
Abstract
Study Design:
The following is a narrative discussion of bundled payments in spine surgery.
Objective:
The cost of healthcare in the United States has continued to increase. To lower the cost of healthcare, reimbursement models are being investigated as potential cost saving interventions by driving incentives and quality improvement in fields such a spine surgery.
Methods:
Narrative overview of literature pertaining to bundled payments in spine surgery synthesizing findings from computerized databases and authoritative texts.
Results:
Spine surgery is challenging to define payment modes because of high cost variability and surgical decision-making nuances. While implementing bundled care payments in spine surgery, it is important to understand concepts such as value-based purchasing, episodes of care, prospective versus retrospective payment models, one versus two-sided risk, risk adjustment, and outlier protection. Strategies for implementation underscore the importance of risk stratification and modeling, adoption of evidence based clinical pathways, and data collection and dissemination. While bundled care models have been successfully implemented, challenges facing institutions adopting bundled care payment models include financial stressors during adoption of the model, distribution of risks, incentivization of treating only low risk patients, and nuanced variation in procedures leading to variation in costs.
Conclusion:
An alternative for fee for service payments, bundled care payments may lead to higher cost savings and surgeon accountability in a patient’s care.
Introduction
The cost of healthcare in the United State as measured by the percentage of the Gross Domestic Product spent has consistently grown since the early 1960’s. 1,2 Recently observed contributing factors of this growth include aging populations and work forces, advances in medical technology, income growth, and increases in population coverage. 3 As a result, pressure is mounting to reform the system to deliver better care for a lower cost. The fee for service model of payment, which was the traditional payment model, rewarded doctors on a volume of work basis. While volume-based payments were once the standard for healthcare in the United States, there is growing concern surrounding the sustainability of growing healthcare costs. Furthermore, there is little evidence that the high cost of healthcare in the US delivers high value compared to other modern industrial countries. 4,5 Bundled payment models shift payment from volume to value in an effort to slow costs and improve quality of care. In general, bundled payment models have shown success during implementation in countries such as the United States, Taiwan, Denmark, England, Netherlands, New Zealand, Portugal, and Sweden. Of 32 studies evaluating medical spending in bundled payments, 20 showed cost-saving with varying effects. In addition, this cheaper care is largely delivered without compromising patient care as only 2 studies showed detrimental effects on quality of care. In fact, 18 of 32 studies showed an improvement in quality of care delivered. 6
Payments pertaining to a surgical procedures conceptually are easy to create bundled payment models. The characteristics that lend themselves to bundled payments are definable start dates, high volume of procedure, high costs of procedure and related care, and a definable duration of costs related to the procedure. When examining costs associated with inpatient spine procedures, it is apparent that currently there is a wide variation in payments, therefore, payment models for surgery are a potential target for improvement of cost efficiency and resource utilization. 7 As a result, bundled payments for care spine surgery episodes, rather than discrete interventions (volume based payments) have been proposed as a way to drive quality improvement and outcome based decision making. 8 Championing the potential benefits of a bundled payment system, joint arthroplasty has served as pilot procedure demonstrating the cost savings in hospitals adopting this system. 9 -11
Spine surgery is a high complexity procedure with heterogeneous patient populations and poorly defined outcome measures. 12 When examining Medicare data, costs for patients with lumbar spinal stenosis approaches that of chronic diseases such as diabetes and cardiovascular disease 13 and have seen 3.3 fold increases over a decade span. 14 As a result, the specialty has also felt the pressure to deliver higher quality care at a lower cost. 15 While the field has worked to advance quality and outcome measurements through development of large outcome databases such as N2QOD, SweSpine, and AO Spine, 16 there is still plenty of room for developments in cost efficiency. Among many other quality improvement interventions, shifting to value-based care will be an important tool for spine surgeons moving forward. We aim to provide insight into the key concepts of bundled payment models for spine surgery, implementation of bundled payments, and barriers to success.
