
Abstract
Study Design:
Retrospective review of consecutive series.
Objectives:
This study sought to assess the incidence, risk factors, and outcomes of pulmonary complication following complex spine deformity surgery in a low-resourced setting in West Africa.
Methods:
Data of 276 complex spine deformity patients aged 3 to 25 years who were treated consecutively was retrospectively reviewed. Patients were categorized into 2 groups during data analysis based on pulmonary complication status: group 1: yes versus group 2: no. Comparative descriptive and inferential analysis were performed to compare the 2 groups.
Results:
The incidence of pulmonary complication was 17/276 (6.1%) in group 1. A total of 259 patients had no events (group 2). There were 8 males and 9 females in group 1 versus 100 males and 159 females in group 2. Body mass index was similar in both groups (17.2 vs 18.4 kg/m2, P = .15). Average values (group 1 vs group 2, respectively) were as follows: preoperative sagittal Cobb angle (90.6° vs 88.7°, P = .87.), coronal Cobb angle (95° vs 88.5°, P = .43), preoperative forced vital capacity (45.3% vs 62.0%, P = .02), preoperative FEV1 (forced expiratory volume in 1 second) (41.9% vs 63.1%, P < .001). Estimated blood loss, operating room time, and surgery levels were similar in both groups. Thoracoplasty and spinal osteotomies were performed at similar rates in both groups, except for Smith-Peterson osteotomy. Multivariate logistic regression showed that every unit increase in preoperative FEV1 (%) decreases the odds of pulmonary complication by 9% (OR = 0.91, 95% CI 0.84-0.98, P = .013).
Conclusion:
The observed 6.1% incidence of pulmonary complications is comparable to reported series. Preoperative FEV1 was an independent predictor of pulmonary complications. The observed case fatality rate following pulmonary complications (17%) highlights the complexity of cases in underserved regions and the need for thorough preoperative evaluation to identify high-risk patients.
Background
The surgical management of complex spine deformity is technically challenging and associated with significant perioperative complications.1-4 Postoperative pulmonary complications remain one of the leading causes of mortality in complex spine surgery.5-7
Despite the variations in the definition of postoperative pulmonary complications, the conditions classified as such generally include empyema, hemothorax, pleural effusion, hypoxia, pneumonia, pneumothorax, pulmonary edema, pulmonary embolism, respiratory arrest, atelectasis, and prolonged intubation with ventilation support.7-10
The cumulative incidence of pulmonary complications after spine surgery has ranged from 0.6% to 14.9%.2,7-9,11,12 The differences in incidence may be attributable to the variations in the definition of pulmonary events in the various studies, the underlying etiologies, and surgical complexities.2,7-12 Higher rates of pulmonary complication have been reported for neuromuscular patient populations. 10
The concern for pulmonary complications is even greater in underserved regions with limited expertise and resources. Patients in these regions typically report to health facilities when spine deformities have significantly progressed. 13 Severe spine deformities, especially thoracic curves, are known to be associated with poor pulmonary function,14-18 although the degree of pulmonary compromise is not attributable to curve magnitude alone.15,17 Impaired pulmonary function increases the risk of postoperative pulmonary complications after spine surgery. 18 The presence of other comorbidities such as malnutrition, cardiac anomalies, and neuromuscular disease coupled with major surgical procedures further increases the risk of pulmonary complications. 7 Moreover, spine surgery for these patients is characterized by significant blood loss, long operative time, and the use of 3-column osteotomies, which further increases the risk for neurologic and nonneurologic complications. 1
The mechanism of pulmonary complication following spinal surgery may be related to direct lung tissue trauma, embolization of marrow material into the lung, including fat, ventilation-associated lung injury, and transfusion-associated lung injury.19-22
Apart from increasing morbidity and mortality, postoperative pulmonary complications affect the length of stay and cost of hospitalization. 11 Identification of risk factors will help in their mitigation and perioperative management to avert pulmonary complications. However, there is paucity of literature on pulmonary complications following complex spine deformity surgery in the pediatric and young adult patients in underserved regions such as West Africa. The aims of the study were to assess the incidence and risk factors and treatment outcomes of postoperative pulmonary complications in a unique series of pediatric and young adults with severe spine deformities in a specialist orthopedic hospital in Ghana, West Africa and to demonstrate which measures can be put in place to mitigate risks and improve outcomes.
