
Abstract
Study Design:
Narrative review.
Objective:
To address the gap in the literature on specific return to play protocols and rehabilitation regimens for golfers undergoing lumbar spine surgery with a high impact swing.
Methods:
This review did not involve patient care or any clinical prospective or retrospective review of patient information and thus did not warrant institutional review board approval. The available literature of PubMed, Medline, and OVID was utilized to review the existing literature.
Results:
Studies have shown that the forces through the lumbar spine in the modern-era golf swing are like other contact sports. Methods of protecting the lumbar spine include proper swing mechanics, abdominal and paraspinal musculature strengthening and flexibility as well as physical fitness. There are a variety of treatment options available to treat lumbar spine pathology each with a different return to play recommendations from doctors in the field.
Conclusions:
With the introduction of a high impact, modern-era swing to the game of golf, the pathology is seen in the lumbar spine of both young, old, professional, and amateur golfers with low back pain are similar to other athletes in contact sports. Surgery is effective in returning athletes to a similar level of play even though no protocols exist for an effective and safe return. There have been many studies conducted to determine appropriate treatment and return to play for these injuries, but there is a gap in the literature on specific return to play protocols and rehabilitation regimens for golfers undergoing lumbar spine surgery with a high impact swing. As return to competitive play is important, especially with professional golfers, studies combining the use of swing mechanics changes, rehabilitation regimens and the type of surgery performed would be able to provide some insight into this topic now that golf may begin to be considered a contact sport.
Introduction
In the modern era of golf, 62% of golfers in the United States suffer an injury directly related to golf, 1 and as golf continues to grow with an estimated 55 million players by 2020, 2 golf-related injuries will become more prevalent. According to Hosea and Gatt 3 and Armstrong, 4 most cases of golf-related spine problems are caused by mechanical damage to the spinal column or the associated structures. Local soft tissue damage in the form of muscle strains, disc disruption, and facet joint capsule trauma is the most frequent cause of low back pain given the limited range of axial rotation in the lumbar spine and emphasis of torsional loading during the swing. 5
In the 1997 Masters, an estimated 44 million viewers experienced the introduction of a golf swing with a significant amount of axial rotation and torsional loading in a high impact athlete into what was, once considered by many, a low impact sport requiring minimal stress on the body. Tiger Woods dominated in his first major championship win at the 1997 Masters by 12 strokes and of note, averaged 295.35 meters (323 yards) off of the tee during the week which was 21.03 meters (23 yards) more than the next longest driver. 6 He accomplished this feat using a steel-shafted, small-headed driver that would be considered an antique compared to today’s technology. The amount of stress placed on the body to generate the amount of energy needed to create a 193.12 kph (120 mph) swing speed is comparable to approximately 8 times an individual’s body weight and found to be similar to the stress a college football lineman places on his body during full-contact practice. 7
A Sport of Athletes With a New Approach
With the introduction of “The Tiger Factor” in the 1997 Masters, the popularity of golf exploded and in 2017, over 32 million Americans 6 years and older played golf on nearly 15,000 courses. 8 This explosion in popularity also began to draw more high impact all-around athletes to the sport of the likes of Dustin Johnson and Keegan Bradley who have been known to be able to dunk a basketball, Gary Woodland who played collegiate basketball, Sergio Garcia who has been known for his soccer talents, Matt Kuchar who is a very proficient tennis player, and Rory McIlroy. 9 These athletes began to take more athletic approaches to the game of golf by implementing swing mechanics, fitness, and other factors that generated the highest quality results with the smallest margins of error. This new approach to the game seems like a reaction to a recent study that showed over 80% of professional golfers experience spine problems during their careers.10,11
The etiology of spine problems in golf is commonly multifaceted and identifying a specific pathology is often difficult. Potential nociceptive contributors to spine problems may include the intervertebral disc, facet joints, vertebral endplates, the vertebral ligaments, and tendons. 12 Diminished lumbar musculature size and integrity and core abdominal and low back muscle-weakening are associated with spinal issues and can result in motor control deficiencies and asymmetries.13-20 Biomechanical research suggests that individuals with recurrent spine issues lack adequate spinal stabilizing contractions and may demonstrate impaired postural control, delayed muscle reflex latencies, and trunk muscle recruitment pattern abnormalities.21,22 which is why physical fitness and precise, consistent swing mechanics have become such an integral part of a professional golfers preparation for the sport.
