
Abstract
Study Design:
Systematic review.
Objectives:
Synthesize previous studies evaluating clinical utility of preoperative Hb/Hct and HbA1c in patients undergoing common spinal procedures: anterior cervical discectomy and fusion (ACDF), posterior cervical fusion (PCF), posterior lumbar fusion (PLF), and lumbar decompression (LD).
Methods:
We queried PubMed, Embase, Cochrane Library, and Web of Science for literature on preoperative Hb/Hct and HbA1c and post-operative outcomes in adult patients undergoing ACDF, PCF, PLF, or LD surgeries.
Results:
Total of 4,307 publications were assessed. Twenty-one articles met inclusion criteria.
PCF and ACDF:
Decreased preoperative Hb/Hct were significant predictors of increased postoperative morbidity, including return to operating room, pulmonary complications, transfusions, and increased length of stay (LOS). For increased HbA1c, there was significant increase in risk of postoperative infection and cost of hospital stay.
PLF:
Decreased Hb/Hct was reported to be associated with increased risk of postoperative cardiac events, blood transfusion, and increased LOS. Elevated HbA1c was associated with increased risk of infection as well as higher visual analogue scores (VAS) and Oswestry disability index (ODI) scores.
LD:
LOS and total episode of care cost were increased in patients with preoperative HbA1c elevation.
Conclusion:
In adult patients undergoing spine surgery, preoperative Hb/Hct are clinically useful predictors for postoperative complications, transfusion rates, and LOS, and HbA1c is predictive for postoperative infection and functional outcomes. Using Hct values <35-38% and HbA1c >6.5%-6.9% for identifying patients at higher risk of postoperative complications is most supported by the literature. We recommend obtaining these labs as part of routine pre-operative risk stratification.
Level of Evidence:
III
Keywords
Introduction
Preoperative optimization is an important aspect of successful postoperative recovery in adult patients undergoing spinal surgery.1,2 In addition to baseline patient comorbidities,3-5 there is increasing evidence that abnormal preoperative lab values such as hemoglobin (Hb), hematocrit (Hct), Hemoglobin A1c (HbA1c), and electrolyte abnormalities are risk factors for poor post-operative outcomes.4,6
Hb is a polymeric protein found in red blood cells (RBCs) and is the primary mechanism of oxygen delivery to tissues. Normal lab values range from 14-18 g/dL for males and 12-16 g/dL for females and reflects the concentration of this protein in whole blood. 7 Hct is the percentage of the volume of red blood cells over total blood volume and is an indirect measure of oxygen carrying capacity. Normal Hct values range from 40 to 54% for males and 36 to 48% for females. 7 Low values of either parameter indicates anemia, which can be secondary to many etiologies including iron deficiency, chronic disease or malignancy, and vitamin B12 deficiency. 8 HbA1c is a measure of the percentage of glycated Hb and is associated with diabetes mellitus (DM), with values greater than 6.5% being diagnostic for DM. 9 Elevated HbA1c is associated with long-term DM complications and is an independent risk factor for stroke and heart disease. 9
To our knowledge, there are no comprehensive systematic reviews on the use of Hb/Hct or HbA1c in preoperative risk stratification for spinal surgery that synthesize the literature and provide an overview of the consensus recommendations. Our aim was to perform a systematic review on the utility of preoperative Hb/Hct and HbA1c for adult patients undergoing 4 common spinal procedures: anterior cervical discectomy and fusion (ACDF), posterior cervical fusion (PCF), posterior lumbar fusion (PLF), and lumbar decompression (LD).
Methods
Protocol
Our systematic review of the literature was constructed in accordance with Preferred Reporting Items and Meta-Analyses (PRISMA) guidelines and protocol. 10
Eligibility Criteria and Information and Search Strategy
Inclusion and exclusion criteria are demonstrated in
Study Selection
Two independent reviewers (K.S and K.W.) performed the initial screening of all studies based on article titles and abstracts. A third reviewer (B.Z.) served as an arbitrator when there was disagreement between the 2 primary reviewers.
Data Extraction and Data Items
The following data was extracted from each study utilizing a standardized data extraction form: title, authors, study design, study cohorts, type of spinal surgery, number of levels operated on, sample size, patient demographics, primary outcome measures, post-operative transfusion rates, mean length of stay (LOS), functional outcomes measures following surgery (visual analog scale (VAS), Japanese Orthopedic Association (JOA) scores, Oswestry Disability Index (ODI)), fusion rate, postoperative complications, and follow-up duration. Reported statistical differences for primary outcomes, including odds ratios and relative risks, were recorded for each included study.
