
Abstract
Study Design:
A retrospective study.
Objective:
To investigate the effect of pedicle subtraction osteotomy (PSO) level on the surgical outcomes in ankylosing spondylitis-related thoracolumbar kyphosis with the same curve pattern.
Methods:
ankylosing spondylitis (AS) patients with thoracolumbar kyphosis, who underwent 1-level lumbar PSO between March 2006 and June 2017, were retrospectively reviewed. Criteria for curve-matched thoracolumbar kyphosis were: (1) have same level of preoperative apex (pre-apex); (2) have similar global kyphosis (GK, the angle between the superior/inferior endplate of the maximally tilted upper and lower end vertebra) (the difference of GK less than 15˚). The radiographic parameters measured were sagittal vertical axis (SVA, the horizontal distance between the C7 plumb line and the posterosuperior corner of the S1), GK, thoracic kyphosis (TK, the angle between the T5 superior endplate and the T12 inferior endplate), lumbar lordosis (LL, the angle between the L1 and S1 superior endplate), sacral slope (SS, the angle between the sacral endplate and the horizontal line), pelvic tilt (PT, the angle between the vertical and the line joining the midpoint of the sacral plate and hip axis), and pelvic incidence (PI, the angle between the line vertical to the superior margin of S1 and the line connecting the sacral plate midpoint with the hip joint axis). All of these parameters and health-related quality of life (HRQoL, evaluated by preoperative and the last follow-up questionnaires including ODI and VAS) scores were collected before surgery and at the last follow-up. According to their osteotomy level, patients were devided into 2 sub-groups (L1 group and L2 group), and differences of these mentioned parameters between 2 groups were compared.
Results:
26 curve-matched patients were recruited with a mean follow-up of 37.2 months. All patients improved significantly after surgery in HRQoL scores (VAS 1.6 vs 5.4, P < 0.001; ODI 11.9 vs 26.4, P < 0.001). Except for TK and PI, those radiographic parameters were also observed to be significantly changed after surgery. Compared to L2 group, PSO at L1 may have larger correction of TK (ΔTK -6.8 vs -0.3°, P = 0.164), PI (ΔPI -7.4 vs -0.7°, P = 0.364) and smaller correction of SVA (ΔSVA -105.3 vs -128.5 mm, P = 0.096), LL (ΔLL -31.1 vs -43.0°, P = 0.307) and SS (ΔSS 6.9 vs 12.2°, P = 0.279) but had no statistical significance.
Conclusion:
The results of this investigation showed that in AS-related thoracolumbar kyphosis patients with the same curve pattern, the different levels of osteotomy had little effect on the improvement of surgical outcomes. However, osteotomy at L2 is more likely to obtain a larger correction of SVA compared to osteotomy at L1.
Keywords
Introduction
Thoracolumbar kyphotic deformity (TLKD) is the most common deformity in those patients with ankylosing spondylitis (AS)-related kyphosis. More than 30% of those patients suffer from this condition. 1 When AS-related kyphosis seriously affects the function of patients’ daily life and causes serious psychological burden, pedicle subtraction osteotomy (PSO) at lumbar segment is generally considered as an effective solution.1-3
Relationship between the level of osteotomy and the correction of spinopelvic sagittal alignment following PSO has been investigated in several studies.4-8 Recent work by Lafage et al has reported the correlation between PSO level and the correction of pelvic tilt (PT) (r = -0.41, P < 0.001) in adult spinal deformity (ASD) patients. Greater reduction of PT was observed when the PSO was performed at a more caudal level in their study. 4 In AS-related thoracolumbar kyphosis, Van Royen and Slot hold the view that that the osteotomy level should be selected in the lower lumbar segment for the consideration that more SVA correction might be obtained if the osteotomy was performed at a more distal level. 6 However, preoperative sagittal alignment might also have influence on the improvement of surgical outcomes and no previous studies have compared the correction of spinopelvic sagittal alignment between AS patients undergoing osteotomy at different levels with similar preoperative sagittal curve patterns.
To minimize the potential influence of preoperative sagittal alignment on the improvement of surgical outcomes, the present study compared the correction of spinal sagittal alignment and clinical outcomes between AS patients who underwent 1-level PSO at different levels with similar preoperative sagittal curve patterns.
Material and Methods
A retrospective review of AS patients with thoracolumbar kyphosis hospitalized at one single institution between March 2006 and June 2017 was performed. The indications for the osteotomy in our study were: (1) unable to look straight forward without the help of hips and/or knees flexion; (2) unable to stand upright or lie down flat; (3) severe limitations in daily activities such as walking, sleeping, driving, and interpersonal communication due to thoracolumbar kyphosis; and (4) severe compression of the abdominal visceral organs secondary to thoracolumbar kyphosis.2,3,9
Criteria for selecting the subjects were: (1) pre-operative apex located at T11-L2; (2) underwent single level PSO at L1/L2; (3) at least 2 years of follow-up. Exclusion criteria were having previous spinal surgery, pathological spinal fractures, pseudarthrosis or flexion contractures of the hip joint. Patients without complete HRQoL questionnaires were also excluded. The definition of curve-matched thoracolumbar kyphosis was (1) have same level of preoperative apex (pre-apex); and (2) have similar global kyphosis (GK) (the difference of GK less than 15˚).
