
Abstract
Study Design:
Retrospective observational cohort.
Objective:
A review of efficiency and safety of fluoroscopy and stereotactic navigation system for minimally invasive (MIS) Sacroiliac (SI) fusion through a lateral technique.
Methods:
Retrospective analysis of an observational cohort of 96 patients greater than 18 years old, that underwent MIS SI fusion guided by fluoroscopy or navigation between January 2013 and April 2020 with a minimum of 3 months follow-up. Intraoperative neuromonitoring (IONM) with a variable combination of electromyography (EMG), somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) was also utilized.
Results:
The overall complication rate in the study was 9.4%, and there was no difference between the fluoroscopy (10.1%), and navigation groups (8%). Neurological complication rate was 2.1%, without a significant difference between both intraoperative guidance modality groups (p = 0.227). There was a significant difference between the modalities of IONM used and the occurrence of neurological injury (p = 0.01).The 2 patients who had a neurological complication postoperatively were monitored only with EMG and SSEP, but none of the patients (n = 76) in which MEPs were utilized had neurologic complication. The mean pain improvement 3 months after surgery was greater in the navigation group (2.44 ± 2.72), but was not statistically different than the improvement in the fluoroscopy group (1.90 ± 2.07) (p = 0.301).
Conclusions:
No difference in the safety of the procedure was found between the fluoroscopy and the stereotactic navigation techniques. The contribution of the IONM to the safety of SI fusions could not be determined, but the data indicates that MEPs provide the highest level of sensitivity.
Introduction
The sacroiliac joint (SI) is a common source of chronic low back pain with a prevalence reported in the literature between 15 to 30%.1-3 The SI joint has also been shown to be a significant pain generator following lumbar and lumbosacral fusion procedures, being responsible for up to 40% of new-onset low back pain postoperatively. 4 The lack of long-term effectiveness of nonsurgical treatments for chronic SI joint dysfunction and superiority in improvements in pain and quality of life with minimally invasive surgical (MIS) SI arthrodesis, led to an increase in usage of SI fusion procedures over the past several years. A successful arthrodesis alleviates pain by stabilizing the SI joint, improving neurologic functional outcomes and quality of life.5,6
The execution of a safe and successful SI arthrodesis through a MIS technique is dependent on the use of intraoperative imaging. The procedure can be done with either a fluoroscopic technique or with stereotactic navigation using intraoperative computed tomography (CT) data. Navigation is believed to increase the accuracy of implant insertion, thus avoiding complications such as implant malposition and damage to adjacent structures such as the L5 or S1 nerves. 7
The use of intraoperative neurophysiological monitoring (IONM) in spine surgery aims to improve the patient’s safety, through real time-assessment of neural structures at risk. For MIS SI fusion, there are very few reports correlating IONM usage to postoperative outcomes. Comparable to pedicle screw testing in lumbosacral fusions, triggered EMG may prompt a subset of low-threshold screws to be revaluated and re-inserted thereby theoretically reducing the likelihood of postoperative neurologic complications from nerve impingement. 8 In MIS SI fusion triggered EMG is used only sparingly given the inherent difficulty of performing it through this technique. Additionally, patients with negative triggered EMG during SI fusion may still have neurologic complications. 9 There is no evidence that that spontaneous EMG or somatosensory evoked potentials added any diagnostic value in SI fusions.8,9 Regarding MEPs, there is only one case report indicating that the addition of this modality may improve the sensitivity in diagnosing neurologic complications during SI fusions. 10
This project was developed as an initiative to improve the evidence-based use of intraoperative image-guidance and IONM in sacroiliac joint fusions. This study’s aim was to analyze the importance of the use of fluoroscopy, stereotactic navigation, and different modalities of IOMN in the safety of MIS SI joint fusion.
