
Abstract
Study Design:
Retrospective cohort study.
Objectives:
The identification of case types and institutional factors associated with reduced length of stay (LOS) is a key initial step to inform the creation of clinical care pathways that can assist hospitals to maximize the benefit of value-based payment models. The objective of this study was to identify preoperative, intraoperative, and postoperative factors associated with shorter than expected LOS after adult spinal deformity (ASD) surgery.
Methods:
A retrospective cohort study was performed of 82 patients with ASD who underwent ≥5 levels of fusion to the pelvis between 2013 and 2018. A LOS <6 days was determined as a basis for comparison, as 5.7 days was the “expected LOS” generated through Poisson regression modeling of the sample. Clinical, radiographic, surgical, and postoperative factors were compared between those staying ≥6 days (L group) and <6 days (S group). Logistic regression was used to identify factors associated with LOS <6 days.
Results:
A total of 35 patients were in group S (42.7%). Gender, age, body mass index, ASA (American Society of Anesthesiologists) class, and use of preoperative narcotics, revision surgery, day of admission, and surgical complications did not vary between the cohorts (P > .05). Mild-moderate preoperative sagittal deformity (sagittal Schwab modifiers 0 or +), lower estimated blood loss (<1200 mL), fewer levels fused (7 vs 10 levels), shorter operating room time, procedure end time before 15:00, and no intensive care unit stay, were associated with short LOS (P < .05). Only 1 major medical complication occurred in the short LOS group (P < .05).
Conclusions:
This study identifies the ASD “case phenotype,” intra-, and postoperative benchmarks associated with shorter LOS, providing targets for pathways designed to reduce LOS.
Introduction
Surgical intervention is effective in improving spine-related health quality in adult patients with symptomatic adult spinal deformity (ASD). 1 However, as nationwide health care expenditures grow, the value of any intervention becomes increasingly important. Payers incentivize providers to improve quality while minimizing expenditures through value-based payment models, such as bundled care payments. 2 Multidisciplinary patient risk-stratification, predictive decision-making assistance, and innovative resource allocation have formed the key provider-based initiatives to reduce overall spine-related costs at spine “centers of excellence.” 3 For an individual patient care episode, costs are driven by the length of hospitalization, readmissions, and postdischarge rehabilitation use. 4,5 The high cost of complex spinal deformity surgery is one barrier to improving its value. A recent cost-effectiveness study estimated the cost of the initial deformity surgery and hospitalization at $120 000, which is over 90% of the 2-year cost associated with the intervention. 6
Clinical care pathways have been shown to improve surgical outcomes and decrease costs, allowing institutions to maximize financial incentives while ensuring high-quality care for patients. 3,7 -11 While these pathways have led to improvements in many patient outcomes, reductions in length of stay are less consistent. 10,12 -14 Length of stay (LOS) has been implicated as a key determinant in the cost complex spine surgery. 4,5 Given the contribution of LOS to the total cost of spine deformity surgery, reduction of LOS should be a priority of clinical care pathways. The design of a pathway targeted at LOS reduction relies on the identification of modifiable factors associated with short LOS. However, while past literature has identified patients at risk for extended LOS, there is little research on determinants of short LOS after ASD surgery. Given that most studies have defined extended LOS as either >75th percentile or an arbitrary value of greater than 5 days, 15 -18 historically identified factors may not be applicable to the creation of expedited care pathways. Furthermore, very few studies have reported on the relationship between LOS and process components of the hospital course, such as mobilization protocols or the intraoperative details of surgery (such as blood loss, length of surgery, or levels of fusion), modifiable factors that show promise in reducing LOS. 19
While multicenter databases may generate several variables associated with a shorter LOS, the center-to-center heterogeneity in surgical technique, approach, perioperative care, and administrative processes, can make it difficult to generalize conclusions into an institution-specific intervention. Successful clinical care pathways have targeted center-specific processes in order to achieve desired outcomes. 7,20 Thus, the purpose of this study was to identify pre-, intra-, and postoperative factors associated with shorter than expected length of stay after ASD surgery, to provide targets for future expedited care pathways aimed at decreasing LOS.
Materials and Methods
Patient Sample
Following approval by the institutional review board, a retrospective chart review was performed of all adult patients (age ≥18 years) with a diagnosis of adult spinal deformity who had undergone 5 or more levels of fusion to the pelvis by either of 2 senior authors between 2013 and 2018 (primary or revision cases). Exclusion criteria included patients with skeletal dysplasia, neuromuscular, postinfectious, or traumatic deformities and those with incomplete records.