Methods
Data of 276 consecutive complex spine deformity patients aged 3 to 25 years who were treated at a single site in Ghana, West Africa from January 2015 to December 2017 was retrospectively reviewed using information from the FOCOS Spine Registry and medical records. Institutional review board approval was obtained from the Noguchi Memorial Institute for Medical Research prior to initiation of the study (Certified Protocol Number: 057/16-17). Research data was initially extracted in Microsoft Excel format and exported into Stata 14 software for analysis. The primary outcome was postoperative pulmonary complication, which was defined as any adverse pulmonary event requiring intervention beyond the postoperative standard of care. These events include respiratory distress, prolonged intubation of more than 48 hours, re-intubation, pneumonia, acute respiratory distress syndrome, significant pneumothorax requiring chest tube insertion and tracheostomy. Record review for adverse pulmonary events was restricted to events that occurred within the first 6 weeks after surgery. Spine deformity etiology of any type was included in the analysis. Patients were divided into 2 groups for the analysis of complications and risk factors: group 1—patients who developed pulmonary complications and group 2—patients who did not develop pulmonary complications. Multivariate logistic regression analysis was performed to evaluate the strength of the association of risk factors.
Results
A consecutive series of 276 pediatric and young adult spine deformity patients were reviewed. 94 patients (34.06%) were aged 3 to 10 years, 141 patients (51.09%) were aged 11 to 17 years, and 41 patients (14.86%) were aged 18 to 25 years. Surgical procedures included posterior-only in 262 patients, combined anterior and posterior in 7 patients and 2-staged posterior-only procedures in 7 patients, staged on the average 1 week apart. Etiology of the deformities was idiopathic in 145 patients (52.54%), congenital in 59 patients (21.38%), post tuberculous (post TB) in 44 patients (15.94%), neuromuscular in 14 patients (5.07%), and neurofibromatosis in 14 patients (5.07%). A total of 154 patients (55.8%) had scoliosis, 60 patients (21.74%) had kyphosis, and 62 (22.46%) had kyphoscoliosis. A total of 17 patients had postoperative pulmonary complications (group 1) representing a cumulative incidence of 6.16%. In all, 259 patients had no pulmonary complications (group 2). Gender ratio (male/female) was similar in both groups: 0.89 versus 0.63. Mean age was 13.2 years (±5.0) and 12.5 years (±4.48) in groups 1 and 2, respectively (P = .55).
The mean preoperative body mass index (BMI) was comparable in group 1 (M = 17.2 ± 2.31 kg/m2) and group 2 (M = 18.4 ± 3.49 kg/m2, P = .15). Preoperative sagittal Cobb angles were similar in both groups (M = 90.6° ± 39° vs M = 88.7° ± 48°, P = .87), respectively. The range of preoperative sagittal Cobb angles were 41° to 203° (group 1) versus 11° to 263° (group 2). Average preoperative coronal Cobb angle in group 1 was 95° (±24.68°) compared with 88.5° (±32.28°) in group 2 (P = .43). The range of preoperative Coronal cobb angles were 56° to 144° (group 1) versus 18° to 231° (group 2).
In terms of pulmonary function, preoperative forced vital capacity (FVC) (%) was significantly lower in group 1 (M = 45.3 ± 15.59) compared with group 2 (M = 62.0 ± 24.69, P = .02). Likewise, preoperative forced expiratory volume in 1 second (FEV1) (%) was lower in group 1 (M = 41.9 ± 15.45) compared with group 2 (M = 63.1 ± 21.13, P < .001). Halo gravity traction had no effect on pulmonary function test in either group (Table 1).