Methods
Study Design and Setting
This is a retrospective observational cohort study that incorporated all patients that underwent a MIS SI Fusion for the treatment of a SI joint dysfunction between January 2014 and April 2020 at a single quaternary spine surgery service, and had a minimum of 3 months follow-up. Primary variables evaluated included weather the procedure was performed using fluoroscopy or with stereotactic navigation, and IONM modalities used. In all cases the MIS SI fusion was performed through a lateral technique with triangular titanium implants (iFuse SI Bone Santa Clara, CA). The iFuse implants initially used were titanium treated with a plasma spray to encourage bone on-growth. Subsequent implants used, iFuse 3D are 3D printed titanium with surface technology and open architecture designed to encourage better bony integration through on-growth and through-growth. The study protocol was approved by the Jefferson Institutional Review Board (IRB) (Approval number 17D.390), and was initially exempted from patient consent by the IRB before the initiation.
Participants
Eligibility criteria for the study cohort included all patients over 18 years old undergoing a MIS SI fusion by the senior author, a neurosurgical spine surgeon, in an elective manner after fulfilling the North American Spine Society (NASS) coverage guidelines for MIS SI Fusion. All patients were followed per routine post-procedure in the clinic for at least 3 months. A total of 96 patients were included in the analysis. The cohort of patients who underwent a MIS SI joint arthrodesis fluoroscopy-assisted (n = 46) were compared with the participants who underwent a MIS SI joint fusion guided by stereotactic navigation (n = 50).
Variables and Data Measurement
The major outcome investigated was the impact of the use of fluoroscopy versus 3-dimensional navigation system as well as the effects of different IONM modalities used in the detection of possible intraoperative neurological injury and postoperatively complications in patients undergoing SI joint fusion.
The following demographics and clinical variables were collected from each of the cohorts: age, gender, body mass index (BMI), presence of diabetes, bone health (osteoporosis/osteopenia), scoliosis (Cobb angle of more than 10° in the coronal plane), 11 lumbosacral transitional anatomy, smoking status, previous lumbar or lumbosacral surgery, presence of complications (hematoma, pseudoarthrosis, wound-related issues), neurological complication (radicular pain, neural impingement, lower extremity paresis, or paresthesia), surgical procedure (side, primary, late revision, contralateral), need of early revision (<3 months), the configuration of implants (Type A and Type B) (Figure 1), use of triangular versus 3-D printed implants, type of IONM used (EMG, SSEP, tcMEP, triggered EMG), IONM change from baseline and VAS improvement 3 months after surgery. For SSEPs, posterior tibial nerve and ulnar nerve SSEPs were recorded bilaterally and average responses were obtained relatively continuously throughout the procedure. For EMG and MEP monitoring, bipolar differential recordings were obtained from each muscle using subdermal uninsulated electrodes inserted approximately 2 cm apart in the same muscle. Quadriceps, tibialis anterior, gastrocnemius, and foot intrinsic muscles were recorded bilaterally. The alert guidance for SSEPs was a 50% or greater attenuation from recent values. The alert guidance for spontaneous EMG was sustained putative neurotic activity, and the alert guidance for MEPs was a 50-75% amplitude attenuation.

Configuration of sacroiliac fusion implants.
Statistical Analysis
Statistical analysis was conducted using SPSS software, Version 26.0 for Windows (IBM Co., Chicago, IL, USA). The primary exposure of interest was the intraoperative guidance modality (Fluoroscopy vs. 3-dimensional navigation system) used. The primary metric of interest was the occurrence of neurological complications, defined as a binary variable, and its association with changes in the IONM. Categorical variables were reported as frequency and percentage, and continuous variables were reported as mean and standard deviation. Univariate comparisons between cohorts were conducted using a chi-square test, Fisher’s exact test, the unpaired 2-tailed Student’s t-test and the Mann–Whitney U-tests as appropriate based on frequency table cell counts, and assumptions of normality. A p-value <0.05 was set for statistical significance.
