
Abstract
Study Design:
Prospective study.
Objectives:
To study the increasing divergence between targeted and achieved distractions observed with magnetically controlled growing rod (MCGR)lengthening, and the relationship of this reduced rate of achieved lengthening with remaining rod length.
Methods:
Patients with early onset scoliosis (EOS) who underwent MCGRs with minimum 2-year follow-up were consecutively enrolled. Targeted and achieved lengths were compared. Correlation between percentage of lengthening achieved from targeted length was identified with the timing of rod exchanges.
Results:
A total of 20 patients fulfilled the inclusion criteria. The mean age at index surgery was 9.5 years and mean postoperative follow-up was 68 ± 28 months. Of these, 8 patients had at least one rod exchange that occurred at 23 ± 4 months. A decrease in rate of achieved lengthening was observed when compared with targeted distractions. The achieved lengthening drops from 86% of targeted length at the first distraction to only 58.8% at the 21st distraction episode for the first set of rods. After rod exchange, the average achieved lengthening went back up to 81.3% of the targeted length but subsequently had a gradual reduction to 35% at the 19th distraction episode.
Conclusions:
We propose a “law of temporary diminishing distraction gains” that MCGR users should be aware of when monitoring rod lengthening. Diminishing distraction length gains is observed as the rod is lengthened and is a phenomenon independent of patient factors. It is only temporary as the rates of achieved lengthening returns to baseline after rod exchange.
Keywords
Introduction
Growing rods are a popular choice for managing early onset scoliosis (EOS) as it provides a minimally invasive nonfusion method of stabilizing the spine, which accommodates spinal lengthening to mimic spinal growth.1-3 Traditional growing rods (TGRs) have previously been the mainstay surgical option but require repeated manual distractions under general anesthesia and thus is associated with increased risks of anesthetic and wound complications.4-6 Since 2009, the development of magnetically controlled growing rods (MCGRs) have revolutionized EOS management. 7 The MCGR is lengthened via an external magnet thereby allowing outpatient awake distraction with continuous neurological monitoring. Consistent spinal lengthening and control of the spinal deformity is achievable7-14 and with its capacity for gradual correction, its indications have been extended to safe gradual correction of severe deformities.15,16 With more frequent distractions, increased radiation exposure can be avoided with ultrasound.17,18 As compared with TGRs, the MCGR is an overall less costly option for EOS with reduced surgical visits.19-21
A unique phenomenon observed from TGR is the “law of diminishing returns” whereby decreasing gains in spinal lengthening is observed and may occur as early as the first successive lengthening.22,23 This likely reflects the progressive stiffness of an immature spine with prolonged instrumentation in situ or autofusion as a result of trauma to spinal ligaments after forceful distractions at infrequent intervals. 23 Spontaneous fusion may also result from trauma to the spinal ligaments due to sudden and forceful distractions at infrequent intervals. Since MCGR allows for noninvasive lengthening, distractions may be performed more frequently and in small increments to avoid autofusion.
The short-term results with MCGRs contradicts in terms of diminishing returns and may be related to the large variations in distraction techniques and frequencies.9,12,24,25 There is apparent divergence observed between targeted (intended amount of lengthening input in the external remote controller) and achieved (actual length measured on radiographs or ultrasound) lengthening with increasing MCGR distraction.26,27 One interesting observation suggests that the reductions in lengthening is due to reduced distraction forces as the rod lengthens rather than internal spinal stiffness. This has been supported with a longer-term follow-up clinical study 11 and via biomechanical analysis. 28 The generated maximum force by the MCGR reduces as the rod is lengthened, which is a possible rationale for these transient reductions in distraction length gains. 28 Thus, the aim of this study was to determine the relationship of reduced achieved lengthening with remaining rod length, and whether such phenomena persists with rod exchange.
Patients and Methods
Subjects
This was a prospective study of consecutive patients with EOS who underwent primary dual MCGRs. All patients were consecutively enrolled between December 2009 to May 2017 and had minimum 2-year follow-up. Patients were excluded if they had prior spinal surgery such as traditional growing rods, which may reduce the likelihood of the spine to lengthen, and any complications that required early removal of the rod such as deep wound infection. Ethics was approved by the local institutional review board (UW 16-336).