Method
This review did not involve patient care or any clinical prospective or retrospective review of patient information and thus did not warrant institutional review board approval. The available literature of PubMed, Medline, and OVID was utilized to review the existing literature. The search terms were used were: “Low Back Pain in Golf Players,” “Lumbar Injuries in Golf Players,” “Golf Swing and Lower Back Injury,” “Golf-Related Lower Back Injuries,” and “Biomechanics of Golf.”
Biomechanics of Golf Swing in Relation to the Lumbar Spine and Pelvis
Han et al. 23 studied the relationship between the hip-shoulder torsional separation style (X-factor pattern) and kinematic sequences and reported that how the golfer separates the shoulders from the hips during the backswing affected the kinematic sequences (backswing, transition, and downswing). In this study, Han et al. classified 74 male skilled golfers into 5 groups: late shoulder acceleration (LSA) group (n = 14), large backswing stretch (LBS) group (n = 15), large downswing stretch (LDS) group (n = 15), small total stretch (STS) group (n = 15), and medium total stretch (MTS) group (n = 15). Han et al. identified the LBS group as the most ideal swing style which promotes proximal-to-distal kinematic sequences. The LBS pattern is characterized by an elongated transition phase (end of pelvis rotation [EPR] to top of backswing [TB]) and prepares the body sufficiently taking advantage of the stretch-shortening cycle style muscle activation (Figure 1). In this group, the transition phase, the early downswing phase (TB to arm-based early downswing EDA), and the late downswing phase (EDA to ball impact [BI]) showed an almost 1:1:1-time ratio. The groups with poor preparation during the backswing (LDS and STS groups) tended to have a short transition phase and prolonged early downswing phase and have to ready the body at the beginning of the downswing instead of at the end of the backswing during the transition phase. The study findings by Han et al. 23 can help to explain why proper mechanics could be linked to the amount of axial, torsional force that is placed on the lumbar spine when the muscles surrounding the spine are not activated or readied at the appropriate time. Han et al., 24 by involving 63 skilled male golfers, looked at different external torque generation mechanisms: ground reaction force (GRF) torque, pivoting torque, and foot contact torque. Their results show that the external torque about the forward/backward axis was mainly produced through the GRF torque mechanism by the lead leg and that the external torque about the vertical axis was mainly produced through the pivoting mechanism by the trail foot. Moreover, they show that the peak torques were significantly correlated to clubhead speed, and the peak GRFs of the lead foot (backward, away, and upward) and trail foot (forward) were also significantly correlated to clubhead speed. They concluded that the weight shift from the trail foot to the lead foot played an important role in this. In summary, Han et al.’s 24 showed the importance of the golfer-ground interaction, the use of lower body during the swing, and lower-body driven swing is more rhythmical and dynamic and important in a smooth transfer of large amounts of energy from the lower body through the lumbar spine into the upper body and eventually the club.
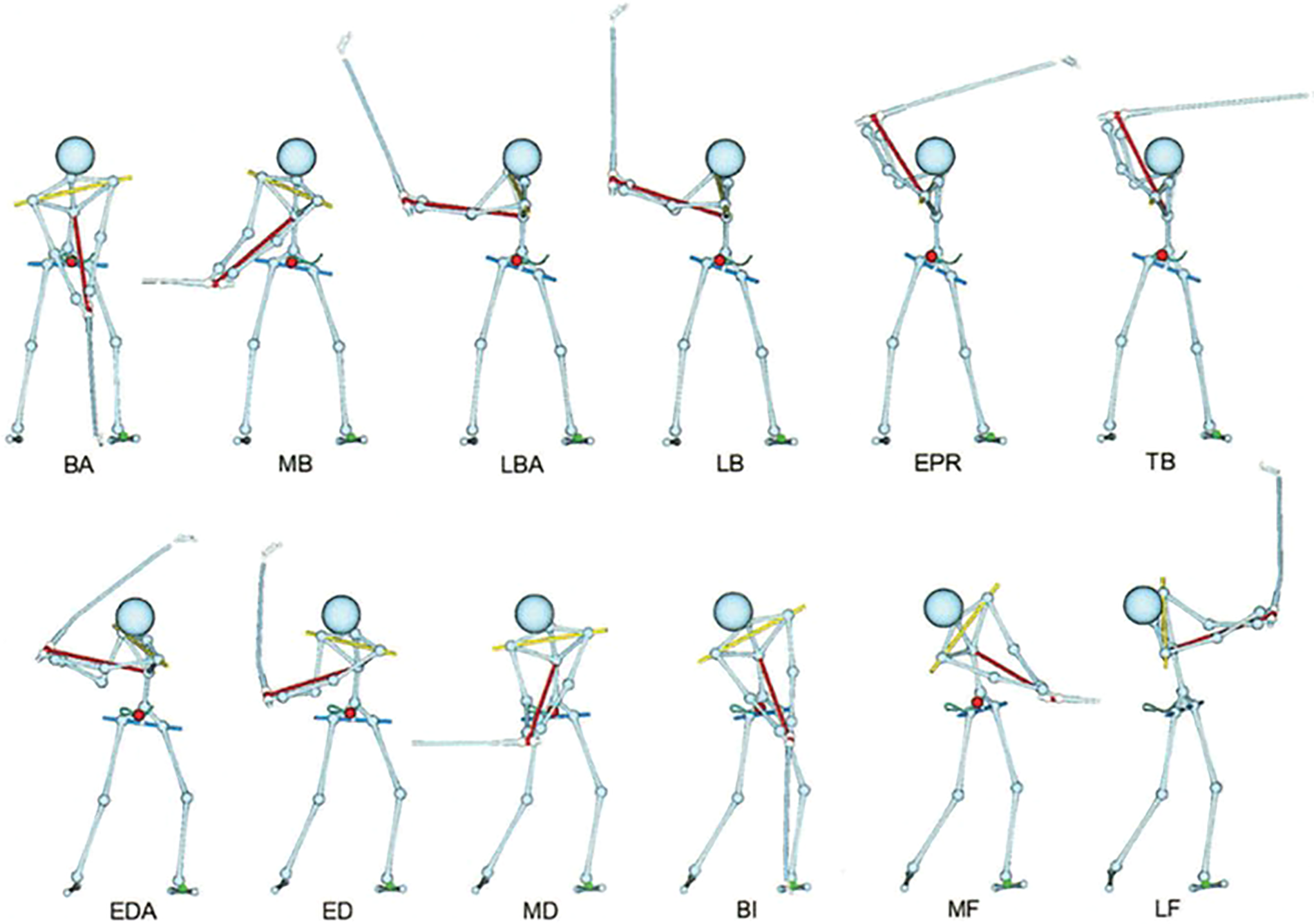
Club/lead-arm position-based swing events: BA (Breakaway), MB (Mid Backswing), LBA (Late Backswing, Arm-Based), LB (Late Backswing), EPR (End of Pelvis Rotation), TB (Top of Backswing), EDA (Early Downswing, Arm-Based), ED (Early Downswing), MD (Mid pact), MF (Mid Follow-Through), and LF (Late Follow-Through).
