
Abstract
Study Design:
Retrospective cohort study.
Objectives:
The purpose of this study was to report incidence of cardiopulmonary complications in elective spine surgery, demographic and surgical predictors, and outcomes. Understanding the risks and predictors of these sentinel events is important for risk evaluation, allocation of hospital resources, and counseling patients.
Methods:
A retrospective review of the National Surgical Quality Improvement Program (NSQIP) was performed on 60 964 patients undergoing elective spine surgery (any region; laminectomy, arthrodesis, discectomy, or laminoplasty) between 2011 and 2013. Incidence of myocardial infarction, cardiac arrest, unplanned reintubation, on ventilator >48 hours, perioperative pneumonia, and pulmonary embolism was measured. Demographic and surgical predictors of cardiopulmonary complications and associated outcomes (length of stay, discharge disposition, and mortality) were measured using binary logistic regression controlling for confounders.
Results:
Incidence rates per 1000 elective spine patients were 2.1 myocardial infarctions, 1.3 cardiac arrests, 4.3 unplanned intubations, 3.5 on ventilator >48 hours, 6.1 perioperative pneumonia, and 3.7 pulmonary embolisms. In analysis of procedure, diagnosis, and approach risk factors, thoracic cavity (odds ratio = 2.47; confidence interval = 1.95-3.12), scoliosis diagnosis, and combined approach (odds ratio = 1.51; confidence interval = 1.15-1.96) independently added the most risk for cardiopulmonary complication. Cardiac arrest had the highest mortality rate (34.57%). Being on ventilator greater than 48 hours resulted in the greatest increase to length of stay (17.58 days).
Conclusions:
Expected risk factors seen in the Revised Cardiac Risk Index were applicable in the context of spine surgery. Surgical planning should take into account patients who are at higher risk for cardiopulmonary complications and the implications they have on patient outcome.
Keywords
Introduction
The United States is seeing an increasing utilization of complex surgical procedures on the spine, which leads to an increased risk of life-threatening complications and readmissions. 1,2 Spine surgeries are typically longer than other elective surgeries and are associated with major blood loss, fluid shifts, and transfusions, all of which are factors that can induce or exacerbate hemodynamic stress in a patient. 3 Cardiopulmonary complications are among the most common after spine surgery and are known to increase the risk of mortality as well as generate long-term complications related to multiple mechanical failures of cardiac function. 4 –6 Respiratory complications can arise from the proximity of the respiratory system to the thoracic spine, and many spine surgeries even violate the thoracic cavity to perform surgery. 7 Furthermore, there is currently no clear indication to immediately begin anticoagulation in patients postoperatively. 8 These complications can detract significantly from postoperative quality of life.
Risk factors for cardiopulmonary complications, as established by the Revised Cardiac Risk Index (RCRI), include both intraperitoneal approach and intrathoracic approach, which are frequently indicated in spinal procedures. 9 Despite presumed additional risk factors for major morbidity, which include age, surgical invasiveness, and comorbidities, many of these links remain unvalidated in the context of spine. For example, Carabini et al in 2014 investigated the application of the RCRI to spinal fusion patients and were unable to determine the predictive value of the index in the context of spine surgeries. 3
Previous large database studies have evaluated the demographic and comorbid risk factors for complications following spine surgery, but none have focused specifically on cardiopulmonary risks and related mortality. For this reason, the authors queried the National Surgical Quality Improvement Program (NSQIP) database with the goal of elucidating the incidence of cardiopulmonary complications following elective spine surgery and their associated risk factors.
Methods
The American College of Surgeons’ NSQIP was implemented in 1991 by the US Department of Veterans Affairs in order to model patient risk-adjusted outcomes for patient factors and operative procedure. Patient data is collected by a Surgical Clinical Reviewer auditing participating hospitals. It samples all patient populations undergoing general, spinal, or epidural anesthesia. Patient data collected includes primary diagnosis in the form of an ICD-9-CM code, procedures underwent by Current Procedural Terminology (CPT) coding, 70 preoperative risk factors, 11 variables on the operation, and 24 postoperative outcomes. Complications, outcomes, and any further procedures are recorded for 30 days after enrollment. More detailed information on the NSQIP design is available at https://www.facs.org/quality-programs/acs-nsqip/about. 10 Institutional review board approval is exempt from studies using de-identified NSQIP data. CPT and ICD-9-CM codes used to identify patient diagnoses and procedures undergone are available in Appendix A (available online at http://journals.sagepub.com/home/gsj).