From March 2006 to June 2017, out of 242 hospitalized AS patients, 192 patients receved single level PSO and had at least 2 years of follow-up. 71 patients met the above-mentioned inclusion criteria. Finally, 13 couple of patients (21 male and 5 female) met the criteria of curve-matched thoracolumbar kyphosis, while underwent 1-level PSO at different location. The average age of those enrolled patients was 34.7 ± 9.3 years (range, 20-53 years), and the mean follow-up was 37.2 ± 13.7 months (range, 24-60 months). The preoperative apex of the kyphosis was located at T11 in 2 cases, T12 in 8 cases, L1 in 12 cases, and L2 in 4 cases. According to their PSO level, patients were divided into 2 groups: L1 Group (PSO at L1, N = 13) and L2 Group (PSO at L2, N = 13).
Patients underwent lateral whole spine radiography. Radiographs were taken when patients were required to assume a comfortable standing posture, with their arms flexed, and their hands placed on the level of their shoulders using a standard method. 10 All lateral radiographs included hip joints. The sagittal parameters assessed included the following: (1) sagittal vertical axis (SVA, the horizontal distance of a C7 plumb line (C7PL) to the posterosuperior corner of the S1, positive if the C7PL is anterior to the corner of the S1, and ideal sagittal balance was defined as a C7 plumb line less than 50 mm) 11 ; (2) global kyphosis (GK, the angle between the superior endplate of the maximally tilted upper end vertebra and the inferior endplate of the maximally tilted lower end vertebra) 12 ; (3) thoracic kyphosis (TK, the angle between the upper endplate of the T5 vertebra and the lower endplate of the T12 vertebra using Cobb’s method) 13 ; (4) lumbar lordosis (LL, the Cobb angle between the superior endplate of T12 and S1 vertebra, positive if the curve is kyphotic) 12 ; (5) sacral slope (SS, the angle between the sacral endplate and the horizontal line) 14 ; (6) pelvic tilt (PT, the angle between the vertical and the line joining the midpoint of the sacral plate and hip axis, positive if the hip axis is located anterior to the midpoint of the sacral plate), 14 and (7) pelvic incidence (PI, the angle between the line perpendicular to the sacral endplate at its midpoint and the line connecting the midpoint of the sacral plate to the hip axis). 14 PI-LL meant the mismatch between pelvic incidence and lumbar lordosis. Preoperative and the last follow-up questionnaires were requested for HRQoL assessment. 15
Clinical data, including age, sex, number of fused vertebra, intraoperative blood loss, operation duration was reviewed. Preoperative demographic, radiographic and HRQoL scores were compared with those at the last follow-up by the paired-samples t test.16-19 Comparison between 2 groups was also performed. The changes of sagittal parameters and HRQoL scores between preoperatively and at the last follow-up were also compared between 2 groups. The statistical analysis was performed with SPSS version 18.0 software (SPSS Inc., Chicago, IL). A P value of P < 0.05 was considered to be statistically significant.
Results
Out of 26 enrolled patients, comparison of demographics between 2 groups indicated that no significant difference was found in mean age (32.6 vs 36.9 years, P = 0.248) and gender proportion (P = 0.267) between the 2 groups.
Comparison of patients’ radiographic parameters between preoperative and the last follow-up indicated that patients had significant improvement in the radiographic measurements, such as less SVA (151.4 vs 34.5 mm, P < 0.001), GK (66.8 vs 20.4°, P < 0.001), LL (0.3 vs -36.7°, P < 0.001), PT (36.1 vs 22.4°, P < 0.001), PI-LL (42.6 vs 3.4°, P < 0.001), and larger SS (8.1 vs 17.7°, P < 0.001), except for the TK (45.0 vs 41.5°, P = 0.145) and PI (44.2 vs 40.1°, P = 0.257). Patients’ quality of life also improved significantly, with less VAS (5.4 vs 1.6, P < 0.001) and ODI (26.4 vs 11.9, P < 0.001) (Table 1).
Comparison of Radiographic Parameters and HRQoL Assessments of Patients Between Preoperative and the Last Follow-Up.
