
Abstract
Study Design:
A systematic review and meta-analysis.
Objectives:
Outpatient cervical disc replacement (CDR) has been performed with an increasing trend in recent years. However, the safety profile surrounding outpatient CDR remains insufficient. The present study systematically reviewed the current studies about outpatient CDR and performed a meta-analysis to evaluate the current evidence on the safety of outpatient CDR as a comparison with the inpatient CDR.
Methods:
We searched the PubMed, Embase, Web of Science, and Cochrane Library databases comprehensively up to April 2020. Patient demographic data, overall complication, readmission, returning to the operation room, operating time were analyzed with the Stata 14 software and R 3.4.4 software.
Results:
Nine retrospective studies were included. Patients underwent outpatient CDR were significantly younger (mean difference [MD] = −1.97; 95% CI −3.80 to −0.15; P = .034) and had lower prevalence of hypertension (OR = 0.68; 95% CI 0.53-0.87; P = .002) compared with inpatient CDR. The pooled prevalence of overall complication was 0.51% (95% CI 0.10% to 1.13%) for outpatient CDR. Outpatient CDR had a 59% reduction in risk of developing complications (OR = 0.41; 95% CI 0.18-0.95; P = .037). Outpatient CDR showed significantly shorter operating time (MD = −18.37; 95% CI −25.96 to −10.77; P < .001). The readmission and reoperation rate were similar between the 2 groups.
Conclusions:
There is a lack of prospective studies on the safety of outpatient CDR. However, current evidence shows outpatient CDR can be safely performed under careful patient selection. High-quality, large prospective studies are needed to demonstrate the generalizability of this study.
Introduction
Cervical disc replacement (CDR) is a commonly used procedure for the treatment of cervical degenerative disc disease (CDDD). With the aging of population and change of lifestyle, the number of CDR performed annually is increasing, with an average of 17% increment per year. 1 Compared with the traditional anterior cervical discectomy and fusion (ACDF), CDR preserves the motion function at pathological levels and restores the biomechanical properties of the intact cervical spine to the most extent. Biomechanical studies have shown that the intervertebral disc pressure and segmental motion at adjacent levels of CDR are comparable with those of the intact cervical spine. 2 -4 Randomized controlled studies (RCTs) also demonstrated that CDR could prevent adjacent segment degeneration (ASD) compared with ACDF. 5 -7 Therefore, CDR has become an important option for the treatment of CDDD.
Although CDR is efficient in treating cervical degenerative disc disease, the costs of this procedure are very high. Kumar et al 8 used the MarketScan database and found that the mean cost of CDR was $28 664. Jain et al 1 reviewed the PearlDiver Patient Record Database and found that the mean cost for single-level CDR was about $35 000 and for multilevel CDR was about $62 000. Their evidence suggests that CDR brings a great economic burden to patients and the health care system.
Recently, with the advances in anesthesiology and the development of Enhanced Recovery After Surgery (ERAS), many surgeries have been transited to outpatient procedures. The outpatient surgery does not need an overnight stay in the hospital, this not only increases patient satisfaction 9,10 but also reduces hospital-related costs. In fact, several studies reported that compared with inpatient procedures, outpatient CDR reduced the mean cost by 42% to 84%. 11,12 Therefore, outpatient CDR could be a useful way to reduce costs.
Outpatient CDR has been performed with an increasing trend in recent years. 1,13 Several studies have reported the efficacy and safety of outpatient CDR. 11 -19 However, the generalizability of these studies is limited by the small sample size and lack of control groups. Therefore, the safety profile surrounding outpatient CDR remains insufficient.
In this study, we systematically reviewed the current studies about outpatient CDR and performed a meta-analysis to evaluate the current evidence on the safety of outpatient CDR as a comparison with the inpatient CDR.
Methods
This study was conducted following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines. The protocol of this study has been registered on the Open Science Framework website (10.17 605/OSF.IO/3597Z).
Search Strategy
We searched the following database from inception to April 15, 2020: PubMed, Embase, Web of Science, and Cochrane Library. The following search keywords were used in all databases: “total disc replacement,” “outpatients,” “ambulatory.” The search strategy uploaded onto the Open Science Framework website (osf.io/szuy9/). Articles wrote in English were included. The reference lists of the eligible studies were reviewed to identify the potentially relevant studies.
Eligibility Criteria
The inclusion criteria of this study were listed as follows: (1) Type of studies: Considering that the majority of published studies on this topic are retrospective studies, both prospective studies and retrospective cohort studies were included. (2) Type of interventions: Studies reporting the outcomes of outpatient CDR were included. (3) Types of outcomes: Studies reporting the incidence of overall complication, readmission, and reoperation after outpatient CDR were included. Two authors (XW and HW) independently included the eligible studies, and no disagreement was noted in this process between the 2 authors.
Data Extraction
The following data was extracted: (1) Study information, including author name, year of publication, conflict of interest, funds, type of study, sample size, type of device, definition of outpatient surgery, and follow-up time period. (2) Patient information, including age, gender, body mass index (BMI), and comorbidities. (3) Surgical information, including operating time, surgical level, and length of stay. (4) All reported outcomes, including complications found in outpatient CDR, readmission, and reoperation. Data extraction was performed by 2 authors (XW and HW). Any disagreement between the 2 authors was solved by consulting a senior author (HL).
Quality Assessment
The Newcastle-Ottawa scale (NOS) was used to evaluate the quality of eligible studies. Two authors (XW and HW) performed the assessment independently according to previous research. Any disagreement between the 2 authors was solved by consulting a senior author (HL).
Statistical Analysis
This meta-analysis was conducted using Stata (V.14, StataCorp) software, and R (V.3.4.4, R Foundation for Statistical Computing). Mean differences (MDs) with 95% confidence intervals (CIs) were used to display continuous variables. Odds ratio (OR) with 95% CI were used for the analysis of categorical variables. The incidence of overall complication of outpatient CDR was pooled and displayed with 95% CI. P < .05 was considered to be statistically different. The heterogeneity among included studies was assessed using the I2 test. An I2 value >50% was considered as high heterogeneity, and data was analyzed using the random-effects model. Otherwise, data was analyzed using the fixed-effects model. Subgroup analysis was performed according to the surgical level. The funnel plot, Begg’s test, and Egger’s regression test were used to examine the publication bias.
Results
Literature Search Results
Nine retrospective cohort studies matched the eligibility criteria of our study (Figure 1). Among them, 1 study was published in 2010 and the rest of the studies were published between 2017 and 2020. Five studies compared the safety of outpatient CDR with inpatient CDR, 1 study compared the outpatient CDR with outpatient ACDF, while 3 studies only reported outcomes of outpatient CDR. The basic characteristics of these studies are summarized in Tables 1 and 2. Bovonratwet el al 15 and Segal et al 14 used the same database (National Surgical Quality Improvement Program [NSQIP]) and may have overlapping data sets. However, the study by Segal et al 14 had a larger sample size; therefore, it was included in the quantitative analysis.