Summary of Demographic, Clinical and Surgical Logs by Postoperative Pulmonary Complication Status.a
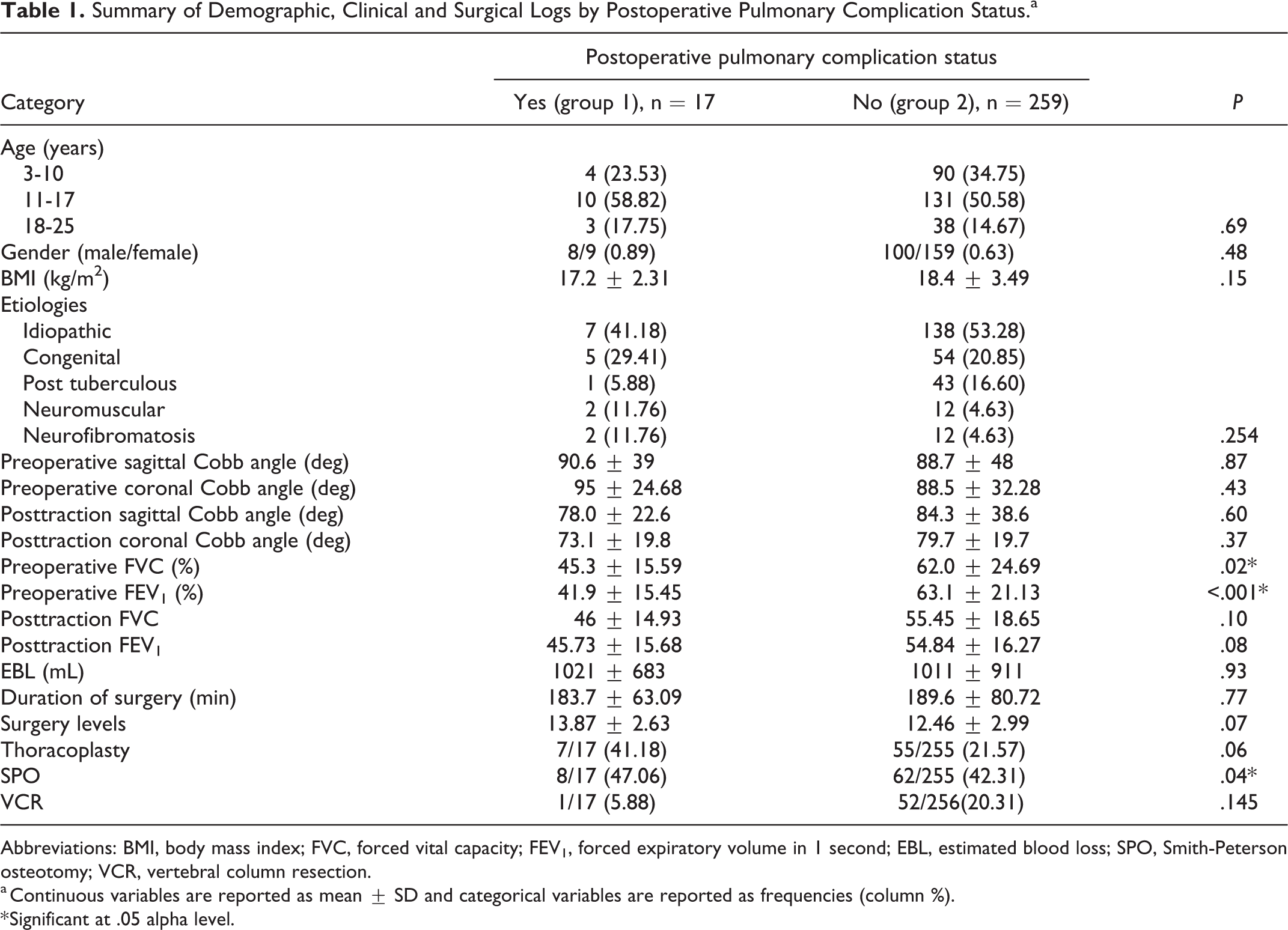
Abbreviations: BMI, body mass index; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; EBL, estimated blood loss; SPO, Smith-Peterson osteotomy; VCR, vertebral column resection.
a Continuous variables are reported as mean ± SD and categorical variables are reported as frequencies (column %).
