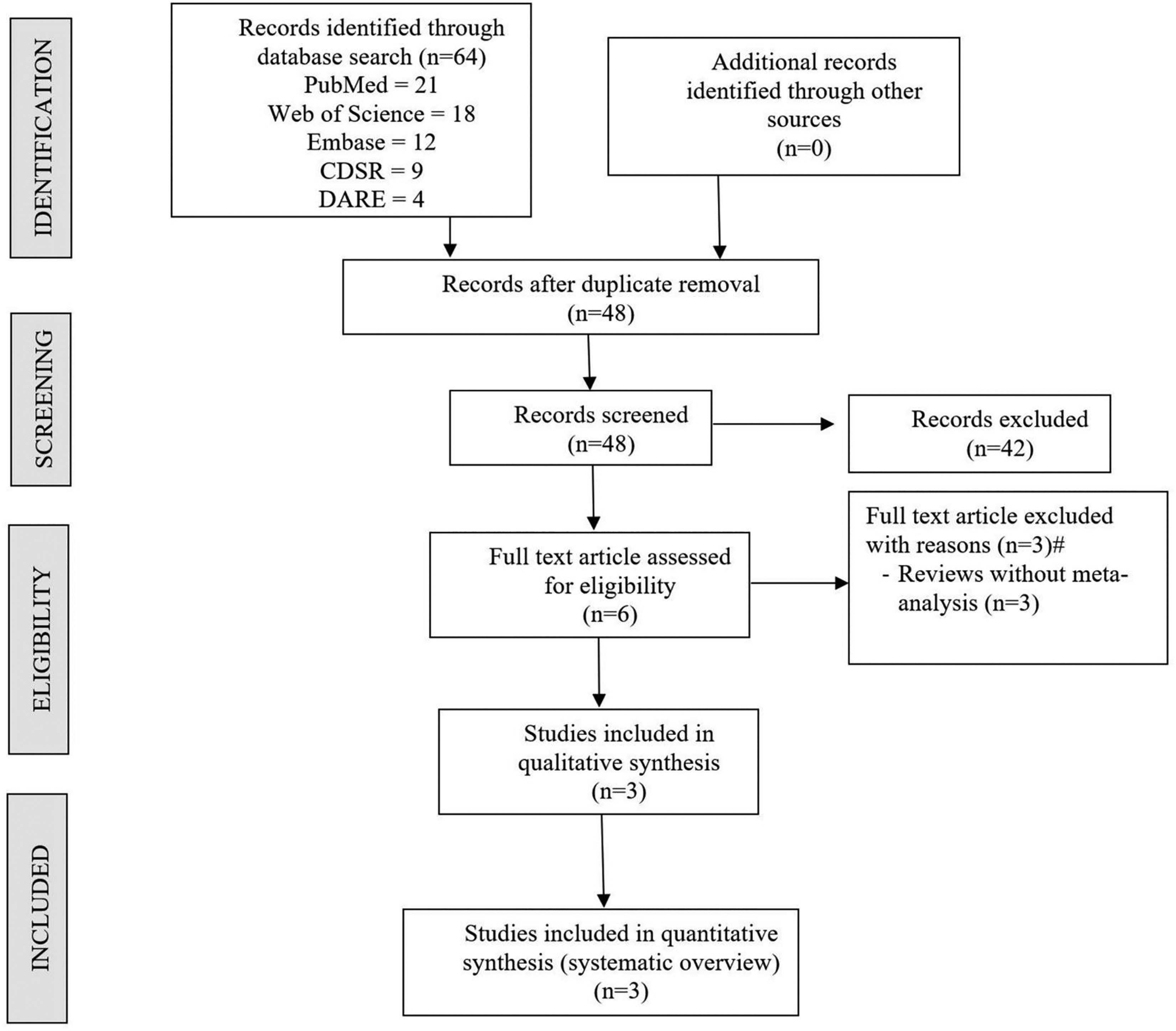
PRISMA flow diagram of the included studies.