Perioperative care protocols were the same throughout the study period with no purposeful changes made to decrease LOS. Preoperatively, patients were evaluated at a medical screening clinic in order to ensure optimization before the procedure. Those with preoperative narcotic utilization were referred for additional management by a specialized pain team. 21 In addition to medical screening, patients attended a preoperative education class and visited a case manager before the day of surgery. 20 Intraoperatively, all patients underwent a single-stage, posterior-only approach, with the assistance of a private physician assistant or spine surgery fellow. Neuromonitoring was used universally. Postoperatively, patients were discharged to the intensive care unit (ICU) or postanesthesia care unit (PACU) at the discretion of the anesthesiologist. Postoperatively, all patients were placed on patient-controlled-analgesia (PCA), managed by a specialized acute pain team, who wean the PCA and administer adjunct analgesics (eg, acetaminophen, gabapentin) if deemed clinically useful by the attending anesthesiologist. Thus, other than avoidance of non-steroidal anti-inflammatories, pain management was at the discretion of the acute care team. Patients were followed postoperatively by one of several medical physicians specializing in perioperative care and were mobilized by physical therapy, usually starting postoperative day (POD) 1, and discharged to home or a rehab once deemed appropriate by all members of the care team.
The primary outcome of interest—inpatient hospital LOS—was defined as the number of days between the date of discharge and date of admission. The electronic medical records, physical patient charts, and operative records were reviewed for multiple variables with a possible effect on LOS. Preoperative factors included age, gender, body mass index in kg/m 2 (BMI), American Society of Anesthesiologists (ASA) class, surgical indication/diagnosis, primary versus revision surgery, chronic opioid use before surgery, and day of the week of admission. Intraoperative factors included procedure length (skin incision to closure, measured in hours), time of day out of the operating room, estimated blood loss (EBL), admission to ICU versus standard PACU, number of levels fused, number of 3-column osteotomies, number of Smith-Peterson osteotomies (grade 2 Schwab), and use of an interbody fusion (IBF). Postoperative factors included total number of postoperative transfusion episodes (ie, number of separate occasions patient underwent a blood transfusion postoperatively), postoperative day of ambulation, intraoperative surgical complications, inpatient surgical and medical complications, and discharge destination (home vs rehabilitation facility). Sagittal alignment parameters were collected from full-length standing radiographs.
Statistical Analysis
While past studies have utilized the mean or an arbitrarily defined percentile to categorize hospital LOS, we elected to utilize predictive modeling to generate a more accurate estimate of the “expected” LOS for our sample. Poisson regression modeling is a statistical method which can predict the probability of a certain outcome per dependent unit variable. In contrast to binomial distributions, which are utilized when the outcome variable is dichotomous, Poisson distributions are utilized when the outcome is a count variable (ie, number of days in the hospital). Thus, using Poisson regression modeling, the most probable length of stay per patient was calculated, generating an average expected LOS of 5.7 days for our single-center patient sample. Accordingly, a LOS of <6 days was determined as the basis for comparison, and the cohort was then split into 2 groups, defined as the “short stay” and “long stay” groups. Demographic, clinical, and radiographic parameters were then compared between the 2 cohorts to identify factors associated with short length of stay. Categorical variables were compared using chi-square or Fisher’s exact when appropriate. Continuous variables were analyzed for normality and compared using either Student’s t test or Wilcoxon rank-sum tests as appropriate. Linear regression was used to generate odds ratios for each factor, with length of stay as the outcome of interest. A P value of <.05 was chosen as the type 1 error rate for all tests. Statistical analyses were performed using Stata SE 14.0 (StataCorp).
Results
A total of 102 patients were eligible for review, 20 were excluded based on the exclusion criteria above, leaving 82 available for analysis. Based on an expected length of stay of 5.7 days (as generated by the regression model), 35 patients (43%) were assigned to the short stay cohort and 47 (57%) to the long stay cohort. Average LOS was 6.5 ± 3.2 days overall for the entire patient sample (range 2-23, short stay 4.2 ± 0.92, long stay 8.3 ± 3.2). No preoperative clinical factor, including age, gender, BMI, ASA class, preoperative opioid use, or day of surgery was found to be associated with shorter length of stay (P > .05) (Table 1). In the short stay cohort, 11 patients (39.3%) were greater than 70 years old, compared with 17 (36.2%) in the long stay cohort (P = .654). Year of surgery was also similar between the 2 cohorts (mean, short stay 2016 ± 1.3 vs long stay 2016 ± 1.4, P = .167).
Clinical Factors.