* Significant at .05 alpha level.
The average duration of surgery (minutes) in group 1 (M = 183.7 ± 63.09) was comparable to that in group 2 (M = 189.6 ± 80.72, P = .77). Average number of levels fused in group 1 (M = 13.87 ± 2.63) was similar to that of Group 2 (M = 12.46 ± 2.99, P = .07). The average estimated blood loss (EBL) in group 1 (M = 1021 ± 683 mL) was comparable to group 2 (M = 1011 ± 911 mL, P = .93). In terms of osteotomies, thoracoplasty and spinal osteotomies such as Ponte, pedicle subtraction, and vertebral column resection were performed at similar rates in both groups. However, Smith-Peterson osteotomy was performed at a higher rate in group 1 (Table 1).
Predictors of Pulmonary Complications in Multivariate Analysis
Only preoperative FEV1 was found to be a significant independent predictor of pulmonary complication in multivariate analysis. Multivariate logistic regression revealed that every 1% increase in preoperative FEV1 (%) decreases the odds of pulmonary complication by 9% (OR = 0.91, 95% CI 0.84-0.98, P = .013), after controlling for age, gender, coronal and sagittal curve types and magnitude etiology, BMI, FVC, duration of surgery, EBL, thoracoplasty, and spinal osteotomies (Table 2).
Multivariate Logistic Regression Estimates of the Risk Factors for Pulmonary Complications.
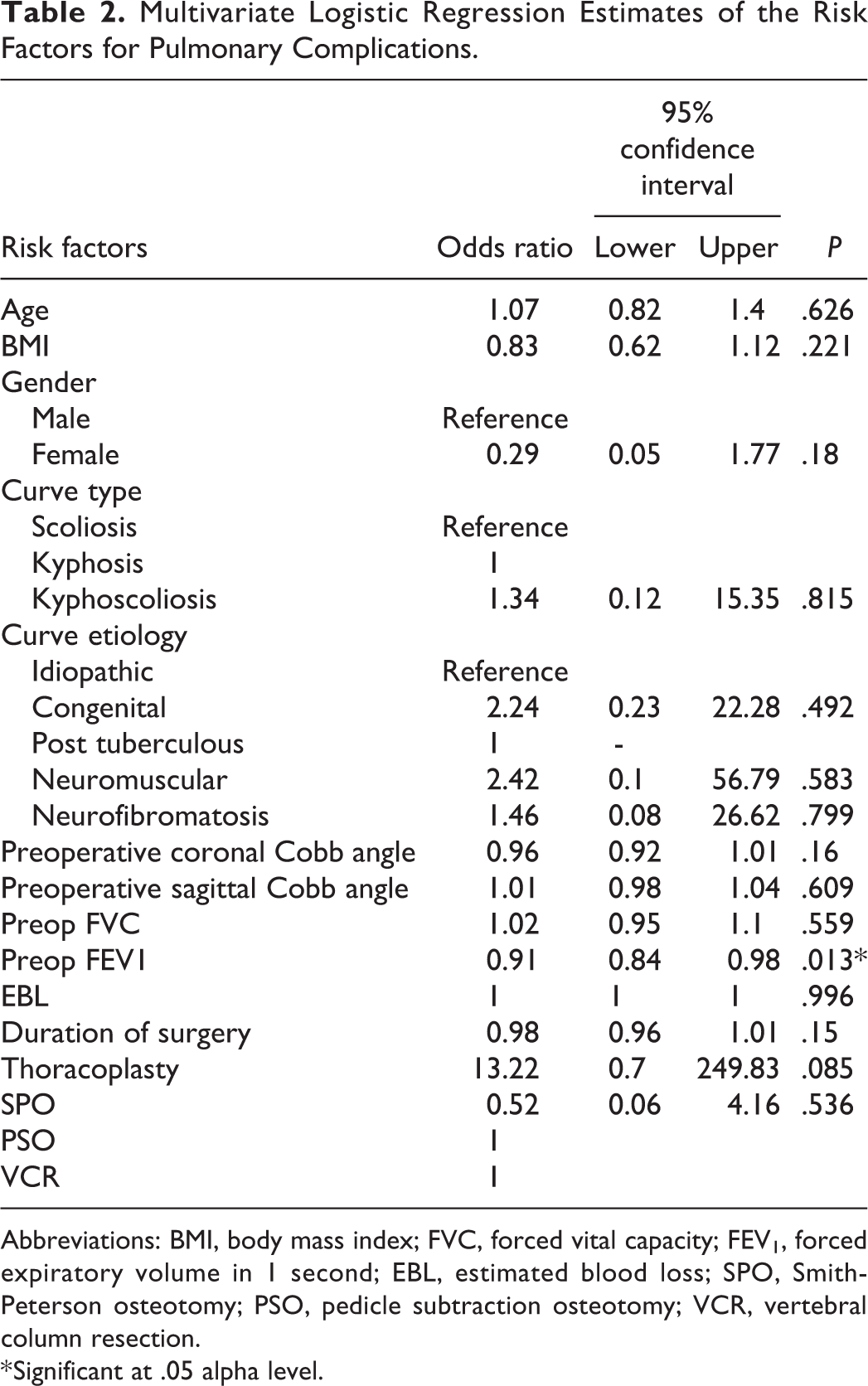
Abbreviations: BMI, body mass index; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; EBL, estimated blood loss; SPO, Smith-Peterson osteotomy; PSO, pedicle subtraction osteotomy; VCR, vertebral column resection.
* Significant at .05 alpha level.
Outcomes of Pulmonary Events by Etiology
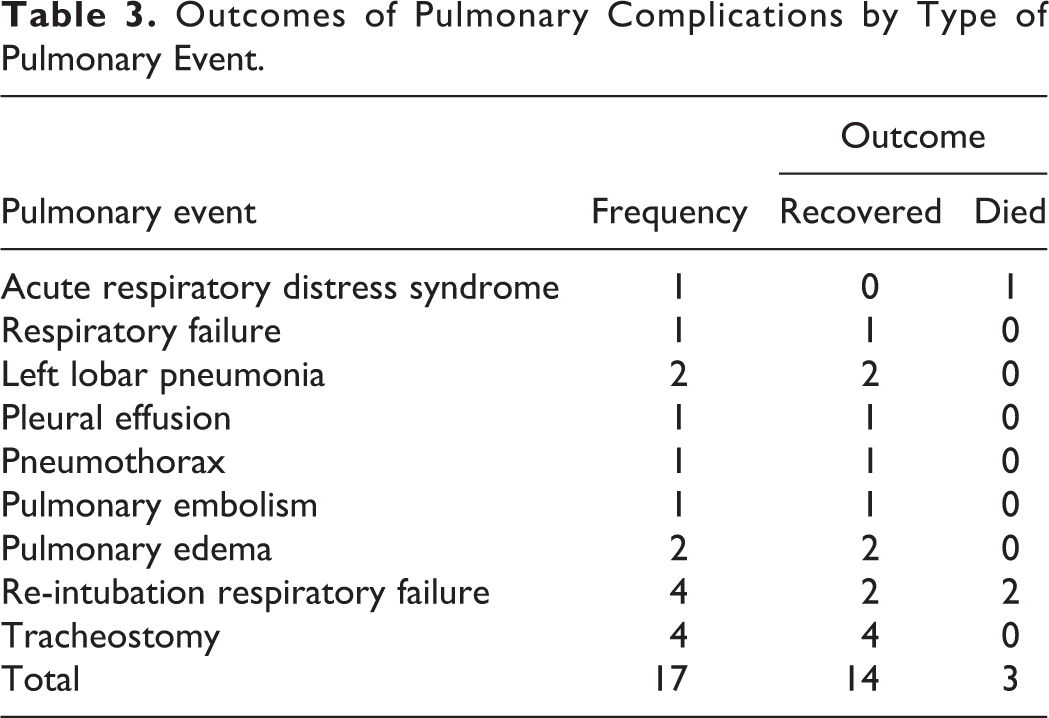
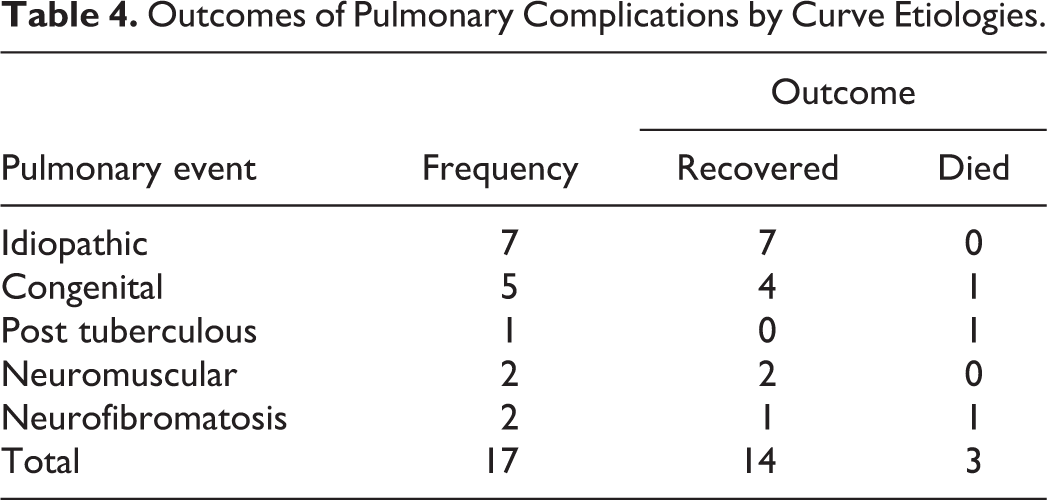
The etiologies of the 17 (6.16%) patients who developed complications as a percentage of the total cohort (276 patients) comprised 7 (2.54%) idiopathic, 5 (1.81%) congenital, 2 (0.72%) neuromuscular (NM), 2 (0.72%) neurofibromatosis (NF), and 1 (0.36%) post TB. A stratified