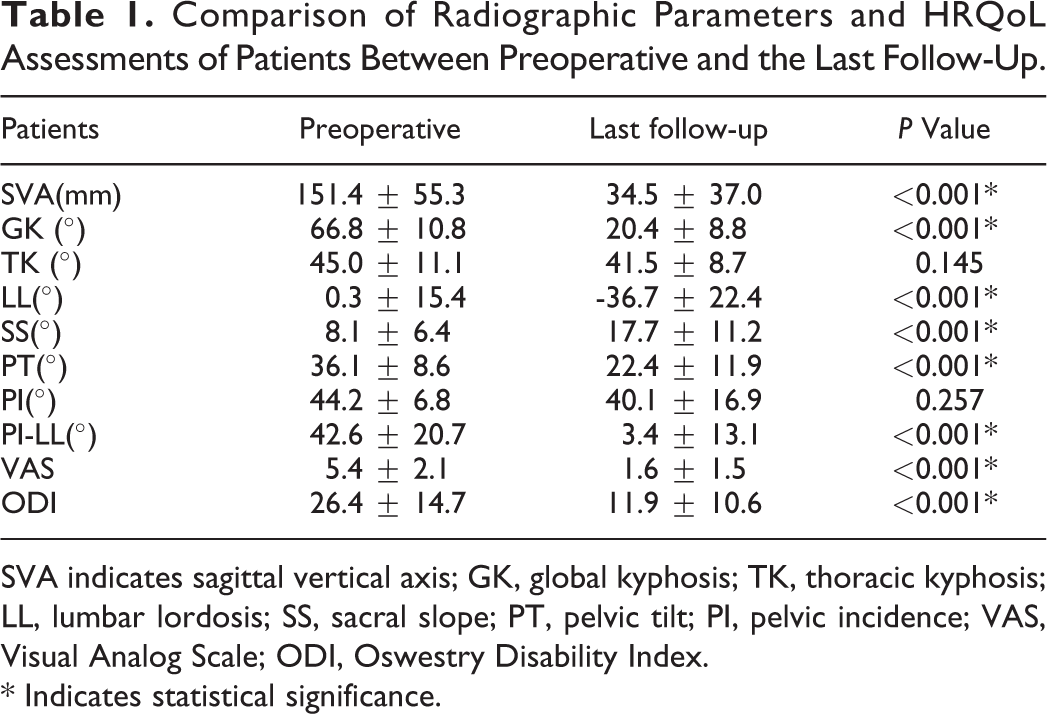
SVA indicates sagittal vertical axis; GK, global kyphosis; TK, thoracic kyphosis; LL, lumbar lordosis; SS, sacral slope; PT, pelvic tilt; PI, pelvic incidence; VAS, Visual Analog Scale; ODI, Oswestry Disability Index.
* Indicates statistical significance.
Comparison of preoperative radiographic parameters between the L1 Group and L2 Group showed that patients in L1 Group have less SVA (141.9 vs 160.9 mm, P = 0.067) and larger SS (9.8 vs 6.5°, P = 0.094) compared with those in L2 Group, and other radiographic parameters showed no significant difference. According to the comparison of HRQoL measurements, no significant intergroup difference was observed (Table 2). There was also no significant difference in the proportion of osteotomy at the kyphosis apex between the 2 groups (4/13 vs 2/13, χ2 = 0.867, P = 0.352).
Comparison of Radiographic Parameters and HRQoL Assessments Between 2 Groups at Preoperative and the Last Follow-Up.
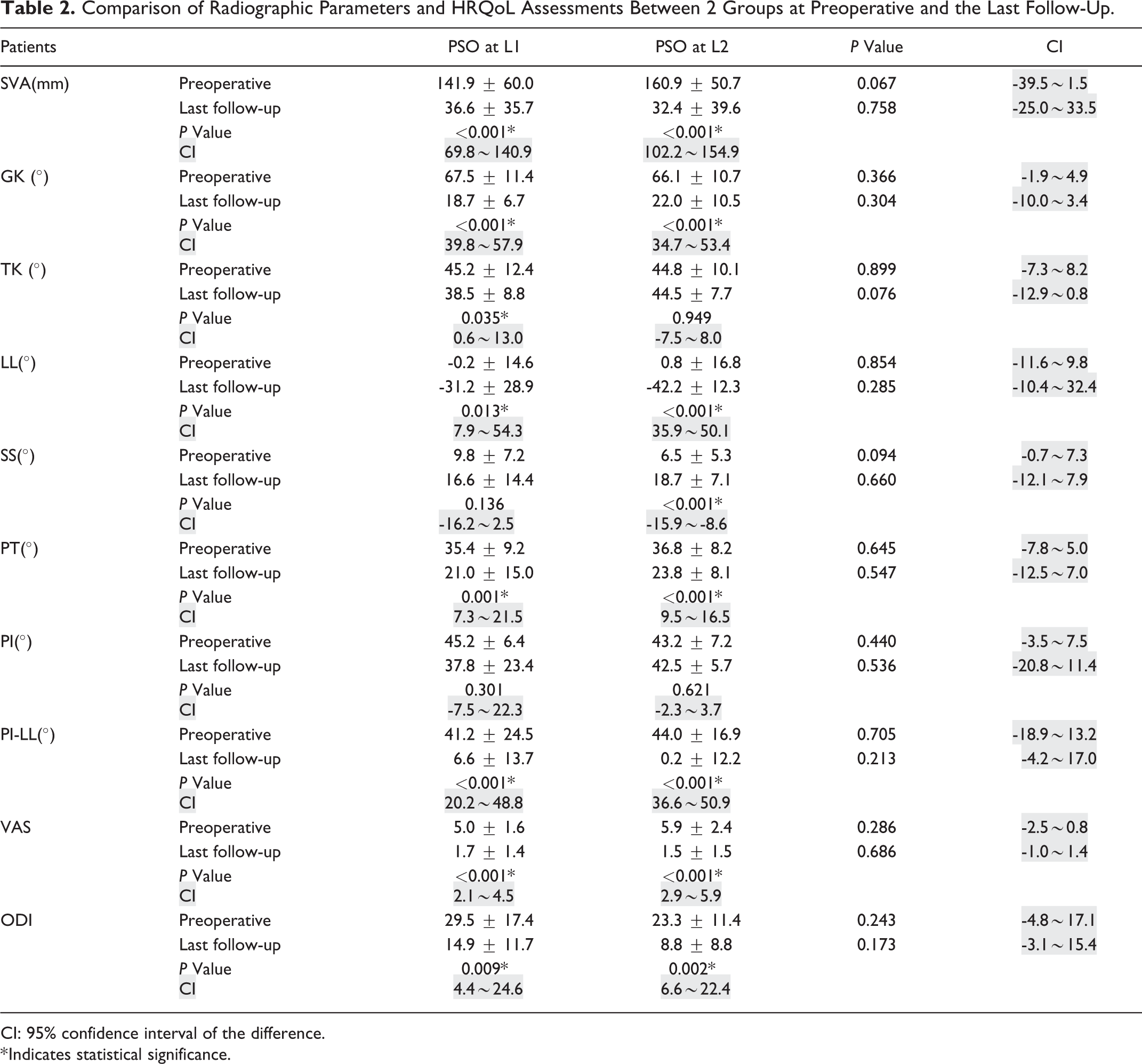
CI: 95% confidence interval of the difference.
* Indicates statistical significance.
At the last follow-up, 17 of 26 patients (65%) maintained their ideal sagittal alignment (SVA < 50 mm), correction of the SVA was similar in patients who received osteotomies at L1 and L2 (8 of 13 patients vs 9 of 13 patients, P > 0.05). The comparison of radiographic parameters indicated that patients in L1 Group seemed have lower TK (38.5 vs 44.5°, P = 0.066) compared with those in L2 Group, but also had no statistical