Assessing Risk of Bias and Data Synthesis
2 independent reviewers determined level of evidence, sample size, data source/outcome assessors, and follow-up for each study utilizing a standardized assessment form (
Results
Of the 4307 articles originally identified, we identified 51 for full-text review. Ultimately, 21 articles were included in the systematic review (
Figure 1
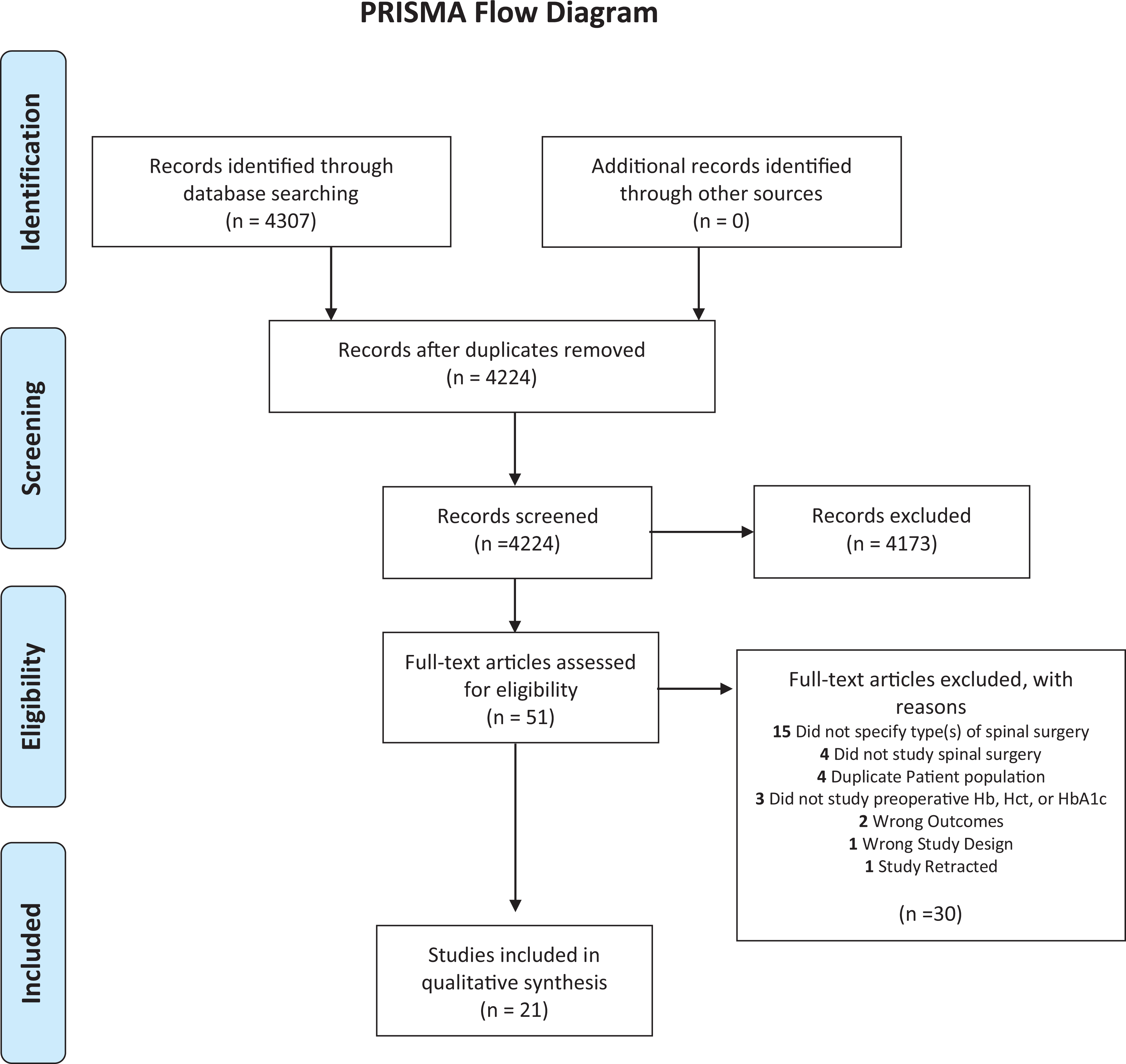
Literature search was performed using PubMed, Embase, the Cochrane library, and web of science databases in July 2020. The purpose was to determine the clinical utility of preoperative hemoglobin/hematocrit and HbA1c in patients undergoing ACDF, PCF, PLF, or LD.
Included Studies Evaluating Preoperative Hemoglobin or Hematocrit Levels and Postoperative Risk Following Spinal Surgery.
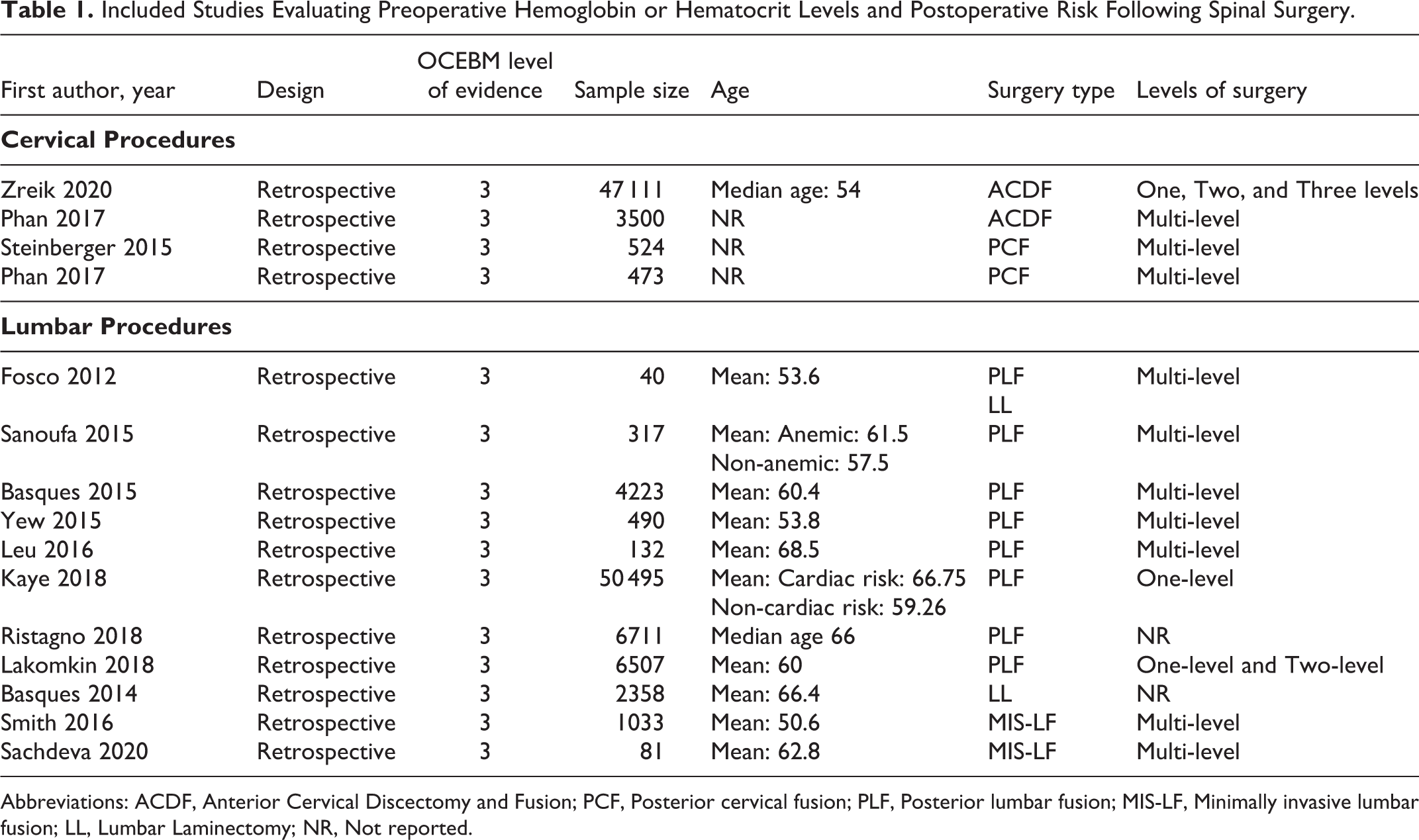
Abbreviations: ACDF, Anterior Cervical Discectomy and Fusion; PCF, Posterior cervical fusion; PLF, Posterior lumbar fusion; MIS-LF, Minimally invasive lumbar fusion; LL, Lumbar Laminectomy; NR, Not reported.