Results
Descriptive Data
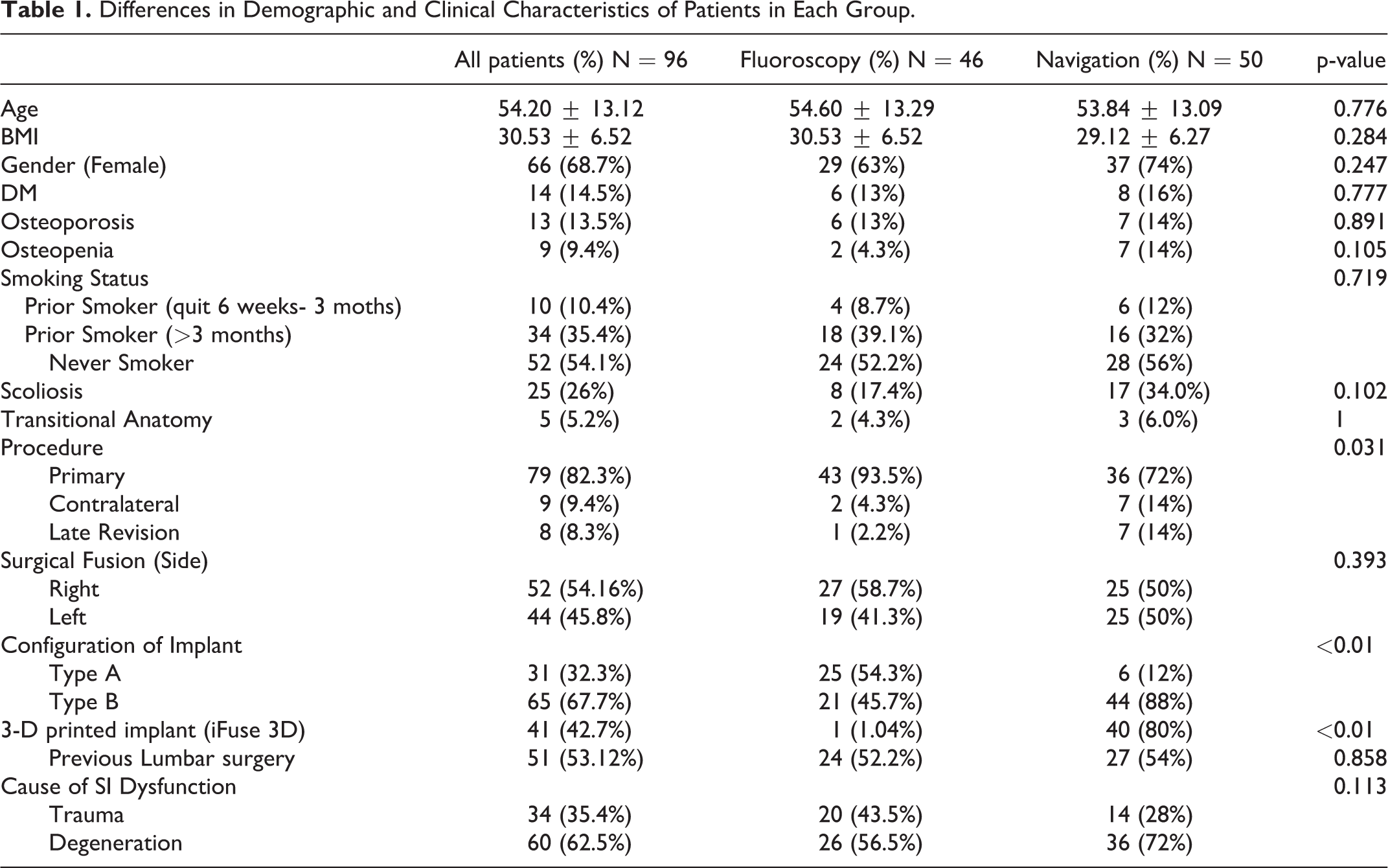
A total of 96 patients were analyzed. The population demographics categorized by the subgroup of patients are summarized in Table 1, and the trends in the choice of both intraoperative image-guidance modalities throughout the years studied are shown in Figure 2. The only variables that were statistically different between both cohorts of patients were the subtype of procedure (primary, contralateral, late revision) (p = 0.03), the configuration of implants (type A and type B) (p < 0.01), the use of 3D-printed implants (p < 0.01), and the type of IONM modality used, EMG with SSEP (p < 0.01), SSEP and tcMEP (p < 0.01). The range of ages for patients undergoing SI joint fusion was from 29 to 83 and the mean age of patients analyzed was 54.2 ± 13.1, 66% were female, 13.5% had a history of osteoporosis treated with teriparatide before the procedure (2 patients were late revisions), 36.8% had a history of smoking 6 weeks or more before the surgery (all patients who had surgery had no nicotine levels detected at the time of the procedure), 26% had scoliosis, and 5.2% had a lumbosacral transitional anatomy (Tables 1 and 2).