The Titleist Performance Institute also describes the importance of the pelvis-lumbar spine relationship by demonstrating the appropriate parameters for pelvic tilt during a golf swing. At address, the pelvis is resting in approximately 25-30 degrees of flexion, and eventually, the pelvis finishes in approximately 3 degrees of flexion at the completion of the swing also known as pelvic rollback. When pelvic rollback occurs, the energy generated from the lower body is transferred into the upper body to allow for generation of swing speed. The oblique abdominals are contracting to provide this appropriate pelvic rollback and extend the pelvis from its resting position in flexion. 25
Now a Contact Sport With a High Impact Swing
While a properly executed golf swing may not appear overtly stressful, biomechanical studies show that many body parts are moving at high velocity and through extreme ranges of motion.26,27 Tiger Wood’s in his early career clearly demonstrates these findings. Additionally, these movements are complex and require a high degree of coordination as stated above.28,29 Lumbar spine flexion and extension at address to the ball can be another risk factor to increase the compressive forces between the lumbar vertebrae. 30 “Slouching” or beginning with the spine in flexion at address increases the disc pressure before the swing even begins.5,31 The most profound difference between golfers and other athletes is the enormous amount of rotation that occurs over a fixed base and the extraordinary torque it generates in the spine. In other sports in which an implement is swung around the body, the athlete’s body is in constant motion. Golf is the only sport that requires the athlete to be very still prior to unleashing a sudden explosion of rotation. The sudden explosion of rotation in a flexed posture repeated several hundred times per day exposes the lumbar spine to significant compression, anterior-posterior shearing, torsion, and lateral bending forces during the golf swing.32,33 Without knowledge of proper swing mechanics, golfers could be at increased risk for development of low back problems as demonstrated by Hosea and Grant with the use of lumbar spine kinematic, kinetic, and electromyography (EMG) data that was collected using surface electrodes and human motion capture system. 34 In 2 separate studies, these authors demonstrated the amount of compressive loads across the lumbar spine in 2 different high impact athletes, Division 1-A college football linemen hitting a blocking sled and professional golfers, which were calculated to be 8,679 ± 1,965 Newton (N) and 7,584 ± 2,422 N, respectively. 35 Previous research using X-ray and computed tomography have demonstrated asymmetric degenerative changes in the lumbar facet joints of professional golfers compared with non-golfer controls as the facet joints resist more than 50% of the anterior-posterior shear load which has been estimated in amateur golfers’ swings to peak around 5,966 ± 514 N.34,36-38 2-3 degrees of intersegmental rotation is required to produce microtrauma in the lumbar facet joints. 39 The effects of these compressive loads and shear loads have been demonstrated in cadaveric specimens where disc prolapse occurred with compressive loads of 5,448 N and pars interarticularis fractures occurred with cyclic loading of 5,706 ± 190 N.40-42 Golf instructors put emphasis on the lumbar spine loading, creating tremendous amounts of torque. It has been shown that the most common cause of disc herniation in a healthy disc was lateral bending combined with compression and torsion, all of which are major components of the golf swing.43,44 Based on analysis of the forces generated by the golf swing, it is clear how repetitive lumbar spine loads may potentially predispose a golfer to muscle strains, herniated nucleus pulposus, stress fractures of the vertebral body and pars interarticularis, spondylolisthesis, and facet arthropathy. 3 A group of surgeons from Barrow Neurological Institute postulated that modern-day golfers, particularly elite players who have high impact golf swings are repeatedly traumatizing their lumbar spine. They called it “repetitive traumatic discopathy” (RTD). 45 Is there anything that can be done to mitigate the amount of damage that is imparted to the lumbar spine by the modern-era golf swing?