Patient Identification
This study selected patients on NSQIP undergoing laminectomy, arthrodesis, discectomy, and/or laminectomy in any region of the spine in the years 2011 to 2013. Patients undergoing nonelective surgery, as recorded in NSQIP data sheets, were excluded from analysis.
Statistical Analysis
Patient baseline demographics and comorbidities were analyzed between patients who experienced a cardiopulmonary complication and those who did not using χ 2 tests in categorical variables and Student’s t tests in continuous variables. Cardiopulmonary complications assessed were available as part of NSQIP 30-day data collection sheets: myocardial infarction (MI), cardiac arrest, unplanned intubation, on ventilator >48 hours, perioperative pneumonia, and pulmonary embolism. Baseline demographics included sex, race, and American Society of Anesthesiologists (ASA) class. Baseline comorbidities assessed included age >80, body mass index (BMI) >30, BMI >40, diabetes, smoking status, dyspnea, chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), hypertension, chronic steroid use, >10% weight loss within the last 6 months (weight loss), any bleeding disorder (eg, vitamin K deficiency, hemophilias, thrombocytopenia, chronic anticoagulation therapy), preoperative blood transfusion within 72 hours, and any para- or hemiplegia. Binary logistic regression then analyzed comorbidities as independent risk factors for sustaining a cardiopulmonary complication by simultaneously controlling for BMI, race, sex, ASA class, and all comorbidities except for the one being calculated.
Procedure, region, and diagnosis of the surgery were stratified into clinically relevant variables and analyzed as risk factors for each respective adverse cardiopulmonary event by binary logistic regression. Regression analysis controlled for invasiveness of the surgery (as defined by Mirza et al, 11 which adds 1 point for every level fused, decompressed and instrumented), in addition to BMI, sex, race, smoking status, ASA class, bleeding disorder (eg, vitamin K deficiency, hemophilias, thrombocytopenia, chronic anticoagulation therapy), history of transient ischemic attacks, history of MI in 6 months prior to surgery, history of percutaneous coronary intervention, history of cardiac surgery (eg, valve replacement, bypass surgery, atrial or ventricular repair), history of angina in 1 month prior to surgery, history of revascularization/amputation for peripheral vascular disease, and history of CHF within 1 month prior to surgery. Procedures were analyzed according to any presence of CPT or ICD-9 codes (see Appendix A, available online at http://journals.sagepub.com/home/gsj) procedure performed anterior fusion, posterior fusion, combined approach fusion, anterior decompression, posterior decompression, and interbody. Region (cervical, thoracic, and lumbar) and diagnosis (stenosis, spondylosis, scoliosis, fracture, and cancer) were analyzed with similar technique.
Finally, discharge status in patients sustaining cardiopulmonary events was analyzed compared to controls using ANOVA t test: length of stay (LOS), discharge status (expired, home, not-home), and unplanned reoperation within 30 days.
Results
This study examined 60 964 spine surgeries (average age 55.8 years, 55.3% female) and found 1285 major cardiopulmonary complications. Incidence rates per 1000 elective spine patients were 2.1 MIs, 1.3 cardiac arrests, 4.3 unplanned intubations, 3.5 on ventilator >48 hours, 6.1 perioperative pneumonia, and 3.7 pulmonary embolisms.
Procedures Performed
A total of 28 419 patients underwent fusions (53.4%; average of 3.53 levels fused). A total of 59.4% of patients received decompression procedures as part of care, 37.0% interbody device placement, and 1.3% 3-column osteotomy. A total of 3.8% of surgeries began in the thoracic spine, 20.5% in the cervical spine, and 75.6% in the lumbar spine. Other complex procedures performed included Smith-Petersen osteotomy 1.1%, 3-column osteotomy 0.3%, iliac fixation 0.7%, and revision 3.5%.