Differences in Demographic and Clinical Characteristics of Patients in Each Group.
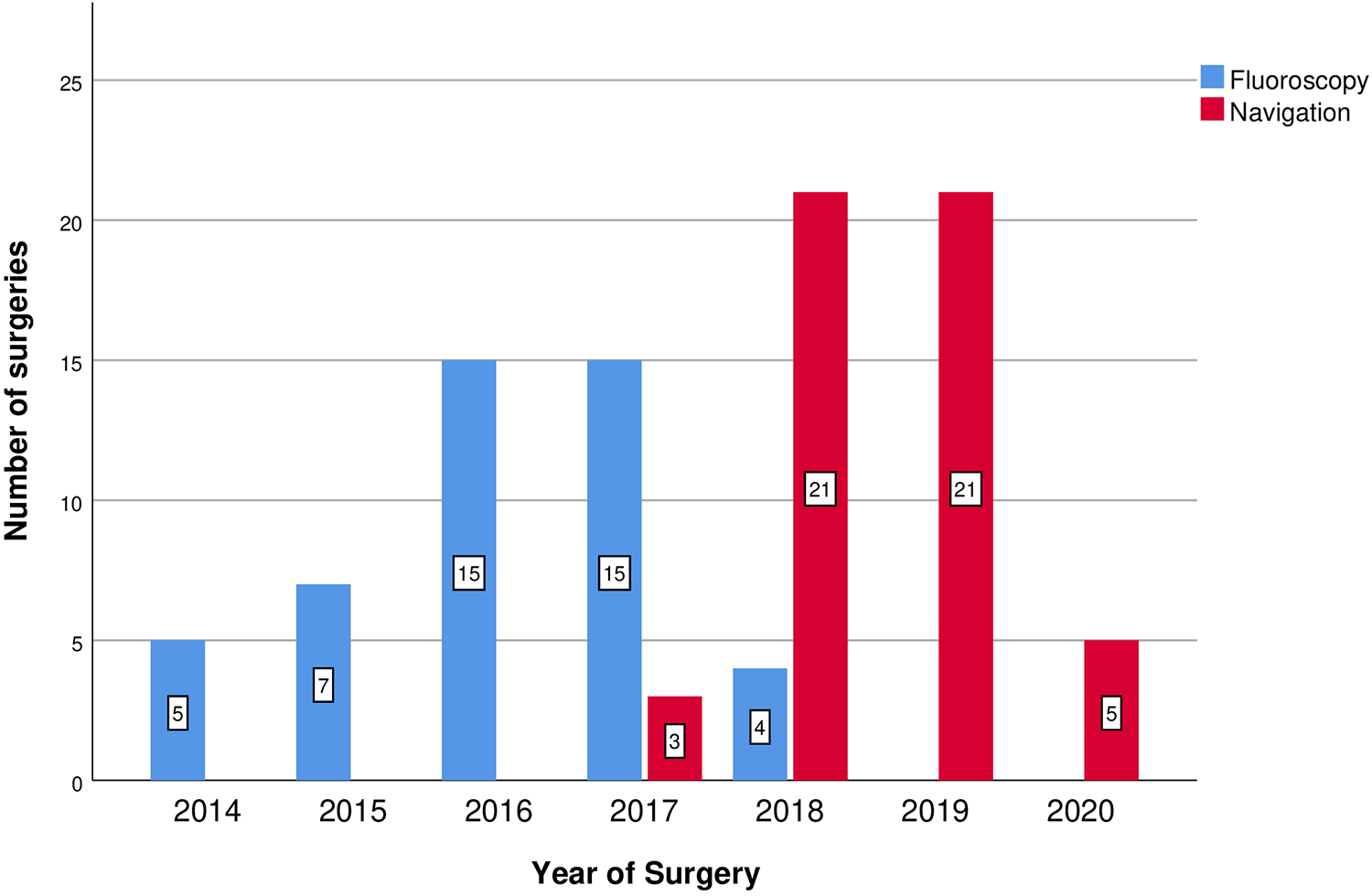
Number of surgeries per year that fluoroscopy and stereotactic navigation was used in the study timeline.