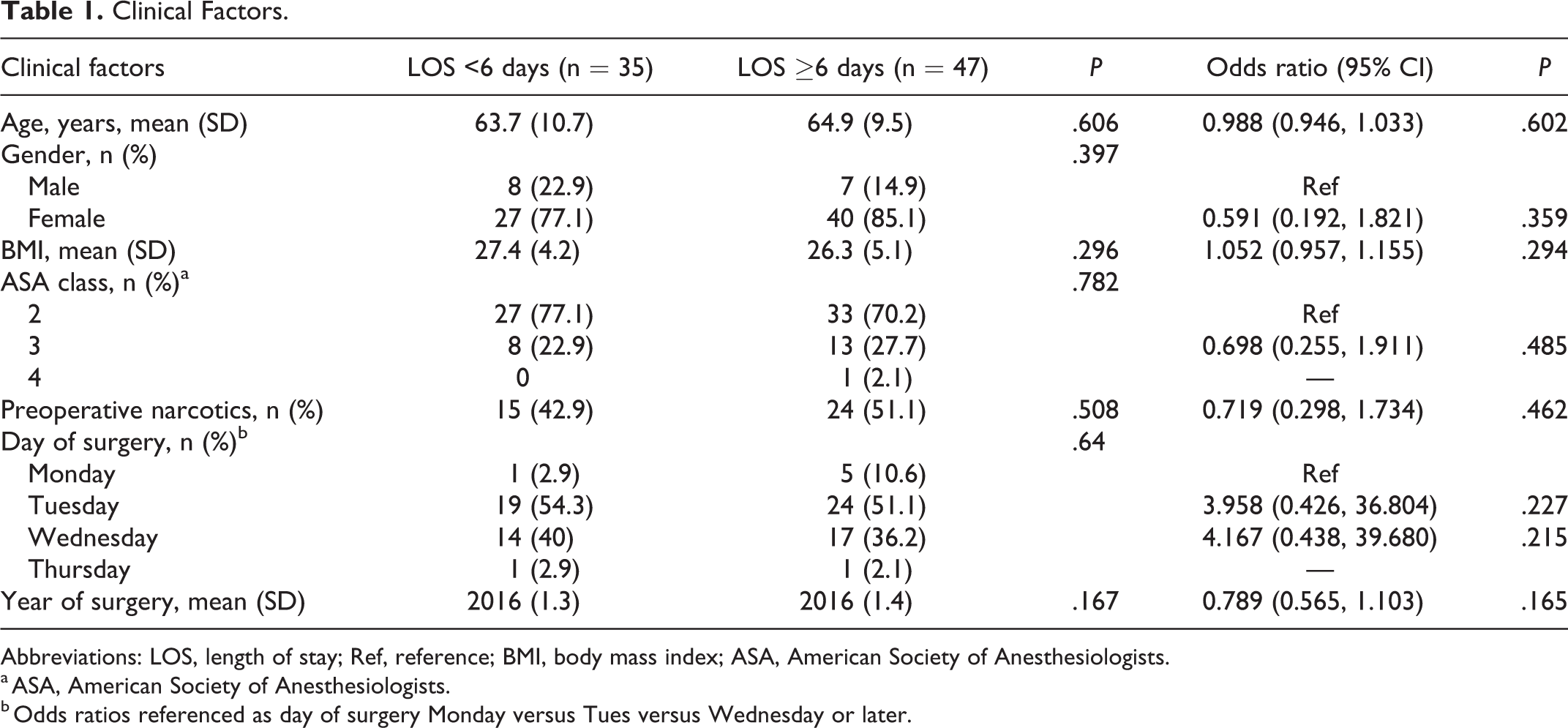
Abbreviations: LOS, length of stay; Ref, reference; BMI, body mass index; ASA, American Society of Anesthesiologists.
a ASA, American Society of Anesthesiologists.
b Odds ratios referenced as day of surgery Monday versus Tues versus Wednesday or later.
Multiple intraoperative factors were associated with short LOS (Table 2), including EBL (1141 ± 693 short stay vs 1580 ± 1168 mL long stay, P = .051). In univariate regression, patients with an EBL of >1200 mL were over 3 times as likely to have a long stay (odds ratio [OR] 3.20, 95% confidence interval [CI] 1.28-7.97, P = .013). Operating time was also associated with LOS (4.8 ± 1.4 short stay vs 5.5 ± 1.3 hours long stay, P = .024). Similarly, patients who left the operating room before 15:00 were more likely to be in the short stay group (57.1% short stay vs 34% long stay, OR 0.39, 95% CI 0.16-0.95, P = .039). Significant differences between cohorts were found with regards to the number of levels fused (7 [interquartile range IQR 6-8] short stay vs. 10 [IQR 8-15], P < .001) and number of Smith-Peterson osteotomies (1 [IQR 0-3] short stay vs 2 [IQR 1-4], P = .014). The use of a 3-column osteotomy was not significantly associated with length of stay (14.3% short stay vs 23.4% long stay, P = .402).