Included Studies Evaluating Preoperative Hemoglobin A1c Levels and Postoperative Risk Following Spinal Surgery.
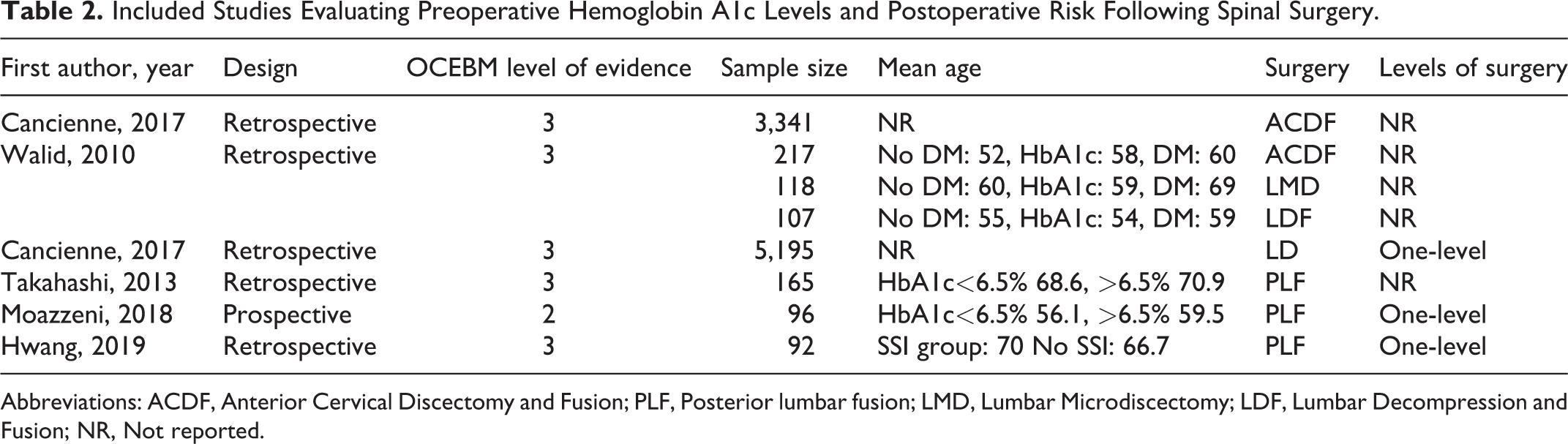
Abbreviations: ACDF, Anterior Cervical Discectomy and Fusion; PLF, Posterior lumbar fusion; LMD, Lumbar Microdiscectomy; LDF, Lumbar Decompression and Fusion; NR, Not reported.
Utility of Preoperative Hemoglobin or Hematocrit in Spinal Surgery
The cut-off value for low Hb/Hct was slightly different for each study and can be found in Table 3 .
Definitions of Anemia or Patient Hemoglobin/Hematocrit Criteria.
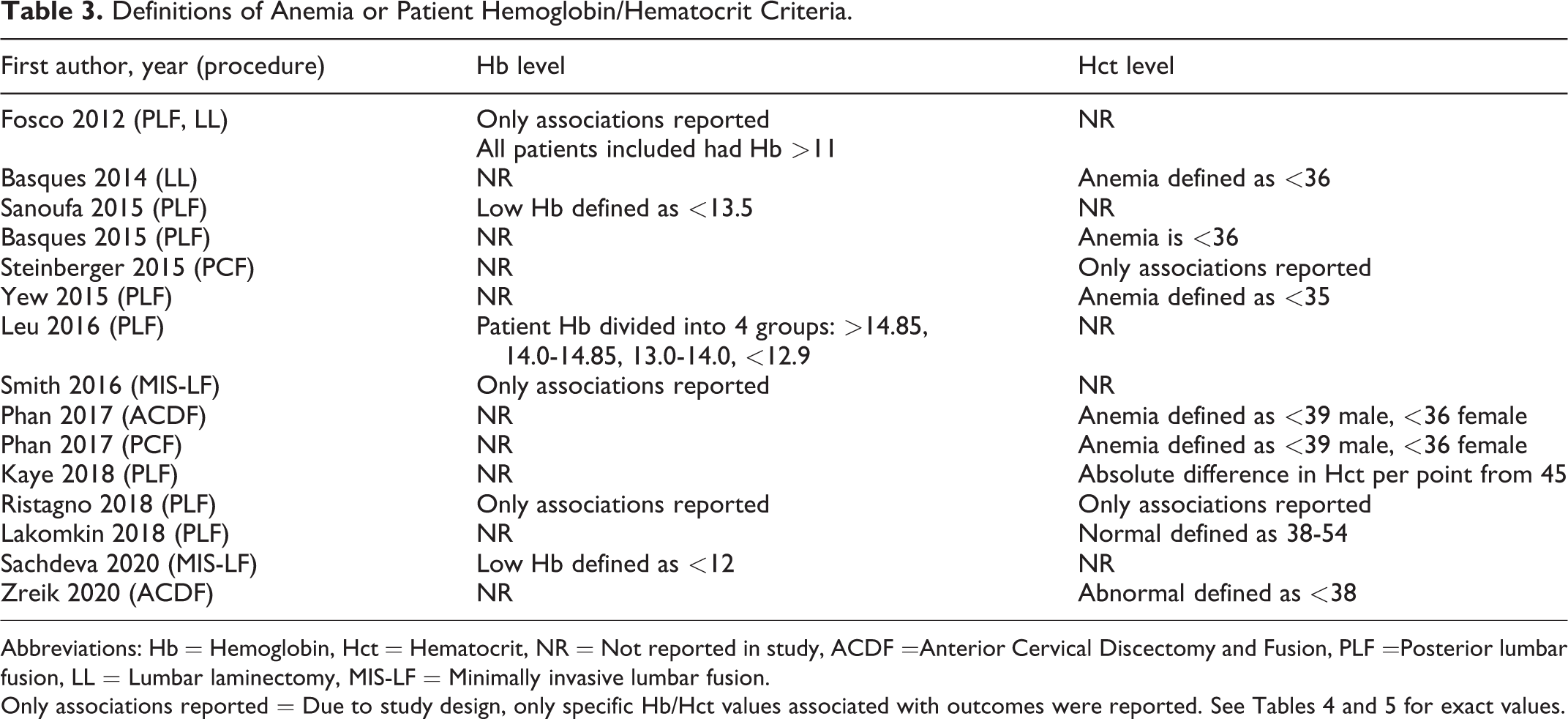
Abbreviations: Hb = Hemoglobin, Hct = Hematocrit, NR = Not reported in study, ACDF =Anterior Cervical Discectomy and Fusion, PLF =Posterior lumbar fusion, LL = Lumbar laminectomy, MIS-LF = Minimally invasive lumbar fusion.