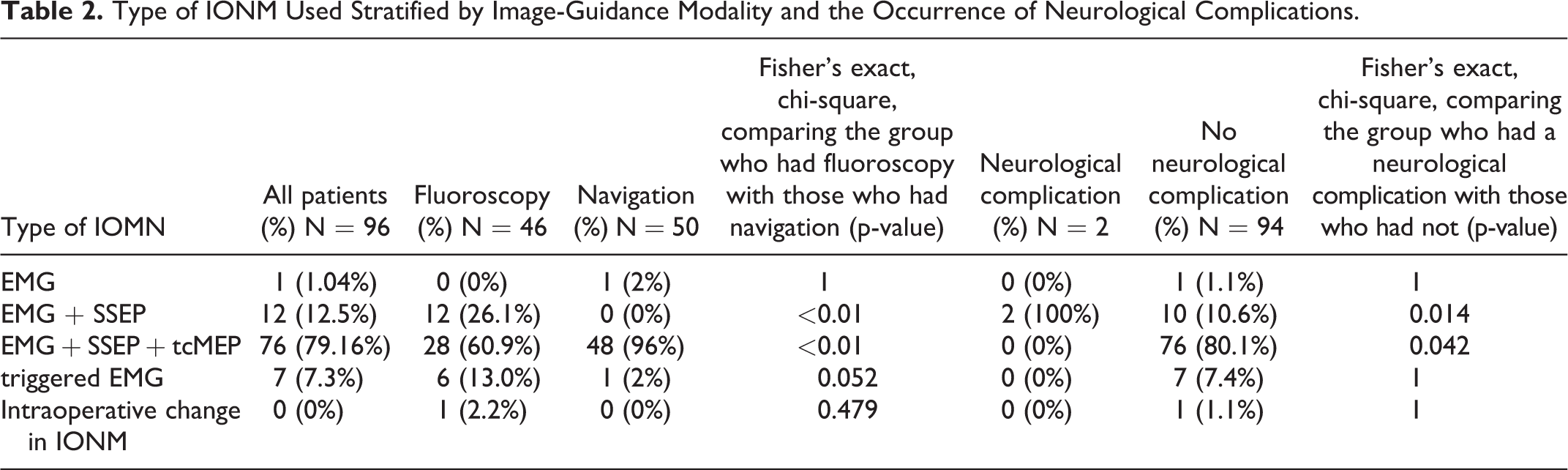
Type of IONM Used Stratified by Image-Guidance Modality and the Occurrence of Neurological Complications.
Out of the 96 patients analyzed, 82.3% had a primary SI joint fusion. 53.12% of the patients had a previous lumbar surgery. The neurological complication rate was 2.08%, 4.2% of the cases were complicated by pseudoarthrosis, and 5.2% of patients underwent an early revision. The implant configuration most commonly used was the type B (67.7%), 42.7% of patients had the newer 3D printed implant, and the most common SI dysfunction etiology was to degenerative pathology (62.5%). The most common IONM modality combination used was the association of electroneuromyography (EMG), somatosensory evoked potential (SSEP), and transcranial motor evoked potentials (tcMEP) (79.16%) (Tables 1 and 2).