Demographic and Comorbidity Risk
Tables 1 and 2 details incidence of any cardiopulmonary event according to demographic and comorbidity status. The strongest predictors for any cardiopulmonary complication were >10% weight loss within 6 months of surgery (odds ratio [OR] = 3.0; confidence interval [CI] = 1.7-5.2), preoperative blood transfusion (OR = 2.1; CI = 1.0-4.1), and paraplegia (OR = 2.0; CI = 1.2-3.3). Black race was also predictive of a cardiopulmonary event (P = .006), as was increasing ASA class (P < .001).
Demographics of Patients Experiencing a Cardiopulmonary Event.a
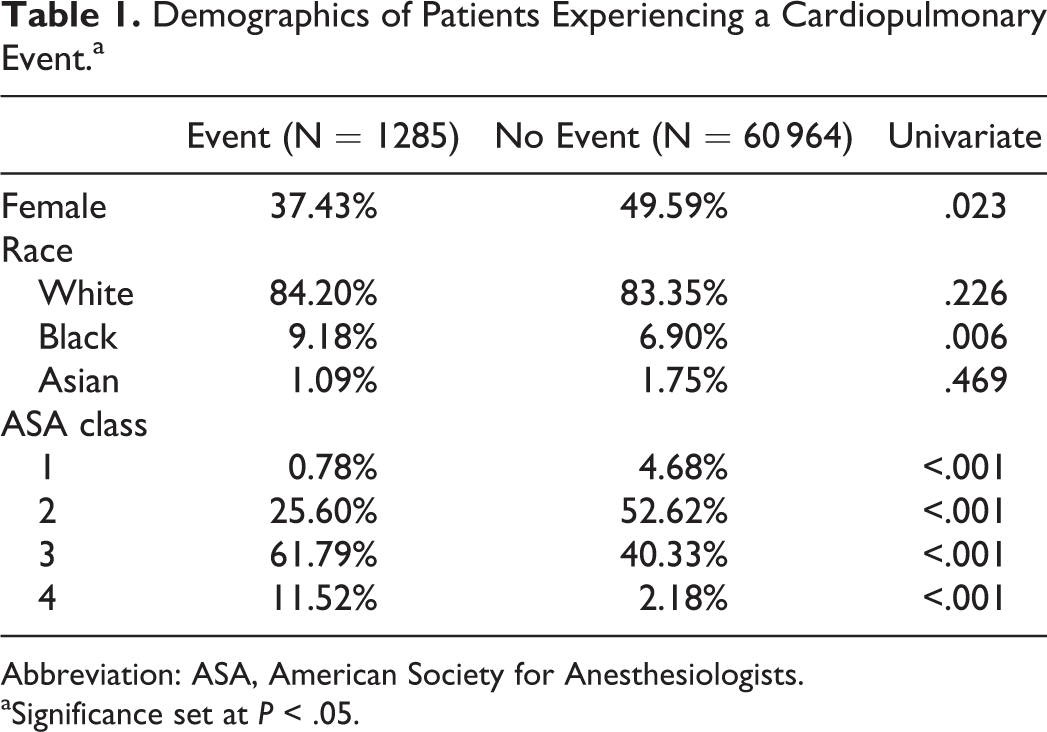
Abbreviation: ASA, American Society for Anesthesiologists.
aSignificance set at P < .05.