ACDF
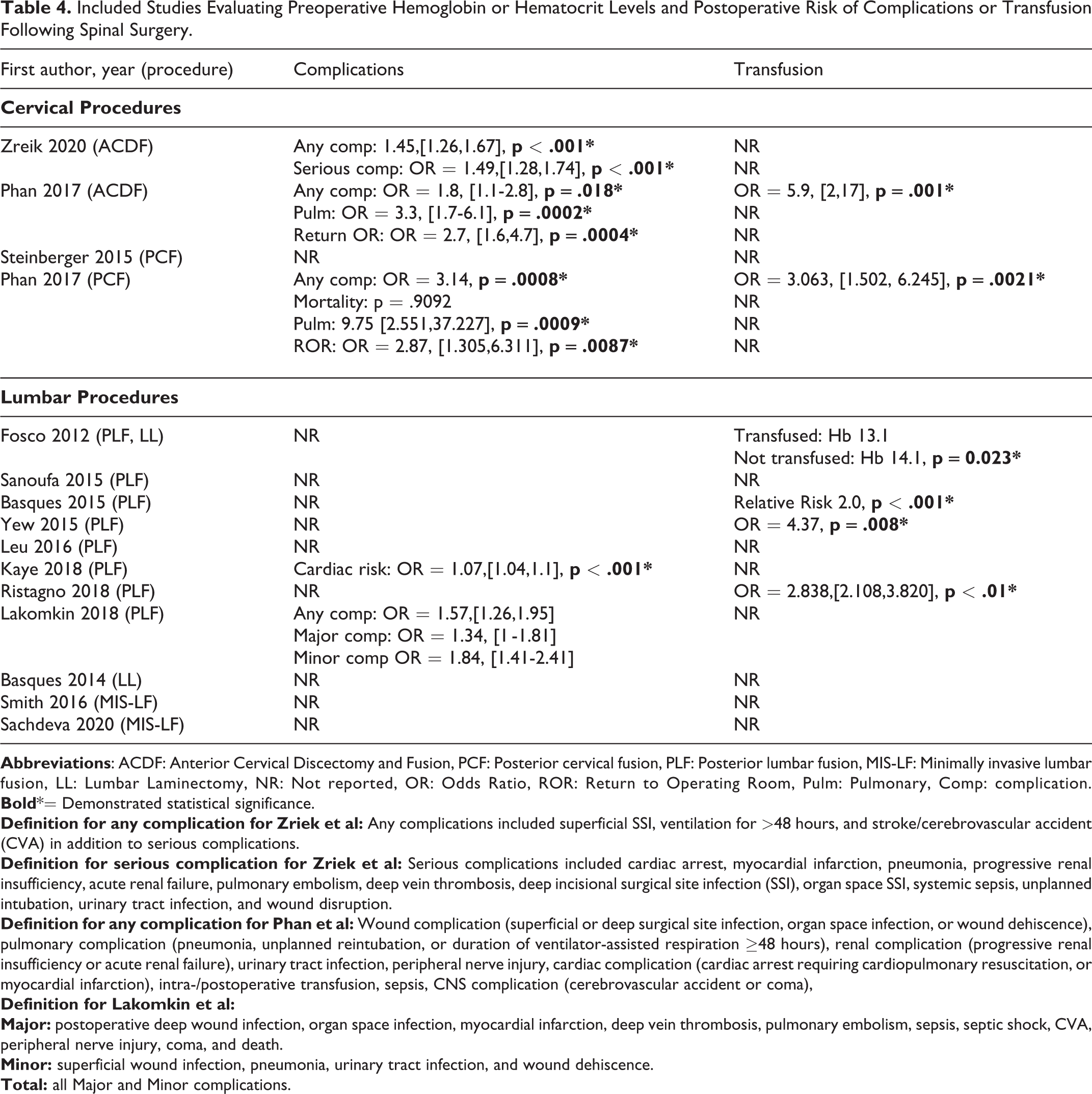
Two studies reported on association of preoperative Hct and adverse outcomes in multi-level ACDF procedures.4,13 Low preoperative Hct was associated with significantly increased risk of any complication
Included Studies Evaluating Preoperative Hemoglobin or Hematocrit Levels and Postoperative Risk of Complications or Transfusion Following Spinal Surgery.