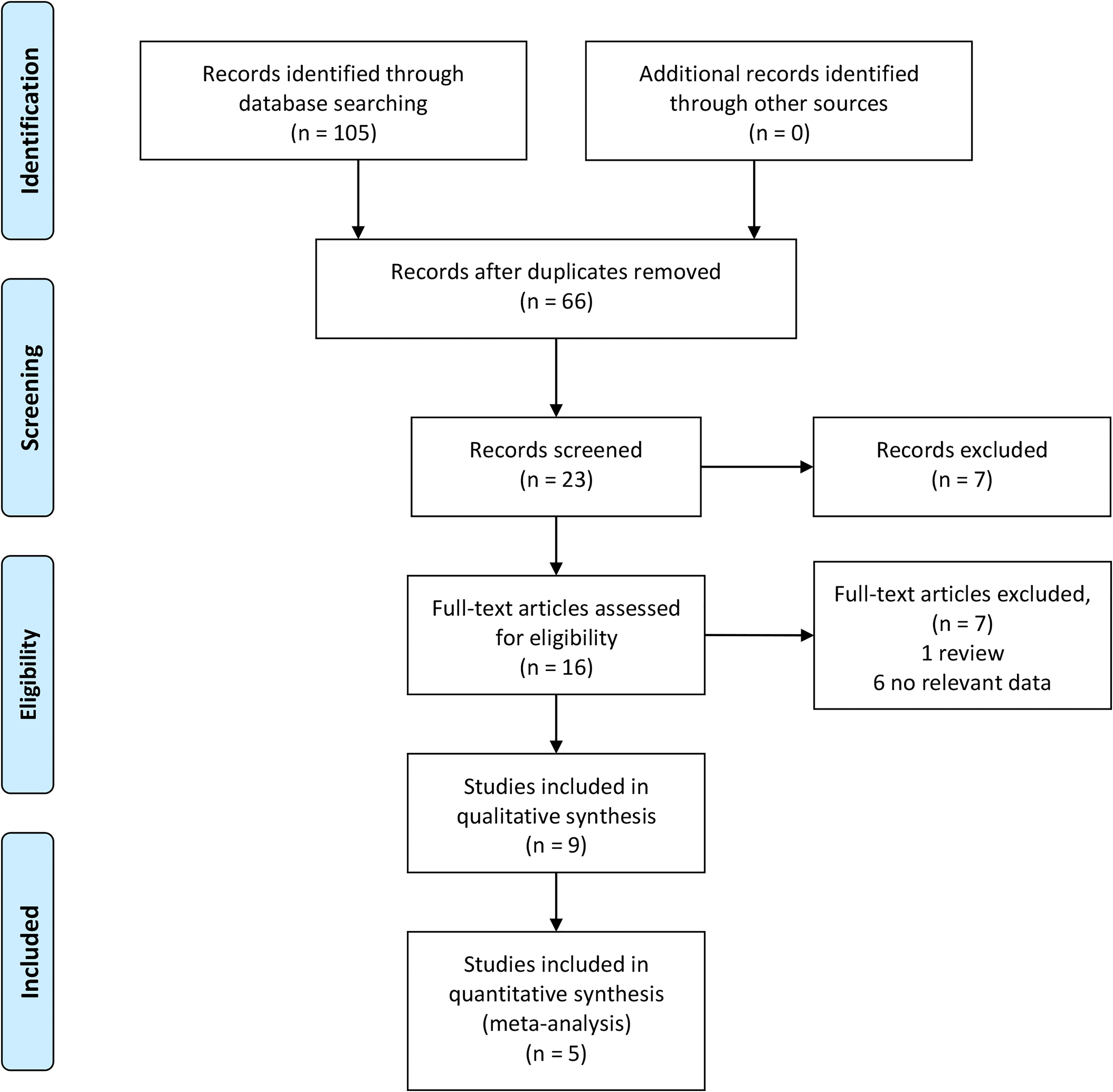
PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) flowchart.
Summary of the Safety Profile of Outpatient Cervical Disc Replacement.
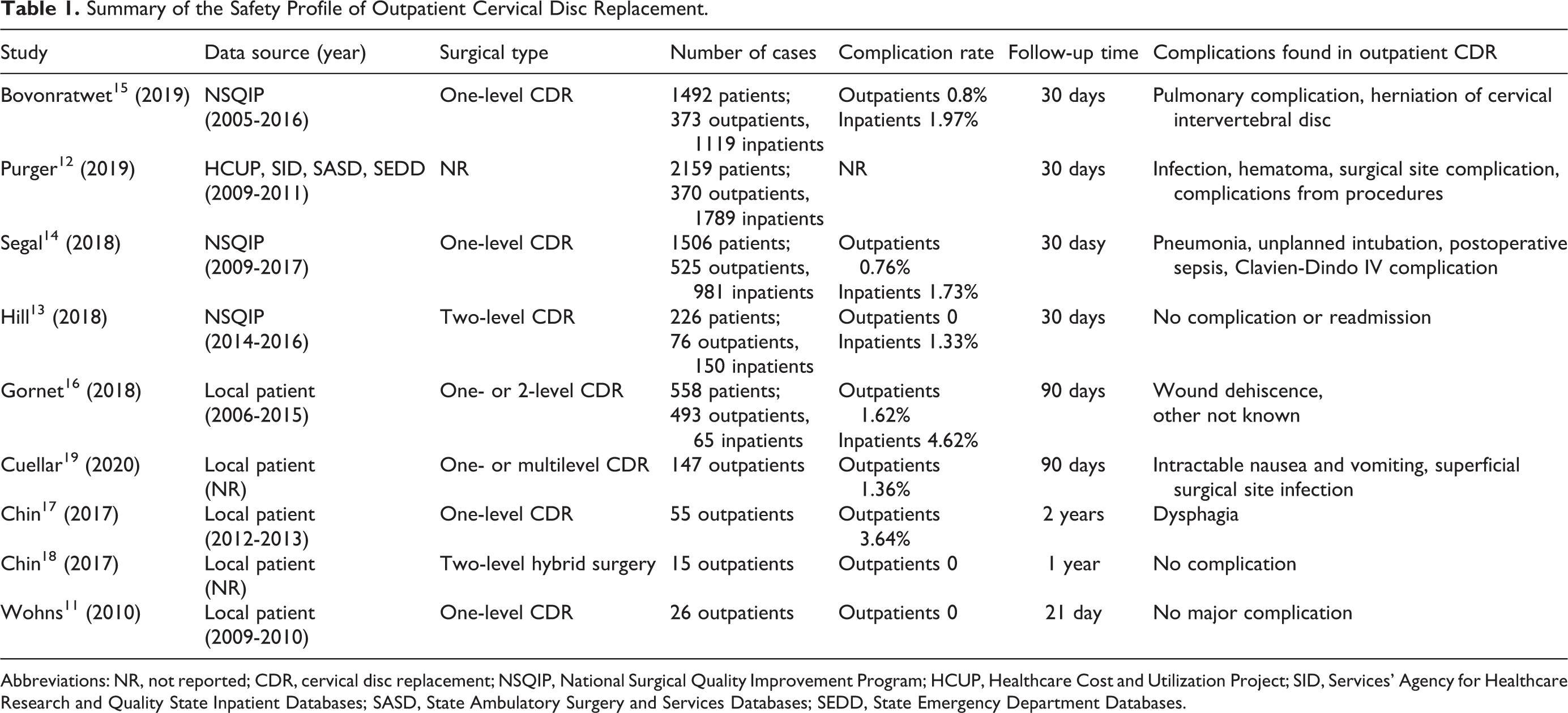
Abbreviations: NR, not reported; CDR, cervical disc replacement; NSQIP, National Surgical Quality Improvement Program; HCUP, Healthcare Cost and Utilization Project; SID, Services’ Agency for Healthcare Research and Quality State Inpatient Databases; SASD, State Ambulatory Surgery and Services Databases; SEDD, State Emergency Department Databases.
Basic Characteristics of Included Studies.
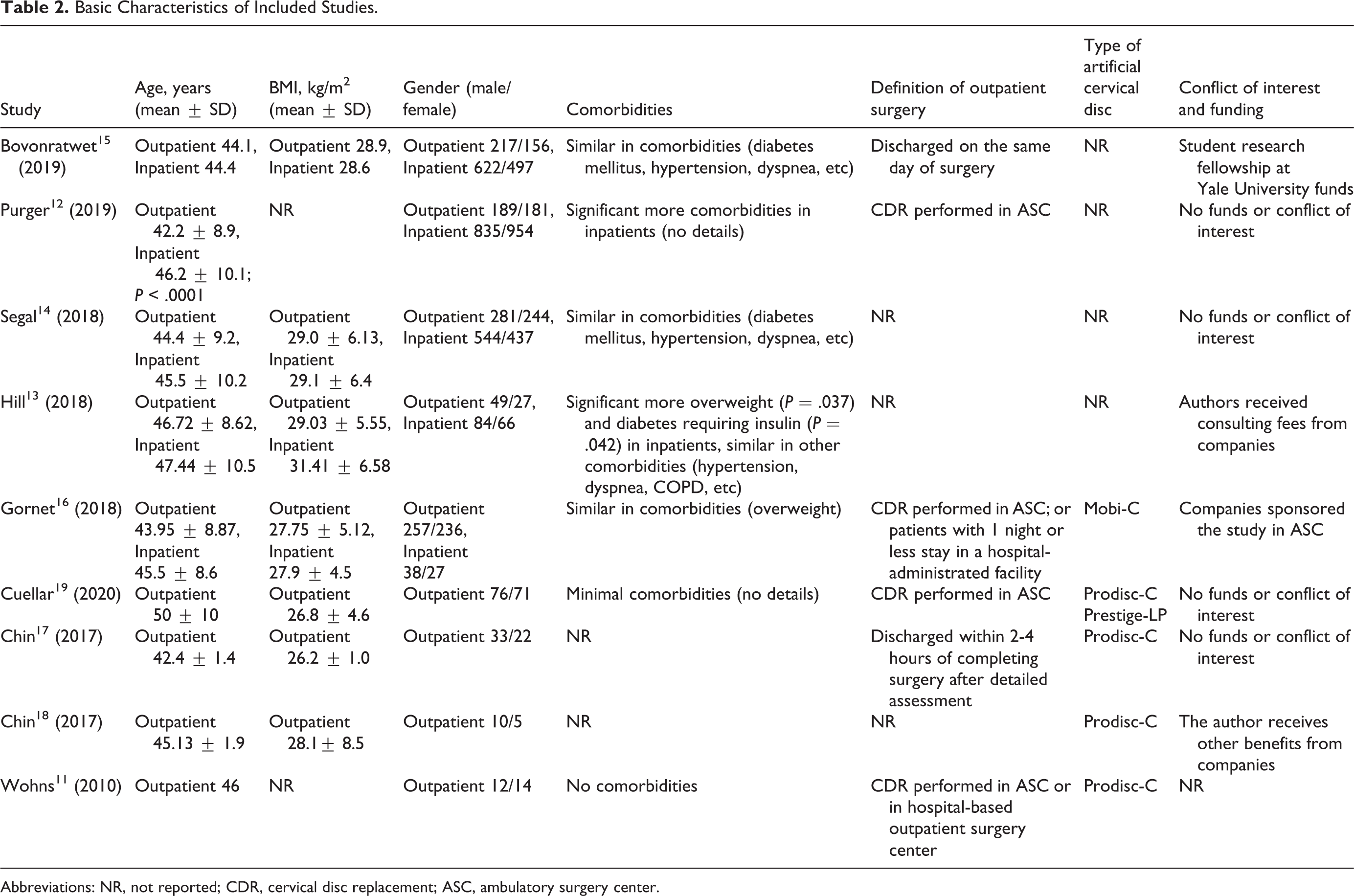
Abbreviations: NR, not reported; CDR, cervical disc replacement; ASC, ambulatory surgery center.