Main Results
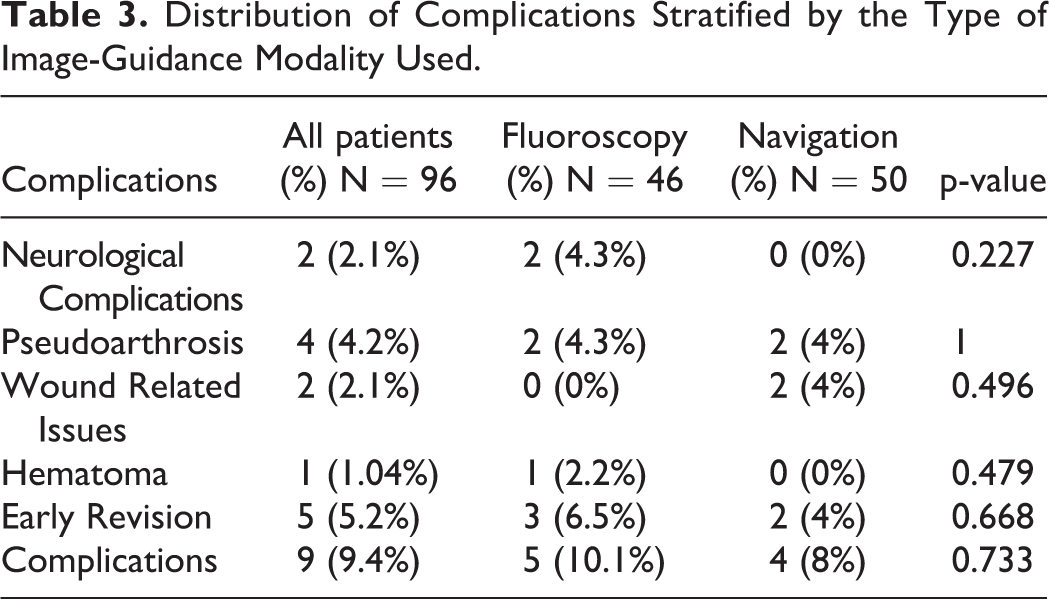
The occurrence of neurological complications was compared between the group of patients who underwent MIS SI joint arthrodesis image-guided by fluoroscopy (2 [4.3%]) and by a stereotactic navigation system (0 [0%]). All the patients who had neurological impingement recorded in this cohort of patients were from the fluoroscopy group, although the difference between the groups did not reach statistical significance (p = 0.227). The association of the different intraoperative guidance modalities and the occurrence of pseudarthrosis was also analyzed, and no significant difference was found between the fluoroscopy (2 [4.3%]) and the navigation (2 [4%]) group of patients (p = 1.00) (Table 3). The use of 3D printed implants was also not associated with the occurrence of pseudoarthrosis (p = 1.00).
Distribution of Complications Stratified by the Type of Image-Guidance Modality Used.
The association between IONM modality used and the occurrence of neurological injury was evaluated. A significant association was found between the group of patients who experienced a neurological complication and the use of EMG and SSEP alone (p = 0.01)). In addition the use of tcMEP was associated with no neurological injury postoperatively (0.042). The 2 patients who had a neurological complication postoperatively (S1 radiculopathy and sensory deficit in the right leg) were monitored only with EMG and SSEP, representing 16.7% (2/12) of patients who had a SI joint fusion and this combination of IONM. The sensitivity and specificity of MEPS was 100% as 76/76 patients had no uncorrected MEP changes and no postoperative deficit; in contrast, the 2 patients with neurological complications did not have MEP monitoring, and thus the sensitivity of SSEPs and EMG alone was 0%. None of the patients who were monitored alone with EMG and SSEP had any change in the baseline signal of the neurophysiology studies recorded intraoperatively. Out of the 76 patients monitored with MEP, 1 (1.3%) patient had the gastrocnemius MEP attenuated greater than 50% and an alert was generated, postoperatively this patient was neurological intact (Table 2).
The overall complication rate (percentage of patients who experienced a neurological complication, needed an early revision or developed pseudoarthrosis) in the study was 9.4%, and there was no significant difference between the fluoroscopy (5 [10.1%]), and the navigation group (4 [8%]) (p = 0.733). The early revision rate between the fluoroscopy (3 [6.5%]) and the navigation group (2 [4%]) was also not significantly different (0.668). However, all the cases that needed an early revision in the fluoroscopy group were implant position related were as in the navigation group all were for wound-related issues (Table 3).
The patient-reported pain improvement after surgery was also a variable of interest evaluated. The mean pain improvement 3 months after surgery was greater in the navigation group (2.44 ± 2.72), but was not statistically different than the improvement in the fluoroscopy group (1.90 ± 2.07) (p = 0.301) (Figure 3).