Patients who were eligible for MCGRs were patients with EOS (diagnosis <10 years of age) with major curve Cobb angles >50°. Standard implantation of MCGRs was performed without any additional intraoperative rod distraction attempted beyond just achieving spinal balance. All dual MCGRs were of 5.5 mm in diameter and were placed in a standard and offset configuration. All patients underwent monthly 2 mm distractions to both rods starting at 2 months after MCGR implantation. This is a protocol utilized in previous studies.11,12 Each distraction aimed at 2 mm on the concave side rod then the convex side rod. Three experienced surgeons performed all surgeries and managed all distraction clinics. Radiographs were obtained every 6 months for assessment of the spinal deformity and to identify any rod-related complications. Ultrasound was used to monitor successful distractions at each monthly distraction. This ultrasonographer was independent and performed all measurements and is blinded to the distraction procedure. Pre- and postdistraction assessment was performed at each distraction. The ultrasonographer performed 3 measurements of each reading and the average was taken for recording. Standard measurement was made at the distal extendable portion of the rod. 17 In the case of a failed successful distraction observed by the ultrasound, alternate distracting technique with smaller intervals or repositioning the patient such as sitting would be performed.
Study Parameters
Demographic data included patient gender, age at MCGR implantation, and diagnosis (congenital, neuromuscular, syndromic, idiopathic). The targeted and achieved lengths (mm) of the right and left rods were recorded via the input in the external remote controller and the measurement of the extended portion of the MCGR by ultrasound. 17 Ultrasound has been validated to be as accurate as radiographs.17,18 The differences between targeted and achieved lengthening per rod per distraction episode were also recorded.
Distraction Problems and Complications
Whether any rod slippage/rod stalling occurred were also noted. Rod slippage indicates a slippage of the magnetic mechanism and presents with a clunking sound or feeling during the distraction. If rod slippage occurs, other distraction techniques such as single magnet distraction, alternate distraction between rods by smaller amounts (ie, 0.5 mm) or alternative patient positioning would be adopted to reach the same intended 2 mm expected lengthening. Any rod exchanges and timing of rod exchanges were also recorded. Rod exchanges were considered when rods are lengthened to maximum 48 mm, unable to distract despite height gain in at least 2 successive distraction episodes despite positional changes, and if complications such as rod fracture and implant dislodgement precluding further distractions occurred.
Statistical Analysis
Measurements of left and right rods were combined in statistical analysis. Descriptive statistics were calculated as means, standard deviations (SD), and percentages. Comparison between different time points (preimplantation, immediately after implantation, last distraction episode, and immediately after rod exchange or definitive procedure) were tested using analysis of variance (ANOVA). A P value of <.05 was considered to be statistically significant. Correlation (R2) between percentage of lengthening achieved from targeted length was identified, as well as its relationship with timing of rod exchanges. Charts were created by Microsoft Excel (Microsoft Corp).