Demographic and Comorbidity Status as Predictors of Cardiopulmonary Complications.a
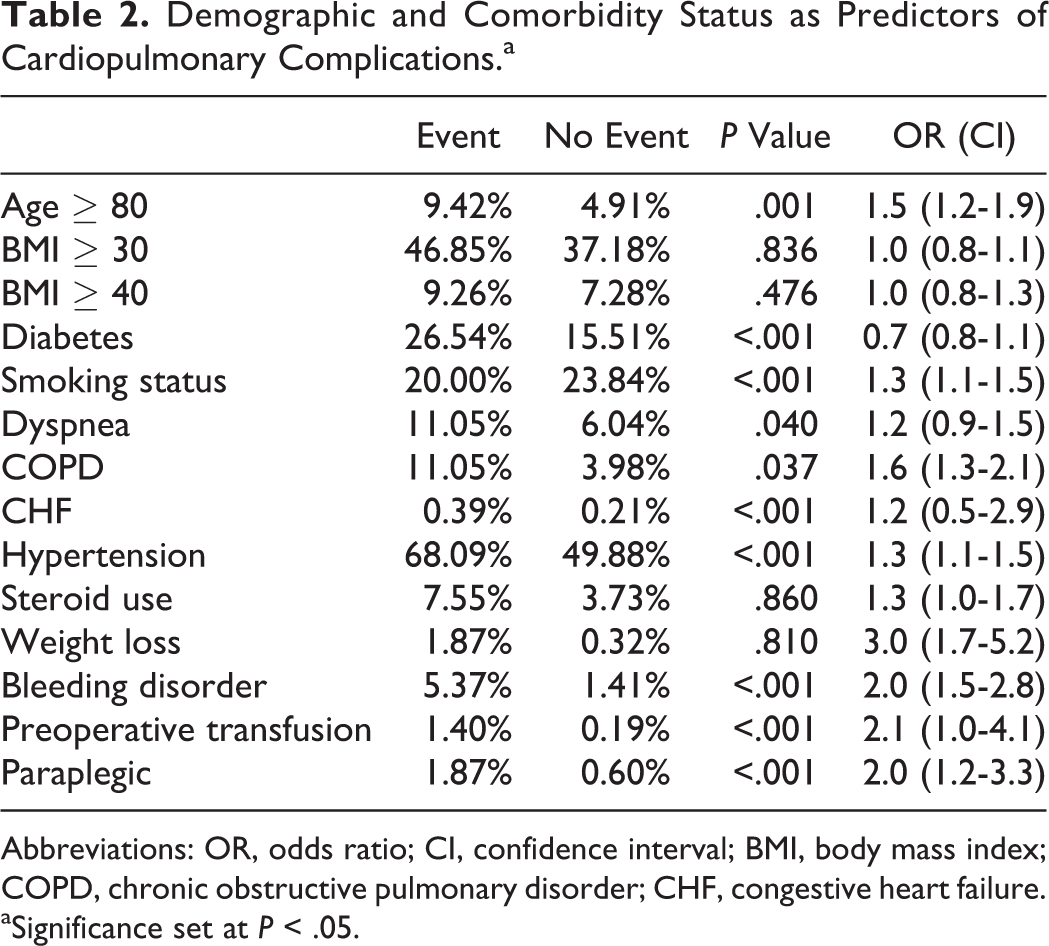
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; COPD, chronic obstructive pulmonary disorder; CHF, congestive heart failure.
aSignificance set at P < .05.
Procedure Risk
Controlling for overall surgical invasiveness, anterior approach was an independent risk factor for any cardiopulmonary event (OR = 1.74; CI = 1.42-2.13; Table 3). Anterior approach including decompression resulted in particularly high risk for airway-related complications: unplanned reintubation (OR = 2.61; CI = 1.89-3.61), extended ventilation (OR = 3.2; CI = 2.28-4.5), and pneumonia (OR = 1.9; CI = 1.39-2.59). Conversely posterior approach procedures displayed decreased odds for airway-related complications (OR < 1). This trend was reversed in pulmonary embolism complications: anterior approach fusion procedures were protective against pulmonary embolism (OR = 0.55; CI = 0.38-0.79), while posterior approach fusion procedures increased risk (OR = 1.43; CI = 1.06-1.91). Procedure-derived odds ratios predicting cardiopulmonary complications were in general close to 1 (range = 0.35-3.81).