Intra- and Postoperative Factors.
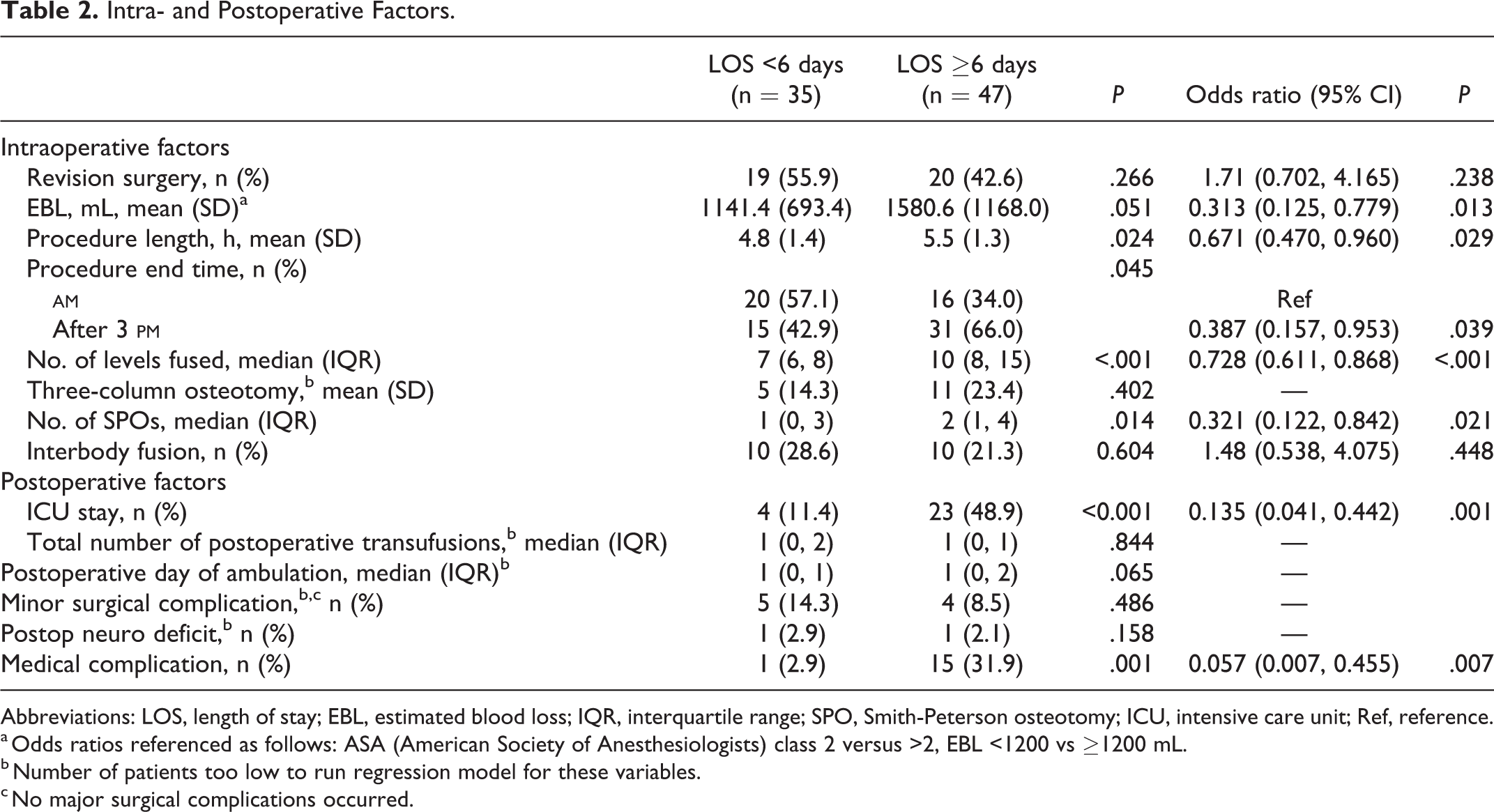
Abbreviations: LOS, length of stay; EBL, estimated blood loss; IQR, interquartile range; SPO, Smith-Peterson osteotomy; ICU, intensive care unit; Ref, reference.
a Odds ratios referenced as follows: ASA (American Society of Anesthesiologists) class 2 versus >2, EBL <1200 vs ≥1200 mL.
b Number of patients too low to run regression model for these variables.
c No major surgical complications occurred.