Search Methodology
Although the included meta-analyses made a comprehensive literature search, the search databases were discordant among them. All studies searched PubMed/Medline databases. While Embase was searched by 2 of the included studies,19,21 Cochrane, Web of Science or Scopus were also searched by one of the included studies. All the included studies had a linguistic restriction in their selection criteria. None of the included studies searched grey for eligible studies. Further details on the search methodology employed by the included studies were presented in Table 3.
Search Methodology Used by Each Study.
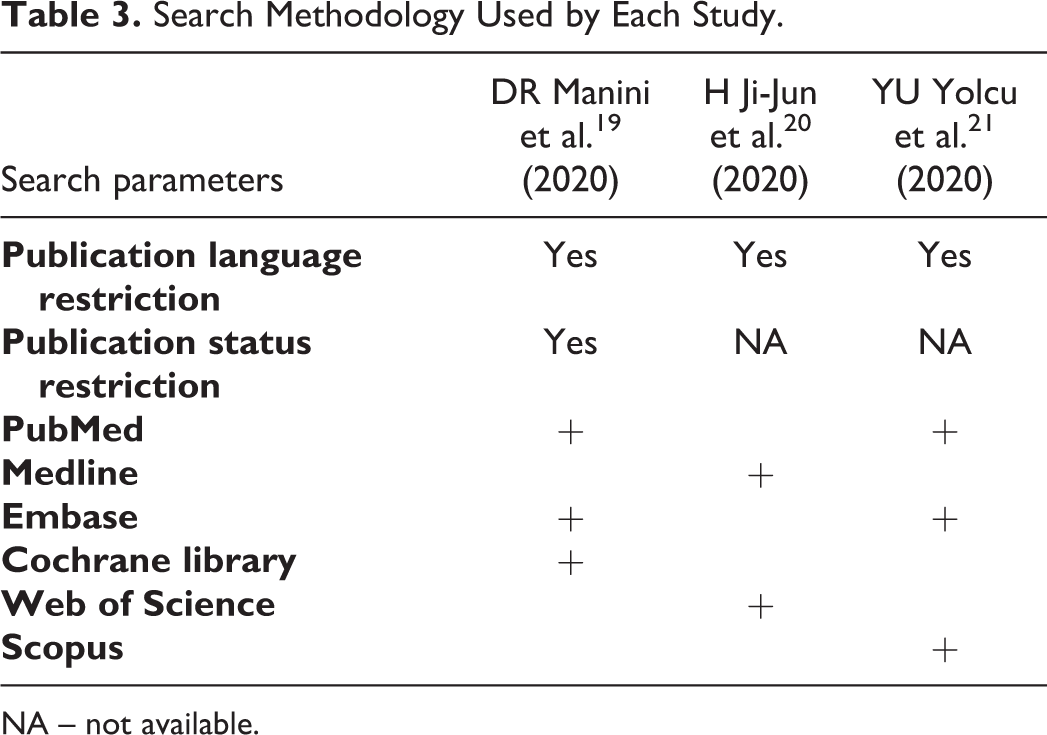
NA – not available.
Methodological Quality
Using Oxford Levels of Evidence, we determined the quality of the included studies based on the nature of the primary studies included in their analysis. All the 3 included studies were of Level II evidence since they included a mixed collection of randomized controlled trials, non-randomized controlled clinical trials, and retrospective cohort studies as shown in Table 4. All the included studies used RevMan for data analyses. Besides, one study utilized the GRADE system, 21 one conducted a sensitivity analysis to identify the source of heterogeneity in results obtained, 20 and one made subgroup analysis 19 based on the concentration of platelets in the primary studies included. Two of the 3 included studies analyzed possible publication bias.20,21 As shown in Table 5, the AMSTAR scores of the included studies ranged from 5 to 8 (mean 6.3). Based on the AMSTAR 2 grading, none of the included studies were without critical methodological flaws in the conduction of the meta-analysis. Of all the included studies, the meta-analysis by YU Yolcu et al. 21 was found to be of the highest quality with an AMSTAR score of 8/11 as shown in Table 5. However, it also suffered from critical methodological flaws such as non-making a priori design for the conduction of the study and not providing the list of excluded studies with their reason for exclusion.