Risk Factors for Sustaining a Cardiopulmonary Complication Based on Procedure Type, Spinal Region, and Diagnosis.a
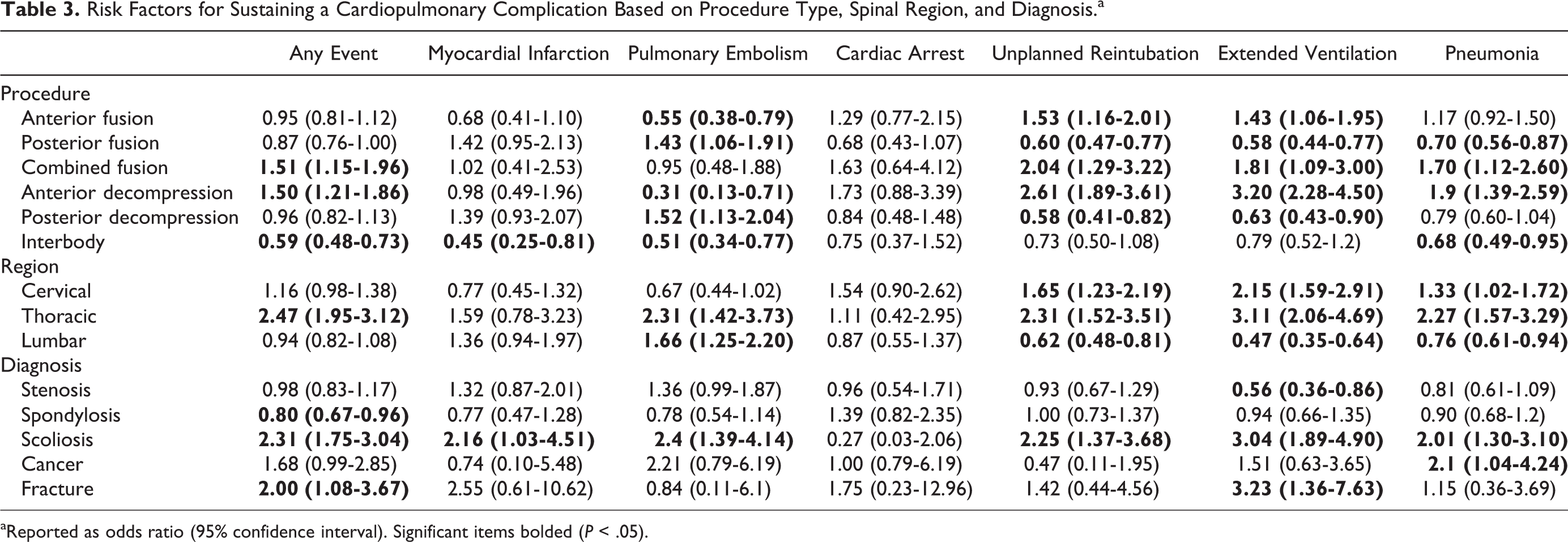
aReported as odds ratio (95% confidence interval). Significant items bolded (P < .05).
Region
After controlling for effects of the overall surgical complexity, only thoracic (OR = 2.47; CI = 1.95-3.12; Table 3) approach independently increased risk for cardiopulmonary complication, particularly extended ventilation (OR = 3.11; CI = 2.06-4.69). Cervical approach was an independent risk factor for airway-related complications (OR > 1), but not cardiac-related complications (OR not significant). Lumbar approach displayed a protective effect against airway complications (OR < 1), but significantly increased risk for pulmonary embolism (OR = 1.66; CI = 1.25-2.2).
Diagnosis
Cancer diagnosis was not a significant risk factor for cardiopulmonary complication (OR = 1.68; CI = 0.99-2.85; Table 3). Scoliosis diagnosis procedures displayed particularly high risk for airway-related complications (OR < 1). However, fracture diagnoses did not, only demonstrating significantly increased risk of extended ventilation (OR = 3.23; CI = 1.36-7.63).
Outcomes after Cardiopulmonary Event
Table 4 follows inpatient outcomes in those patients who experienced a major cardiopulmonary event. Mortality, LOS, discharge status, and reoperation rate were all significantly worsened by cardiopulmonary events (P < .001). Mortality was highest among patients who suffered cardiac arrest (34.57%). Patients on a ventilator >48 hours had the longest LOS (17.58 days), followed by unplanned reintubations (13.04 days). Thirty-day reoperation rates also increased between 325% and 789%, P < .001. A total of 88.09% patients who did not experience any cardiopulmonary event were discharged home.