Study Quality Assessment
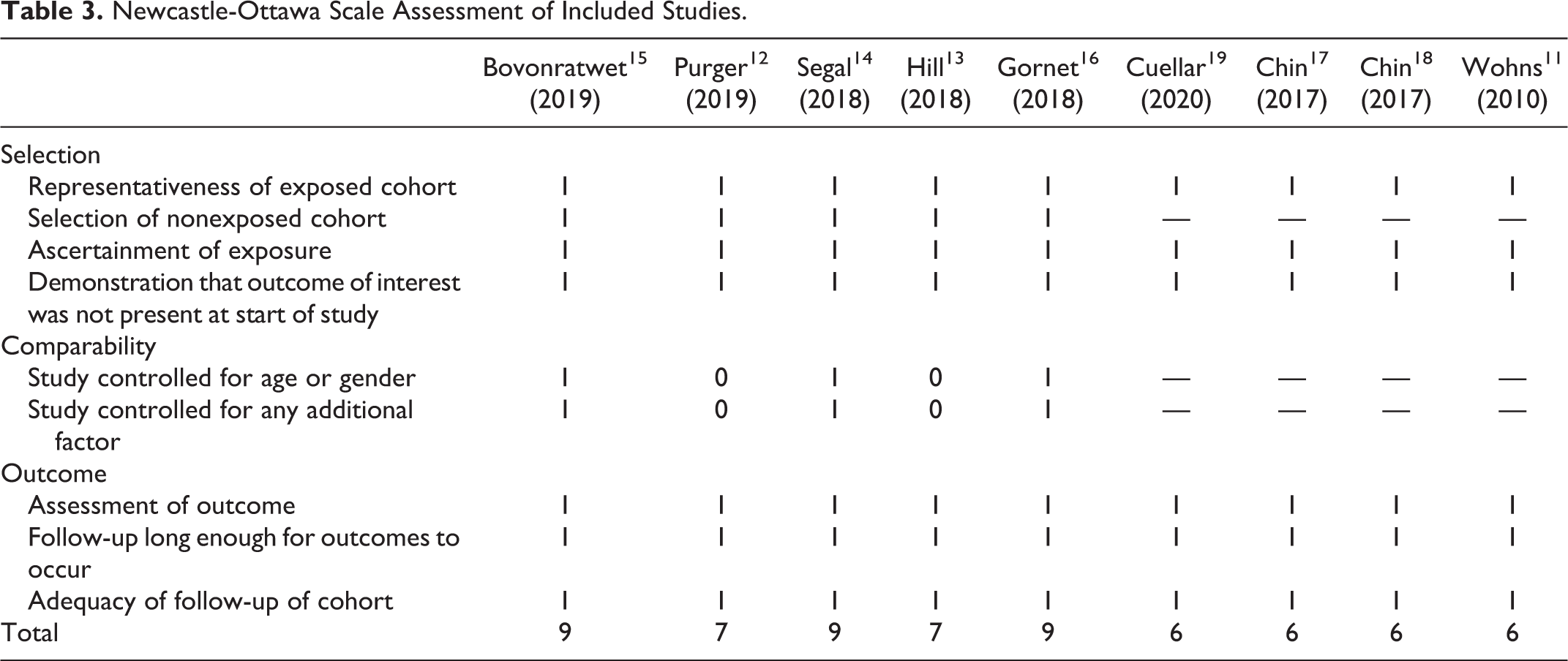
The results of the quality assessment are listed in Table 3. For studies that directly compared outcomes of outpatient CDR with inpatient CDR, 3 of them scored 9 points, and 2 of them scored 7 points. The other 4 studies that reported outcomes of outpatient CDR scored 6 points. All studies were of good quality.
Newcastle-Ottawa Scale Assessment of Included Studies.
Demographic Data of Included Studies
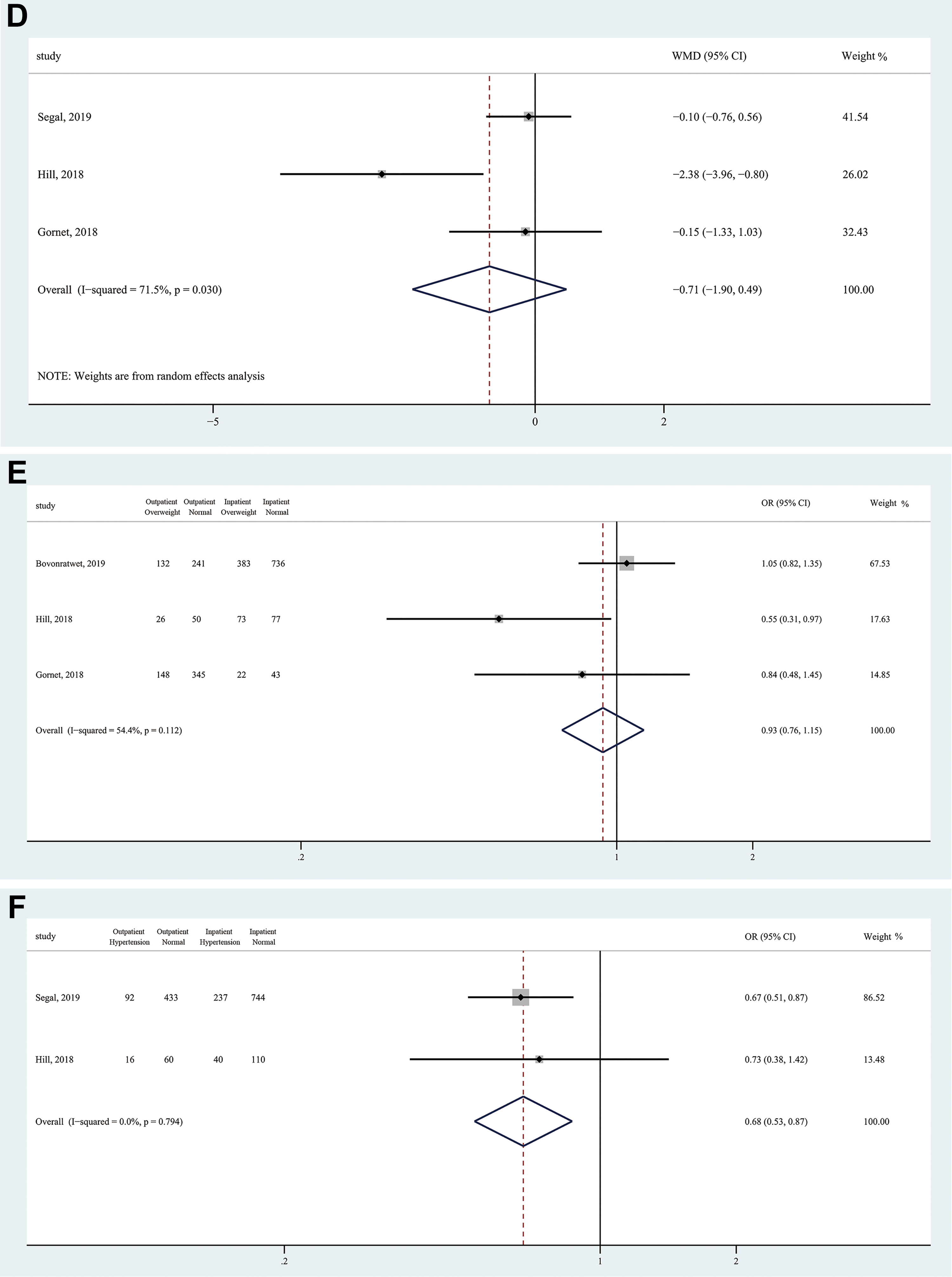
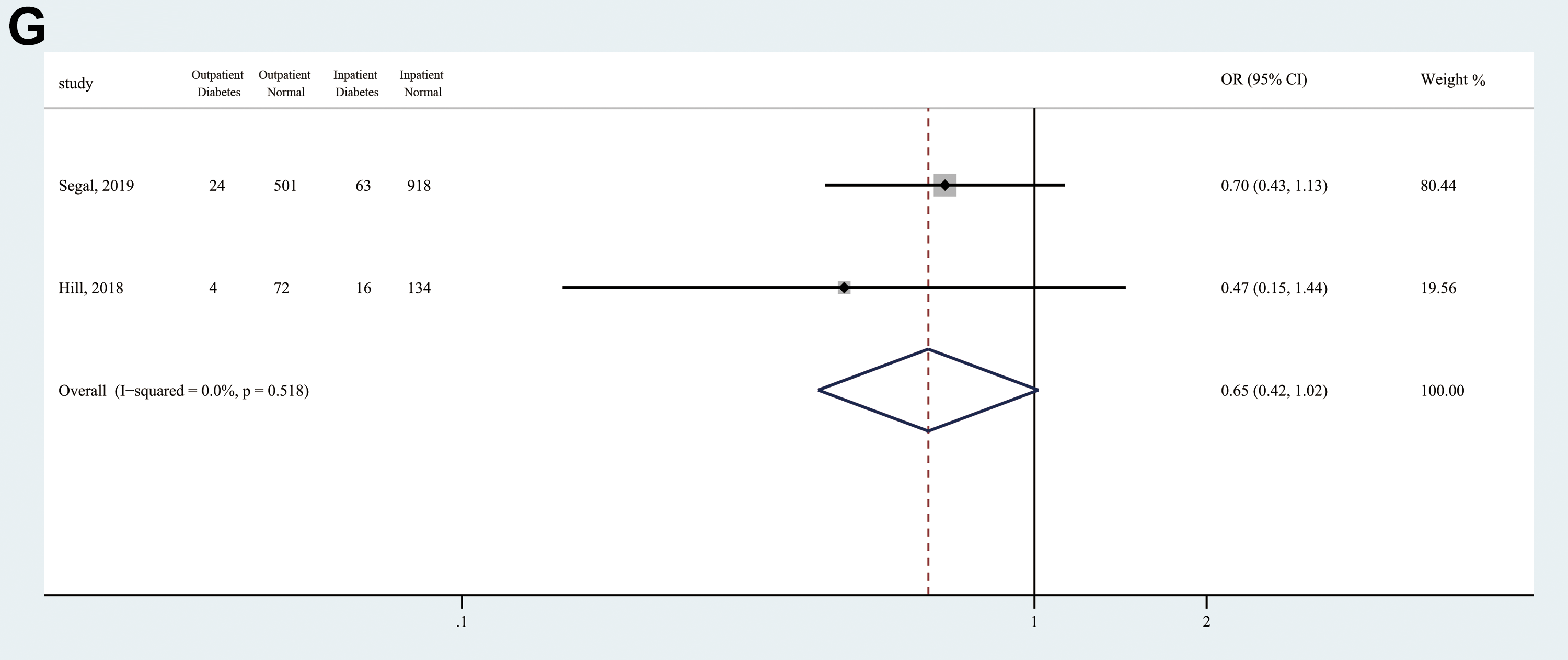
The demographic data of included studies is summarized in Table 2 and Figure 2. Outpatients and inpatients had a similar sex distribution (OR = 1.04, 95% CI 0.90-1.20; Z = 0.55, P = .582), body mass index (BMI) (MD = −0.71, 95% CI −1.91 to 0.50; Z = 1.16, P = .245), smoking status (OR = 1.02, 95% CI 0.91-1.28; Z = 0.14, P = .888), and the prevalence of diabetes (OR = 0.65, 95% CI 0.42-1.02; Z = 1.89, P = .059) and overweight (OR = 0.93, 95% CI 0.76-1.15; Z = 0.66, P = .508). However, outpatients had significantly younger age (MD = −1.97; 95% CI −3.80 to −0.15; Z = 2.12; P = .034) and lower prevalence of hypertension (OR = 0.68; 95% CI 0.53-0.87; Z = 3.09; P = .002) compared with inpatients.
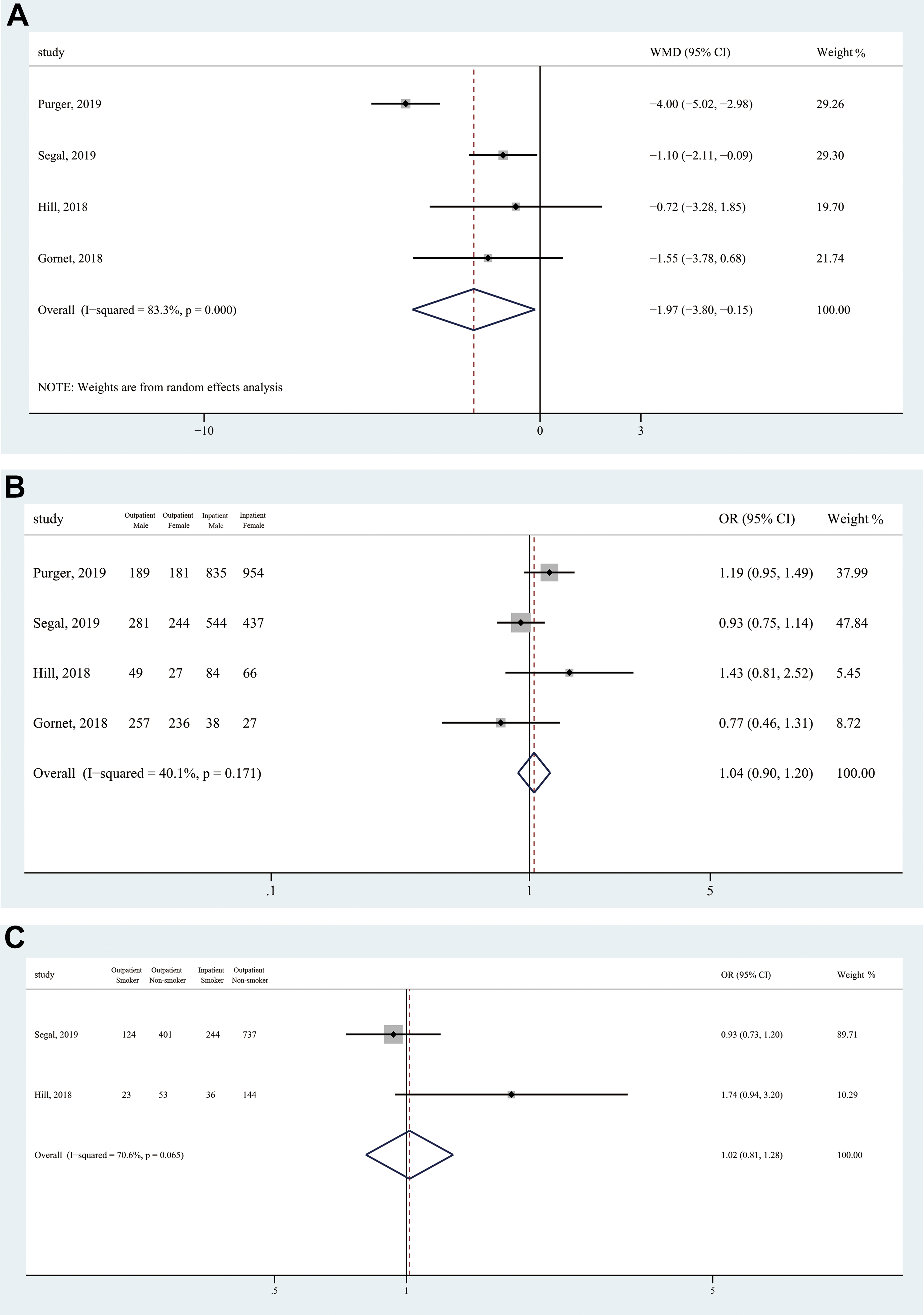
Forest plots of patients’ demographic data among included studies. (a) Age, (b) gender, (c) smoking status, (d) body mass index, (e) overweight, (f) hypertension, and (g) diabetes.