significance. For HRQoL measurements, there was no significant difference between these 2 groups(Table 2). According to the criteria mentioned in the study of Schwab, the optimal sagittal alignment were: PT < 22°; PI-LL < 10°; and SVA < 47 mm. 20 The proportion of patients who met this criteria after surgery were also compared and no significant difference was observed between the 2 groups (2/13 vs 4/13, χ2 = 0.867, P = 0.352). The preoperative and the last follow-up sagittal parameters and HRQoL scores were also compared in each group. In both groups, almost all the radiographic measurements and HRQoL scores were significant improved after PSO. While in L1 Group, SS (9.8 VS 16.6°, P = 0.136) and PI (45.2 vs 37.8°, P = 0.301) had no significant difference between preoperative and the last follow-up. In L2 Group, no significant difference was found in TK (44.8 vs 44.5°, P = 0.949) and PI (43.2 vs 42.5°, P = 0.621) (Table 2).
The changes of spino-pelvic parameters and HRQoL scores from preoperative to the last follow-up were analyzed between groups. Results showed that PSO at L1 may lead to larger correction of TK (-6.8 vs -0.2°, P = 0.164), PI (-7.4 vs -0.7°, P = 0.364) and smaller correction of SVA (-105.3 vs -128.5 mm, P = 0.096), LL (-31.1 vs -43.0°, P = 0.307) and SS (6.9 vs 12.2°, P = 0.279) but still had no significant difference. The improvement of HRQoL scores also revealed no statistical significance between groups (Table 3).
Comparison of the Changes of Radiographic Parameters and HRQoL Assessments Between 2 Groups.