Outcomes after Cardiopulmonary Event.a
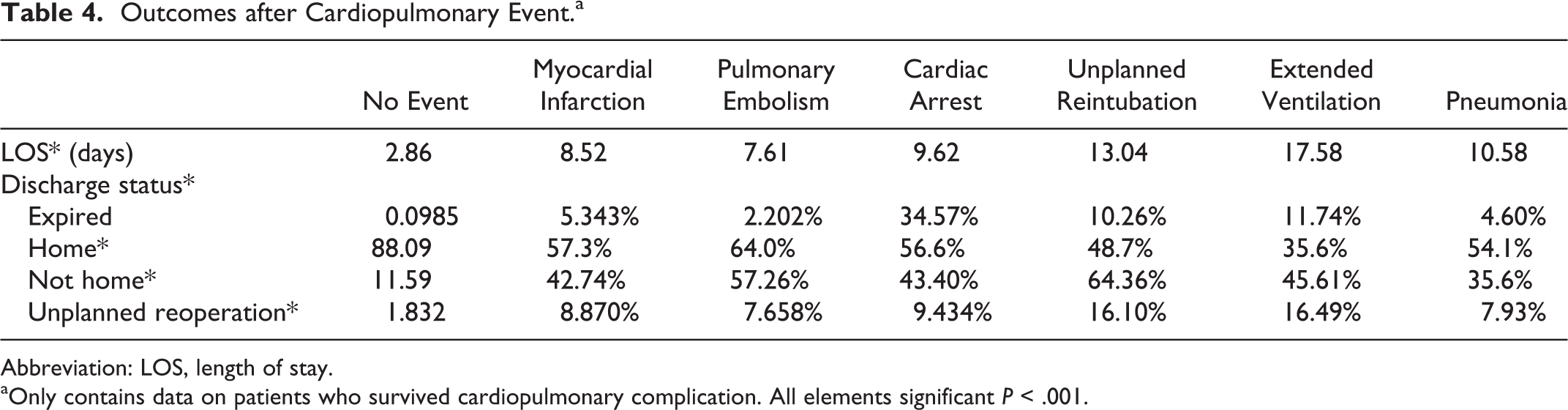
Abbreviation: LOS, length of stay.
aOnly contains data on patients who survived cardiopulmonary complication. All elements significant P < .001.
Discussion
This study demonstrates the incidence and predictors of cardiopulmonary complications following elective spine surgery. Understanding the incidence and risk factors for complications following spine surgery is essential for optimizing postoperative outcomes and improving patient perceptions of their care. Cardiopulmonary complications are the most common cause of death in patients undergoing spinal surgery. 12 Despite this, no study to date has analyzed risk factors for these adverse events in the overall spine cohort.
In our cohort, cardiac arrest had the highest mortality rate following spine surgery. The importance of preoperative cardiac evaluation cannot be understated. Patients with history of coronary artery disease, heart failure, valvular heart disease, arrhythmias, and pulmonary vascular disease deserve special attention and risk stratification. 13 The preoperative assessment should include an evaluation of major adverse cardiac event (MACE) risk using at least one risk stratification tool, the most accepted of which are the RCRI, the NSQIP Myocardial Infarction and Cardiac Arrest, and the NSQIP Surgical Risk Calculator. The RCRI is the most well known and simplest to use, and incorporates high-risk surgery, history of ischemic heart disease, history of congestive heart failure, history of cerebrovascular disease, preoperative treatment with insulin, preoperative creatinine >2.0 mg/dL—interpolating them into a numerical score for interpretation. 9 Patients with MACE >1% according to the RCRI should undergo functional capacity evaluation prior to elective spine surgery.
The risk of MI in spine surgery has been previously studied with reported incidences 30 days postoperatively ranging from 0.13% to 1.6%, with odds significantly increasing with age >65 years, postoperative stay >7 days, operative time >5 hours, intraoperative blood transfusion, baseline creatinine >1 mg/dL, and fusions greater than 1 level. 14,15 Our data supports these previous conclusions and again demonstrate the importance of preoperative cardiac risk stratification. We found that low invasive posterior fusions were associated with a 2-fold rate of MI. Posterior approaches requires going through more layers of tissue, which can increase perioperative blood loss and can lead to hemodynamic instability.