analysis of pulmonary complication rates based on deformity etiologies were 4.83% among idiopathic patients, 8.47% in congenital patients, 14.29% among NM patients, 14.29% among NF patients, and 2.37% in post TB patients. There were 3 mortalities (1 NF, 1 post TB and 1 congenital) representing a case fatality rate of 17.6%. The details of the outcomes of pulmonary events by type of pulmonary event and deformity etiologies are shown in Tables 3 and 4, respectively. Table 5 shows details of patients with postoperative pulmonary fatalities.
Outcomes of Pulmonary Complications by Type of Pulmonary Event.
Outcomes of Pulmonary Complications by Curve Etiologies.
Details of Patients With Postoperative Pulmonary Fatalities.
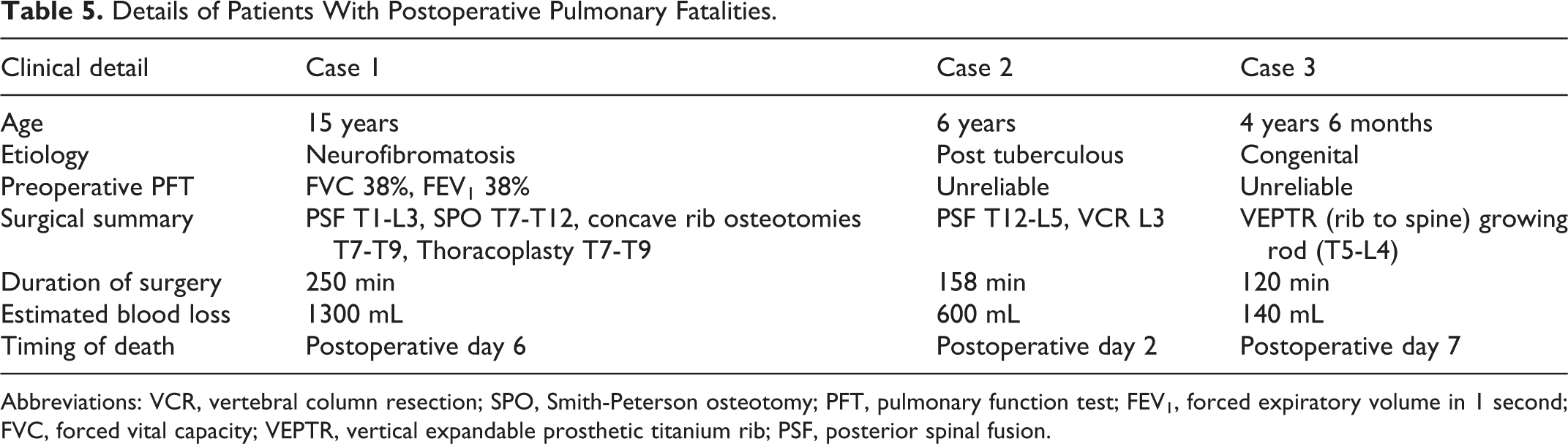
Abbreviations: VCR, vertebral column resection; SPO, Smith-Peterson osteotomy; PFT, pulmonary function test; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; VEPTR, vertical expandable prosthetic titanium rib; PSF, posterior spinal fusion.