High Impact Sport Without Proper Protection
The most common cause of injury in both professional and amateur golfers is repetitive swing motion and associated axial torque, which may be amplified by poor mechanics.32,46 Poor swing mechanics are the second most frequent cause of injuries.
47
Upper body-driven swings with no balance with the lower body generally have some of the following characteristics: Slow and quiet backswing using the arms predominantly; Abrupt transition from the backswing to the downswing; Insufficient preparation of the body (muscles) during the backswing using eccentric muscle activation
23
; Excessive pelvis motion at the beginning of the downswing
Approach to Non-Operative Treatment: The Right “Equipment”
Smith et al performed a systematic review looking at a variety of risk factors and the association with low back pain in golfers. Of the variables analyzed, an increase in body mass index, asymmetry of the side to side oblique and abdominal muscles, asymmetry of hip internal rotation, and earlier onset/activation of back muscles in the downswing were all associated with low back pain. On the contrary, low handicap golfers were found to have strong erector spinae and oblique musculature. 49 With recognition of a possible cause of LBP in golfers, literature does show that improved swing technique and physical fitness11,28 appear to reduce injury frequency. Efforts to prevent back injury typically focus on strengthening and flexibility exercises. 50 Exercise strategies may address trunk muscle coordination, strength, and endurance. Other strategies may focus on identifying and correcting muscle contraction issues, and movement directional preferences. Such golf exercise programs may allow the lumbar spine to better withstand the biomechanical stress of the full recoil swing; however, the potential for injury still exists because it is the execution of the full recoil swing that induces injuries.3,46,51 Neighbors et al suggested that a short backswing with minimal rotation provides a similar and a more consistent clubhead velocity at ball impact than a long backswing with maximum torso rotation. 52 Similar findings were reported by Bulbulian et al. in which reduced back muscle activation with a short backswing without decrements in swing accuracy and clubhead velocity and possibility of reduced risk for low back injury and pain. 53 There is no definition of a physiological golf swing method in the available literature that can be cited as an injury-preventing guideline. The study by Goebel et al. 54 analyzed classic golf swing kinematics in comparison to the core balance Free-Release method and defined a physiological golf swing for amateur and professional golf players that respects the anatomical range of the lumbar spine. They demonstrated that a healthy golf swing is possible. Strengthening muscles without eliminating any major swing pattern issues is also bad. It is like building a bigger structure on a shaky foundation and increasing the chance of collapse. Rigorous muscle actions with poor swing biomechanics simply destroy the body. The ultimate prevention strategy is development of a dynamic and rhythmic swing pattern with active lower body motion during the backswing and the downswing and continuous transition from the backswing to the downswing. 23 Additionally, maintaining strength and flexibility of the musculature heavily involved in this rhythmic swing pattern would only provide more of a benefit.