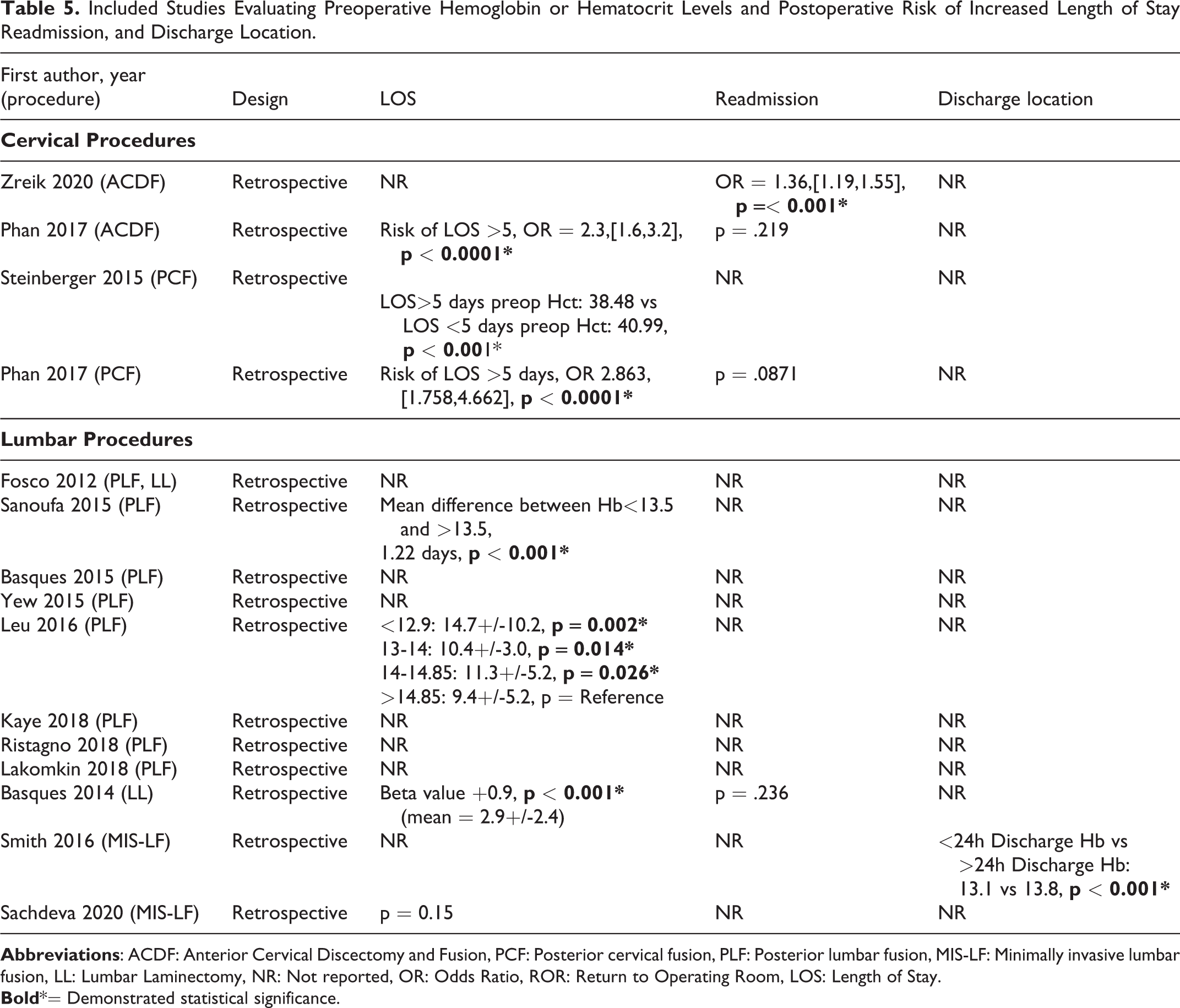
Included Studies Evaluating Preoperative Hemoglobin or Hematocrit Levels and Postoperative Risk of Increased Length of Stay Readmission, and Discharge Location.
PCF
Two studies reported on the association of preoperative anemia and postoperative outcomes following multi-level PCF.6,14 Steinberger et al reported that patients with increased LOS>5 days were more likely to have lower preoperative Hct (Hct: 38.48 vs 40.99,
PLF
Eight studies demonstrated the association of preoperative anemia with postoperative outcomes following PLF.15-22 Four studies reported that low preoperative Hb/Hct was associated with increased risk of blood transfusion postoperatively(
Table 4
).15,17,18,20 Two studies reported that low preoperative Hb was associated with increased LOS (
Table 5
).16,22 In single level PLF, increasing absolute difference in Hct from 45 was associated with significantly increased risk of adverse cardiac events (OR 1.07,
LD
Two studies reported on the association of preoperative Hb/Hct and postoperative outcomes following lumbar laminectomy.15,25 Fosco and Di Fiore found that patients who received postoperative blood transfusion had significantly decreased preoperative (Hb: 13.1 vs 14.1, p = 0.023,
Table 4
). Basques et al reported that low preoperative Hct was associated with increased LOS (Beta value, +0.9,
Utility of Preoperative HbA1c in Spinal Surgery
The cut-off value for an elevated HbA1c was slightly different for each study and can be found in Table 6 .
Clinical Definition of Elevated HbA1c.