Results
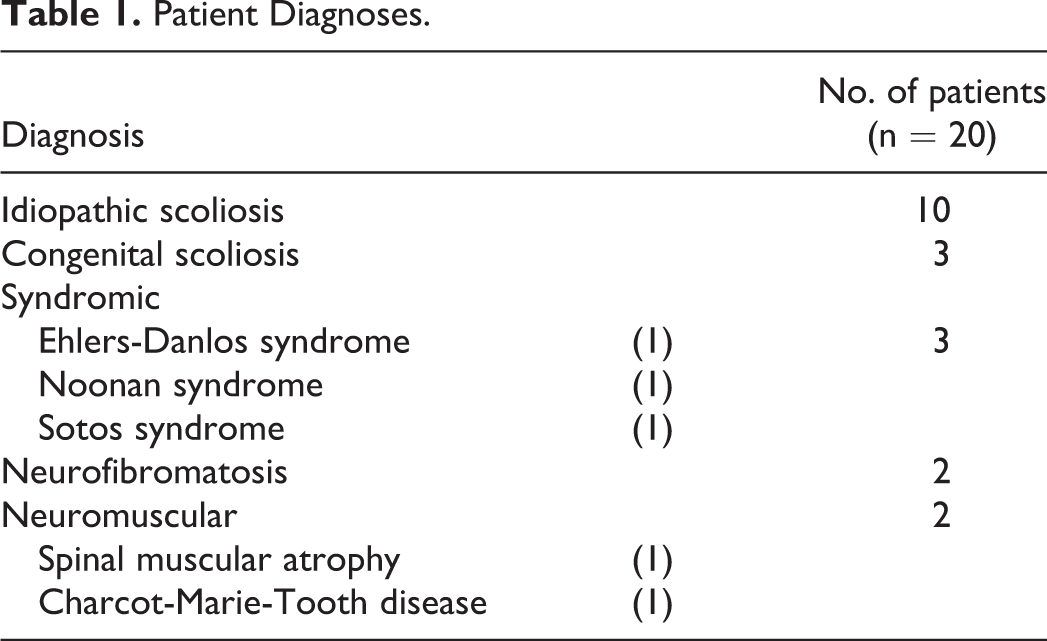
A total of 20 patients (male 5; female 15) were included in the study. Their diagnoses are listed in Table 1. All patients had primary dual rods inserted and did not experience any complications such as infection, rod fractures, housing pin dislodgement, or implant dislodgement that required early removal of the rods. The mean age at index surgery was 9.5 ± 3.4 years (range: 4.1-14.8 years) and mean postoperative follow-up was 68 ± 28 months (range: 24-115 months). There was a mean of 27 ± 9 (range: 14-41) total distraction procedures. Half of the patients (n = 10) reached skeletal maturity before exchange of rods and underwent fusion surgery. The remaining 10 patients had at least one rod exchange, which occurred at 23 ± 4 (17-28) months. None of the rod exchanges were due to complications such as housing pin and rod fracture, or proximal junctional kyphosis. However, not all rods were able to distract till full 48 mm (maximum lengthening allowed by the MCGR) as the mean distracted length before rod exchange was 34.8 ± 6.2 mm. The mean Cobb angle before surgery was 56.5° ± 7.4°. The greatest correction of the curve was achieved immediately after rod implantation (24.8° ± 8.6°) and maintained throughout the follow-up period (Table 2). Gradual increases were observed for height measurements and instrumentation length.
Patient Diagnoses.
Changes in Parameters With Major Events.
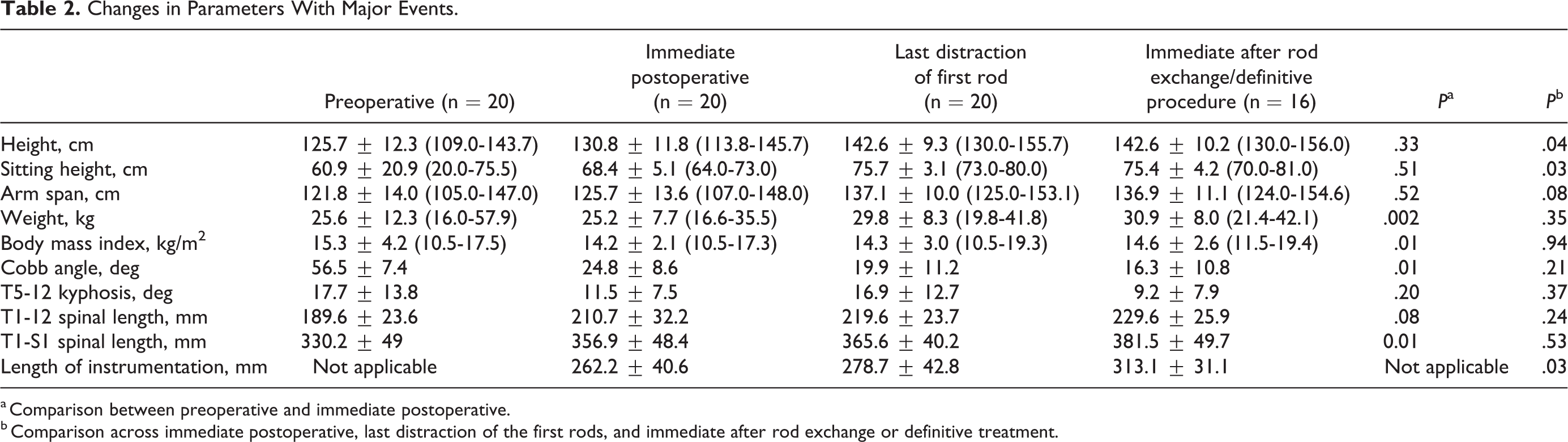
a Comparison between preoperative and immediate postoperative.