Methodological Information of Each Study.
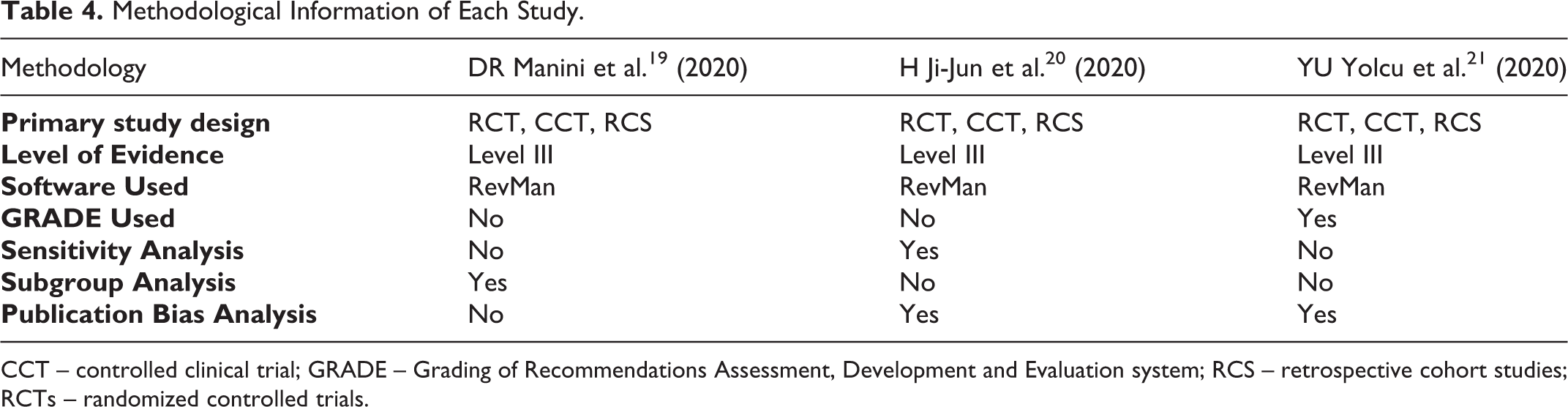
CCT – controlled clinical trial; GRADE – Grading of Recommendations Assessment, Development and Evaluation system; RCS – retrospective cohort studies; RCTs – randomized controlled trials.
AMSTAR Scores and AMSTAR 2 Grading for Included Studies.a
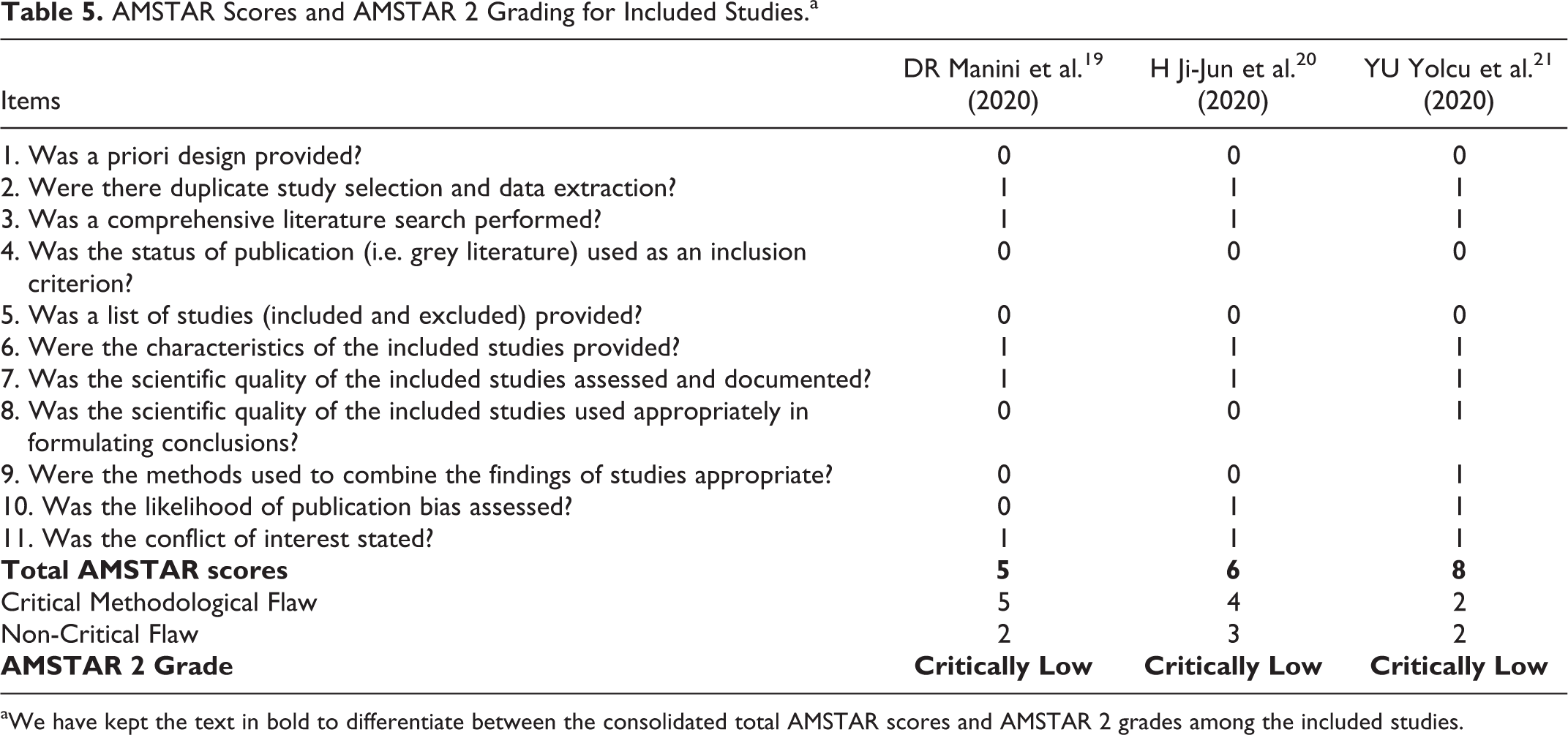
aWe have kept the text in bold to differentiate between the consolidated total AMSTAR scores and AMSTAR 2 grades among the included studies.
Heterogeneity Assessment
All the studies included used I2 statistic for heterogeneity assessment. Mild heterogeneity was noted in outcomes like VAS, time to fusion, and estimated blood loss as shown in Table 6. Nevertheless, the heterogeneity of the fusion rate and fusion density was significant. To explore the sources of heterogeneity only one study conducted a sensitivity analysis, 20 and one made subgroup analysis 19 as shown in Table 4.
I2 Statistic Values of Variables Analyzed in Each Meta-Analysis.