Discussion
The occurrence of pulmonary complications after spine surgery depends on preoperative comorbidities, underlying etiology, surgical complexities, and age. The cumulative incidence of postoperative pulmonary complications observed in this cohort was 6.16%. The stratified analysis of pulmonary complication rate based on etiology was 4.83% among idiopathic patients, 8.47% in congenital patients, 14.29% among NM patients, 14.29% among NF patients, and 2.37% in post TB patients. This incidence is within the range reported by previous studies.2,7-9,11,12 Reames et al 9 reported an overall pulmonary complication rate of 1.0% after reviewing a heterogenous cohort of 19 360 patients following pediatric scoliosis surgery. Patil et al 11 also reported a postoperative pulmonary complication rate of 8.1% among idiopathic scoliosis patients <18 years old. Wu et al 8 reported a pulmonary complication rate of 13.5% among a cohort of 323 patients with congenital scoliosis who underwent posterior instrumentation and fusion. Yin et al 12 also reported a 14.9% postoperative pulmonary complications in patients who underwent posterior instrumentation and fusion surgery for congenital scoliosis. Kang et al, 10 however, reported 50% rate of pulmonary complications in patients with NM scoliosis.
One mechanism of pulmonary complication is the direct injury to pleural tissues associated with invasive surgical spine procedures that exposes the thoracic or pleural membranes.19,22 For our patient cohort, thoracoplasty was performed to reduce posterior thoracic rib prominence or as part of the exposure and complex releases to the spinal column and rib cage. The proportion of patients who underwent thoracoplasty was similar in patients who developed pulmonary complications (41.18%) and those who did not develop pulmonary complication (21.57%), P = .06.
Spine surgery can cause significant transient decline in PFT up to 60% of preoperative values with a gradual return to baseline 1 to 2 months after surgery. 23 Patients with poor baseline PFT are more likely to experience further deterioration in their PFT after spine surgery compared to their counterparts with good baseline pulmonary function. Nevertheless, there are mixed findings in literature about the effect of baseline PFTs on pulmonary complications after spine deformity surgery. In the present study, we observed that patients who developed pulmonary complications had significantly lower baseline FVC and FEV1 values (% predicted) than those who did not develop pulmonary complications. Further analysis with multivariate logistic regression revealed that only preoperative FEV1 was an independent predictor of pulmonary complications. Yin et al 12 found that FEV1 and FVC were not independent predictors of pulmonary complication in a cohort of patients with congenital scoliosis. Likewise, Liang et al 24 found that baseline PFT was not an independent predictor of pulmonary complication in their cohort of 88 scoliotic patients consisting of heterogenous etiologies. However, Kang et al 10 found that low preoperative FEV1 (<40%) was an independent predictor of pulmonary complication in patients with neuromuscular scoliosis. They also found that FVC <39.5% was an independent predictor of pulmonary complication.