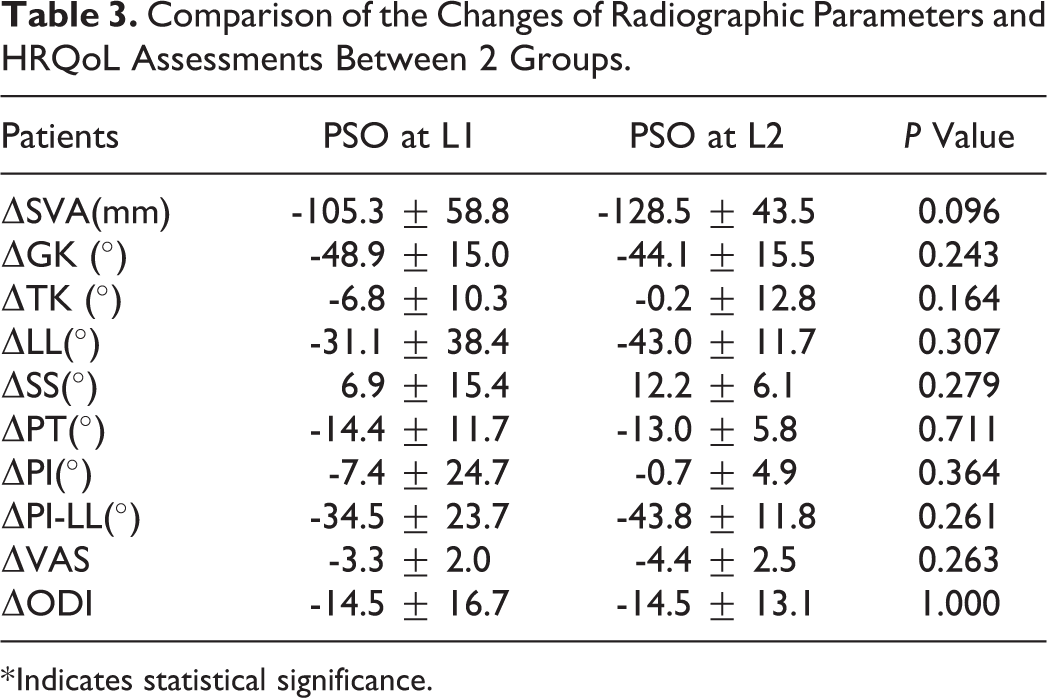
* Indicates statistical significance.
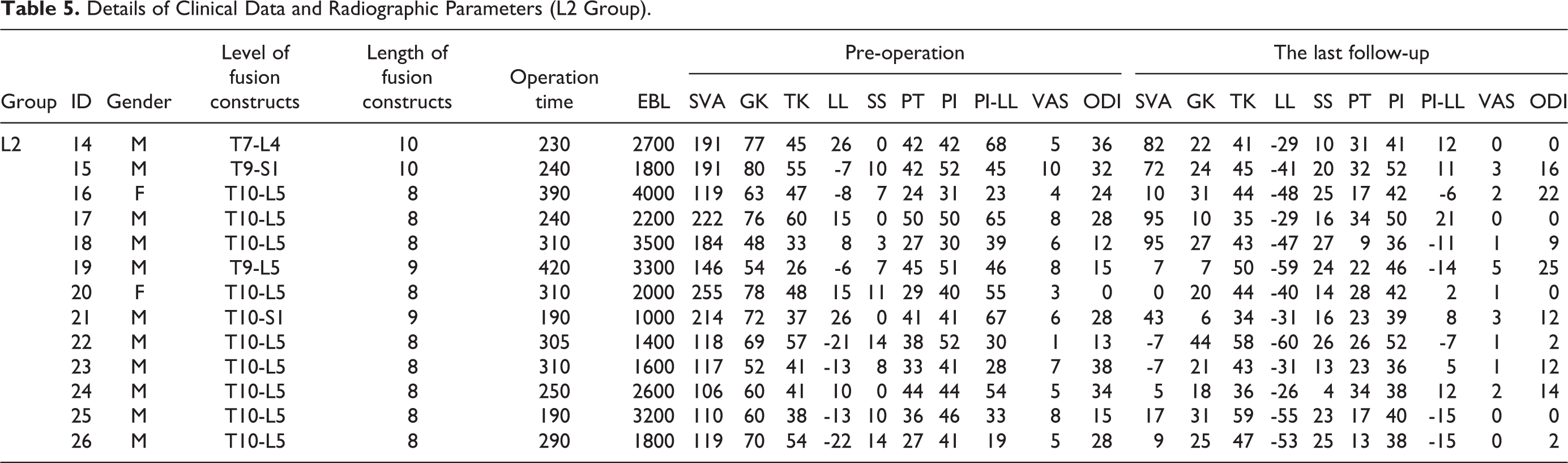
The average operative time was 280 min (range, 190-420 min) for L1 group and 300 min (range, 180-400 min) for L2 Group (P > 0.05). The mean blood loss in L1 group was 2400 ml (range, 1000-4000 ml) and 1800 ml (range, 800-3200 ml) in the other group (P > 0.05). The average length of fusion constructs also had no difference between the 2 groups (8.53 vs 8.46, P > 0.05) (Tables 4 and 5).
Details of Clinical Data and Radiographic Parameters (L1 Group).