Patients in the short stay cohort had a milder degree of sagittal deformity, as measured on preoperative lateral radiographs (Table 3). The mean T1 pelvic angle was lower in the short stay cohort (T1PA) (21.4° ± 10.4° vs 28.5° ± 12.8°, P = .009) and the short stay group also had a lower mean C7 sagittal-vertebral axis (49.9 ± 59.6 vs 97.0 ± 77.9 mm, P = .004).
Radiographic Parameters.
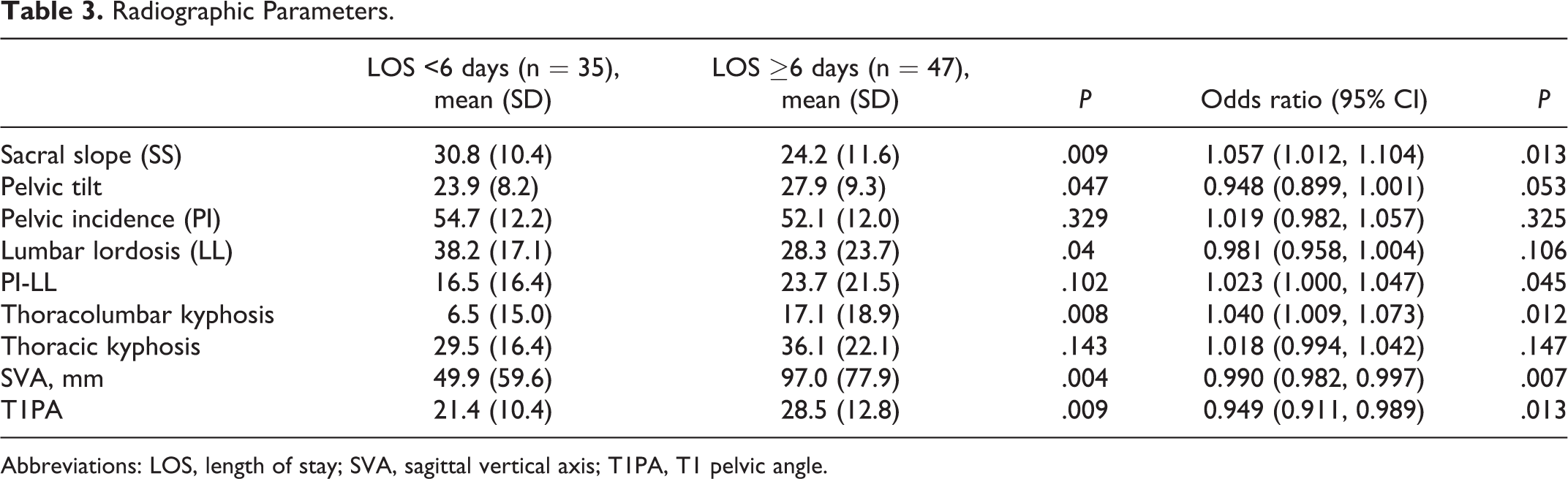
Abbreviations: LOS, length of stay; SVA, sagittal vertical axis; T1PA, T1 pelvic angle.
Postoperative factors associated with LOS were related to the patient’s medical recovery (Table 2). Patients admitted to the ICU postoperatively were more likely to have a long LOS (OR 7.42, 95% CI 2.26-24.37, P = .001). Fifteen patients (31.9%) in the long stay cohort had 1 or more medical complication, compared with 1 patient (2.9%) in the short stay cohort (P = .001). Medical complications were as follows: ileus (n = 4), pleural effusion (n = 4), pulmonary emboli (n = 5), new arrhythmias (n = 3), urinary tract infections (n = 2), pneumonia (n = 2), and sepsis (n = 1). However, surgical complications (all dural tears) were seen at similar rates (5 patients [14.3%] short stay vs 4 [8.5%] long stay, P = .486). Two new neurologic deficits occurred (1 [2.9%] short stay vs 1 [2.1%] long stay, P = 1.000). Median day of ambulation was POD 1 in the short stay group (IQR 0-1) and POD 1 in the long stay group (IQR 0-2) (P = .065). The total number of postoperative transfusions was not associated with LOS (short stay, 1 [IQR 0-1] vs long stay, 1 [IQR 0-2], P > .05).