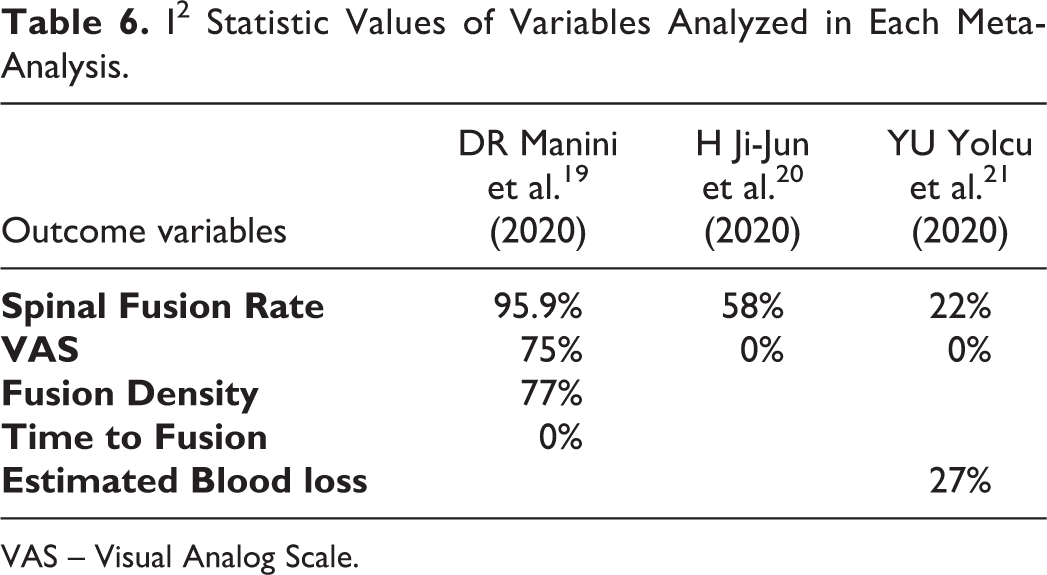
VAS – Visual Analog Scale.
Results of the Jadad Decision Algorithm
The pooled results from each of the included meta-analyses were given in Figure 3. To identify the study that provides the best possible evidence to generate treatment recommendations, we adopted the Jadad decision algorithm. Considering that all the 3 included meta-analyses tried to answer the same clinical question despite having a varied spectrum of primary studies being analyzed, the study with the highest quality is selected based on its methodological quality, restrictions involved in study selection such as language, databases involved, and data analysis protocols as shown in Figure 4. Eventually, we identified the meta-analysis by YU Yolcu et al. 21 as the highest-quality study among the included meta-analysis based on the Jadad decision algorithm. This study has shown that the utilization of PRP was not associated with significant improvement in patient-reported outcomes such as Visual Analog Score for pain compared to the standard fusion procedure. Moreover, PRP was found to be associated with lower fusion rates.