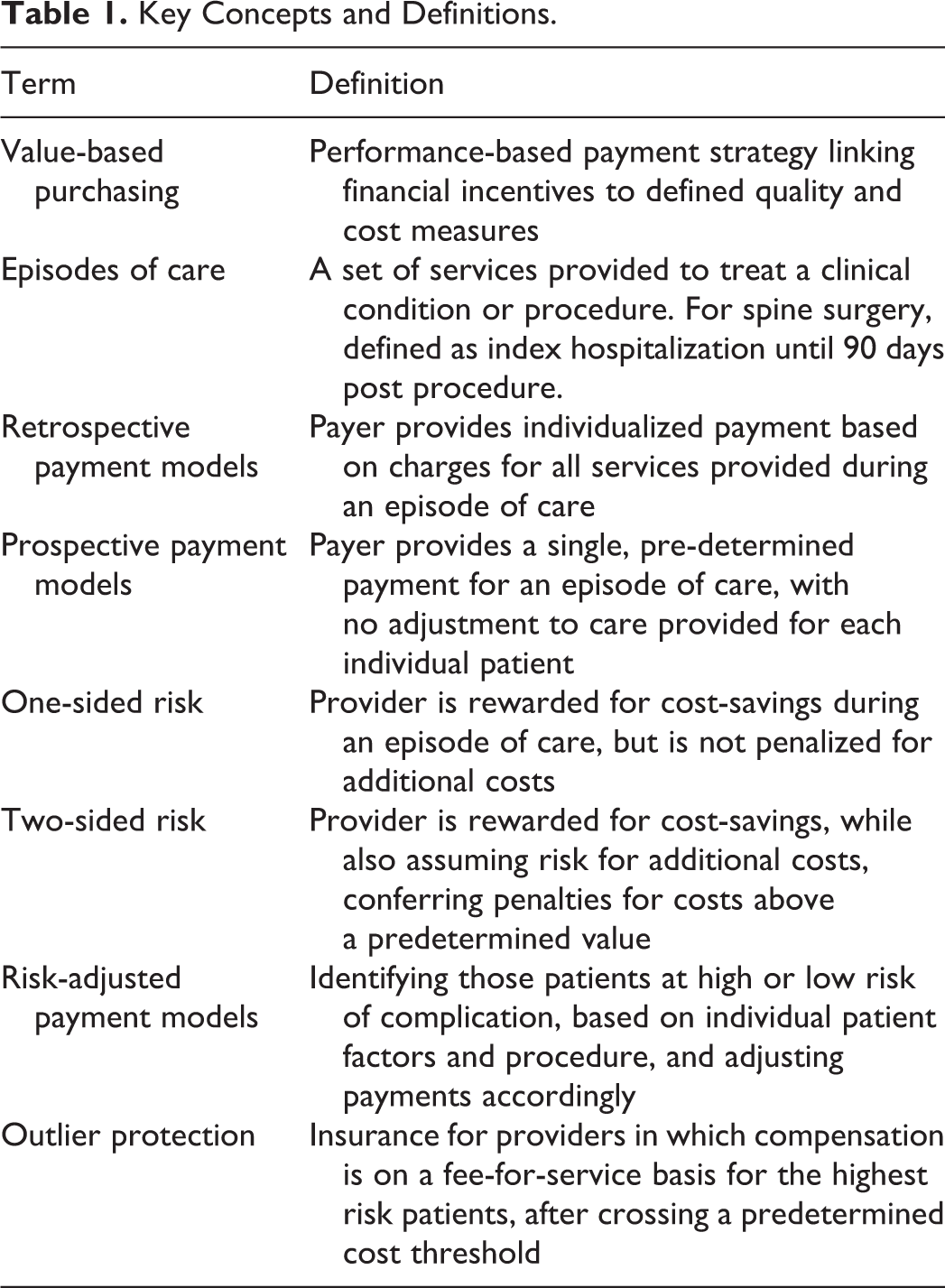
Key Concepts
One of the important drivers of a bundled payment model in spine surgery is the concept of
The measures used to assess the value and quality of care pertain to
Among bundled payment models, there are 2 main subtypes:
In addition to the different types of repayment, there are also different types of risk models associated with bundled payment contracts. In
Finally, as mentioned earlier spine surgery has extremely variable costs associated with a single episode of care. This variability allows the provider to assume a large proportion of risk. As a result, individualized
Another risk shifted to providers in bundled payments are
Key Concepts and Definitions.