b Comparison across immediate postoperative, last distraction of the first rods, and immediate after rod exchange or definitive treatment.
A decrease in rate of achieved lengthening was observed when compared with targeted distractions. The actual distraction lengths deviated from the targeted lengths by an average of −0.14 ± 0.38 mm at the first distraction episode. This deviation then gradually increased to −0.9 ± 0.82 mm at the last distraction of the first pair of rods. After rod exchange, the deviation restored back to −0.5 ± 0.58 mm but increased more aggressively than the first rod to −1.2 ± 0.25 mm, as many patients needed repeated distraction at the end of the follow-up period (Figure 1). When presented in percentages of lengthening achieved from targeted length (Figure 2), the rates dropped from achieving 86% of targeted length for the right and left rods combined at the first distraction to only 55.2% of targeted length at the 19th distraction episode. The rates returned to 81.3% at the first distraction after rod exchange and decreased to 35% at the 19th distraction episode after rod exchange.
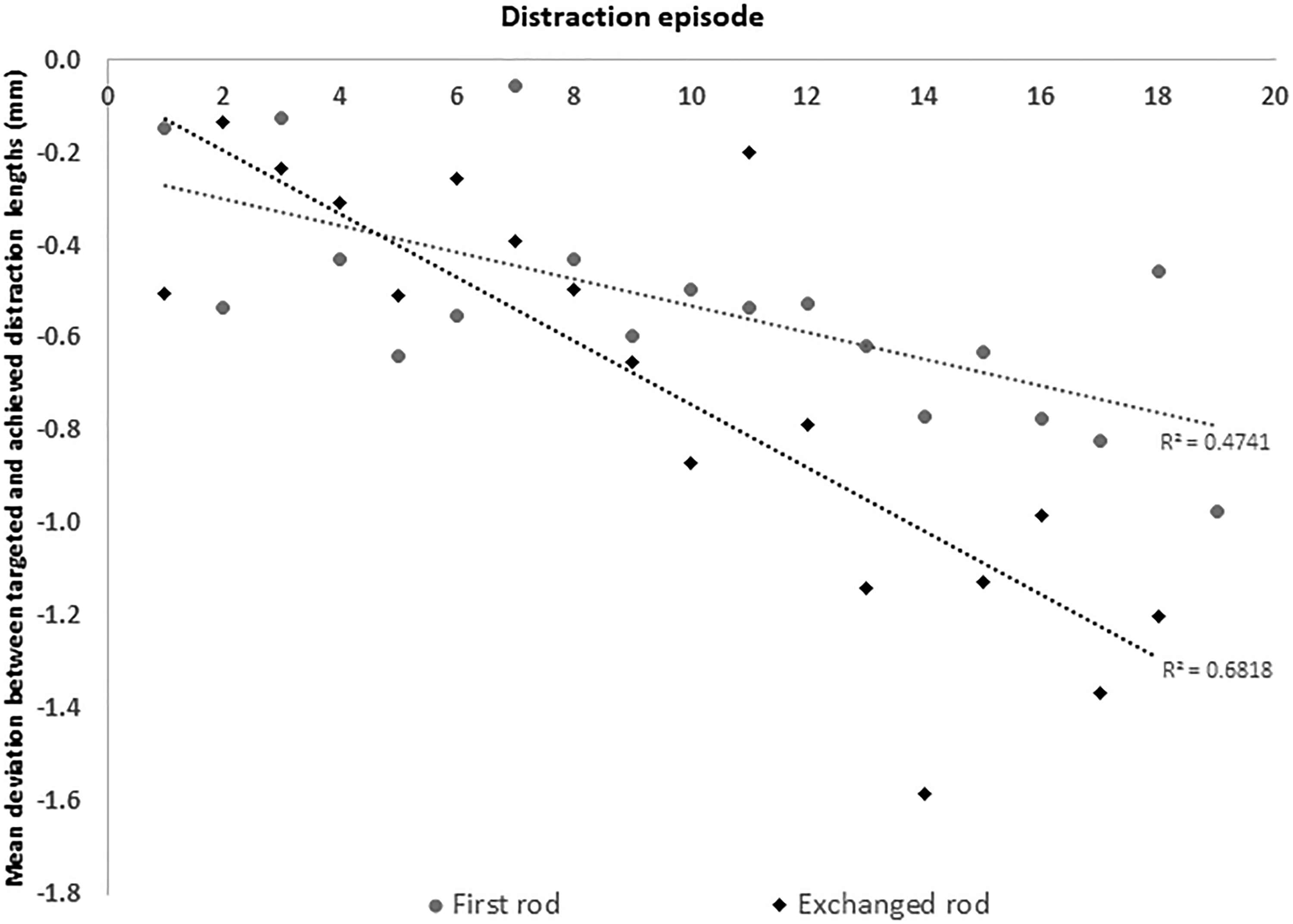
Mean deviation between targeted and achieved distraction lengths.
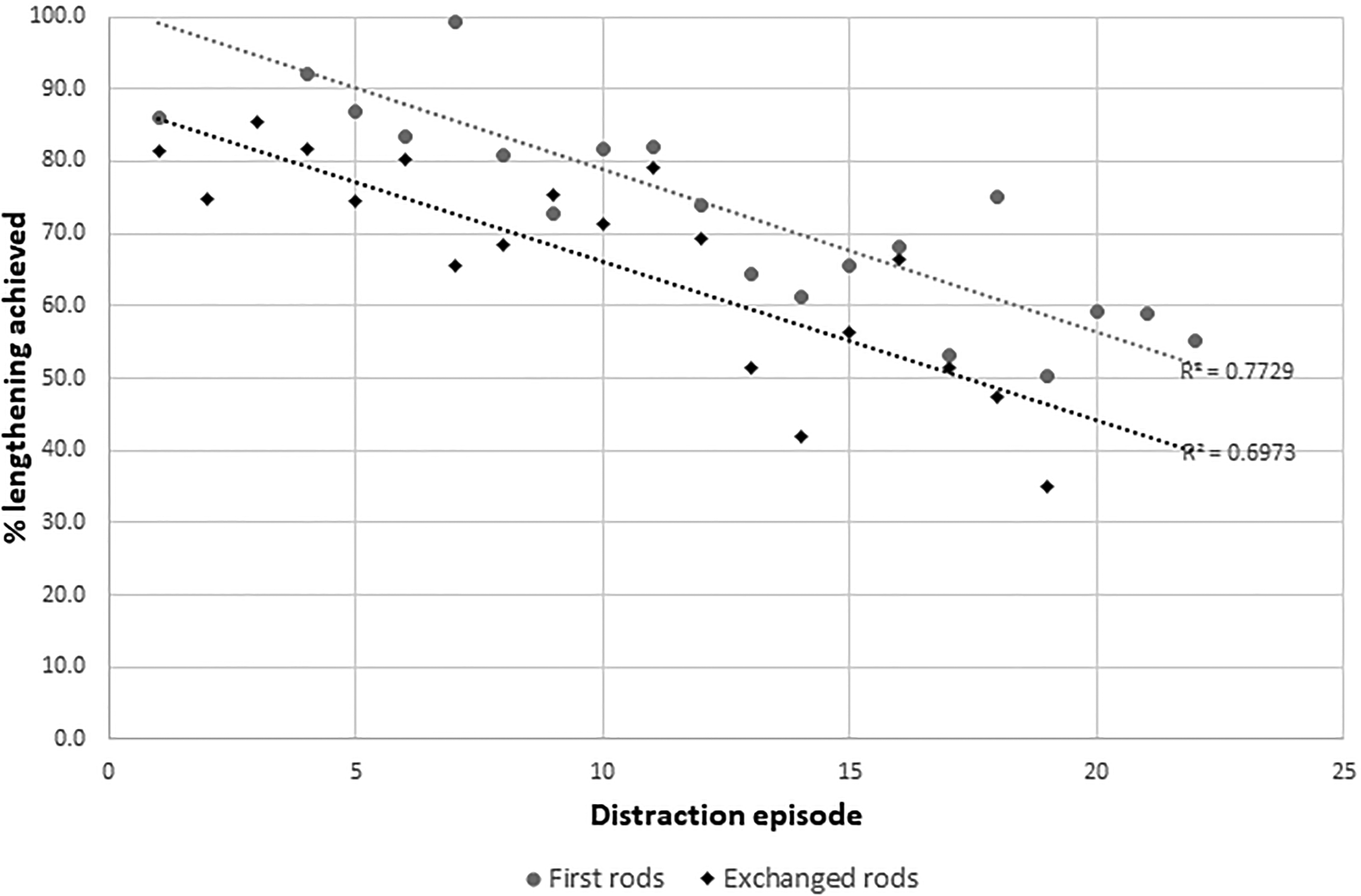
Percentage of lengthening achieved from targeted length.
Discussion
MCGR provides benefits of noninvasive outpatient lengthening and thus allows for more frequent distractions with smaller lengthening increments. This may avoid the autofusion events seen with TGR that is associated with poor lengthening outcomes. However, poor lengthening outcomes is not unique to TGR. Target and achieved lengthening mismatch is a well-recognized problem