In this study, thoracic and anterior approaches were associated with a significantly higher risk of an adverse cardiopulmonary event, which is consistent with previously reported data. We report an unplanned reintubation rate of 0.43% for all elective spine surgery, with OR significantly higher for anterior cervical procedures. Unplanned reintubation is a well-known complication of anterior cervical spine fusions, the incidence of which has been reported to be 0.5%, which increases to 1.6% with ≥3-level fusions. 16 –19 Possible causes have been attributed to soft tissue swelling, hematoma, and injury from instrumentation. 16 –19 Duration of intubation was also an identified risk factor for perioperative mortality. It is worth noting that this measure may reflect the complex medical circumstances surrounding these patients, which may confound the effect of duration of ventilator dependence itself on mortality rate.
The incidence of pneumonia after anterior cervical discectomy and fusion has been reported to be 0.45% with age being greatest risk factor for this complication. 20 For posterior lumbar interbody fusion, a rate of 0.59% has been reported with comorbid COPD presenting the greatest risk factor. 21 Our cohort is consistent with these previous reports, with a pneumonia rate of 0.61% for all patients in this cohort. The slight increase may be attributable to the fact that our data included patients with thoracic approaches, which may predispose to postoperative respiratory issues.
We found that patients with preoperative chronic spinal cord injury were at higher risk of cardiopulmonary complication following spine surgery. This patient population has been described as vulnerable to thromboembolic disease and autonomic dysreflexia, which can cause rapid changes in hemodynamic stability. 22 Although not without its own risks, inferior vena cava filters have been demonstrated to be protective against pulmonary embolism in patients at high risk for thromboembolic disease and should be considered in these patients prior to surgery. 23
Undergoing any cardiopulmonary event significantly increased the LOS in patients. Yadla et al found the mean LOS increased the most in patients who experienced a pulmonary complication. 24 Similarly, our study found that the LOS was increased the most in patients who had extended ventilation (mean 17.58 days) followed by unplanned reintubation (mean 13.04 days). Similarly, discharge status was significantly poorer in patients who experienced an adverse event. While 88.09% of patients who experienced no event were discharged home, only 35.6%% of patients who required extended ventilation were discharged home. The percentage of people who were discharged to places other than home were increased up to nearly 6-fold in those experienced an adverse event. Discharge to a subacute or nursing facility has been found to be highly correlated with an increased LOS. 25 This change in discharge disposition is expected as these patients may require prolonged care at rehabilitation centers or nursing homes that are equipped to deal with any further complications that may arise.
We found that patients who experienced any cardiopulmonary event also had much higher rates of unplanned reoperation. It is important to note that this includes any and all types of surgical procedures so those patients who experienced an adverse event may not have necessarily had to undergo further spinal surgery. Even so, patients who experience such events are more prone to receiving additional procedures, which may be necessary not only to treat those pathologies but also expose patients to the risks that come along with them.
This study has several limitations, including its retrospective nature. A problem inherent to large database studies is that data analysis is limited to what was included in the database design. Specifics of surgical technique, diagnostic imaging, and a complete list of medical comorbidities are not reported and therefore there are likely some outcomes which are not captured or which are influenced by confounding variables for which there is no control. In general, however, the NSQIP database is a representative national sample with generalizable results.
Conclusion
This study reports the rates of cardiopulmonary complications after spinal surgery. The strongest risk factors for these events include thoracic approaches, as well as patients with anterior or combined approach procedures, and patients indicated for high-risk procedures. This agrees with risk factors seen in the RCRI. These patients deserve special attention during presurgical planning, with emphasis on cardiac risk stratification in order to prevent or anticipate complications during the hospital stay.
Supplemental Material
Supplemental Material, Appendix_A - Adverse Outcomes and Prediction of Cardiopulmonary Complications in Elective Spine Surgery
Supplemental Material, Appendix_A for Adverse Outcomes and Prediction of Cardiopulmonary Complications in Elective Spine Surgery by Peter G. Passias, Gregory W. Poorman, Edward Delsole, Peter L. Zhou, Samantha R. Horn, Cyrus M. Jalai, Shaleen Vira, Bassel Diebo, and Virginie Lafage in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
The supplemental material is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.