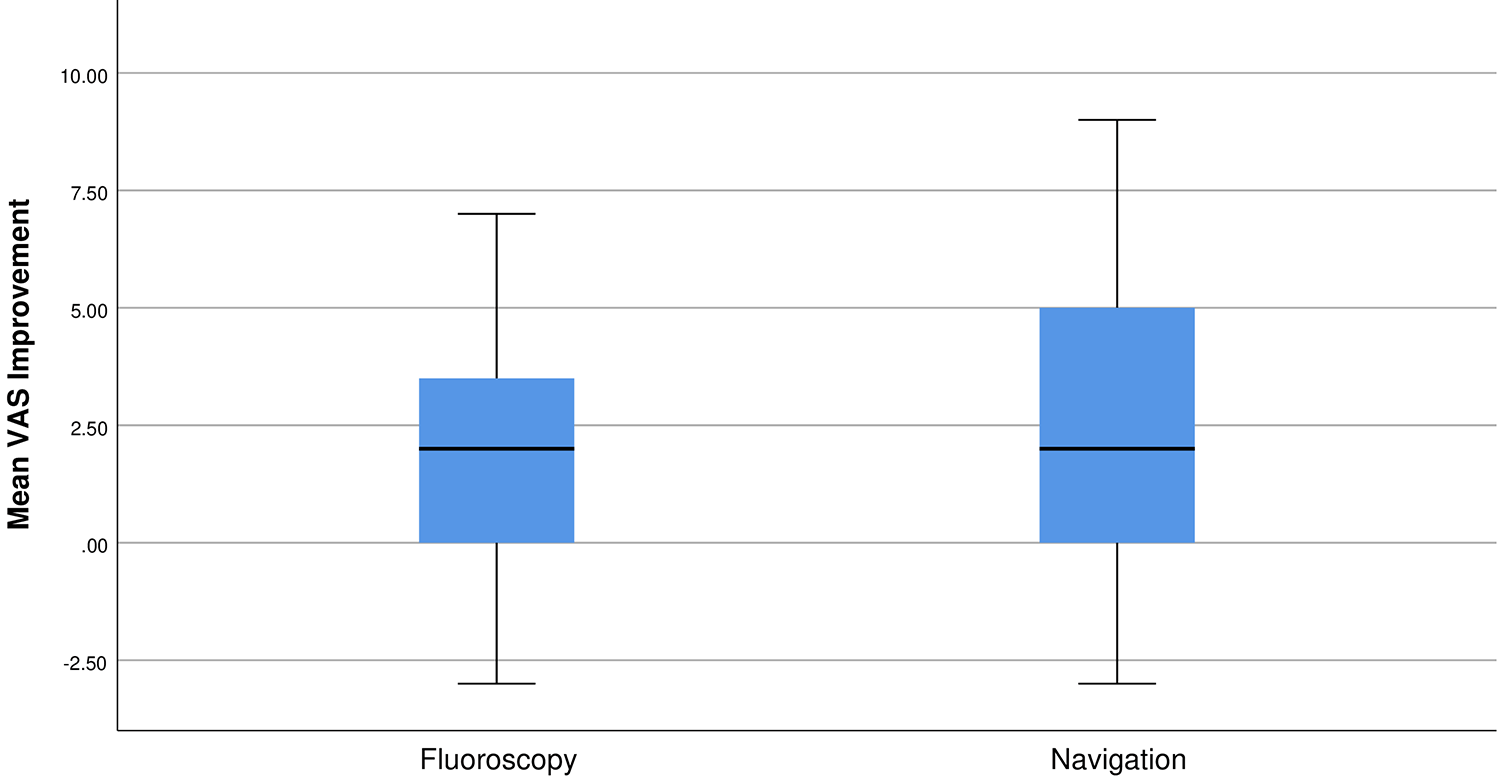
Box/whisker plot for the distribution of change in in VAS in Sacroiliac Fusions, stratified by image-guidance modalities. Box/whisker plot box upper/lower bounds are the 25% and 75% limits (Interquartile Range).Solid lines are the mean delta VAS.