Overall Complication
Eight studies reported overall complication rates for outpatient CDR, ranging from 0% to 3.64%. The safety profile is summarized in Table 1. Four studies reported overall complication rates for inpatient CDR, ranging from 1.33% to 4.62%. The pooled prevalence of overall complication was 0.51% (95% CI 0.10% to 1.13%) when applying the fixed-effects model (Figure 3A). Subgroup analyses were performed based on levels of operation using the fixed-effects model. One-level outpatient CDR showed a lower complication rate (0.37%; 95% CI 0.01% to 1.04%) than multilevel outpatient CDR (1.15%; 95% CI 0.14% to 2.76%). There were no deaths after outpatient CDR in included studies.
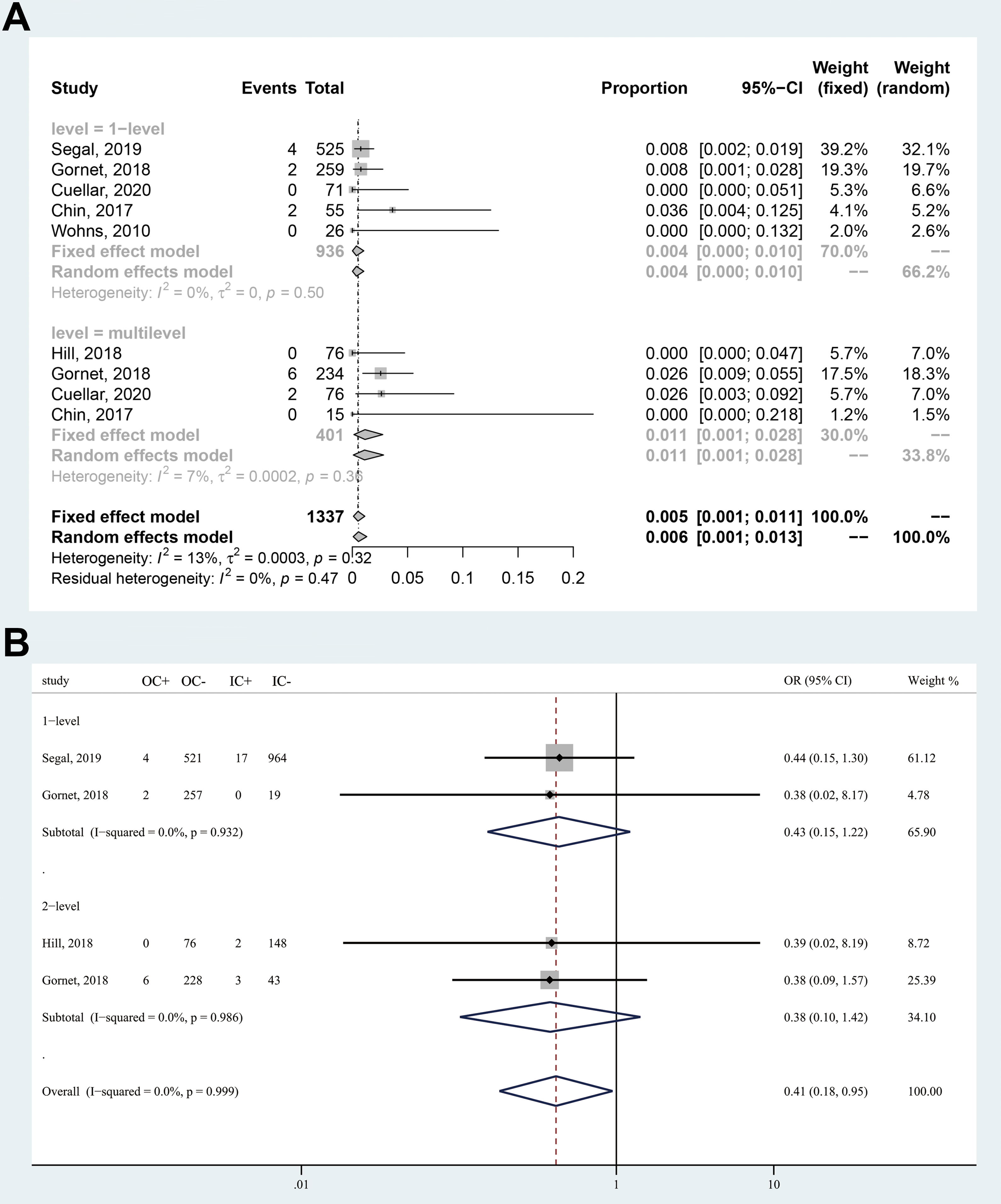
Forest plots of complication rate after surgery. (a) Overall complication rate after outpatient cervical disc replacement. (b) Comparison between outpatient and inpatient procedure. “C+” indicates number of patients with complications; “C−” indicates number of patients without complications; “O” indicates outpatient; “I” indicates inpatient.
Compared with inpatient CDR, patients underwent outpatient CDR had a 59% reduction in risk of developing complications (OR = 0.41; 95% CI 0.18-0.95; Z = 2.09; P = .037) without heterogeneity (I2 = 0), as showed in Figure 3B.
The included studies reported no deaths during their follow-up period. The detailed complications for outpatient CDR are listed as follows. Bovonratwet et al. 15 reported that one patient occurred pulmonary complications (on ventilator >48 hours, unplanned intubation, or pneumonia) during the 30-day postoperative period after discharge. Segal et al 14 reported 4 patients with postoperative complications, including 1 Clavien-Dindo IV complication, 1 pneumonia, 1 unplanned intubation, and 1 sepsis. Hematoma was reported by Purger et al 12 with an incidence of 0.27%. Purger et al 12 and Cuellar et al 19 reported 1 case of surgical site infection separately. Cuellar et al 19 also reported 1 case of intractable nausea. Gornet et al 16 reported 8 adverse events, but only wound dehiscence was shown in their article. Dysphagia was reported by Chin et al. 17
Readmission
Three studies reported the incidence of readmission within 30 days after outpatient CDR compared with inpatient procedure (Figure 4). Patients had a 47% reduction in risk of returning to hospital after surgery if they underwent outpatient CDR (OR = 0.53; 95% CI 0.25-1.11; Z = 1.68; P = .094). The result showed no heterogeneity (I2 = 0). Although the result favored outpatient CDR, it was not highly significant.