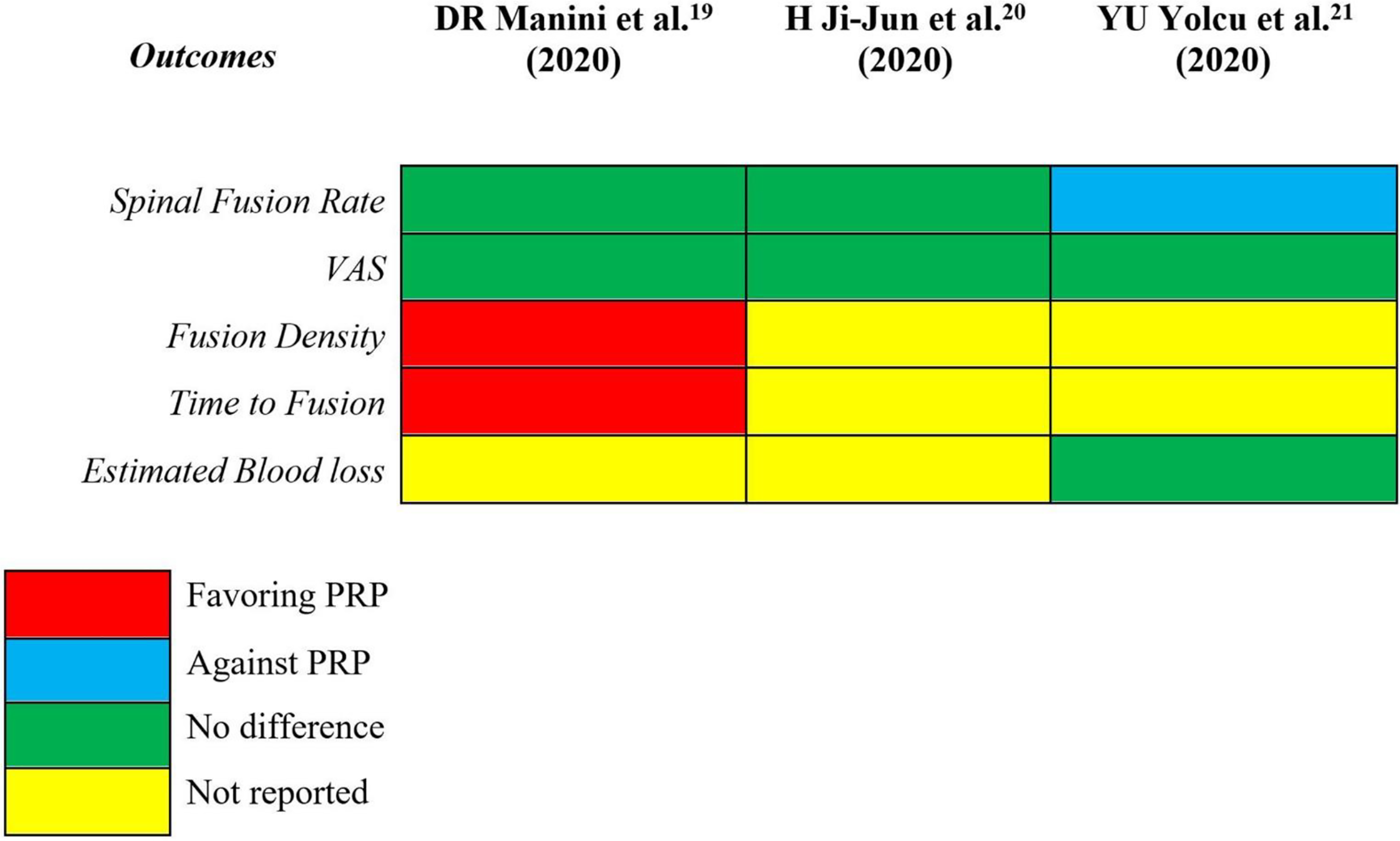
The pooled results of each included meta-analyses.
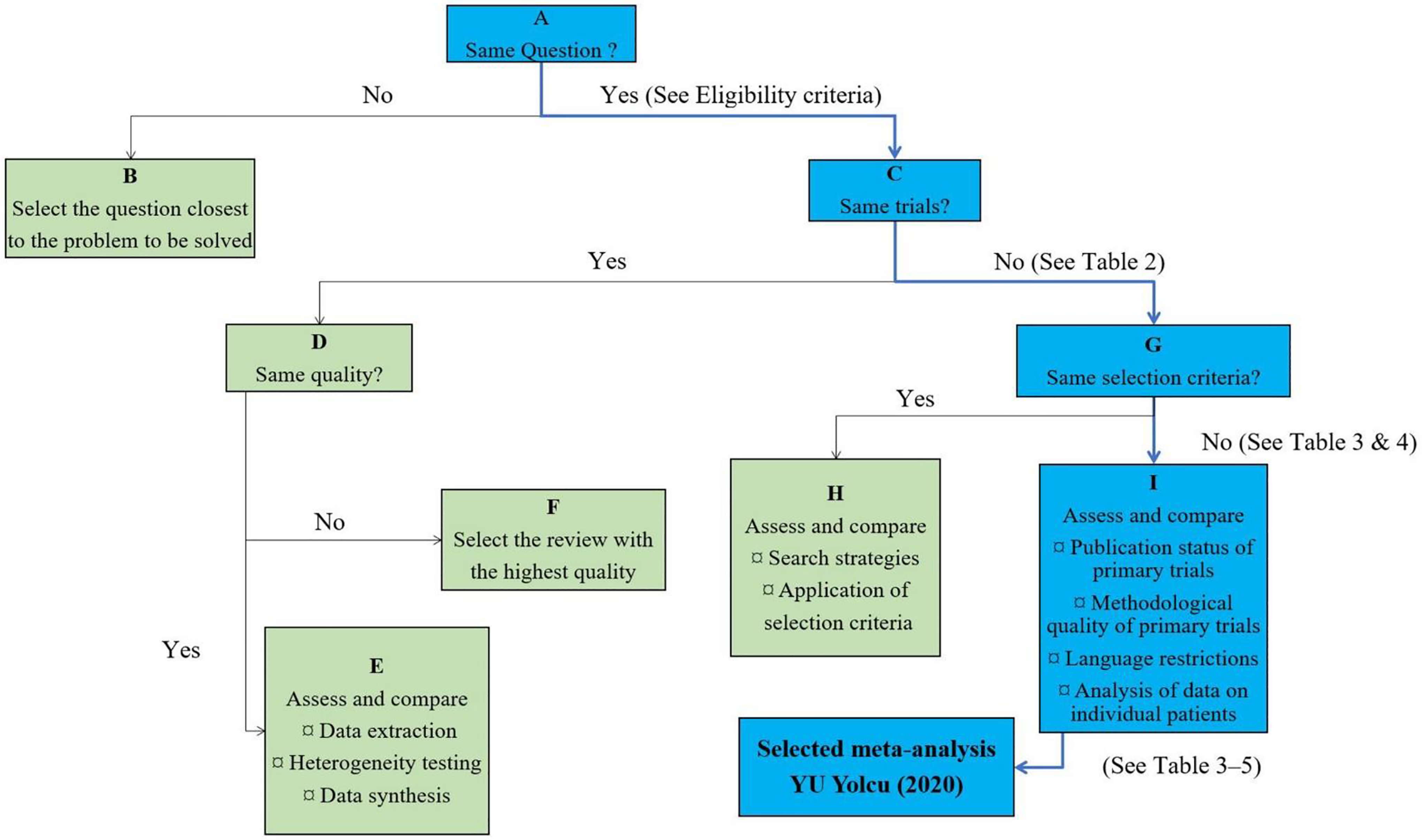
Application of Jadad decision algorithm to identify the high-quality study.
Discussion
Of late, numerous augmentation measures have been implemented in spinal fusion procedures to prevent complications like pseudoarthrosis. 35 Autografts, allografts, bone morphogenic protein were noteworthy of those measures.36,37 Although allografts have been shown to provide promising results in various studies, their efficacy and safety were not equivalent to autologous grafts. This makes autologous grafts, the gold standard material of choice to enhance the fusion process. 38 However, autografts have an inherent limitation in their limited availability and complications related to their harvesting procedure such as donor site morbidity, increased operative time, and blood loss. 39 Hence, there is an ongoing search for potential alternatives to meet their function.
The utilization of PRP in spine surgery has been started as a hybrid method since they bear the autologous nature of autograft and readily available nature of allograft. 40 PRP is prepared by a double centrifugation process to achieve the supra-normal concentration of viable platelets. 41 Various preparation protocols have been employed by various commercially available systems to improve the concentration and effect of PRP isolated. It was evident from the selected meta-analyses that the addition of PRP did not show significant improvement in the fusion rate, in the contrary, fusion rates were better in groups not using them. 21 Moreover, no significant difference was noted in patient-reported outcome measures or blood loss compared to the controls. Elder et al. 12 in their systematic review arrived at a similar conclusion that PRP despite being a promising strategy to enhance fusion, there is a lack of evidence to recommend its use in daily practice.