Discussion
The average length of stay in our single-institution sample was comparable to past reports. 15,16,19 In a multicenter sample of 380 patients undergoing ASD surgery, Klineberg et al 16 reported an average LOS of 7.8 ± 3.8 days, just slightly longer than our average of 6.5 ± 3.2. Adogwa et al 19 compared early to late ambulators in a cohort of 125 patients who underwent ASD surgery (no minimum number of fusion levels), finding an average LOS of 5.3 ± 3.0 and 8.1 ± 7.7 days, respectively. In a Danish cohort, notably a health care system with an alternate payment model, the mean LOS was 10.1 ± 7.6 days (median 8 days). 15 However, our basis of comparison was the “expected LOS” as modeled by Poisson regression (5.7 days). The expected LOS was lower than the average LOS, as would be predicted when accounting for unpredictable postoperative events, such as complications or rehabilitation bed availability delays. Of note, this expected LOS was institution-specific, based on the cases seen at our center and may not be generalizable to other centers with different care protocols, patient populations, or payer mixes.
Our findings offer important insight into the importance of preoperative risk-stratification for expedited care pathways aimed at reduced LOS (Figure 1). While advanced age has been demonstrated as a risk factor for extended LOS in the past, 16,18 our study did not find that younger age was associated with reduced LOS. The definition of “extended LOS” may also explain this deviation from previous research. For example, though Kim et al 18 specifically examined age as a risk factor for complications after ASD surgery, extended LOS was arbitrarily defined as >5 days—which would have qualified as “short LOS” in our sample. Health status is likely more influential to the patient’s LOS through its relationship to medical complications. While both cohorts were relatively healthy (77.1% ASA class II short stay vs 70.2% long stay, P = .782), the long stay cohort had a much higher rate of postoperative medical complications (as expected). Surprisingly, preoperative opioid use was also not associated with short stay. Notably, our institution employs a specialized perioperative pain team for these patients, which was likely why preoperative narcotic use did not affect length of stay in our study. 21 In summary, given that our center already employs the preoperative elements key to many clinical care pathways (enhanced medical screening, patient education, and preoperative pain planning), it is likely that preoperative risk factors were anticipated appropriately by the medical teams, explaining the lack of association with LOS in our analysis. Our findings support that preoperative screening, patient education, and pain planning are essential for any expedited care pathway, especially one designed to reduce LOS.
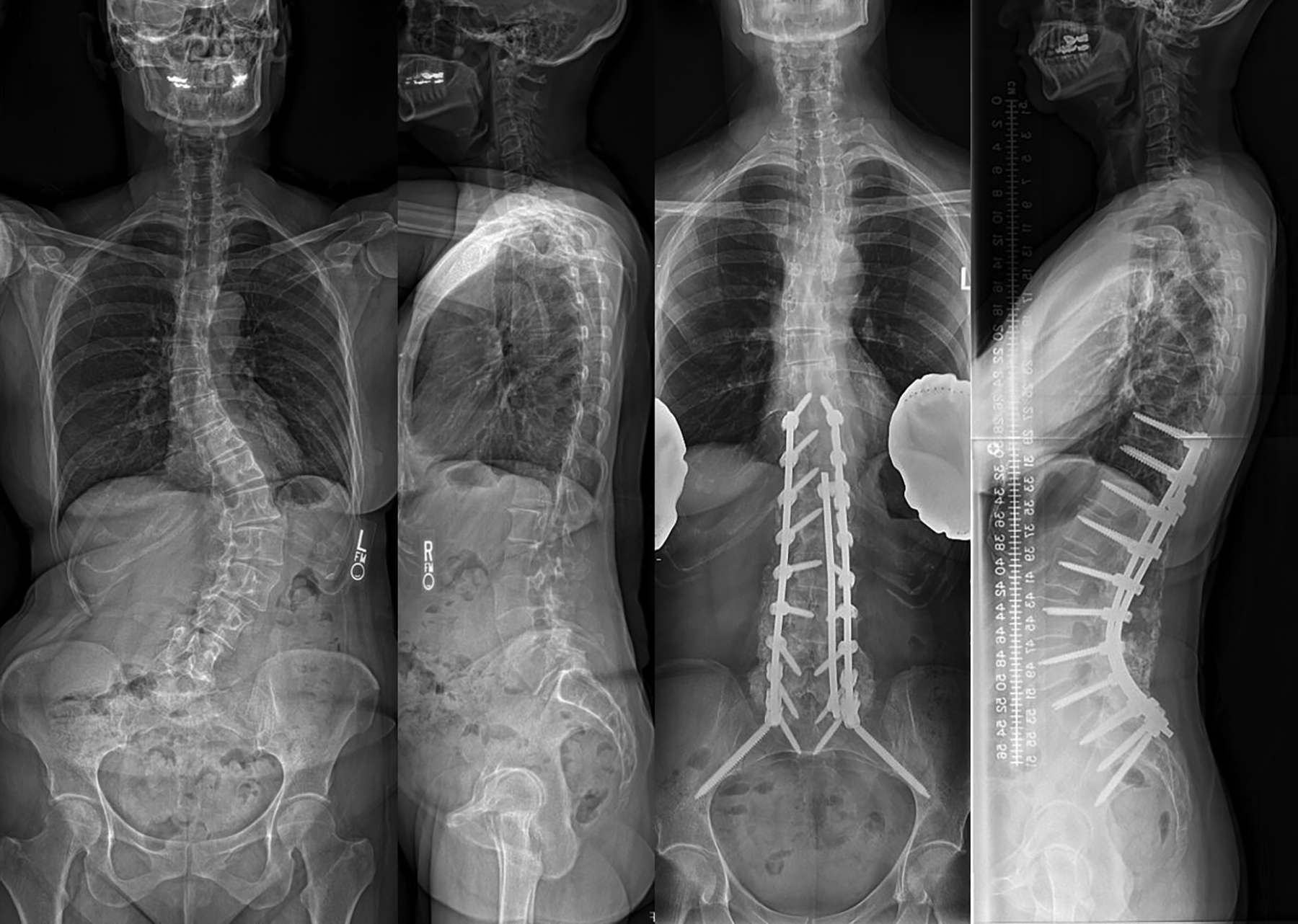