Discussion
Chronic back pain is prevalent in the United States, affecting up to 40% of the population. 12 The sacroiliac joint may be responsible in up to one-third of these cases.1-3 The number of SI joint fusion procedures performed in the United States has increased dramatically in recent years with the advent of MIS techniques to address the pathology. It is believed that the popularity MIS technique has contributed to a 4 times increase in SI fusions from 2014 to 2019.13,14 In addition, there may be a trend in the change of the use of intraoperative image-guidance modalities from fluoroscopy to 3-dimensional navigation systems.
The safety and efficacy of the SI joint arthrodesis is a topic of growing interest given the increase in the utilization of minimally invasive techniques for the treatment of non-traumatic SI joint pain. 13 The overall neurological complication rate of 2.1% determined by this study is in good agreement with findings from other investigations that reported rates ranging from 0.9% to 6.2% .14,15 All the neurological complications reported were in the fluoroscopy group. Still, as the ratio of neurologic injury was low, no statistically significant difference was found between both intraoperative image-guidance modalities analyzed.
The use of IONM techniques have been increasing in different spinal procedures, although its cost-effectiveness has not been demonstrated in the SI joint arthrodesis. 16 This study demonstrated that only 1 patient from both of the cohorts analyzed had a change in the baseline signals in the neurophysiologic studies during the surgical intervention and both of the cases who experienced a neurological injury the IONM modality used (EMG and SSEP alone) showed no changes in the waveform, which questions the cost-effectiveness use of this IONM modalities.
The reduction of the tcMEP waveform has been previously associated with neurological injury in lumbosacral spine fusion patients, suggesting that this association might also be true in the SI joint arthrodesis. 17 Even though a statistical association between the use of tcMEP and the absence of neurological damage has been found in the study suggesting that tcMEPS reliably predict intact neurologic function, this significance needs to be analyzed cautiously before translated into improved safety, given the absence in the change of the baseline signal of IONM in the majority of patients analyzed in this study, and the patient who had a change in the baseline signals had no damage postoperatively, which cannot be disregarded as a possible false positive. The value of routine IONM is still to be determined and studies with a greater number of patients should be reproduced to confirm this association and to determine the cost-effectiveness of the routine use of IONM.
The overall complication rate of the cohort o patients analyzed was 9.4%, also in agreement with other studies that range from 3.5% to 18%.14,15,18 Despite the fact that there was no significant difference between the fluoroscopy and the navigation group, half of the complications observed in the navigation group were outweighed due to wound-related issues at the navigation pin site. In contrast, 10.1% of all patients from the fluoroscopy group had a complication recorded, and 40% of them (2/5) were neurological complications.
Finally, no substantial difference was noted in the pain improvement comparing the fluoroscopy and the stereotactic navigation group. This result suggests that despite fluoroscopy being a less traumatic intraoperative image-guidance technique, it is not associated with less pain postoperatively in comparison with the patients who underwent the same procedure image-guided by the navigation technique.
Limitations
This retrospective study evaluated the impact of the use of intraoperative guidance modalities and the use of IONM in the safety and complication rates of MIS SI joint fusions. Despite the efforts to minimize bias and to standardize both groups analyzed, this study has limitations. Given that the results reflect findings at a single institution, the external validity is limited. The small sample of some subgroups of the cohort analyzed may have biased some results. Although the data has been collected prospectively, the analysis of data has been done retrospectively. Despite the fact that both groups were shown to not be statistically different with respect to the neurological complications, there may have been other variables not assessed that impacted results.
Conclusions
This study evaluated the safety of the use of different intraoperative image-guided modalities in the surgical treatment of SI joint dysfunction and showed no difference in overall complications or neurological injury between the fluoroscopy and the stereotactic navigation technique. The association of the tcMEPS seems to contribute to the safety of the SI joint fusion, but the value of routine IONM is still to be determined. Further studies are necessary to clarify the impact of neurophysiological monitoring in the safety of this procedure and the cost-effectiveness of its routine use.
Footnotes
Authors’ Note
No portion of the paper has been presented previously, published, or submitted for review in any other journal.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors do consulting with SI-Bone, but they did not sponsor or financially support the study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.