As stated earlier, there is no perfect swing that has been developed to prevent injury, but just like Diebo et al discussed the use of gait analysis to understand deformity, there may be utility in using swing analysis, spine kinematics, and EMG to diagnose, to treat, and to guide surgeons and therapists on the intended form of intervention. 55 Similarly, this approach could be expanded to the post-operative period to prevent recurrent disease and further injury and decrease return to playtime.
Non-Operative “Equipment”
Teaching Golfers to Be Their Own Therapist
It is critical in any rehabilitation or conditioning program to educate the patient to be keenly aware of what the spine needs to remain healthy, pain-free, and able to support a quality golf game. Each patient needs to be taught proper posture strategies and trained to rotate from the thoracic cage. This is not a natural movement for many golfers, and many must “un-learn” unhealthy movements that have become almost instinctive over years of improper form.
Decompression Exercise
Patients also should be taught specific decompression techniques. Most traditional decompression techniques, such as traction and inversion tables, are passive in nature and offer limited benefits. However, there is a specific active decompression technique called ELDOA™ that is particularly effective in achieving this important result (Figure 2). ELDOA is a French acronym for Longitudinal Osteo Articular Decoaptation Stretching. It was developed by French osteopathic physician, Dr. Guy Voyer, and there is an ELDOA for each spinal segment as well as other joints such as the hips, SI, and shoulder joints. Each ELDOA is a one-minute posture exercise designed to give space to the targeted joint by putting specific fascial chains under tension. Since patients use their own muscle contractions to perform ELDOA, it is an active form of decompression, not passive. Examples of ELDOA exercises are presented in Figure 2.

Representative ELDOA exercises. A, Rib 10: This is the working posture to open the space between the articulations of the 10th rib and T10. B, T12-L1: This is the working posture to give space between the T12-L1 functional unit. C, L5-S1: this is the working posture to give space between the L5-S1 functional unit.
Strengthening
In strengthening the spine, it is important to recognize the intimate relationship between the spine and the muscles that support it. The spine is often treated as a single column rather than what it is, a marvelous architectural structure made up of 24 independent segments. It is difficult, if not impossible, to maintain a healthy spine for golf and avoid injuries without improving segmental control of the spine. That requires strengthening the abdominal and spinal muscles that control the spine, specifically the rectus abdominis and the external and internal obliques, both supraumbilical and infraumbilical. Strengthening the spinal muscles longissimus, iliocostalis and transversospinalis improves the chances for segmental control and serves to diminish the shear and compressive forces of the golf swing.56,57 A successful rehabilitation program also should include a formula that allows the golfer to play without pain into the future. That formula should be directed at improving posture and flexibility, stability, strength, and power.
Posture and Flexibility
Posture is more important in golf than in any other sport. It is the only sport in which the athlete remains completely quiet and still before exploding into action—in this case by swinging the club. Posture is not only the position from which movement begins and ends, it will also dictate how many degrees of freedom the thoracic cage will have for each swing. If the thoracic cage is too flexed, the amount of rotation will decrease, putting more pressure on the lumbar spine and other joints of the body. Due to the orientation of the facets, the lumbar spine only rotates 3-15 degrees, yet most golfers will generate most of their rotation from the lumbar spine. This is a cause of much injury and pain in the lower back for golfers. Therefore, therapy must also focus on improving the amount of rotation that occurs from the thoracic cage and the hips to take the pressure off the injured or surgically repaired lumbar spine. This should occur in conjunction with rehabilitation of an injured or surgically repaired spine in the golfer, but it should also be standard training to eliminate or prevent back pain for any golfer.
Stability
Paul Chek said, “You can’t fire a cannon from a canoe.” In the case of the golf swing, the canoe is our torso and the cannons are our extremities. It is impossible to generate any power without a stable spine. If we attempt to generate power on an unstable spine, shear compression and torque can destroy the joints and cause pain.