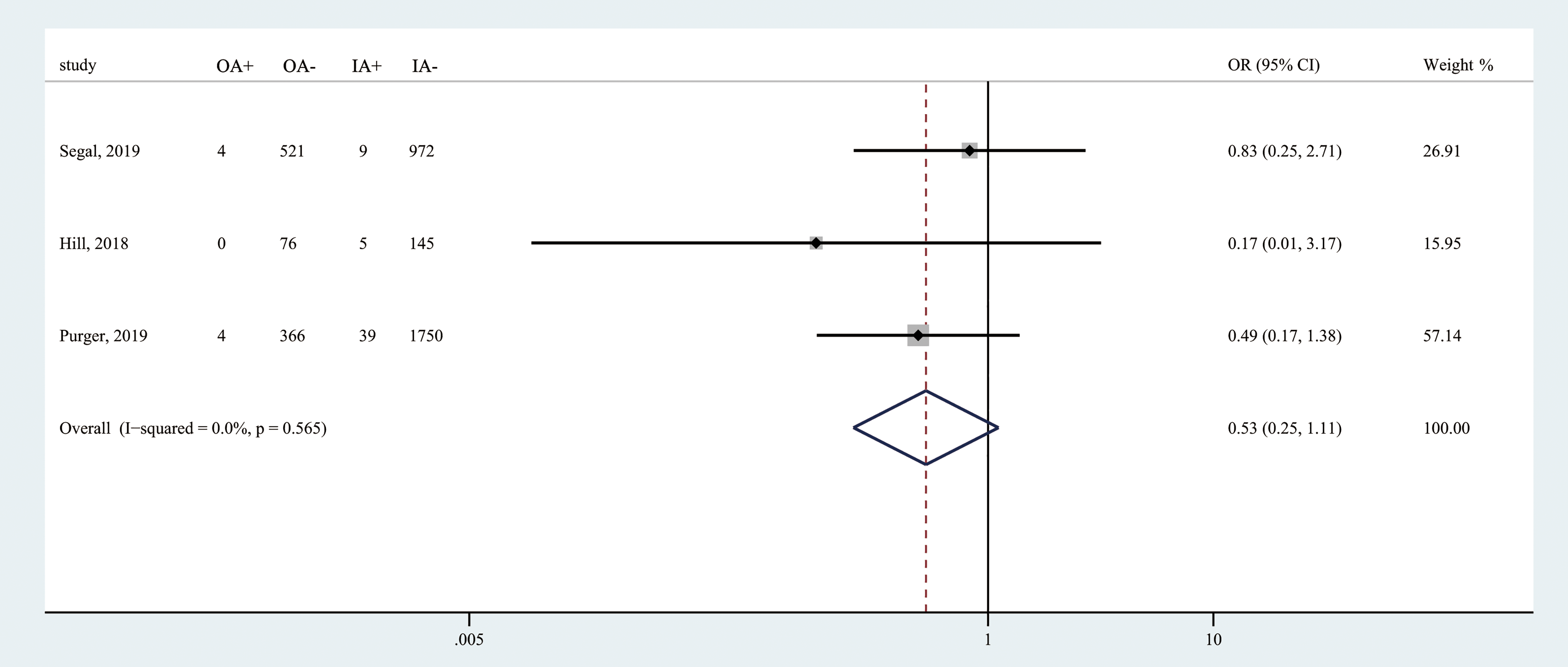
Forest plot of readmission rate among included studies. “A+” indicates number of patients returning to hospital; “A−” indicates number of patients not returning to hospital; “O” indicates outpatient; “I” indicates inpatient.
The reasons for readmission of outpatient CDR are listed as follows. Bovonratwet et al 15 reported 2 readmissions of outpatient CDR, 1 with cervical disc displacement (International Classification of Diseases, Ninth Revision [ICD-9]: 722.0), the other with radiculopathy of the cervical region (ICD-9: 723.4). Purger et al 12 reported 19 times of emergency department visits within 30 days after surgery; reasons included chest pain, nausea/vomiting, limb pain, mental disorder, spasm of muscle, headache, and other symptoms involving head and neck. Among them, 2 patients underwent readmission for infection, hematoma, or surgical site complications. The other 2 patients were readmitted for depressive or other reasons. Cuellar et al 19 reported 2 unplanned readmissions for intractable nausea and wound infection.
Return to the Operation Room
Four studies reported the incidence of returning to the operation room within 30 to 90 days after surgery (Figure 5). Patients had a 51% reduction in risk of returning to operation room if they underwent outpatient procedure (OR = 0.49; 95% CI 0.16-1.49; Z = 1.25; P = .210). However, this result was not statistically significant. There was no heterogeneity among included studies (I2 = 0).
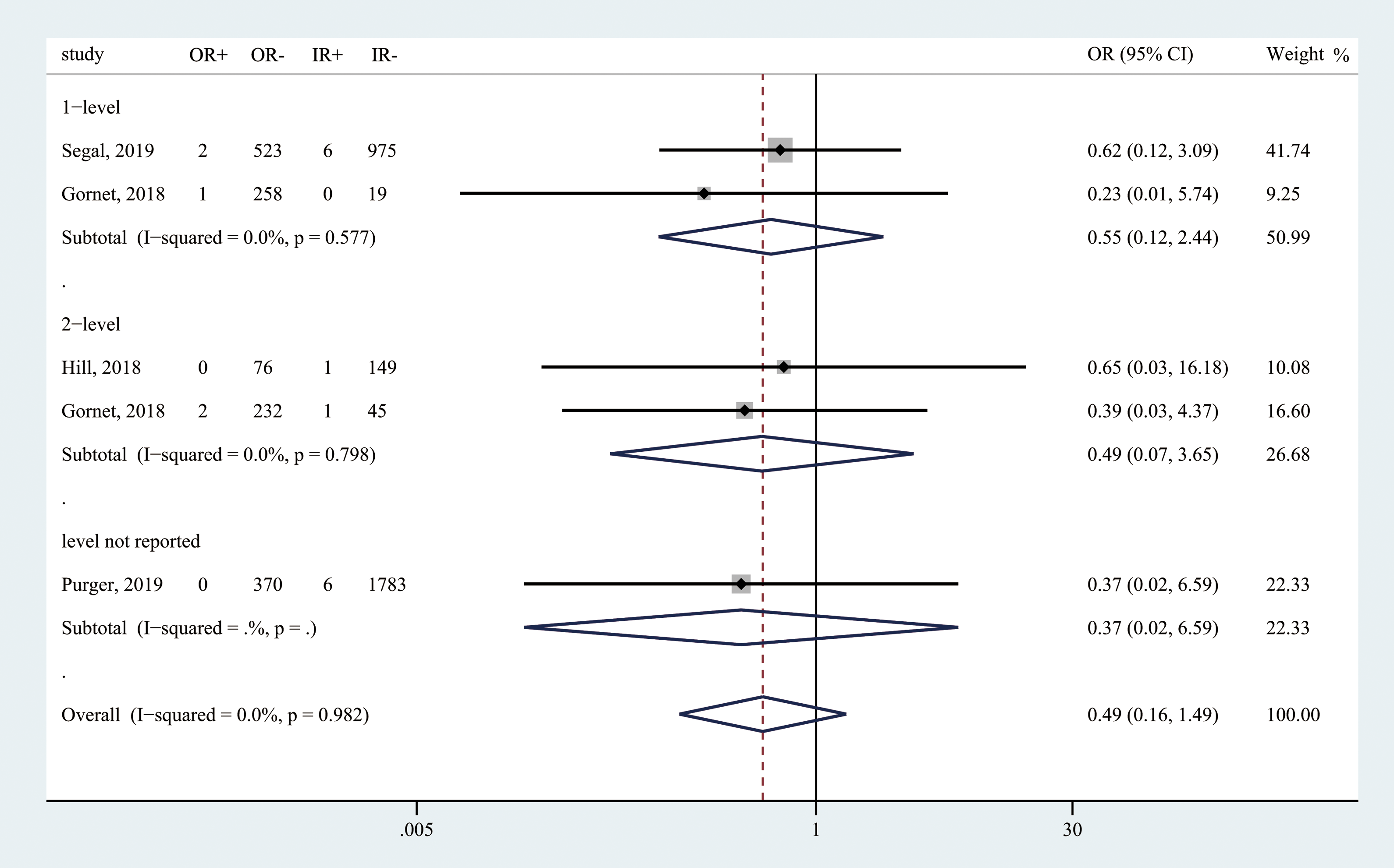
Forest plot of reoperation rate among included studies. “R+” indicates number of patients returning to the operation room; “R−” indicates number of patients not returning to the operation room. “O” indicates outpatient; “I” indicates inpatient.
The reasons for return to the operation room of outpatient CDR are listed as follows. Bovonratwet et al 15 reported 1 patient who underwent secondary surgery due to cervical disc displacement (ICD-9: 722.0). Gornet et al 16 reported 3 patients who underwent additional operation of the cervical spine during the 90-day period postoperation.
Operating Time
Three studies reported the operating time of inpatient and outpatient CDR (Figure 6). Compared with the inpatient group, the outpatient group had a significantly shorter operating time (MD = −18.37; 95% CI −25.96 to −10.77; Z = 4.74; P < .001) with median heterogeneity (I2 = 35.6%).