with MCGR. 29 Despite our intention to achieve consistent spinal length gains, there are inherent restrictions that inhibit the distraction procedure. Our study highlights the relationship between this divergence with the amount of rod length remaining. We observed increasing mismatches between targeted and achieved lengthening as the rod is lengthened. After rod exchange, the targeted and achieved lengthening deviance reduced to what was observed after initial rod implantation. This signifies an issue specifically related to the rod rather than spine or soft tissue factors.
It is important to first clarify the jargon of reduced lengthening. The “law of diminishing gains” as coined by Sankar et al 23 refers to reductions in T1-S1 spine length, which is probably not the most accurate measure for assessing diminishing distraction returns by the MCGR. It is unlikely for the entire spinal column to be instrumented and T1-S1 increases are proportional to growth potential rather than what is achievable through rod distraction. In addition, T1-S1 is influenced heavily by the Cobb angle. Hence reductions in T1-S1 gain may simply indicate curve progression rather than inability for the rod to distract as well. It is understandable to measure the spinal length instead for TGRs as there are no consistent landmarks on the rod for monitoring the distracted length. However, there are easily recognizable contours along the MCGR for accurate measurements on plain radiographs or ultrasound. Such measurements have been reported to be very accurate.17,25 As seen from our results, instrumentation length gains were consistent with height gains throughout treatment while T1-T12 and T1-S1 spinal length did not reflect growth as consistently. Coronal spinal length measurements are thus inherently unreliable and alternatives such as sagittal spine length measurements may be preferable. 30 Thus, “law of temporary diminishing distraction gains” may be a more appropriate term to use for describing such reductions in MCGR lengthening observed here and in past studies.11,12,24,25
The interesting feature of the “law of temporary diminishing distraction gains” is that it is a phenomenon unique only to the currently implanted rod under distraction. The gradual reductions of rod lengthening illustrated by increasing divergence between targeted and achieved length gains is only temporary. With an exchange to a new rod, the ease of length gains returns to the baseline initial rod implanted. The divergence reverts to minimal but reoccurs at a similar timing (19th distraction) after a similar amount of rod lengthening has been achieved. This suggests that diminishing distraction gains are a result of rod factors rather than patient factors. This is supported by a recent biomechanical study on the maximum force output by the MCGR. Poon et al 28 showed that by using a straight MCGR, the maximum force created was 46.8 lbs at 0 mm of actuator lengthening, 44.9 lbs at 25 mm of expansion and 43.2 lbs at 40 mm of lengthening. There is a decrease in maximal force generated as the rod is lengthened suggesting internal biomechanical issues with the MCGR leading to these transient reductions in distraction length gains. However, this decline was observed only in straight rods. It is likely bent rods may show a more significant decline. Further biomechanical studies are necessary to understand this phenomenon further.