Strength
Strength is extremely important in golf, but golf is among the world’s most asymmetrical sports. This asymmetry causes golfers to manifest some of the most extreme muscle imbalances of any athlete. It is therefore imperative to strengthen the body symmetrically to counteract the demands of the golf swing. Additionally, the everyday golfer with a desk job remains in the seated position for extended periods of time leading to deactivation of the gluteal muscles, shortening of the hip flexors, rounding of the thoracic spine, and pelvis extension all of which are detrimental to a balanced golf swing.
Power
In today’s golf world of huge drives, golfers need a lot of power, and developing safe power should be the last phase of any rehabilitation or conditioning program. Power is produced by strength and speed, and safe power will come when posture, flexibility, stability, and strength are assured.
Operative “Equipment”
Ultimately, some symptomatic players with clinically significant degenerative changes may require surgical intervention. Spinal surgery can have good clinical outcomes in appropriately selected patients.58-61 For a golfer to choose to undergo surgical intervention for a surgically remediable lesion is not an easy choice as this can require a golfer to discontinue playing and for professionals, may result in loss of ranking and income.28,51,62 For the everyday golfer, this can limit their ability to work and play a sport that they love. Increasing numbers of patients with active lifestyles undergo spinal surgery with the goal of returning to a normal lifestyle and resumption of recreational activities. 63 Multiple different factors come into play when deciding on treatment regimens for these patients such as level of fitness, ability to rehabilitate, adjacent level disease, comorbidities, expectations of level of play post-operatively, and many more. In the future, additional factors that can be considered are specific swing mechanics, muscle activation patterns, and postoperative swing changes that may have to be made to prevent additional injury. Just like Tiger Woods required multiple microdiscectomies before his eventual fusion, return to pain-free competitive play is the goal and the journey may be long and difficult.
Return to Play Protocol: Straight Forward Surgery, Difficult Decision
The return to athletic sport after spine surgery, especially the ability for professional golf players to return to a prior or better level of play, is an important and disputed topic. Most patients electing to undergo surgery question the timing and ability of return to play before they make their final decision. These are challenging questions to answer because the ability to return to the former level of play can be influenced by many variables, including pain, stiffness, exercise tolerance, loss of mobility, and psychological limitations. 63 Some surgeons remain guarded about the return to play, with concern for excessive motion and strain on the lumbar spine. A large group of spine surgeons was surveyed to determine when golfers could return to play after several different types of spine surgery. 62 Most of the surgeons indicated they would allow patients to return to golf at 6 months after lumbar fusion; however, shorter times were recommended for competitive golfers. 63 A survey of North American Spine Society members was undertaken querying the suggested timing of return to golf. 62 Of 1000 spine surgeons surveyed, 523 responded (52.3%). The timing of recommended return to golf and the reasons were questioned for college/professional athletes and avid and recreational golfers of both sexes. Responses were matched for lumbar spine surgeries. The most common recommended time for a return to golf was 4-8 weeks after laminectomy and microdiscectomy and 6 months after lumbar fusion. There was a statistically significant shorter recommended time for professional and college golfers compared with noncompetitive golfers after lumbar fusion (p < 0.01), anterior cervical discectomy and fusion (p < 0.01), and lumbar microdiscectomy (p < 0.01). A group of investigators from Rush University Chicago completed a specifically designed golf survey of 353 patients who underwent 1- or 2-level primary lumbar fusion surgery for degenerative pathologies. 63 A total met the inclusion and exclusion criteria, with 200 responses (57%) to the questionnaire producing 34 golfers with an average age of 57 years (range, 32-79 years). In 79% of golfers, preoperative back and/or leg pain significantly affected their ability to play golf. Within 1 year from surgery, 65% of patients returned to practice and 52% returned to course play. Only 29% of patients stated that continued back/leg pain limited their play. Twenty-five patients (77%) were able to play the same amount of golf or more than before fusion surgery.