Both beneficial and detrimental effects of PRP has been reported with regard to bone regeneration. Weiner and Walker 42 reported inferior fusion rates when PRP is combined with autogenous bone graft whereas Imagama et al. 11 noted shorter time to fusion with PRP although a significant increase was not noted at final follow-up and Kubota et al.2,15 did not find such reduction in the time needed to achieve bone union. The discrepancy in the results of these studies was mainly due to the variation in the proportion of PRP and other regenerative factors in the PRP injectate utilized and the extraction protocols employed.
Weibrich et al. 43 noted inhibitory and cytotoxic effects of a high concentration of PRP on osteoblastic activity. Further, the variability in the growth factors in the PRP is individualized and the ideal concentration of growth factors required to promote bone fusion has not been ascertained. Although studies on human spinal fusion models found that PRP with more than 10 times the concentration of PDGF and TGF-β in whole blood must be ensured to achieve fusion, 44 if at all these levels are achieved in the injectate, maintaining such concentration at the implantation site is a challenge. All the factors synthesized and released by platelets will be eluded within one hour of its implantation. 45 Without any scaffold to support the PRP the soluble portion would have diffused and moved away from the implantation site post-operatively. Kamoda et al. 8 showed that PRP with hydroxyapatite could achieve interbody fusion in an animal model. However, evaluating whether hydroxyapatite as an optimal scaffold needs further investigation. On longer follow-up, it was also noted that no difference was noted in bone fusion since the action of PRP is limited by time. 40 On a cost-benefit perspective, the utilization of PRP would only add to the cost of the fusion procedure without any demonstrable benefit to the patient. 46 Hence, we no longer support the use of PRP as a biologic of choice to enhance the success of the spinal fusion procedure.
Directions for Future
Among the biologics, Stem cells hold promise as a potential agent hypothesized to augment the efficacy of various surgical procedures.47,48 Eastlack et al. 49 in their study noted significant improvement in functional outcomes like Neck Disability Index, arm VAS, neck VAS with the use of stem cells for anterior cervical discectomy and fusion compared to the cadaver allografts. Similar results were noted in extreme lateral interbody fusion procedures of the lumbar spine with 90.2% fusion at end of 1-year follow-up by Tohmeh et al. 50 Stem cells pose as a replacement to allografts while PRP can only be employed as a combination therapy with allografts. However, large randomized controlled trials are needed to arrive at sufficient evidence to warrant its use in everyday practice. 48
Although our systematic overview did not recommend the use of PRP in spinal fusion, there remains a lack of uniformity among the studies analyzed with regard to the level of surgery, the concentration of growth factors and platelets used among the studies, their preparation protocols, the dosage of injectate and carrier scaffold utilized by them. Moreover methodological quality of the available meta-analyses was not robust to arrive at Level I recommendations. To clarify these aspects, blinded RCTs investigating the above-mentioned lacunae and meta-analysis exclusively involving Level I studies are required in the future to arrive at a consensus on the orthopedic applications of PRP.
Limitations
This study has some limitations. This study identified meta-analyses of mixed study designs that were identified to be of Level II evidence. Hence, we cannot provide a strong Level I recommendation with the current literature. This systematic overview may be influenced by the limitations and biases involved in the meta-analysis and their primary studies.
Conclusion
Based on this systematic overview, the effectiveness of PRP as a biological agent in augmenting spinal fusion is limited. Current evidence does not support the use of PRP as an adjuvant to enhance spinal fusion. Further randomised control trials and meta-analysis from such high-quality studies are warranted to generate a strong recommendation on the use of PRP in spinal fusion procedures.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_2192568220988278 - Is Platelet-Rich Plasma Effective in Enhancing Spinal Fusion? Systematic Overview of Overlapping Meta-Analyses
Supplemental Material, sj-docx-1-gsj-10.1177_2192568220988278 for Is Platelet-Rich Plasma Effective in Enhancing Spinal Fusion? Systematic Overview of Overlapping Meta-Analyses by Sathish Muthu, Madhan Jeyaraman, Parvez Ahmad Ganie and Manish Khanna in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.