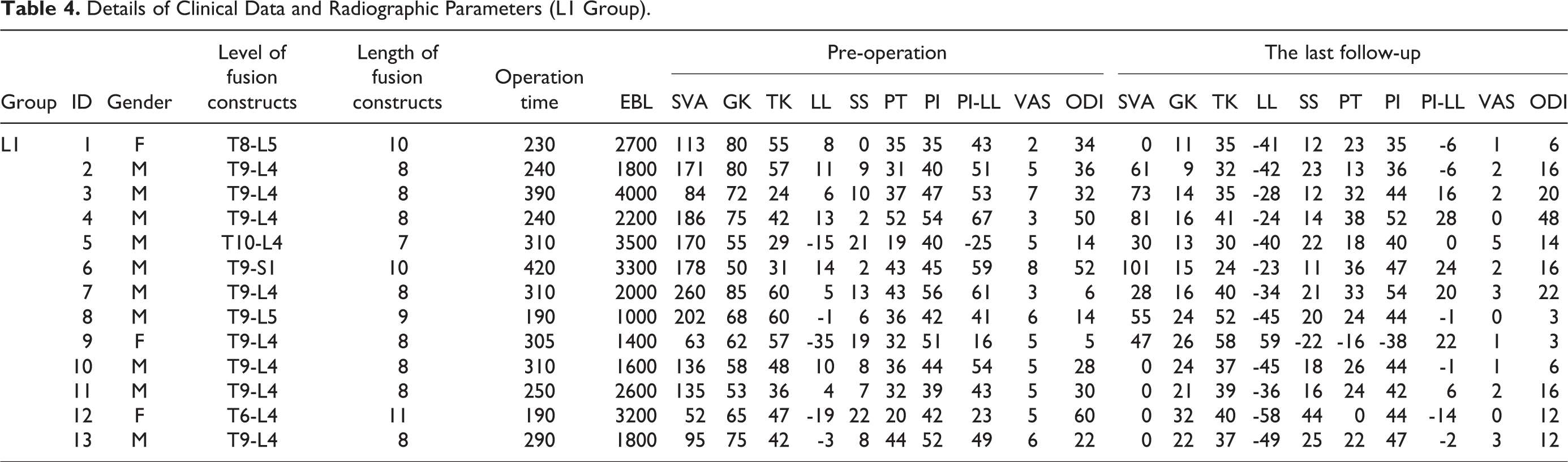
Details of Clinical Data and Radiographic Parameters (L2 Group).
Totally, 5 patients (19.2%) presented with complications. In L1 group, 1 patient had dura tear during the operation; 1 patient had intraoperative vertebral subluxation; the last one had wound dehiscence. There were 2 patients with complications in L2 group, 1 patient had intraoperative vertebral subluxation; the other one had rod fracture and received revision surgery. The complication rates showed no significant difference (3/13 vs 2/13, P > 0.05) between the 2 groups.
Discussion
A strong relationship between HRQoL scores and sagittal parameters (expecially SVA) in AS-related thoracolumbar kyphosis patients has been reported in the literature.4-7 Sagittal parameters of thoracolumbar kyphosis caused by AS can be a indispensable reference for spine surgeons to make surgical decision.21,22 A retrospective cohort studies of Qian et al analyzed those patients with AS-related thoracolumbar kyphosis, and their results showed that patients with large preoperative SVA and large PI are more likely to have postoperative sagittal imbalance after lumbar PSO. 1 However, studies comparing the improvement of clinical and radiographic outcomes in AS patients with curve-matched kyphosis undergoing PSO at different levels were both rare.1,4,7 This retrospective study attempted to compare the improvement of radiographic parameters and clinical outcomes between AS patients who underwent PSO at different levels with similar preoperative sagittal alignment and curve-matched patterns.
Except for TK and PI, almost all of the sagittal parameters were significantly improved after PSO. At the last follow-up, the mean GK significantly reduced from 66.8° to 20.4°. The mean LL significantly changed from 0.3° to -36.7°. The mean SVA was also obviously reduced from 151.4 mm to 34.5 mm. The study of Qian et al in 2016 reported that in those patients with AS-related thoracolumbar kyphosis, their average correction of GK was 46.2°, LL was 45.1° and SVA was 113 mm. 23 The correction of the aforementioned parameters observed in our study was comparable with the results of those previous studies.11,14,23
At the last follow-up, patients in L1 Group had lower TK compared with those in L2 Group. This result was conformed to the results from previous studies in adult spinal deformity patients. 5 According to the standards of optimal sagittal alignment proposed by Schwab et al, the proportion of patients who met the criteria after surgery had no significant difference between the 2 groups in this study. These findings suggested that there might be no significant relationship between osteotomy level and postoperative spinopelvic alignment in AS patients with similar preoperative curve.