Strategies for Implementation
While the push for bundled healthcare services started in 2011 with the Bundled Payments for Healthcare Initiative (BPCI), 23 spinal surgery has only recently aggressively started incorporating these payment methods into the practice. While it is not standard practice yet, preliminary research has noted increasing use of bundled payments in spine with promising results. 24 A survey of 43 spine surgeons showed that bundled care implementation would alter decision making such as more conservative use of allograft rather than autograft, routine neuromonitoring, and rigid post-operative bracing. 25 As payment models shift toward bundled payments, it is important to explore strategies that will promote a smooth transition as well as cost efficiency and outcome-based care.
Given spinal surgery’s wider variability in costs, procedural nuances, and outcome measures, it is important to lesson from other implementations of bundled spinal surgery to aid in this transition. Without understanding successful model integration BPCI may not lead to decreased episode costs, readmission rates, or reoperation rates. 26 Other systems have emphasized several principles: risk stratification and modeling, adoption of evidence based clinical pathways, and data collection and dissemination. 27
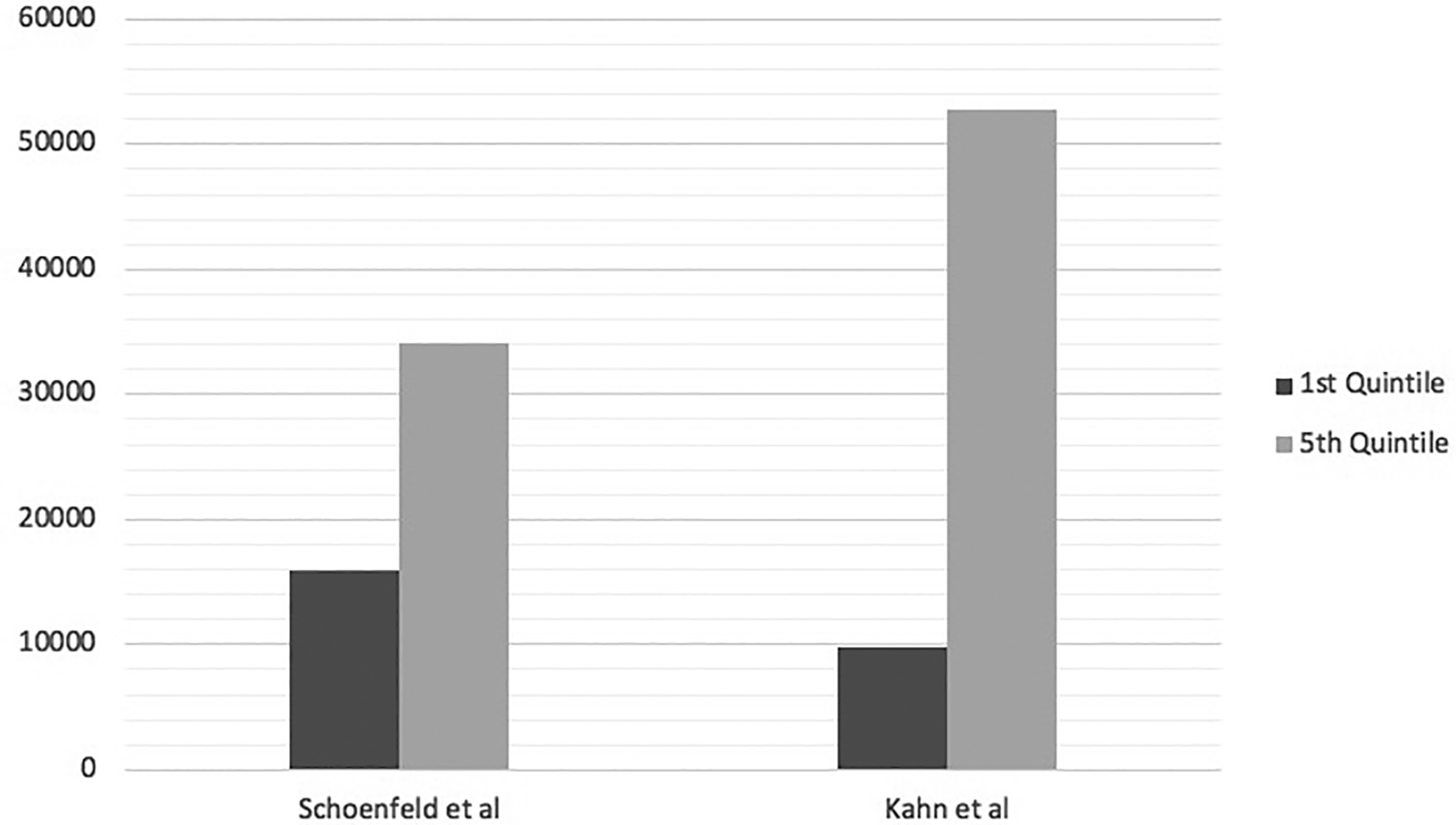
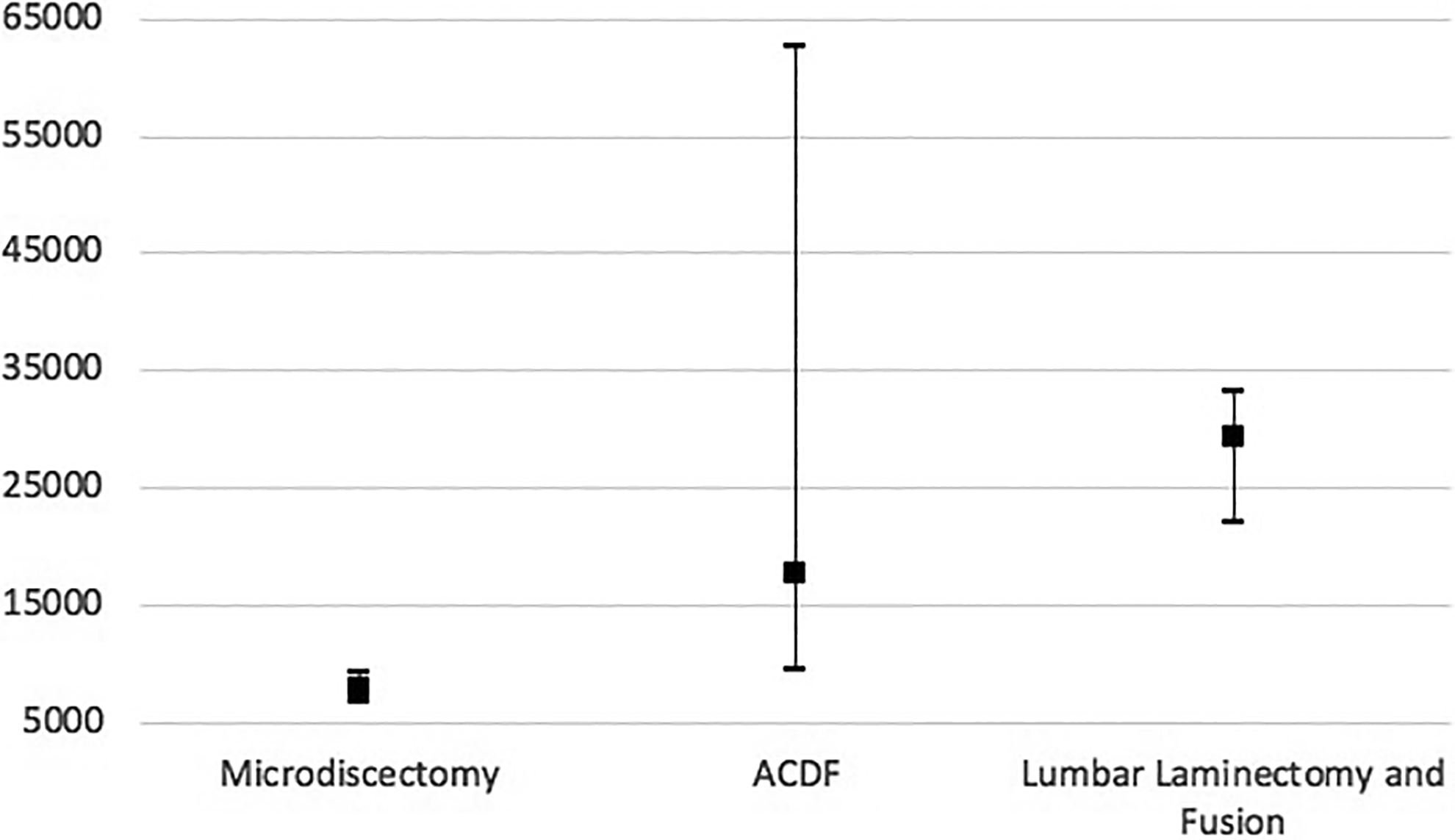
As discussed before, spinal patients demonstrate extreme variations in episode of care cost. Characterizing these patients through diagnosis related groups (DRG) alone is difficult as spinal fusions address varying pathologies with individualized post-operative courses. Within a single DRG, many different combinations of instrumentation, operative levels, grafts, and post operative care may be utilized leading to variations in payments from $80,000 to $253,000. 