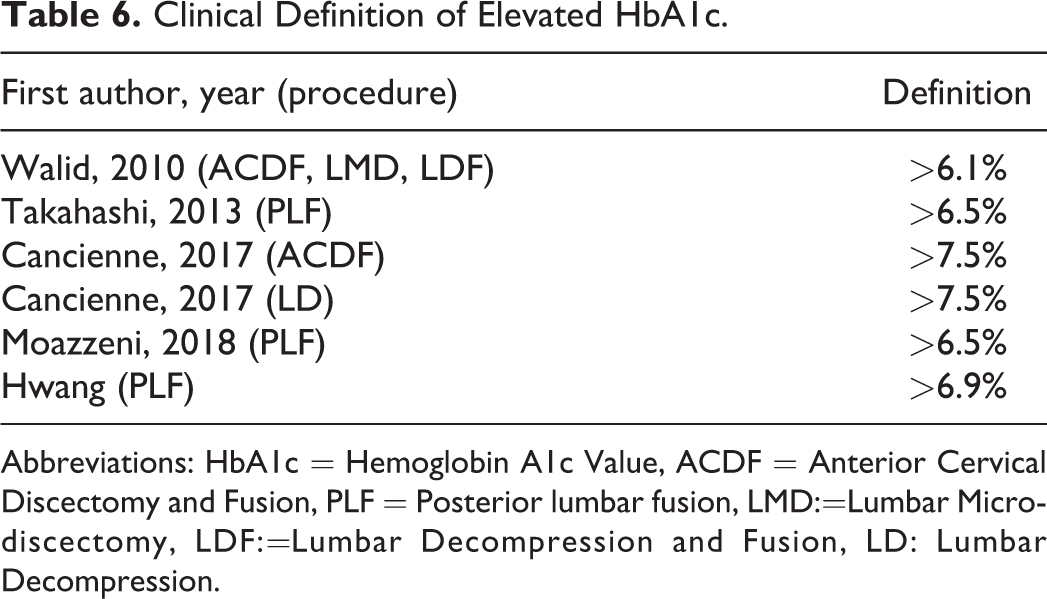
Abbreviations: HbA1c = Hemoglobin A1c Value, ACDF = Anterior Cervical Discectomy and Fusion, PLF = Posterior lumbar fusion, LMD:=Lumbar Microdiscectomy, LDF:=Lumbar Decompression and Fusion, LD: Lumbar Decompression.
ACDF
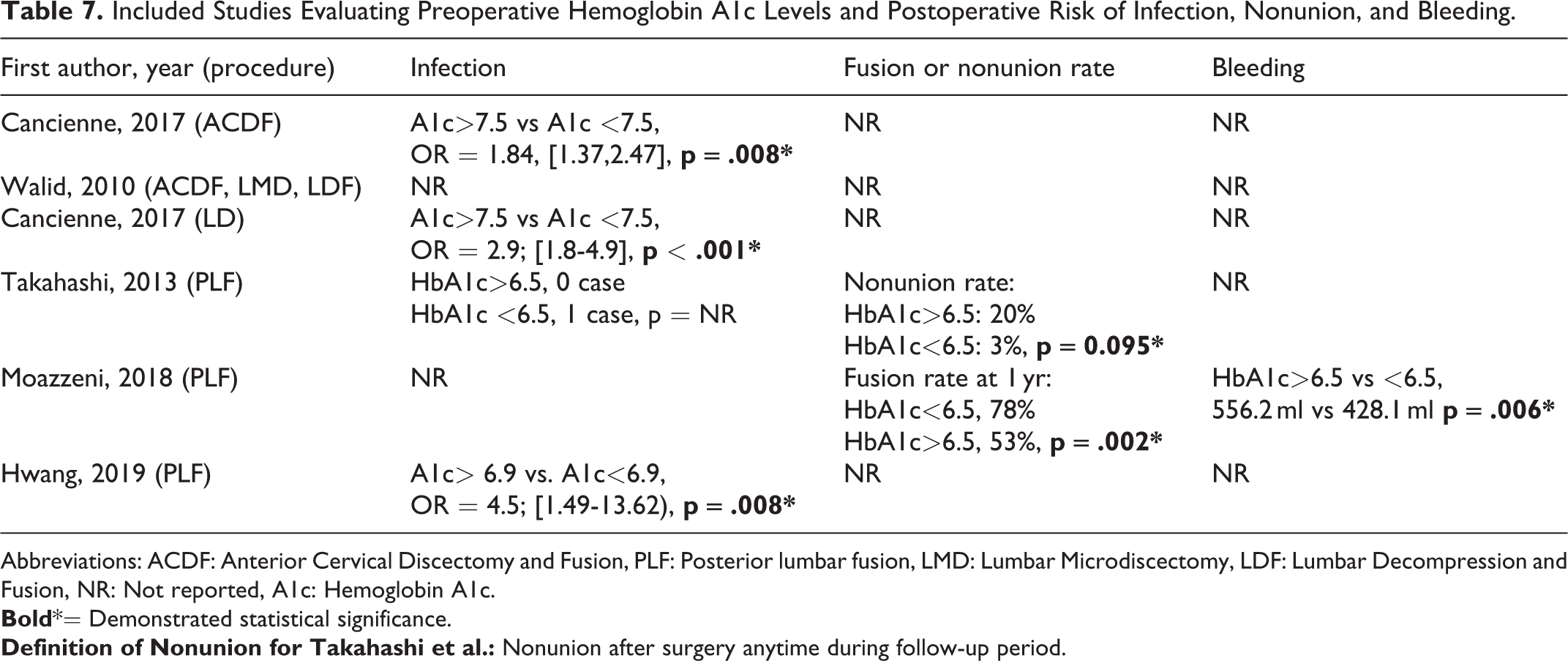
Two studies demonstrated the association of preoperative HbA1c and postoperative outcomes following ACDF.26,27 Cancienne et al reported that elevated HbA1c was associated with increased risk of postoperative surgical site infection (OR 1.84, p = 0.008, Table 7 ). Walid et al demonstrated that patients with an elevated HbA1c and history of DM had significantly increased total hospital cost compared to those without elevation ($36 748 vs $28 363, p < 0.05, Table 8 ).
Included Studies Evaluating Preoperative Hemoglobin A1c Levels and Postoperative Risk of Infection, Nonunion, and Bleeding.
Abbreviations: ACDF: Anterior Cervical Discectomy and Fusion, PLF: Posterior lumbar fusion, LMD: Lumbar Microdiscectomy, LDF: Lumbar Decompression and Fusion, NR: Not reported, A1c: Hemoglobin A1c.
Included Studies Evaluating Preoperative Hemoglobin A1c Levels and Postoperative Functional Outcomes, Length of Stay, and Cost.