Identifying the reason for this mechanical issue is important to improve the design or utility of the MCGR. Rod slippage is a potential cause as they coincide with these lengthening reductions and mismatches between targeted and achieved lengthening. 12 This slippage of the distraction mechanism causes a “clunking” sound and feeling during distractions and represent an inability of distraction forces to overcome internal tissue stiffness. Several risk factors for rod slippage have been proposed including increased body habitus and reduced distance between internal magnets. 12 Rod slippage may be considered as a safety mechanism to avoid forceful distractions beyond which the spine can tolerate and potential implant failure or spinal injury. However, we postulate that persistent rod slippage may not be conducive to the current MCGR design. 31 Anecdotally, if we continuously drive the internal magnet despite rod slippage, we may be inducing mechanical wearing of the device. The O-ring seal failure (junction where the MCGR is extended) and metallosis have been reported and may be related to these slippage events.32,33 However, this is only a postulation and the relationship between rod slippage and metallosis events require further study. 34 In cases of continuous rod slippage and reduced length gains despite spacing out distractions and positive height gain, earlier rod exchange before the rod is completely lengthened may be indicated. The MCGR is likely nonfunctional and lengthening to a full 48 mm is doubtful. There are other considerations such as additional surgery or implant costs. However, maintaining consistent rod lengthening is paramount to the success of growing rod surgery. Our overall results with curve correction and overall spine gains are similar to that of previous reports.11,35 Patients generally do not experience significant curve progression with distractions but in these patients with significant growth potential, consistent spine lengthening is important and is represented by a consistently distractable growing rod. Furthermore, as we do not know the long-term implications of metallosis, we should try to avoid it if possible.
The limitation of this study is the relatively small sample size and heterogenous population. This is the inherent problem of most EOS studies. Some disorders such as Noonan syndrome may growth disproportionately less than idiopathic patients and should be compared in future study. Only half of our total cohort had rod exchanges and hence our findings require validation in larger populations. Utilization of larger multicenter databases may be helpful but only if the treatment method is consistent with standardized data collection. We adopted a standardized monthly distraction protocol with 2 mm targeted distraction per episode and our findings are relevant only to MCGR users who similarly distract as frequently. Whether these findings are applicable to users who distract on 3- or 6-monthly basis will require further study. Further understanding of why these diminishing distraction gains occur and changes that occur in the device is necessary. This may require tests in an experimental environment with repetitive loading in a rod with wear. It is also important to note that the trend of lengthening deviation is more rapid after rod exchange. Whether this persists in further rod exchanges should be determined at longer follow-up.
This study illustrates an interesting phenomenon whereby temporary diminishing distraction gains are observed as the MCGR is lengthened. The smoothness of the distraction procedure returns to baseline after a rod exchange. The original description of the “law of diminishing returns” is only applicable to TGR with regards to T1-S1 length gain. We propose a “Law of Temporary Diminishing Distraction Gains” with the MCGR that users should be aware of when monitoring their distractions. This may be a limitation within the current rod design that requires further examination. Nevertheless, we have shown that these events are caused by rod issues that are largely independent of patient factors. Earlier rod exchange before maximum lengthening may be indicated if there are difficulties in distraction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.