28 Alternatively, if hospitals were to reimburse at the same rate for episodes of care related to the procedure spinal fusion, patients requiring fusion for spondylolisthesis have been noted to have lower LOS, lower hospital costs, less chance of being discharged to an inpatient facility than vertebral fractures despite being reimbursed equal amounts for the encounter. 29 In addition to properly modeling diagnosis related groups and stratifying the different treatments, it is important to model what individual patient characteristics will contribute to the cost of an episode of care. For instance, recent research has explored drivers of 90-day cost variability in lumbar microdiscectomy, anterior cervical discectomy and fusion for degenerative disease, adult thoracolumbar spine deformity surgery, and elective lumbar decompression and fusion. Factors consistently associated with variations in episode costs included obesity, length of surgery, number of levels or extent of surgery, surgical complications, readmission, medical comorbidities such as MI or diabetes, and post-hospitalization care. 30 -33 Figure 2 demonstrates this variability in cost for episodes of care in different procedures. Notably, Bronson et al published their Medicare claims data associated with lumbar fusion after adoption of the BCPI program. They failed to show cost savings using the model. However, the authors note that both case complexity and longer segment fusions had increased in the BCPI group, confounding the comparison with the historical control. 34 Despite not demonstrating savings, the BCPI group did have significantly lower LOS and discharge to inpatient facilities without increased readmission rates. In addition to patient factors, surgeon factors may also affect cost variation such as choice of implant. In a recent study, by Oren et al, standardizing implant cost by requiring vendors to meet reference prices, significant cost savings were demonstrated in patients undergoing single level anterior cervical discectomy and fusion. 35 Understanding the factors driving variability in spine surgery will be a key in implementing a successful bundle payment system.
Aside from understanding drivers of cost variability and incorporating them into payment models, it is important to establish evidence based clinical pathways (EBCP) or bundled care plan. EBCP include care built in after analysis of high quality, large population data that may be applied to episodes of care in the hopes of decreasing complications, reducing cost variability, and improving outcomes. Examples of such pathways include measures against venous thromboembolism (VTE), 36 surgical site infection (SSI), 37,38 and transfusion management. 39 EBCP tend improve outcomes and cost efficiency in patients by reducing modifiable risk factors. The evidence that standardization works to reduce variation in costs and outcomes was adopted from manufacturing concepts popularized by Shewhart and Deming, 40,41 but have been have been successful in other surgical EBCP such as knee arthroplasty. 42 -44 To implement bundled payment systems, EBCP are essential to reducing cost variability and generating data for smaller, less experienced institutions to use in the care of spinal surgery patients.