There is a paucity of literature on return to play in athletes, especially professional golfers, after lumbar spine procedures. Additionally, the introduction of a high impact swing into the sport may sway practitioners toward more conservative measures given recent literature endorsing golf as a contact sport. 45
Lumbar Disc Herniations Requiring Surgery
After surgical intervention for lumbar disc herniations, Eck et al provided recommendations on return to play for non-collision sports at 6-8 weeks and 3 months for collision sports given normal pain relief and range of motion after these time periods. 64 Watkins’ recovery recommendations for lumbar disc injury and repair in athletes was 3 weeks of only walking without bending lifting or driving followed by trunk strengthening and stabilization with a slow transition into sport-specific training. 35 Of 171 professional athletes undergoing surgery for lumbar disc herniation, 89% returned to play at an average of 5.8 months. 65 Another study found that 87% of student-athletes and professional bicycle racers returned to play at an average of 7.5 weeks. 66
Lumbar Fusion for Degenerative Disc Disease, Spondylolysis and Spondylolisthesis
Watkins also made recommendations for the older golf athlete undergoing fusion for RTP in golf at 6 months while those requiring decompression alone without fusion may return to golf at 3 months. 67 Many practitioners can expect athletes to return to their previous level of play at 6-12 months but if a fusion was performed, careers for collision sport athletes may be over. Important return to play consideration for athletes undergoing fusion is whether radiographs show bony union 68 as there is a less predictable course of returning to contact sports after this procedure for spondylolysis and spondylolisthesis. More specifically with recreational golfers, 13 of 13 golfers in a study by Jain returned to golf an average of 8.6 ± 3.6 months. Of note, the driving distance was reduced postoperatively (223 ± 43–212 ± 44 yards, p = 0.042) and handicaps increased (13 ± 8–17 ± 11, p = 0.022). However, there was no significant difference in the amount of the course that patients walked preoperatively and postoperatively. 69 Many authors suggest that, before considering a return to play, an athlete should have radiographic evidence of a solid fusion, resolution of preoperative pain, and restoration of strength, flexibility, and endurance. 70
Total Disc Replacement
One study evaluated 39 athletes treated with TDR for degenerative disc disease and it was found that 95% of the athletes returned to play with subjective full recovery and peak fitness at 5.2 months. 71 The above literature on return to play for athletes and golfers is summarized in Table 1.
Recommendations or Average Return to Play After Surgery for Lumbar Spine Conditions.
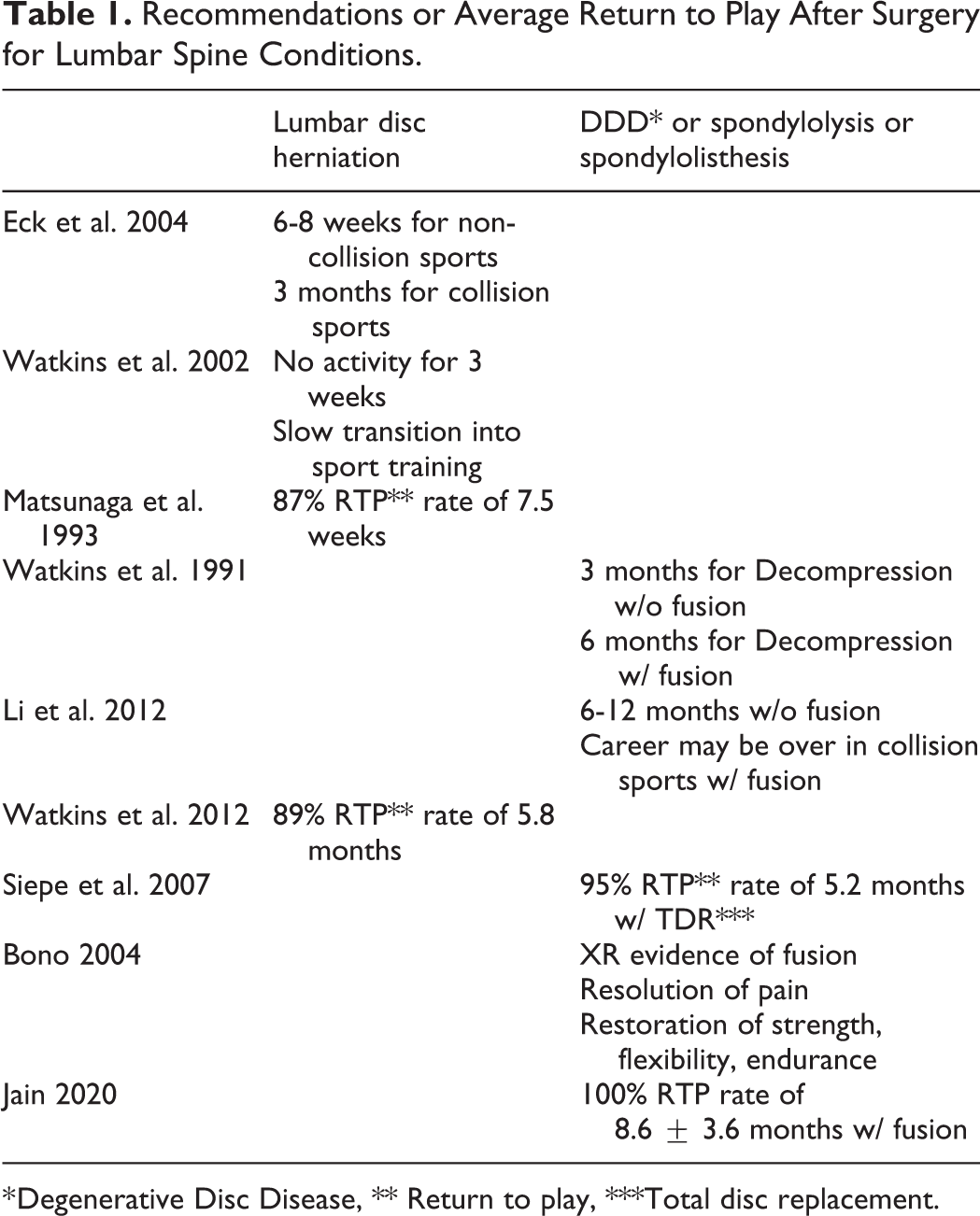
* Degenerative Disc Disease, ** Return to play, ***Total disc replacement.