Case example of patient/case “phenotype” that may be eligible for a short-stay adult deformity pathway. A 52-year-old woman with a 2-year history of progressive lower back pain radiating into the left buttock. Medical history significant for osteoporosis and intermittent supraventricular tachycardia. The patient underwent T10-pelvis posterior spinal fusion with Smith-Peterson osteotomies performed from L1-L5. Total operative time was 3 hours and 27 minutes, and the case ended at 17:00. The patient spent the first postoperative night in the post-anesthesia care unit and was transferred to floor on postoperative day (POD) 1. She walked 5 feet with physical therapy on POD 1. On POD 3, the patient was transfused 1 unit of packed red blood cells for anemia due to acute blood loss. The patient walked 150 feet on POD 3 and was discharged home on the morning of POD 5.
As would be expected, our data show that the degree of deformity and invasiveness of planned surgery correlated with LOS. Furthermore, the variation in LOS was much larger in the long-stay cohort (SD 3.2 days vs SD 0.9 days). These findings suggest that there is a certain “case phenotype” that may be appropriate for expedited-care pathways (Figure 1). A large number of levels fused and extensive osteotomies have been implicated as risk factors for extended LOS and complications in past literature. 16,22 Our data corroborates these findings, as short-stay patients had a median of 7 levels fused (10 in long-stay cohort, P < .001) and fewer Smith-Peterson osteotomies. While the difference in 3-column osteotomies (3COs) was not significant between the cohorts, this was likely underpowered given the small number of 3COs performed in the short-stay cohort (5 [14.3%] vs 11 [23.4%], P = .402). As a correlate, the degree of deformity (as measured by sagittal vertical axis, lumbar lordosis, and T1PA) was lower in the short-stay cohort, corresponding to Schwab sagittal modifier grade 0 or +. While revision surgery has been implicated as a risk factor for complications, 22 there was not a difference in rates of revision versus primary surgery in the short and long stay cohorts in our study, supporting the notion that the overall surgical invasiveness is more important than one single surgical factor in determining LOS. 23 In conclusion, our findings on preoperative characteristics associated with LOS suggest that there is likely a case “phenotype” that would benefit most from a short-stay pathway (with regards to LOS reduction) (Figure 1). While all patients stand to benefit from improved care associated with the adoption of clinical care pathways, reductions in LOS may be less reliable when pathways are applied to exceedingly complex surgeries. This notion has been previously supported by Grasu et al, 10 who instituted a clinical care pathway for patients undergoing metastatic spine tumor surgery, finding almost no impact on any measured outcome, including LOS.