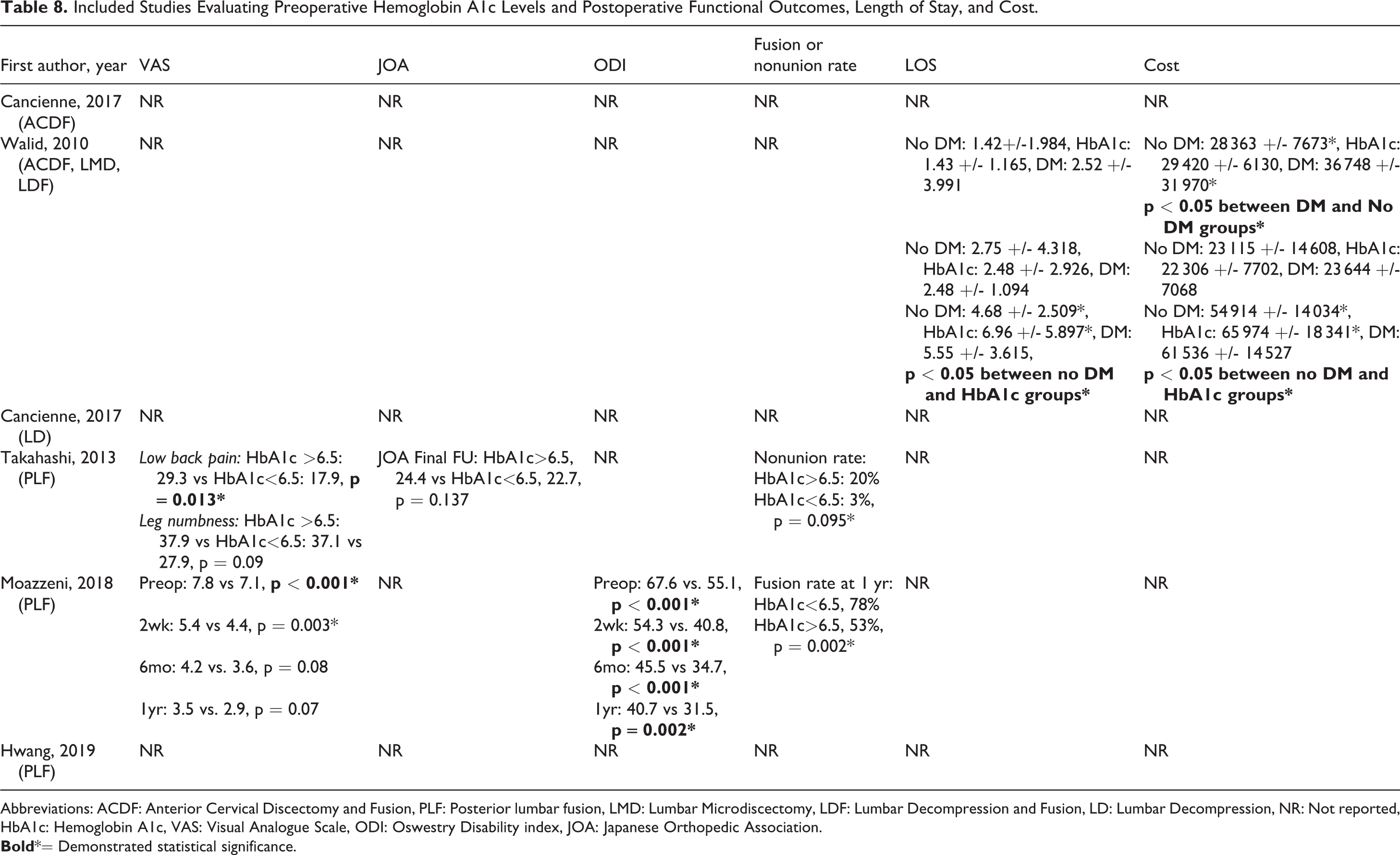
Abbreviations: ACDF: Anterior Cervical Discectomy and Fusion, PLF: Posterior lumbar fusion, LMD: Lumbar Microdiscectomy, LDF: Lumbar Decompression and Fusion, LD: Lumbar Decompression, NR: Not reported, HbA1c: Hemoglobin A1c, VAS: Visual Analogue Scale, ODI: Oswestry Disability index, JOA: Japanese Orthopedic Association.
PCF
None of the studies explored the association between preoperative HbA1c and postoperative outcomes following PCF.
PLF
Four studies reported on the association between elevated HbA1c and adverse postoperative outcomes following PLF.27-30 Takashi et al reported that elevated HbA1c was associated with increased VAS scores for low back pain at final follow-up (29.3 vs 17.9, p < 0.013, Table 8 ). Moazzeni et al reported that VAS scores were significantly different between patients with elevated vs. normal HbA1c for the first 2 weeks postoperatively (5.4 vs 4.4, p = 0.003, Table 8 ) but reported that VAS scores were no longer significant after 6 months (4.2 vs 3.6, p = 0.08, Table 8 ). Elevated ODI scores were demonstrated up to one year postoperatively in patients with elevated HbA1c ( Table 8) . In addition, Walid et al reported an increased LOS (5.55 days vs 4.68 days, p < 0.05) and total cost (61 536 vs 54 914, p < 0.05) in patients with elevated HbA1c ( Table 8 ). Moreover, Takahashi et al reported that patients with an elevated HbA1c has a higher rate of non-unions ( Table 7 ). Similarly, Moazzeni et al reported a decreased fusion rate (53% vs 78%, p = 0.002) and increased postoperative bleeding (556.2 ml vs 428.1 ml, p = 0.006) in patients with elevated HbA1c ( Table 7 ).
LD
Two studies reported on the association between elevated HbA1c and adverse postoperative outcomes following lumbar microdiscectomy or lumbar decompression alone.27,31 Cancienne et al reported that elevated preoperative HbA1c was associated with a significant increase in surgical site infection following single level LD (OR 2.9,
Risk of Bias and Quality of Evidence
Risk of bias was found to be not serious within all included studies. Quality of evidence was determined for all observational studies using the GRADE system. Across 19 included studies, there was low quality of evidence evaluating associations between preoperative Hemoglobin and HbA1c and postoperative outcomes demonstrates that lower preoperative hemoglobin and higher HbA1c values may have some utility in predicting adverse postoperative outcomes. The inconsistency portion of the GRADE system was unable to be evaluated for 2 studies, as primary outcomes in these articles were not evaluated in other included studies. As such, these studies were given a level lower in overall quality (
Discussion
We conducted a systematic review of the literature to determine the clinical utility of obtaining preoperative Hb/Hct and HbA1c in adult patients undergoing cervical and lumbar spinal surgeries. Specific procedures assessed included ACDF, PCF, PLF, and LD. Low preoperative Hb/Hct was found to be significantly associated with elevated risk for any postoperative complication and risk of postoperative transfusion, specifically for ACDF, PCF, and PLF. Decreased preoperative Hb/Hct was significantly associated with increased LOS for all procedures, except for MIS-LF. Preoperative HbA1c was reported to be predictive of postoperative infection following ACDF, LD, and PLF, and was found to be predictive of increased LOS and healthcare cost for PLFs.