For elite athletes to return to active sport, surgeons perform a muscle-sparing minimally invasive lateral or anterior approach, as was performed in the 2019 Master’ Champion’s case. This likely is most advantageous for avid players, given the importance of posterior spinal erector muscles that would be damaged during traditional open posterior approaches. 45 The natural history of the adjacent-segment disease in this vulnerable population will also need to be followed in the years to come as modern-era golfers continue to age and require treatment as spinal fusion alters spinal kinematics, which may ultimately affect the golf swing. 72 By fusing segments in the lumbar spine, the ability to flex and extend the pelvis is altered and the rotation through the lumbar spine is reduced possibly placing more stress on adjacent levels. There is no literature available in regard to swing alterations and the effect on the adjacent level disease in golfers who undergo fusion, but swing analysis, extensive rehabilitation and muscle training may be additional tools that can be used in the postoperative period to adjust patient’s swings and muscular coordination in order to protect the lumbar spine from the continued forces of the modern era golf swing.
As stated above, the return to play protocol is difficult to determine. There is no current literature on the use of EMG, swing analysis, and kinematics serially to determine body’s readiness for return to play for golf. For athletes looking to return to play sooner than expected, there is the possibility of using these tools to aid in that return. Swing analysis and kinematics performed in the postoperative period over sequential weeks, 2 weeks, months, etc. could show golfers where adjustments in their swings need to be made and how these adjustments will increase the longevity of their swing and prevent additional lumbar spine problems. Serial EMG also has utility in that physical therapists and the athletes will have the ability to focus on muscle groups that may have become deconditioned over the course of the treatment period and where efforts should be focused in order to provide the proper structural support to a newly repaired spine. These tools in conjunction with patient factors and clinician experience could help to hone in on the appropriate return to play algorithms in a patient-specific manner. Athletes that show difficulty with making swing changes and weak abdominal and paraspinal musculature may need to delay return to play until these changes can be made while on the contrary, athletes who are able to make these changes and strengthen the specific musculature identified by physical therapists, kinematics and EMG may be able to return to the sport sooner than expected.
Conclusion
Golf, once a low impact sport, has seen the introduction of high impact athletes in recent years, and with the introduction of the high impact athlete to the sport, golfers of all skill levels are beginning to show signs of high impact injuries most specifically in the lumbar spine. As with other high impact sports, proper techniques and equipment have been introduced to limit these high impact injuries. In the sport of golf, these techniques and equipment come in the form of physical therapy, muscle coordination and proper swing mechanics. When these fail, surgical intervention is often required, but the same techniques and equipment are needed postoperatively to ensure a safe and effective return to play. Implementation of swing analysis, like gait analysis to analyze spinal deformity, to diagnose low back pain, to treat certain pathologies, and to prevent additional injury in the postoperative period has not been visited but may be a new area of interest in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.