While preoperative characteristics (ie, the “case phenotype”) are important to determine which patients are eligible for short-stay pathways, we have also identified several intraoperative targets associated with short LOS (procedures ending before 15:00, with a total procedural time <5 hours, and <1200 mL EBL). This suggests that clinical care pathways emphasizing protocols to help reduce EBL and operating room time could also be expected to decrease LOS. One major component could be to consistently utilize a surgical team and anesthesiologist with experience in large deformity cases, a method that has been shown to decrease complications and improve efficiency. 20 While we cannot comment on the exact reasons that patients left the operating room at certain times (eg, lack of recovery unit beds, longer surgeries, delayed extubation, etc), it is likely that a dedicated team would optimize such processes as well. Blood monitoring protocols to reduce coagulopathy have also been described in the setting of complex spine surgery and may contribute to decreased blood loss. 12 Last, there is covariance between the case complexity, EBL, and operating room time, further supporting the notion that only mild-moderate deformity cases are eligible for short-stay clinical care pathways.
Postoperatively, while no one factor reached significance, our data suggests that early mobilization and home discharge should be key targets of any clinical care pathway. While not quite reaching significance (likely secondary to study power) the median day of ambulation in the short-stay cohort was POD 1 (IQR 0-1) compared to POD 1 (IQR 0-2) in the long-stay cohort (P = .065). Adogwa et al 19 also demonstrated that patients who ambulate within 24 hours of ASD surgery had a shorter LOS. While our findings showed that the day of the week of surgery should not affect hospital LOS, this likely depends on the availability of physical therapists. Hospitals looking to institute pathways for ASD cases should closely examine availability of resources each day to determine when cases should occur. Last, there were very few patients in the short LOS group who were discharged to a rehab/inpatient facility. While this may be related to the invasiveness of the surgery and subsequent recovery, the issue of rehabilitation bed availability could certainly impact the day of discharge. Mobilization by therapists on POD 1 allows for discharge recommendations early in the hospitalization so that case managers can anticipate and address potential barriers.
There are several limitations of the current study. First, while we made every effort to collect as many variables as possible, there were some that were not ascertained from the chart for all patients. For example, the time of first case management visit, distance ambulated, type of pain medications used, and return of bowel function are all benchmarks that can delay or expedite a patient’s stay by 1 or 2 days, but could not be addressed in this analysis given that complete data was needed for every patient to be included. This is related to the second limitation of the study—while Poisson modeling most accurately estimates the expected LOS, this technique requires listwise deletions for cases with missing data, which diminished the power of the study. Third, psychosocial variables or patient motivation was not assessed, factors which have been shown to independently effect length of stay after lumbar spine surgery. Fourth, operative techniques (such as the use of anterior/lateral or minimally invasive approaches) may differ in other hospitals. 24 Fifth, the study sample was taken from one institution, leaving certain variables (eg, neuro deficits or day of surgery) underpowered to make definitive conclusions on their effects on LOS. However, a single-institution study preserves surgical technique and perioperative management among patients, providing stronger conclusions with regard to findings that reached significance. On the other hand, the institution in which this study was conducted utilizes medical co-management, specialized perioperative pain teams, and spine-specific physical therapists, limiting the generalizability of our findings to certain centers. We emphasize to readers that the expected LOS is purely based on the institution’s case mix and may vary at other centers. Last, we used a composite measure of overall patient comorbidities, ASA score, which has been previously utilized in spine surgery outcomes research. However, due to variation in reporting of comorbidities in the patient’s charts, we were not able to assess the contribution of specific comorbidities on LOS in an internally valid manner.
In conclusion, this study has identified several factors associated with short LOS that could be targeted in the creation of an adult deformity clinical care pathway designed to reduce LOS. Though there currently exists no official definition on what constitutes an “appropriate” LOS after ASD surgery, bundled care initiatives will soon force centers to begin considering LOS as a key target outcome after adult deformity surgery. Thorough preoperative screening of patients, especially with regards to their medical risk profile, enhances the ability of proposed clinical care pathways to generate predictable outcomes. Factors such as preoperative narcotic use, advanced age, and multiple comorbidities can be mitigated appropriately to reduce their associations with inpatient medical complications. While procedures can be scheduled for any day of the week (provided ample hospital resources), an efficient workflow designed to reduce overall operating room time is essential. Meticulous hemostasis, communication with anesthesiologists, and anticipation of complications is a given. Postoperatively, patients must be of adequate health status to remain on a general floor, ambulate on POD 1, and be recommended for home discharge. Many of these factors are interlinked and beget one another. Further research will be needed to identify particulars, such as patient motivation and psychosocial variables, timing of case management visits, specific strategies for pain control, and management of bowel function. Finally, care pathways should be constructed around the data provided by this study and validated in a prospective manner. Given the center-to-center variations in surgical technique, approach, perioperative care, and administrative processes, institutions can utilize the methodology outlined above to identify even more center-specific targets to be incorporated into care pathways.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.