Spinal operations carry varying risks of intraoperative and postoperative morbidity and appropriate perioperative planning requires preoperative risk stratification,32,33 and optimization of cardiovascular and pulmonary issues, and nutrition prior to surgery. 33 Risk factor evaluation commonly consists of screening labs, which include preoperative Hb/Hct. There is also some evidence supporting obtaining HbA1c in all patients, as prevalence of undiagnosed diabetes is fairly high with reported rates as high as 40.9%. 34
Our review indicates that regardless of exact Hb/Hct values utilized by studies, lower preoperative values are associated with adverse outcomes. Literature suggests that a Hct threshold of <35-38% may portend higher risk with spinal surgery. In our review, various thresholds for low preoperative Hb/Hct were reported ( Table 3 ). Hb cutoff values ranged from 11-13.5 g/dL, with studies reporting overall worse outcomes in patients with values below the reported threshold. Studies included in our review demonstrate that the use of Hb/Hct as a continuous variable is also valuable for postoperative risk assessment.19,22
For HbA1c, a threshold of 6.5-6.9% was associated with increased risk of complications in patients undergoing spine surgery. All 6 studies assessing preoperative HbA1c utilized threshold values ranging from 6.1 to 7.5%. Of these, 4 studies reported extensive postoperative follow-up of over 1 year; 3 of these studies utilized HbA1c threshold ranging from 6.5-6.9%, and indicated that elevated values above threshold were associated with poor long-term functional outcomes, increased nonunion rate, decreased fusion rate, and increased infection rate following PLF.28-30 The remaining study with 1 year follow-up reached similar conclusions but utilized a higher HbA1c threshold (7.5%). 31 Considering that HbA1c thresholds <7.5% still resulted in adverse postoperative outcomes, using lower values to gauge postoperative risk may be more recommended.
Because of strict inclusion and exclusion criteria to conduct the systematic review, we ended up excluding studies that did not directly examine the associations between postoperative outcomes after spinal surgery and preoperative Hb/Hct or HbA1c. A retrospective study performed by Perez et al was excluded because the authors only reported complications associated with decreased postoperative Hb. 35 Similarly, we excluded a retrospective study performed by Cai et al, in which the authors reported that decreased preoperative Hb was a significant predictor of reduced postoperative Hct; the authors did not investigate associations with decreased preoperative Hb/Hct. 36 For HbA1c, we excluded a retrospective study of over four-hundred thousand patients undergoing lumbar fusion as the authors identified diabetics patients using ICD-9 CM codes without examining actual preoperative HbA1c level. 37
The findings of our systematic review must be interpreted within its limitations. First, the heterogeneity of preoperative Hb/Hct and HbA1c thresholds, strict inclusion and exclusion criteria, and the possibility of missing studies may limit our review. Second, the absence of randomized controlled trials and variation in outcomes reported prevented us from performing a meta-analysis. Our review primarily consisted of only level III retrospective studies and one level II prospective study, perhaps because designing randomized controlled studies to evaluate association of preoperative hemoglobin or HbA1c on postoperative outcomes may be unfeasible. However, the lack of level I studies in our review limits our ability to make robust conclusions and provide more granular recommendations regarding preoperative management.
Conclusion
For ACDF, PCF, PLF, and LD procedures, preoperative Hb/Hct are clinically useful predictors for adverse postoperative outcomes, including complications, postoperative transfusion, and increased LOS. Based on this review, Hct values <35-38% and HbA1c>6.5-6.9% may be important thresholds for identifying patients who are higher risk of complications after undergoing spinal surgeries.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_2192568220979821 - Spine Surgery and Preoperative Hemoglobin, Hematocrit, and Hemoglobin A1c: A Systematic Review
Supplemental Material, sj-docx-1-gsj-10.1177_2192568220979821 for Spine Surgery and Preoperative Hemoglobin, Hematocrit, and Hemoglobin A1c: A Systematic Review by Krishna V. Suresh, Kevin Wang, Ishaan Sethi, Bo Zhang, Adam Margalit, Varun Puvanesarajah and Amit Jain in Global Spine Journal
Supplemental Material
Supplemental Material, sj-docx-2-gsj-10.1177_2192568220979821 - Spine Surgery and Preoperative Hemoglobin, Hematocrit, and Hemoglobin A1c: A Systematic Review
Supplemental Material, sj-docx-2-gsj-10.1177_2192568220979821 for Spine Surgery and Preoperative Hemoglobin, Hematocrit, and Hemoglobin A1c: A Systematic Review by Krishna V. Suresh, Kevin Wang, Ishaan Sethi, Bo Zhang, Adam Margalit, Varun Puvanesarajah and Amit Jain in Global Spine Journal
Supplemental Material
Supplemental Material, sj-docx-3-gsj-10.1177_2192568220979821 - Spine Surgery and Preoperative Hemoglobin, Hematocrit, and Hemoglobin A1c: A Systematic Review
Supplemental Material, sj-docx-3-gsj-10.1177_2192568220979821 for Spine Surgery and Preoperative Hemoglobin, Hematocrit, and Hemoglobin A1c: A Systematic Review by Krishna V. Suresh, Kevin Wang, Ishaan Sethi, Bo Zhang, Adam Margalit, Varun Puvanesarajah and Amit Jain in Global Spine Journal
Footnotes
Acknowledgements
We thank Carrie L. Price, MLS, clinical informationist at the Johns Hopkins Welch Medical Library for her assistance in developing our search strategy.
Authors’ Note
This study used publicly available information and was not subject to evaluation by our Institutional Review Board.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or she has no commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.