Comparison of radiographic parameters between preoperative and the last follow-up was performed. The comparison of correction of radiographic measurements in each groups showed that PSO at L1 corrected the sagittal imbalance mainly through thoracic segment, such as TK. While PSO at L2 corrected the sagittal imbalance mainly through lower part of spine, such as LL and SS. The comparison of changes of radiographic measurements indicated that PSO at L2 had larger changes in SVA, although had no statistical significance (P = 0.096) (Table 3, Figures 1 and 2), which was similar to the results of Lafage et al showing that no evidence was found for a linear associations between osteotomy level and sagittal balance (SVA). 4
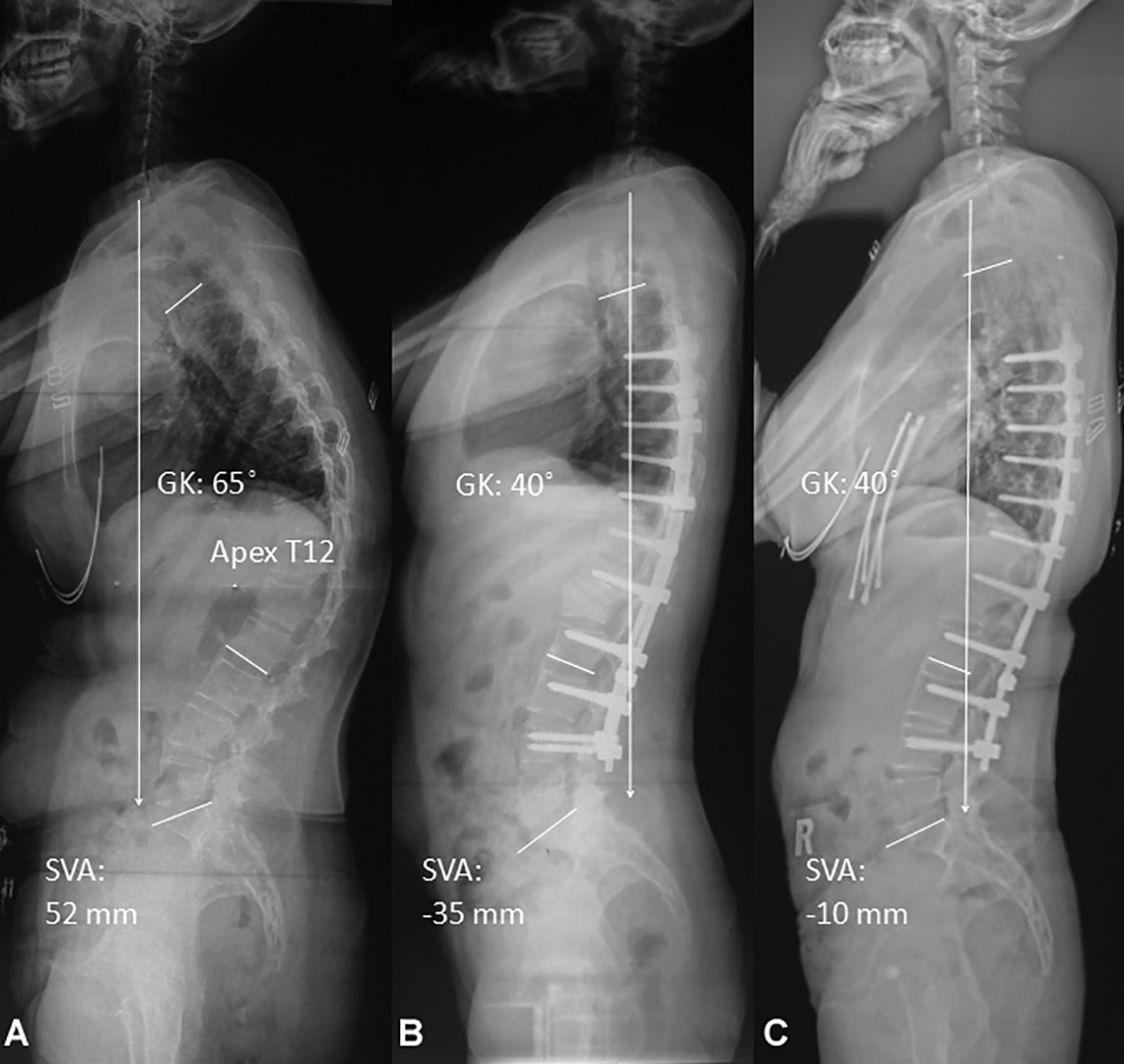
A 23-year-old female AS patient with apex at T12 and underwent PSO at the level of L1. The preoperative SVA was 52 mm, GK was 65˚ (a). Postoperative measurements were SVA of -35 mm, GK was 40˚ (b). At 5-year follow-up, SVA was -10 mm, GK was 40˚ (c).