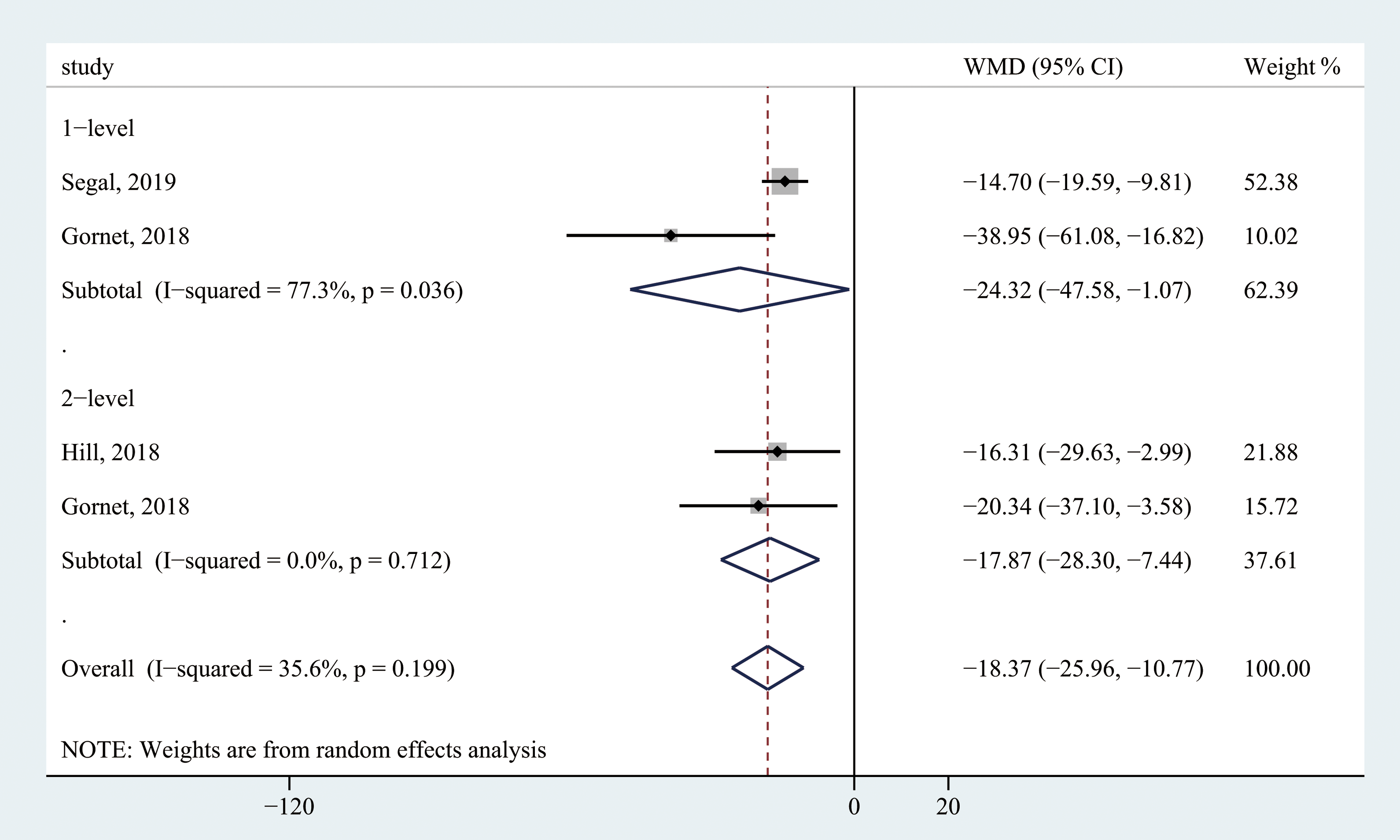
Forest plot of operating time among included studies.
Cost for Outpatient CDR
Two studies reported the cost between the outpatient group and the inpatient group. 11,12 Both studies found the average cost for outpatient CDR was lower compared with inpatient procedure (Table 4). Purger et al 12 calculated the 90-day total cost and actual cost. The outpatient group reduced the total cost by 42.0% ($46 404.03 vs $80 055, P < .0001) and reduced the actual cost by 35.1% ($11 059 vs $17 033, P < .001) compared with the inpatient group. Wohns et al 11 calculated the total cost for surgeries, which was defined as the billed charges for the technical component, implant, and professional fee. They found the outpatient CDR reduced the total cost by 83.6% compared with inpatient CDR ($11 144.83 vs $68 000, P value unknown) and by 62.0% compared with outpatient ACDF ($11 144.83 vs $29 313.43, P value unknown). However, it should be noted that there is a lack of high-quality studies regarding the cost-effectiveness of outpatient CDR.
The Average Costs for Outpatient and Inpatient Cervical Disc Replacement.
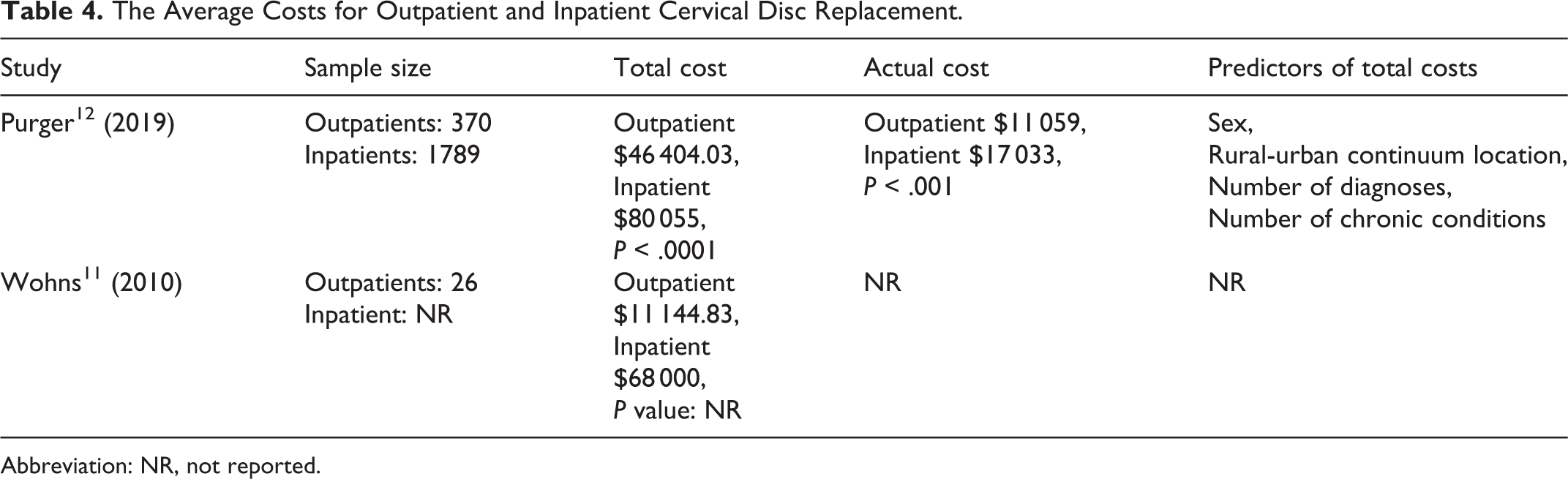
Abbreviation: NR, not reported.
Publication Bias
The funnel plot was graphed to evaluate the publication bias for the overall complication rate (Figure 7). The Begg’s test (P = .462) and Egger’s test (P = .593) showed there was no asymmetry in the funnel plot. Although these results did not reveal publication bias, the evaluating ability declined because of a lack of enough publications.