Lastly, to successfully implement a bundled payment spine surgery model, development of infrastructure to collect institutional or system specific data is imperative. While large databases are crucial in developing data driven spine practices that are applicable to specific spinal surgery populations, 16 institutional or network specific database collection and distribution are paramount to ensuring success in a bundled payment model for spine surgery. This is because after each episode of care, the stakeholders involved in the care of a patient may compare the costs accumulated to the projected cost or contract of the episode. As this data accumulates, spinal surgeons will have the opportunity to review their cost efficiency, complications, and compare complications such as VTE, SSI, or reoperation to particular episode of care’s projections. As seen in other surgical fields such as orthopedics, this educates surgeons on cost and benefit of certain measures with regard to their individualized practices. 45
As institutional data on risk stratification, modifiable risk factors, and ECBP accumulates in spinal surgery, surgeons will be able to identify individual practices that do no mitigate risk nor add patient benefit while still generating cost. These practices are non-value-added care and should be identified so they may be avoided or reduced. This will improve implementation of bundled payment model in spinal surgery.
Challenges
While bundled repayment models have upside in provider accountability, cost efficiency, and standardization of care there are large hurdles for implementation of this system in spinal surgery.
Generally considered a costly intervention, bundled repayment models may strain healthcare systems financially while the process of repayment is optimized and better defined. In a prospective payment model, a single entity receives the payment and must delay payment to all stakeholders until the cost of the episode of care has been determined. Alternatively, providers in a retrospective model will not obtain full payment for services until the episode is completed and final associated cost is determined.
Given that these systems couple large financial risk with surgeons and add delayed reimbursement to the uncertainty may make delivering consistent care difficult. Outcome metrics are not well defined and metrics in chronic back pain patients such as patient satisfaction may play an unfair role in determining the quality of a surgeon’s work. In addition to timing and quality assessment, ensuring accuracy of insurance billing will be a large concern in spinal surgery. For a surgical specialty with nuances altering indication, surgical approach, number of levels, and outcome, it will require provider vigilance and resources to ensure that payments applied to episodes of care account for individualized risk and post-operative course.
In addition to payment allocation, a large concern with transitioning to bundle payment models includes modifying spine surgeons’ incentives. In some models, researchers found that variability in cost was associated with post-acute care factors rather than surgeon controlled variables. 19 Such associations may motivate surgeons to select patients by pathology or anticipated disposition rather than evidence-based indication. Until payment models are optimized, there is concern that these models will financially compel surgeons to preferentially operate on low risk, healthier patients and avoid pathology associated with higher costs of episodes of care. 29 In addition, advanced techniques with only marginal improvement in outcomes may be avoided given associations with increased cost or length or surgery, 46 this may lower costs in the near term but could stifle innovation.
Bundle payment models in spinal surgery offer an alternative to fee-for service payments and may have potential benefits for healthcare in the United States. Bundled care makes spinal surgeons accountable for not only outcome, but also episode cost efficiency and limitation of complications. While this approach is not novel, it has not been fully implemented yet in the United States. Despite success in arthroplasty, spinal surgery has yet to demonstrate clear benefit of bundled payments in spine surgery the United States. Of 3 studies evaluating costs savings for episodes of care associated with spinal surgery, none demonstrated cost reduction. 26,34,47 In addition, it is important to note that it is difficult to evaluate the effect lowering perioperative cost on the context of overall health care spending. To optimize this payment method, stringent risk stratification, development of evidence-based pathways, and dissemination of detailed outcome-based data must be implemented. In addition, hospital systems must evaluate risk allocation as repayment models are defined to avoid financially incentivizing spinal surgeons to select for only healthy patient with low risk pathology. While bundled care payment models have not been clearly successfully implemented in spine surgery in the United States, they warrant further investigation given the success in cost reduction of bundled payments in other specialties and countries.
Footnotes
Authors’ Note
The authors conducted a literature review with the goal of writing a narrative review of bundled payment models in spine surgery. The objectives were to provide readers with key definitions to understand bundled payment models, outline strategies for success implementing such a payment model, and defining challenges to implementing such a system in spine surgery. Using PubMed, a literature review of articles pertaining to episodes of care, bundled payments, and drivers of cost variability in spine surgery were reviewed. In review of the literature, bundled payment models offer potential cost savings and quality improvement incentives in spine surgery. However, successfully implementing these models will be challenging given the variability and nuance inherent in spine diagnosis, pathology, and surgical techniques.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by a grant from AO Spine North America.