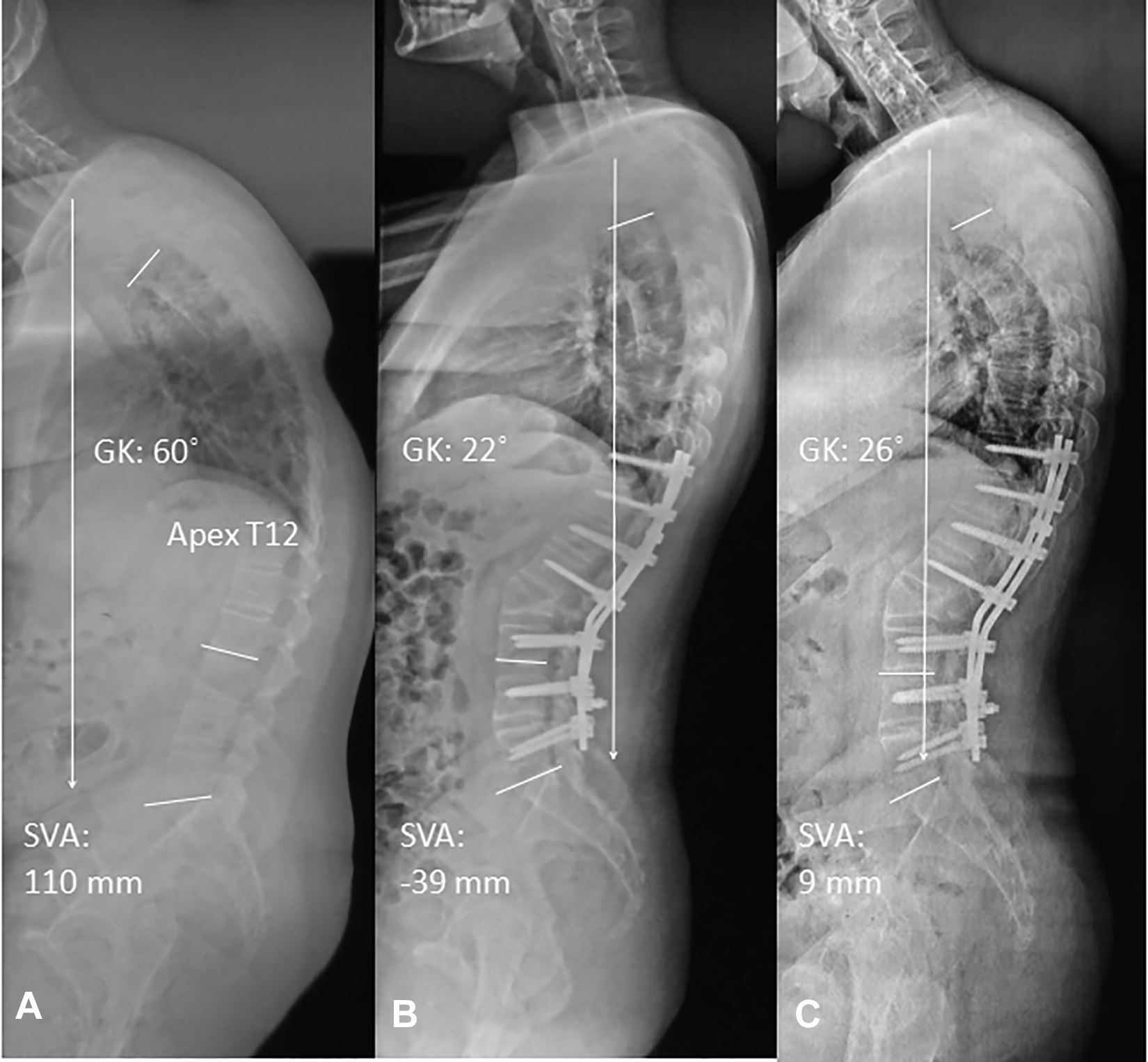
A 24-year-old male AS patient with apex at T12 and underwent PSO at the level of L2, curve-matched with Figure 1. The preoperative SVA was 110 mm, GK was 60˚ (a). Postoperative measurements were SVA of -39 mm, GK was 22˚ (b). At 6-year follow-up, SVA was 9 mm, GK was 26˚ (c).
The proportion of osteotomy at the kyphosis apex was compared between the 2 groups and no significant difference was observed (χ2 = 0.867, P = 0.352), which further indicated that the possible influencing variable (the osteotomy level) relative to the kyphosis apex was well-controlled in this study, which reduced the influence of this variable on the present study.
According to the comparison of HRQoL assessment, both ODI and VAS scores were significantly improved after surgery in each groups. 24 Surprisingly, no significant difference was found in the improvement of these scores between the 2 groups. In our study, AS patients had significant improvement in HRQoL scores while had similar HRQoL scores, although they underwent different level of PSO, and this was comparable to those previous studies in AS patients. 25 Improvement in HRQoL assessment between preoperative and the last follow-up also revealed no significant difference between 2 groups. The comparison of operation time, EBL and complications also indicated that there was no significant difference between 2 groups (P > 0.05).26-29 One possible explanation for these observations is the change of their expectation of quality of life. Postoperatively, AS patients usually have obvious correction for their kyphosis and restore their self-care ability, and the expectation of these patients have changed after surgery. It was interesting that although some patients with AS-related thoracolumbar kyphosis had sub-optimal correction of sagittal alignment, they could also lead a relatively satisfying life. These similar finding were mentioned in the study of Liu. 25 The limitations of our study should be acknowledged. Firstly, it was a retrospective single-center study. Secondly, the sample size was relatively small, which may be due to the strict inclusion criteria in this study. To reduce the influence of the preoperative curve pattern on surgical outcomes, only the patients with curve-matched thoracolumbar kyphosis were included. Therefore, the number of patients for analysis in this study was significantly limited. Future studies with larger sample size were needed to confirm our results.
Conclusion
This study demonstrated that in AS patients with curve-matched thoracolumbar kyphosis (with similar sagittal alignment before surgery), the different levels of osteotomy had little effect on the improvement of surgical outcomes. There was a trend that osteotomy at L2 might obtain a larger correction of SVA compared to the osteotomy at L1.
Footnotes
Authors’ Note
The manuscript submitted does not contain information about medical device(s)/drug(s).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.