Although the overall cumulative incidence of mortality related to pulmonary complications in the entire cohort was 3/276 (≈1.1%), the case-fatality rate was 17.6% among patients who developed postoperative pulmonary complications. This highlights the likelihood of an adverse outcome when there is a pulmonary complication. Previous studies have also documented significant mortality following postoperative pulmonary complications.5-7 Imposti et al 7 found that mortality rate following pulmonary complications was 3.61 per 1000 persons per year. Pumberger et al 5 also assessed the risk factors for in-hospital mortality following lumbar fusion surgery and found that patients who developed postoperative pneumonia had 3 times greater risk of mortality whiles those who developed pulmonary embolism had 10 times greater risk of mortality. The case-fatality rate observed in the present series of pediatric and young adult spine deformity patients underscores the need for proactive perioperative measures to reduce pulmonary complications.
The 6.16% incidence of pulmonary complication recorded in this series is commendable for a private facility in low-resource setting such as Ghana. Various perioperative measures have enabled us to achieve such comparable pulmonary complication rates despite the complexities of the spine deformity cases present in this cohort. These measures include routine preop multidisciplinary case review conference with the various specialties involved (surgery, anesthesia, nutrition, cardiology, physiotherapy and nursing), nutrition optimization to improve BMI, postoperative physical therapy and chest rehabilitation, the use of spirometer for breathing exercises, elective overnight ventilation after surgery, and early application of tracheostomy at the earliest sign of difficulty in weaning off ventilation. In a sense, we have tried to mirror the standard of care in developed regions.
Strengths and Limitations
This article is the largest single-site review of postoperative pulmonary complications following complex spine deformity surgery in West Africa. We have been able to demonstrate the incidence of postoperative pulmonary complications and the risk factors and outcomes of pulmonary events. This study, in our opinion, fills the void in research for this topic in underserved regions where complex spine deformities abound. Our article has demonstrated that comparable postoperative pulmonary complication rates can be achieved with appropriate interventions by a multidisciplinary team even in low-resource settings. This highlight the benefits of skills training and investment in health infrastructure in developing settings. However, as a retrospective study, there are certain limitations. Analysis and findings were based on only data that could be retrieved. The study reported on early pulmonary complications (up 6 weeks postoperatively), hence it is possible that the complication rate may vary if patients were followed over a longer period after surgery. Moreover, we do not perform PFT assessment in children younger than 5 years. Reliable and reproducible PFTs were only obtained in patients >6 years who could cooperate for the pulmonary function testing procedure. PFT assessment in neuromuscular patients is challenging hence sleep studies of oxygen saturation may be a better predictor of pulmonary outcome. Clinical signs that show poor PFT even without numbers are alternative guides for evaluating high-risk patients. These clinical cues include respiratory rate, flaring of alae nasi, use of accessory respiratory muscles, exercise tolerance and oxygen saturation studies.
Conclusion
We report a 6.16% cumulative incidence of pulmonary complication in our series, which is within the range reported in other cohorts. The pulmonary complication rate varied among different etiologies. Preoperative FVC and FEV1 were significantly lower in the group that developed pulmonary complications. However, FEV1 was the only significant independent risk factor for pulmonary complications. The high case-fatality rate observed implies the need for thorough preoperative evaluation to identify high-risk patients and the need for proactive perioperative measures to mitigate morbidity and mortality. Our comparable complication rate demonstrates positive effect of multidisciplinary skills training and appropriate health infrastructure in low-resource settings.
Footnotes
Authors’ Note
Harry Akoto currently practices as a consultant neurosurgeon at the Korle-Bu Teaching Hospital, Accra, Ghana. Audrey Oteng-Yeboah currently practices as a consultant anesthetist at the Korle-Bu Teaching Hospital, Accra, Ghana. Halima Bidemi Yahaya currently practices as a specialist anesthetist at the Zenith Medical and Kidney Center, Abuja, Nigeria.
Acknowledgments
The authors acknowledge other members of the FOCOS Spine Research Group (FSRG) who contributed in diverse ways at various stages of the paper but are not listed, by names, as authors to this study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: OBA receives grants, personal fees, and other from K2M and other from WEIGAO, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.