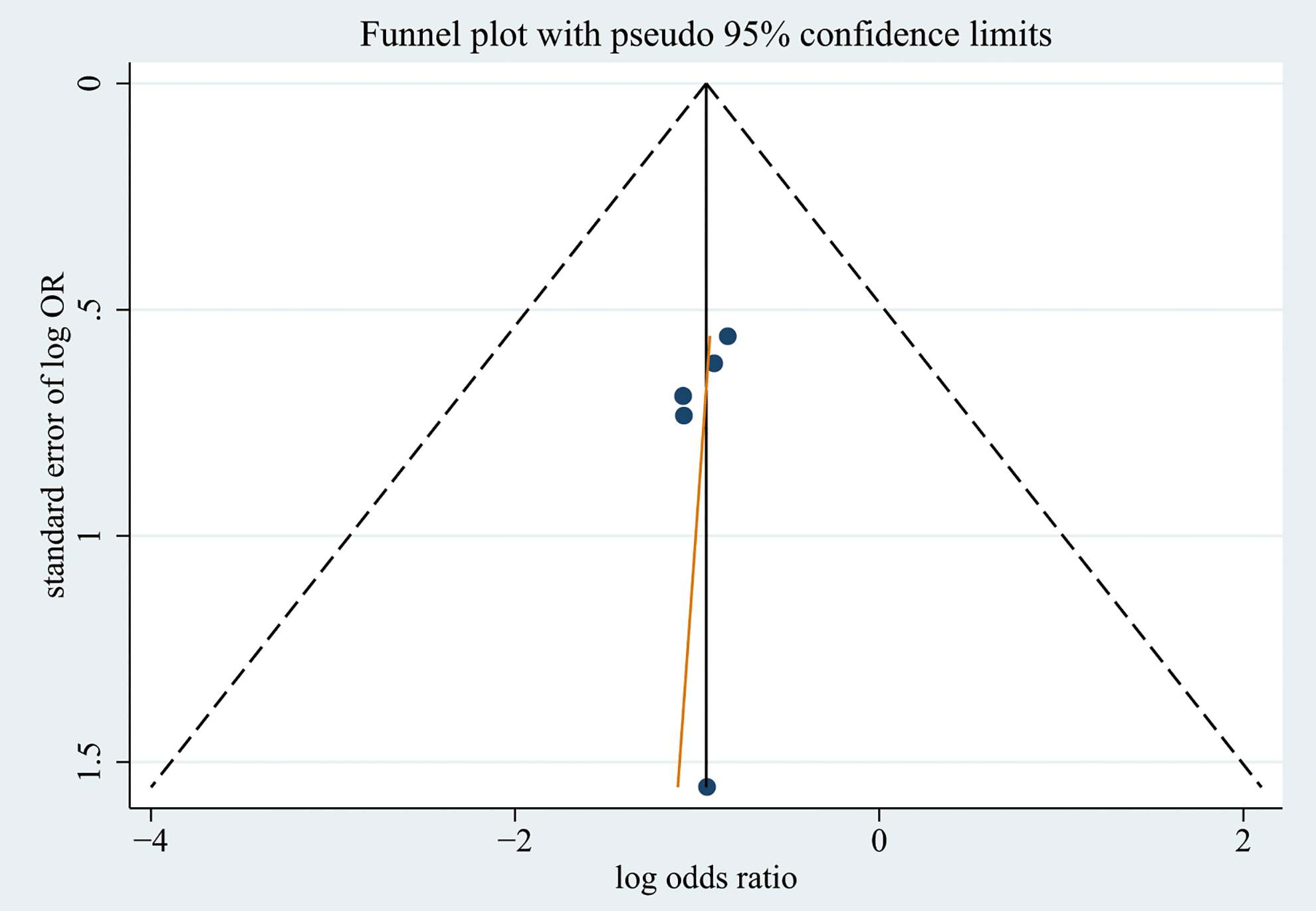
Funnel plot evaluating publication bias for overall complication among included studies.
Discussion
The number of surgeries performed in outpatient centers has dramatically increased from 3.7 million in 1981 to over 54 million annually nowadays. 20,21 The transition of inpatient surgeries to the outpatient setting has been considered as a cost reduction strategy. Spine surgery especially represents a huge development prospect in the outpatient surgery, because spine surgeries represent about 25% of orthopedic surgeries but contribute over 50% to the profit. 20 It is reported that the transition of inpatient spine procedures to outpatient settings could reduce 60% cost associated with the operating room and postoperative care. 20 An obvious reduction in total cost was also reported in outpatient CDR by Wohns et al 11 and Purger et al. 12 However, one of the major concerns that hindering the extension of outpatient spine surgeries is that whether they can be effectively and safely performed.
Currently, there are multiple literature reviews describing outcomes of outpatient lumbar surgery and outpatient ACDF. However, the comprehensive understanding of the safety profile of outpatient CDR is lacking. Hence, we performed this systematic review and meta-analysis of current studies. We found that the readmission and reoperation rates were similar between inpatients and outpatients. In addition, the outpatient CDR had a significantly lower incidence of overall complication and shorter operating time.
There are several reasons for the significantly lower complication rate after outpatient CDR. First, patient selection criteria for outpatient CDR is strict. Usually, younger patients and healthier patients with fewer comorbidities tend to receive outpatient procedures. For instance, Purger et al 12 reported outpatients were 4 years younger than inpatients, and outpatients had significantly fewer comorbidities than inpatients. Hill et al 13 reported that overweight and diabetes were more common in patients who underwent inpatient CDR. It is believed that strict patient selection is important to optimize outcomes and safety of outpatient spine surgeries. 22 -25 However, despite this consensus, currently, there is no evidence-based guideline to help with patient selection.
The second reason that may account for the advantage of outpatient CDR is that the complication criteria varied among included studies. For instance, dysphagia was not considered as a complication in included studies except for the study by Chin et al. 17 Cuellar et al 19 included nausea and vomiting as postoperative complications. Therefore, standard complication criteria, such as the Clavien-Dindo classification, could help get more accurate results. Third, the definition of outpatient surgery may also influence the result of this study. Patients could be divided into either the outpatient group or the inpatient group depending on the definition of the study. For example, some patient may stay overnight in the hospital for postoperative monitoring if their surgeries were scheduled for later in the day, and they were still divided into the outpatient group in the study by Gornet et al, 16 but could be classified into the inpatient group according to the definition of Bovonratwet et al. 15
Although the above factors could affect the accuracy of the results, our study showed that the pooled prevalence of overall complication for outpatient CDR was very low (0.51%; 95% CI 0.10% to 1.13%). With proper patient selection, CDR can be performed safely in outpatient settings.
Except for surgical technique, anesthesiology, and patient selection, discharge criteria also could not be neglected. Mohandas et al 23 suggested that patients underwent outpatient cervical spine surgery should be evaluated with a discharge checklist or scale to determine if they can be safely discharged. However, in the included studies, only Chin et al 17 reported the discharge recommendations. In their cohort, patients received postoperative assessments by a multidisciplinary team, including surgeons, physicians, nurses, and anesthesiologists to ensure that patients are alert and neurologically intact, have no signs of swallowing and respiratory dysfunction, and are aware of the risk of serious complications after discharge. While these procedures may help guarantee patients’ safety, there is no evidence-based discharge criteria at present.
Typically, most life-threatening complications such as hematomas can be detected within 4 to 6 hours after surgery. 26 However, the fear of complications without prolonged monitoring in the hospital may be another barrier of transiting CDR into outpatient settings. 26 Nowadays, with advances in information technology and the development of the internet, remote monitoring and follow-up using smartphones are applied in the management of chronic diseases and ambulatory surgeries, which can provide a practical reference for postoperative monitoring after outpatient CDR. Unfortunately, only one relevant study in outpatient spine surgery has been reported so far. Debono et al 27 found that remote monitoring using a mobile application received high rates of satisfaction and acceptance in patients who underwent ambulatory lumbar discectomy. It is possible that in the foreseeable future, the remote monitoring with smartphones will become an integral part of outpatient CDR.
Our systematic review and meta-analysis indicate that level I or II studies are absent regarding the safety and efficacy of outpatient CDR. All studies included in the quantitative analysis were retrospective studies; therefore, the accuracy of our results may be affected. In addition, the patient selection criteria, complication criteria, and the definition of outpatient surgery differed among included studies, which may also have affected the accuracy of results and limited the generalizability of our findings. However, we strictly followed the PRISMA guidelines to improve the quality of our study. Further studies with prospective design and large sample size are needed to generate evidence-based protocols for patient selection and management.
Conclusion
There is a lack of level I or II studies on the safety of outpatient CDR. However, existing studies indicate that CDR can be safely conducted in outpatient settings, with lower complication rates, shorter operating time, and similar readmission and reoperation rates compared with inpatient CDR. With careful patient selection and proper postoperative management, outpatient CDR can be used to reduce costs and improve patient satisfaction. Further prospective studies with a large sample size are needed to generate evidence-based protocols for outpatient CDR and to demonstrate the generalizability of current results.
Supplemental Material
Supplemental Material, completed_PRISMA_checklist - Comparison of the Safety of Outpatient Cervical Disc Replacement With Inpatient Cervical Disc Replacement: A Systematic Review and Meta-Analysis
Supplemental Material, completed_PRISMA_checklist for Comparison of the Safety of Outpatient Cervical Disc Replacement With Inpatient Cervical Disc Replacement: A Systematic Review and Meta-Analysis by Xiaofei Wang, Yang Meng, Hao Liu, Ying Hong, Beiyu Wang, Chen Ding and Yi Yang in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Science and Technology Program of Sichuan Province, China (2018SZ0045); West China Nursing Discipline Development Special Fund Project, West China Hospital, Sichuan University (HXHL19016); Post-Doctor Research Project, West China Hospital, Sichuan University (2018HXBH002).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.